
Abstract
Background and aim:
Stair ascent is a particularly challenging task for transfemoral amputees. The aim of this clinical note was to describe the kinematic features of foot clearance in transfemoral amputee who can ascend stairs using a step-over-step strategy.
Technique:
The marker trajectories of the first metatarsophalangeal joint (Mt1) and clearance height were measured in two transfemoral amputees who could (TF1) and could not (TF2) climb stairs using a step-over-step strategy.
Discussion:
The Mt1 marker trajectories of the TF1 moved backward in the early swing phase, and the trajectory followed an off-centered parabolic arc to achieve a similar clearance height as able-bodied subjects. TF2 could not climb the stairs without tripping in each step. An effective compensatory strategy to avoid tripping during stair climbing may be to use the hip joint for a backward extension and rapid flexion of the prosthetic leg during the early swing phase.
Clinical relevance
The foot clearance strategy in transfemoral amputees who can climb stairs using a step-over-step strategy will help us better understand adaptive prosthetic control and thus develop more effective gait rehabilitation programs.
Background and aim
Stair ascent is a particularly challenging task for transfemoral amputees (TFAs). Able-bodied individuals generally use a traditional step-over-step (SOS) gait strategy, where one foot is placed on each stair during stair ambulation. 1 However, these tasks are extremely difficult for the TFAs because of the missing biological knee joint. Consequently, TFAs routinely adjust their stair gait strategy, adopting instead a conservative step-to-step (STS) gait strategy, in which they must place both feet on the same step before ascending. 2 A STS strategy not only influences efficiency and speed1,3 but also looks uncosmetic. 4
In a previous study, unique compensatory strategies during the stance phase were observed in TFAs who can ascend stairs using a SOS strategy without an active artificial prosthetic knee joint or handrail use. 5 During the SOS stair ascent strategy, the prosthetic knee joints must flex to permit foot clearance of the stairs to avoid tripping.6,7 However, there is very limited information regarding the compensatory strategy required to avoid tripping during the swing phase in TFAs. The aim of this clinical note was to describe kinematic features of foot clearance in a TFA who can ascend stairs using the SOS strategy.
Technique
Subjects
The study protocol was approved by the local ethical committee and is in accordance with the guidelines set out in the Declaration of Helsinki (1983). Four healthy able-bodied subjects (ABS) and two male TFAs (TF1 and TF2) volunteered for the investigation conducted at National Rehabilitation Center for Persons with Disabilities in Japan. (Table 1). TF1 routinely performed stair ascent in his daily life using the SOS strategy.
Subjects characteristics.
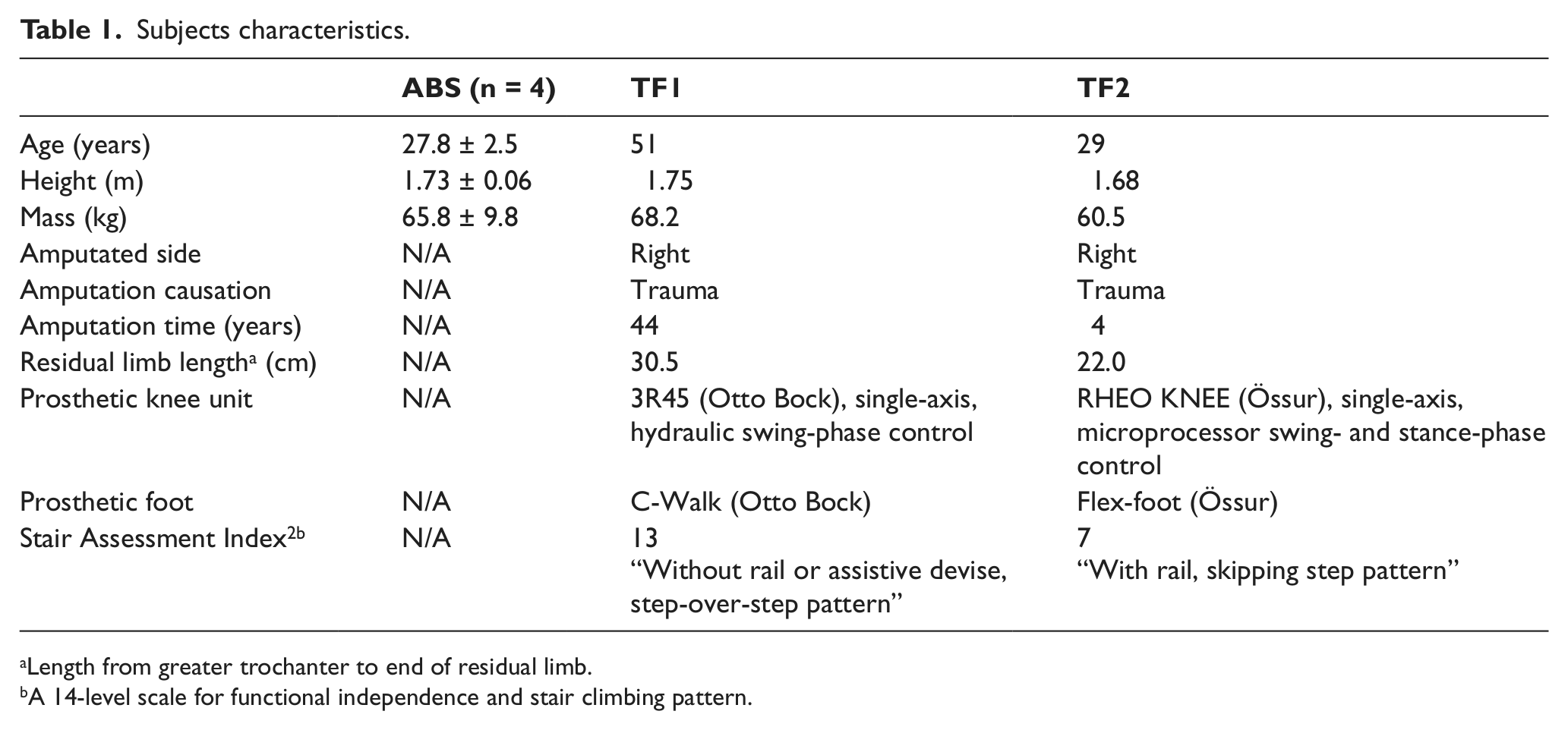
Length from greater trochanter to end of residual limb.
A 14-level scale for functional independence and stair climbing pattern.
Task and procedure
The subjects were asked to perform SOS stair ascent (normal reciprocal stepping pattern) at their preferred speed. From the lowest step, the subjects climbed a custom-built staircase of five steps (height 16 cm, width 80 cm, tread 30 cm, inclination 28°). 5 Although TF1 had mastered SOS stair ascent, he practiced the task for as much time as was needed before data collection. Then, five trials beginning with their sound leg were recorded for the TFAs. The ABS started their stair ascent beginning with their left leg.
Data collection and analyses
In the present study, kinematic data were collected at 60 Hz using a 12-camera motion analysis system (VICON 512; VICON, UK). Reflective markers were placed on the top edges of the second and third steps to mark the support surface. Markers were also placed on the participants’ first metatarsophalangeal joint or similar location of the prosthetic foot (Mt1). The positional data of the reflective markers were low-pass filtered by a fourth-order zero-lag Butterworth filter with a cutoff frequency of 6 Hz.
During the swing phase, we determined the trajectories of the Mt1 markers on the prosthetic foot of the TFA and the right foot of the ABS. Clearance height was defined as the vertical distance between the Mt1 marker and the edge of the stair as the subject’s foot passed over the edge of steps 2 and 3 (Figure 1(a); CLstep2 and CLstep3, respectively). Data were averaged for five trials in both groups.
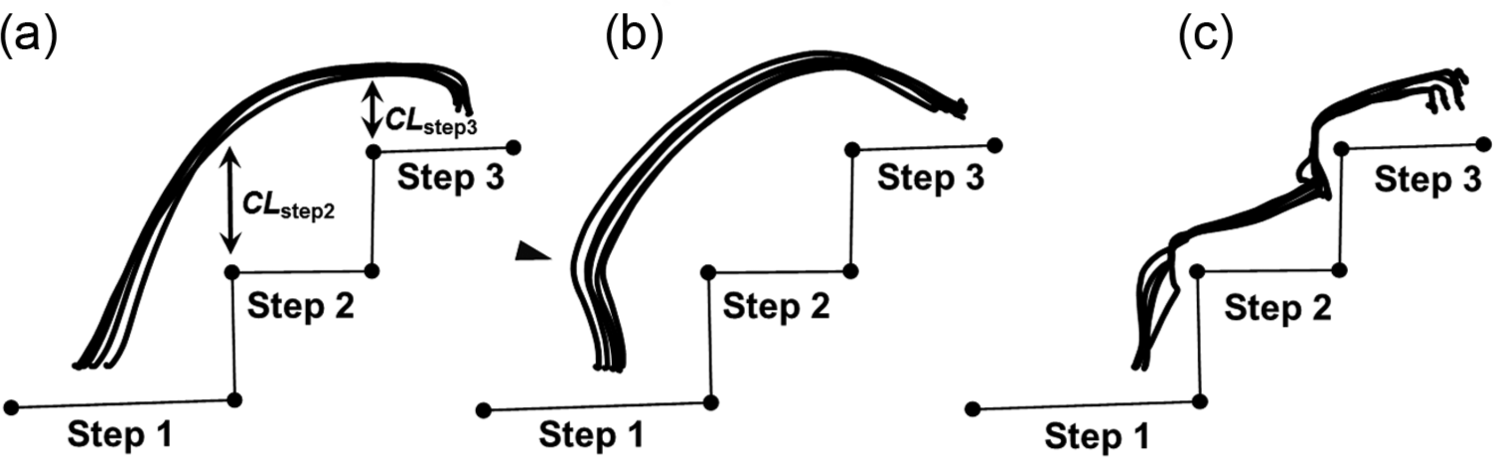
Trajectories of the Mt1 marker during the swing phase in (a) ABS, (b) TF1, and (c) TF2, respectively.
Results
The results from the study can be seen in Table 1 and Figures 1 and 2.
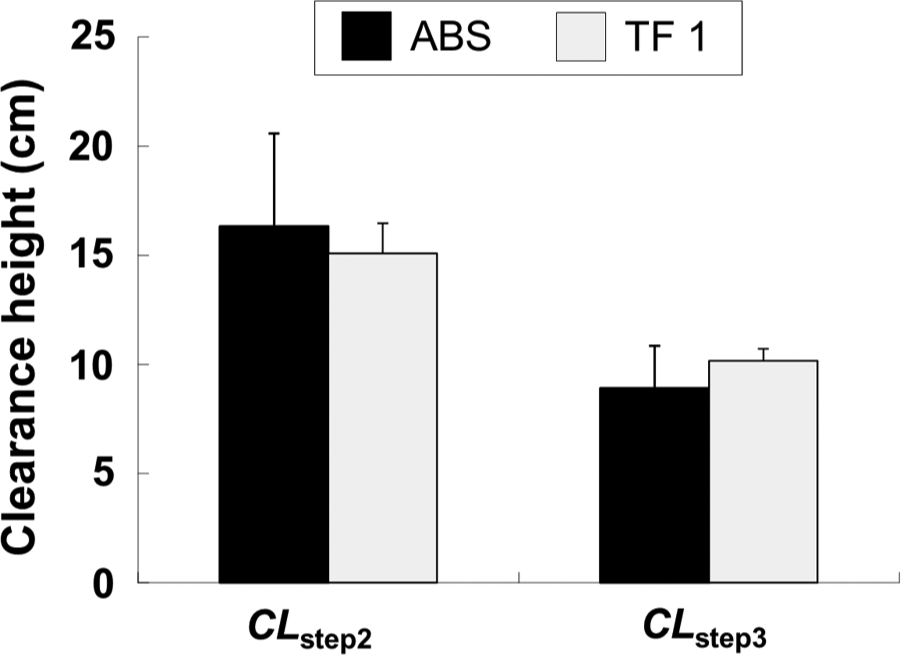
Comparison of clearance height (CLstep2 and CLstep3) between ABS and TF1.
Discussion
The aim of the present study was to describe the kinematic features of foot clearance in a TFA who can ascend stairs using the SOS strategy. In this study, the Mt1 marker in ABS depicted parabolic trajectories (Figure 1(a)), which were consistent with a previous study. 8 Interestingly, the Mt1 marker trajectories of the TF1 moved backward in the early swing phase (arrowhead in Figure 1(b)) and the trajectory followed an off-centered parabolic arc. These movement strategies were not seen in TF2, where Mt1 marker trajectory traced the stairs with tripping in each step (Figure 1(c)). As a consequence, the CLstep2 and CLstep3 of TF1 were similar to those of the ABS (Figure 2).
To our knowledge, this is the first study to evaluate foot clearance strategy during a SOS stair climbing strategy in TFA. The off-centered parabolic trajectory may be a compensatory movement strategy for ensuring foot clearance by the hip joint in a prosthetic leg. Byrne and Prentice 9 reported that a total knee arthroplasty patient was able to maintain toe clearance when overcoming obstacles by increasing hip flexor work during the elevation phase of swing. Furthermore, in our previous study, 5 TFAs who could climb stairs using the SOS strategy showed a greater hip flexion velocity in the prosthetic limb during the early swing phase compared to ABS, suggesting that the TFAs would intentionally flex their hip joints rapidly to replicate the knee joint in conjunction with the hip flexion. Hence, as corroborated by previous research, the present study showed that the combination of extension–flexion by the hip joint in the prosthetic leg during the early swing phase could be an effective compensatory strategy to achieve foot clearance during SOS stair climbing in TFAs.
It is noteworthy that TF1 used a passive, single-axis prosthetic knee joint (3R45; hydraulic, swing-phase control). As we previously reported, 5 a passive single-axis prosthetic knee joint may be an important factor for ascending stairs using the SOS pattern than multi-axis or microprocessor knee because it might increase voluntary control or affect the reaction of the knee when the body moves. Indeed, TF1 preferred to use a nonmicroprocessor knee mechanism rather than C-Leg because it gave them more voluntary knee control. 10 Similarly, another study 11 found that, compared to a multi-axis knee, a single-axis knee component would be more versatile for an amputee who has the muscular ability to control the prosthesis and the endurance to maintain a high level of voluntary control for an extended period of time. The investigators suggested that for these individuals, a single-axis knee would allow them to initiate swing more easily. Therefore, a passive, single-axis prosthetic knee joint would be a reasonable mechanism for TF1 during stair climbing using the SOS strategy.
Despite the recent establishment of rehabilitation for stair descent using the SOS strategy, 12 gait rehabilitation for stair ascent in TFA is not available. We have already reported that both (1) extending the prosthetic knee joint to prevent knee flexion generated by the body’s weight and (2) lifting the entire body in an upward direction using strong counter-movements and greater joint extension of the sound leg during the stance phase are important for SOS stair climbing in TFA. 5 In the present study, we showed that a backward extension and rapid flexion of the prosthetic leg during the early swing phase using the hip joint would also be an effective compensatory strategy to avoid tripping (Figure 1(b)). Therefore, our past and current findings suggest that a combination of these movements could be effective compensatory strategies for SOS stair climbing in TFA without an active artificial prosthetic knee joint or handrail use.
There are several concerns regarding the interpretation of the findings. First, due to the limited number of TFAs who can climb stairs in SOS strategy without an external aid, only one TFA was available for the present study. To verify the effectiveness of the compensatory strategies observed in this study and establish practical gait rehabilitation by the therapist, there should be multiple subjects in future research. Second, we could not determine the ground reaction force and joint kinetics due to the experimental setting. Third, in the present study, we could not identify how our TF1 acquired the compensatory movement over the past decade or so. Stair climbing using SOS strategy would depend on knee mechanism, patient ability, and combinations of both variables. Clearly, additional work is necessary to determine the mechanisms responsible for the SOS stair ascent pattern in TFAs.
Key points
Unlike able-bodied subjects, a transfemoral amputee (TFA) who can ascend stairs using a step-over-step (SOS) gait strategy without an active artificial prosthetic knee joint or handrail use showed off-centered parabolic trajectories of Mt1 marker during the swing phase of stair climbing.
A backward extension and rapid flexion of the prosthetic leg during the early swing phase using the hip joint may be an effective compensatory strategy to avoid tripping during stair climbing.
A passive, single-axis prosthetic knee joint may be a reasonable mechanism for TFAs during stair climbing using the SOS gait strategy.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This work was supported by Grant-in-Aid for Young Scientists (B; No. 21700569) from the Japanese Ministry of Education, Culture, Sports, Science and Technology.