
Abstract
Background: Physical activity is a positive component of human health. Its effects are associated with improvement in physical, psychological and social aspects of quality of life. Physical activity is therefore an important factor in the rehabilitation of amputees.
Objective: To analyse the relationship between physical activity and quality of life for amputees in southern Brazil.
Study Design: Descriptive, cross-sectional design with nonrandomized sample.
Methods: A total of 40 questionnaire instruments were distributed to subjects who met the inclusion criteria, with a response rate of 55% (22 individuals, n = 15 males, n = 7 females). Outcome measurements were obtained through the International Physical Activity Questionnaire and World Health Organization Quality of Life–Bref.
Results: The sample was characterized by physically active adult male prosthetic users with positive quality of life, and amputation below the right knee caused by mechanical trauma related to traffic accidents with motorcycles. Significant correlations were identified between all domains of quality of life and between level of physical activity and psychological quality of life. No correlation was identified between gender and quality of life variables or physical activity levels.
Conclusions: This study showed that in very active amputees of both genders, level of physical activity is not associated with quality of life except for the psychological domain.
Clinical relevance
This paper contributes to understanding of the importance of physical activity for the quality of life of amputees, principally of active individuals with lower limb amputations. It provides evidence for the relevance of physical mobility in the process amputee rehabilitation, mainly for psychological domain of quality of life.
Introduction
Physical activity is associated with physical fitness and can be considered a positive aspect in the rehabilitation of amputees.1-3 Health statistics indicate that about 40% of Brazilians aged 25– 49 years do insufficient physical activity to maintain health. 4 Studies show that physical inactivity causes conditions associated with significant morbidity and mortality in contemporary societies,5,6 which can be associated with some of the causes of amputations.7,8 However, studies indicate that regardless of cause, amputation can cause damage to the welfare and quality of life of affected individuals.7,9,10
Estimates and causes of amputations
Official statistic data show that approximately 24.6 million Brazilians have a disability, and 478,597 have some kind of amputation. 11 Global statistics estimate the incidence of amputation at around 2.8–43.9 cases per 100,000 people per year, 8 while statistics for Brazil estimate the incidence at around 13.9 cases per 100,000 people per year. 12 Studies show that the major cause (80%) of amputations in Brazil is peripheral vascular disease caused primarily by diabetes mellitus.7,9,10,12 This mainly affects individuals aged 50–75 years. 9 Traumatic injuries are the second major cause (10.6%) of amputation in Brazil, primarily affecting individuals aged 25–44 years, and mainly caused by traffic and work accidents.7,9,10
Rehabilitation of amputees
The most severe consequence of amputation is mortality, which results in almost 20% of cases of bilateral lower limbs amputations. 13 However, prevalent consequences of amputation in Brazil include functional impairment, psychiatric disturbances and occupational absence, with reduction in quality of life.7,9-11,12 Rehabilitation of amputees in Brazil has advanced significantly in recent years, highlighting the multidisciplinary interventions and legal support in the public health system. 8 However, studies have demonstrated that the Brazilian health system still presents difficulties in rehabilitation of amputees, such as delays in referral to appropriate treatment, delays in inclusion in rehabilitation programmes, and socioeconomic difficulties.7,10 Numerous studies have shown that an active lifestyle and welfare are important factors in the rehabilitation process.8,10,13-18 However, several studies indicate a lack of consensus on the best way to assess these factors.13,19-22
The purpose of this study
The primary purpose of this study was to analyse the relationship between physical activity and quality of life among amputees in southern Brazil. The secondary purpose was to describe sociodemographic and clinical data as well as physical activity and quality of life characteristics of amputees according to gender. We hypothesized that when the level of physical activity of an amputee is higher, then quality of life, especially among men, will be greater.
Methods
Study design
This research is a descriptive cross-sectional study, with subjects selected by nonrandomized sampling, developed through the application of questionnaires between 2006 and 2009. The study was approved by the Ethical Committee on Research Involving Human Beings of the Santa Catarina State University (Protocol 119/2006).
Subjects
A preliminary survey conducted among administrators of clinics and hospitals providing rehabilitation in the southern states of Brazil identified approximately 800 lower limb amputees aged 18–69 years, who were invited to participate in a meeting in Florianópolis, Santa Catarina, Brazil. The meeting brought together 260 amputees.
A total of 40 subjects were selected from three states in southern Brazil who declared that they had no restrictions that could psychologically or emotionally affect their ability to recall detailed events of the last weeks or evaluate complex situations of everyday life. In addition, they were able to do physical activities such as home/yard, sports, leisure, work-related and transport-related activities.
Subjects were recruited from one rehabilitation clinic attached to a state hospital in Santa Catarina, one rehabilitation clinic-school attached to a state university in Santa Catarina, and four private prosthetic clinics in southern Brazil.
Instruments and procedures
Subjects were asked to complete the International Physical Activity Questionnaire (IPAQ),22,23 the World Health Organization Quality of Life (WHOQOL) questionnaire,24,25 and a data sheet of sociodemographic and clinical information. The IPAQ is composed of 25 questions that evaluate physical activity in four categories: leisure time; domestic and gardening (yard); work-related; and transport-related. 23 The WHOQOL-Bref, the brief version, is composed of 26 questions that quantitatively evaluate quality of life in four domains: physical, psychological, social, and environmental. 24 Based on the literature, the IPAQ and WHOQOL-Bref were chosen for the following five reasons:22–25 (1) they have sufficient psychometric consistency; (2) they are internationally accepted and widely used; (3) they are reliable and validated in the Brazilian context; (4) they have the capability to quantitatively evaluate the target variables; and (5) they provide results of sufficient accuracy to compare different groups or conditions. Scientific use of the IPAQ and WHOQOL-Bref is permitted by the World Health Organization.
On examining the principal databases, a shortage of studies on the relationship between level of physical activity and amputation, using the IPAQ in particular, was evident. Use of the IPAQ was based on the need to obtain comparable data for the general population as well as the study group for tasks both groups were able to carry out, taking into account the physical limitations of amputees. The physical activities assessed in the instrument included daily home/yard, sports/recreation and leisure activities.
The study instruments were self-administered by subjects without the intervention of researchers, who remained at the interview only to answer questions from the individuals. The instruments were returned to the investigators 48 hours after distribution. Additional information about the amputation, such as cause, level, side and treatment, was collected from the subjects’ medical records at the rehabilitation and prosthetics clinics involved.
Data analysis
Data treatment was done using SPSS 17.0 software. Analysis of central tendency through descriptive statistics (standard deviation, mean, minimum value, maximum value) was performed. Analysis of the coefficient of reliability was applied through calculation of Cronbach’s alpha (>0.70). 26 Analysis of normality distribution used the Kolmogorov-Smirnov test to demonstrate nonnormality of the data. Inferential analysis was done using nonparametric tests (the Mann-Whitney U test, Fisher’s exact test and Spearman’s correlation test). The significance level was set at 0.05 for all tests.
Classification of the level of physical activity was performed according to the criteria of the Karolinska Institute 27 and the US government’s Center for Disease Control and Prevention 28 for IPAQ, as well as physical activity level, such as sedentary (<250 metabolic equivalents of task (METs)), irregularly active (250–600 MET), active (600–3000 MET), and very active (>3000 MET). A MET can be considered an expression of the metabolic rate of an individual used to measure energy requirements for different levels of activity. METs were calculated by multiplying the reference value for each activity group (walking at work=3.3; cycling for transportation=6.0; moderate yard work=4.0; vigorous intensity leisure activity=8.0) by time spent on the activity (minimum=10; maximum=960) and number of days per week (maximum=7).27
Classification of the quality of life was performed according to the criteria of the World Health Organization 29 for the WHOQOL-Bref. Quality of life was scored over four domains: physical (7 items); psychological (6 items); social (4 items); environment (9 items); and two related general items. The items were rated on a five-point scale with a higher score indicating a higher quality of life except for items third, fourth and twenty-sixth where a lower score indicated a higher quality of life. Domain scores were calculated by multiplying the mean of the specific scores for the 24 items of the four domains by a factor of 4, which ranged from 4 to 20 scores in each domain. Transformation of the scores on a scale (0=lower quality of life; 100=highest quality of life) was performed by subtracting 4 points from the calculated score and multiplying the rest by 6.25.
Results
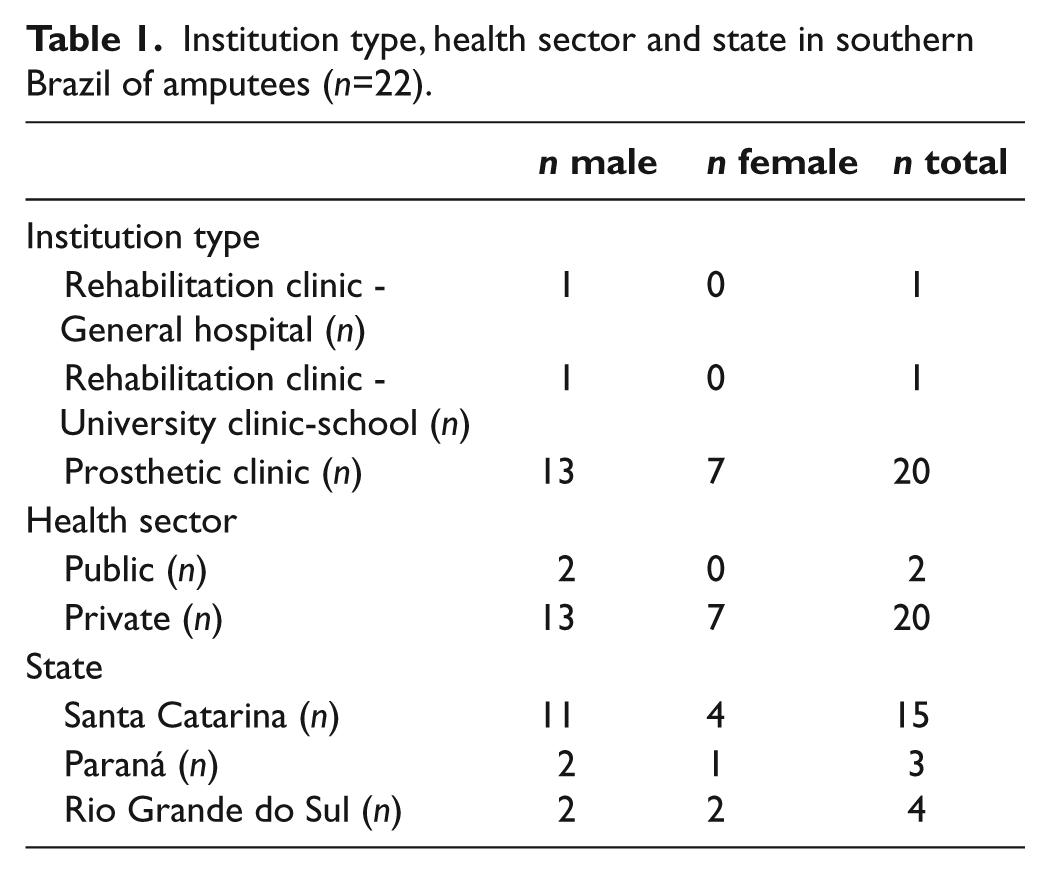
Preliminary analysis of the questionnaires revealed that three questionnaires were not returned, nine subjects did not sign consent forms, and six showed incomplete data. Thus, a total of 22 questionnaires were validated, demonstrating a return rate of 55%, mostly from the private institutions and prosthetics clinics of Santa Catarina State (Table 1).
Institution type, health sector and state in southern Brazil of amputees (n=22).
Cronbach’s alpha test for the IPAQ showed moderate (α=0.55–0.63) and for the WHOQOL good (α=0.84–0.89) internal consistency and reliability.
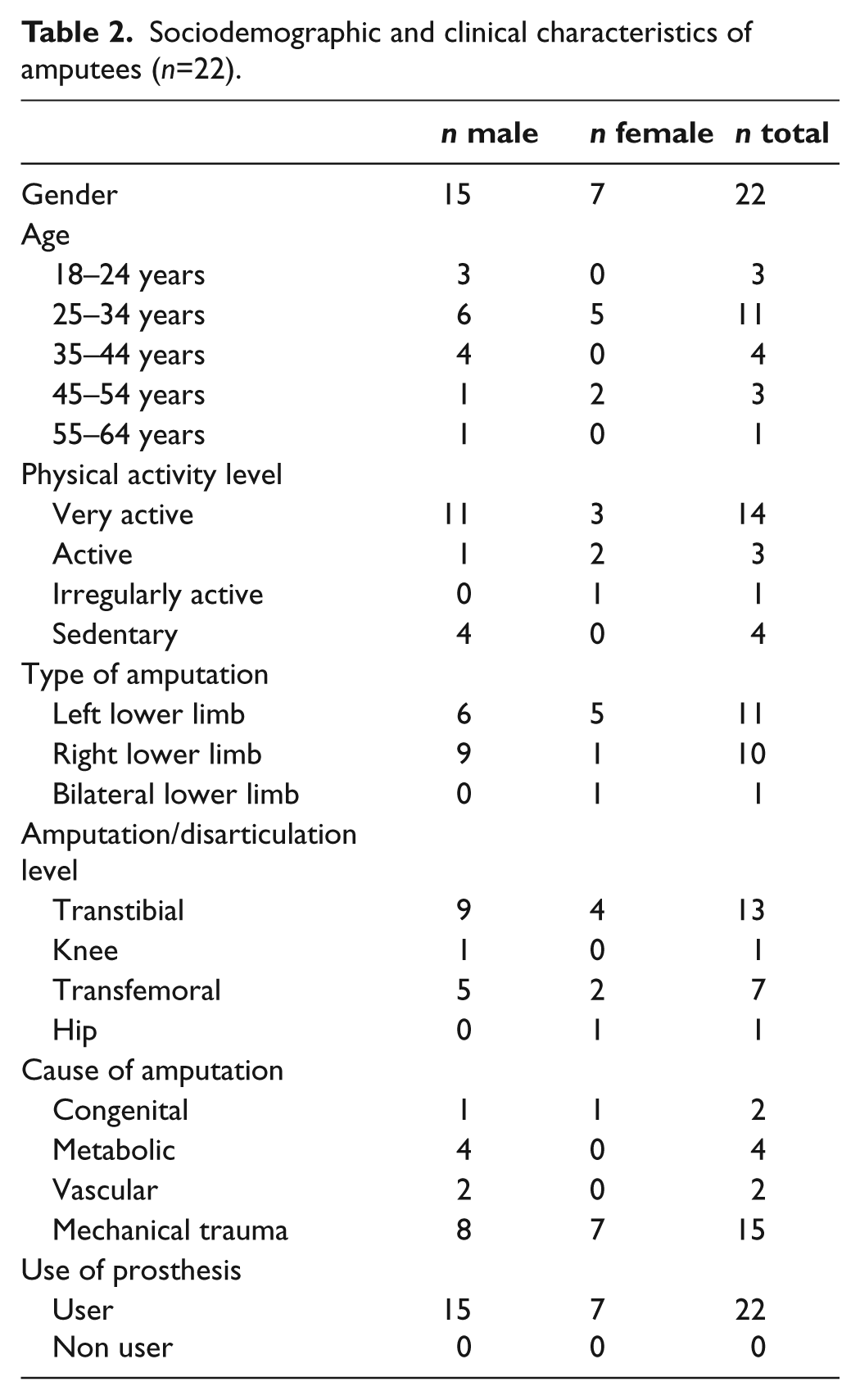
Frequency values showed that subjects in the sample were more often male, most often aged between 25 and 34 years and mostly physically active. In males, there were more amputations below the right knee, most often caused by mechanical trauma (motorcycle accidents) and all subjects were users of orthopaedic prostheses (Table 2).
Sociodemographic and clinical characteristics of amputees (n=22).
Measures of central tendency in this sample showed appropriate values for all physical activities. However, men had higher scores in all physical activity groups and women had values below the recommended level for health in the physical activities of transport and leisure (Table 3). Both genders had high average values related to sedentary behaviour; however, men showed higher scores in all types of sedentary behaviour (Table 3). Both genders showed satisfactory scores for quality of life, with the men having higher values in the social domain while women had higher values in the psychological domain. The lowest values were in the psychological domain for men and the physical domain for women (Table 3). Nevertheless, gender comparison did not show significant differences in physical activities, level of physical activity or quality of life and its domains.
Amputee physical activity, sedentary behaviour and quality of life scores by gender (n=22).
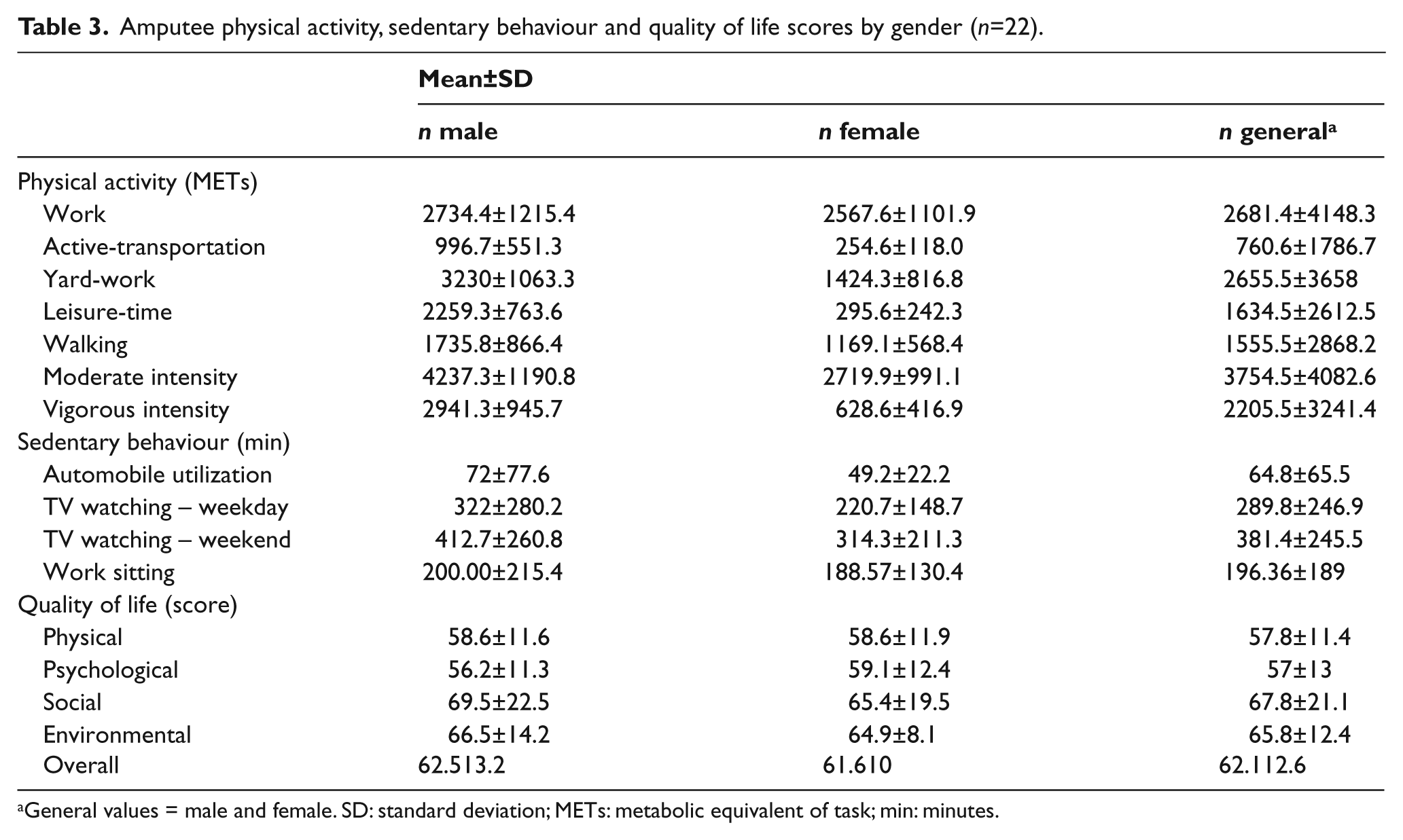
General values = male and female. SD: standard deviation; METs: metabolic equivalent of task; min: minutes.
Correlation values indicated a strong or very strong relationship between the quality of life domains (physical, psychological, social and environmental) and overall quality of life in this sample (p<0.001). However, significant correlation with level of physical activity was found only for the psychological domain in this sample (p=0.028) (Table 4).
Nonparametric correlation values (rs) between amputee physical activity level and quality of life domains (n=22).
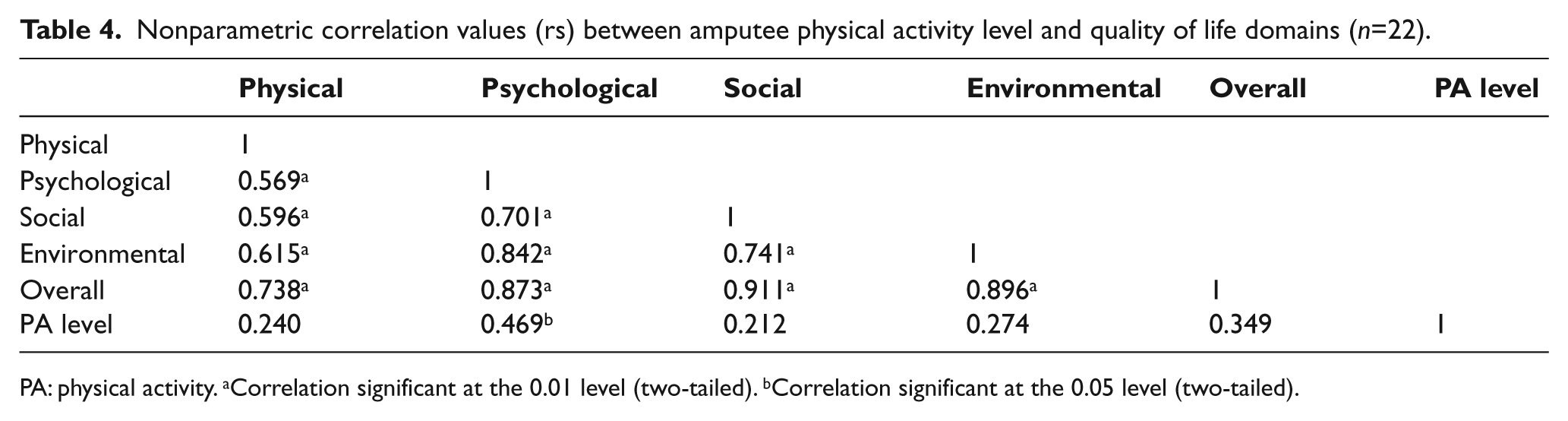
PA: physical activity. aCorrelation significant at the 0.01 level (two-tailed). bCorrelation significant at the 0.05 level (two-tailed).
Discussion
The results of this study must be analysed in the light of three relevant limitations: (a) a severe shortage of baseline studies on the relationship between level of physical activity and quality of life in amputees; (b) nonrandomized sampling based on convenience; and (c) the low number of subjects selected.
The sociodemographic results, principally the higher occurrence of men with amputations than women, are confirmed by other studies.15-17,30 This higher occurrence of amputations in men can be explained by different factors, such as association with professions that involve higher occupational risk, and fixed and modifiable habits that affect health risk.
Clinical results are confirmed by studies showing a higher incidence of traumatic causes of amputation related to transport.16,30 However, other studies show a higher incidence of vascular and endocrine diseases.12,15 In developed countries, an increase in vascular diseases, especially those associated with endocrine disorders, is evident, while in developing countries, trauma caused by working conditions and transport are widespread. 31 Results show that most of the amputations were caused by trauma in motorcycle accidents, despite studies showing that trauma is the second major cause of amputation in Brazil.7,9,10
Clinical results also show that the level and side of amputations are mainly related to etiologic factors, because they are direct consequences of peripheral vascular disease, especially diabetes, which affects the feet. 7 Unilateral amputation results confirm studies that show higher occurrence of amputation on the right side.2,3,17 With regard to the level of amputation, the results corroborate most studies that had no pre-conditions for amputation below the knee as a criterion for inclusion of subjects.15-17,31 The prevalent type of accident (motorcycle accident) may explain the high level of below knee amputation and on the right side, corresponding to the position of the brake system of the motorcycles.
With regard to quality of life and its domains, there were variations in the scores, which can be explained by several factors, such as health, transport, financial conditions and environment. The data in this study showed satisfactory quality of life scores in all domains. However, these results diverge from an Irish study, which identified poor scores in the physical, psychological and environmental domains, and very poor scores in the social domain of amputees. 16 The results are in agreement with a Scottish study that reported good physical domain scores and very good psychological, social, and environmental scores for amputee quality of life. 3
Specialized literature indicates that prosthetic rehabilitation is important, because mobility of the individual is a priority. 9 However, economic and social conditions influence access to and quality of prostheses across private and public health sectors in Brazil. 7 The results are corroborated by studies that demonstrated high prevalence of individuals who use orthopaedic prostheses.15-17 However, this result should be analysed cautiously, because most individuals in this study were selected from prosthetic clinics in the private sector, and the same products and advanced prosthetic treatments are not necessarily available in the public health sector in Brazil.7,9
An extensive literature search of the principal databases revealed a lack of studies on the relationship between level of physical activity and quality of life in amputees. Therefore, we also attempted to analyse articles that adopted other rating scales, both generic and specific. The adoption of a generic questionnaire to assess physical activity level in this study was based on the possibility of comparison with other populations. However, despite the relative reliability of survey-type questionnaires for assessing level of physical activity, this type of evaluation does not allow precise direct and indirect measurements of this variable. 32 No amputee study was found that used the IPAQ, although several studies adopted other scales.
Comparing our results of physical activity level with studies that used other specific scales, we found various studies conducted in the USA. One study of 56 amputees examined body image and participation in physical activities and sports using the Multidimensional Body Self- relations Questionnaire (MBSRQ), and found that only a few subjects could be classified as active (42.9%). 2 A Japanese study of 33 individuals with and without lower limb amputation investigated physical fitness using a cycle ergometer to determine maximal oxygen uptake of the amputees, and observed values comparable with sedentary individuals (VO2max=18.8–4.9). 1 A Brazilian study that used the IPAQ to survey the physical activity level of 2001 individuals in the general population observed that physical inactivity affects almost 60% of the population. 28
The significant correlation between level of physical activity and the psychological domain (p=0.028) was partially corroborated by a Scottish study of 25 lower-limb amputees who used prosthetics, which investigated the relationship between quality of life and the restrictions on physical activity in these individuals. A strong positive relationship was found between level of physical activity and perceived quality of life of the amputees. 3 Despite the literature showing that women have higher rates of physical inactivity than men 28 , the results failed to show significant differences between the type of physical activity, level of physical activity, and quality of life and its domains, thus diverging from the specialized literature.
Conclusion
This study analysed the relationship between physical activity and quality of life among amputees in southern Brazil, and described sociodemographic, clinical, physical activity, and quality of life characteristics by gender. We established that most of the sample was characterized by males, who were adults, prosthetic users, physically active, had a positive quality of life, and had amputation below the right knee caused by mechanical traumas, mainly by traffic accidents with motorcycles. We also verified that despite statistically significant correlation between all the variables of quality of life, significant correlation with level of physical activity only occurred for the psychological domain of quality of life. In addition, it was noted that there were no significant gender differences in quality of life and level of physical activity among this intentionally selected amputee sample. Therefore, it was not possible to consider that an increased level of physical activity is associated with a higher quality of life score in men or women, except for the psychological quality of life.
It is suggested that this study may contribute to the understanding of two relevant aspects of the rehabilitation process of amputees: (1) physical mobility; and (2) the well-being of individuals, mainly for countries with high rates of amputations, which have become a grave public health concern. However, more studies are needed that apply different research instruments among different populations, mainly with larger samples.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors report no conflicts of interest.