
Abstract
Background:
Return to sports (RTS) is frequently considered an indicator of successful recovery after anterior cruciate ligament reconstruction (ACLR). However, despite the well-recognized health benefits of physical activity (PA), little is known about objectively measured PA in the 1 to 2 years after ACLR. Given that young female athletes have a high prevalence of ACLR and lower RTS rates as compared with their male counterparts, an in-depth examination of PA in this subgroup is warranted.
Hypothesis:
We hypothesized that female youth and young adults who have had ACLR in the previous 1 to 2 years would have less moderate or vigorous PA (MVPA) compared with healthy matched controls. We also hypothesized that the ACLR group would report lower levels of sports participation, patient-reported health outcomes, and physical function.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Participants included 51 female athletes with primary unilateral ACLR for a sports-related injury in the previous 1 to 2 years and 51 age- and sports-matched controls. Outcomes included objectively measured PA (GT3X accelerometers), previous and current sports participation and RTS, body mass index, Knee injury and Osteoarthritis Outcome Score (KOOS), triple single-leg hop, and one-leg rise. Mean within-pair differences with 95% CIs were used to assess differences between groups across all outcomes. Multivariable linear regression (clustered by pair) was used to examine whether the ACLR group had less MVPA than did the age- and sports-matched control group, adjusting for total wear time, age, time since injury, and body mass index.
Results:
Median age was 17.8 years (range, 14.6-22.6 years). There was no significant difference between groups in MVPA. However, the injury group had fewer mean minutes per day of vigorous PA (–1.22; 95% CI, −2.40 to −0.04), poorer KOOS values on all subscales, and shorter triple single-leg hop distance. In the injury group, 28 (55%) returned to sports, including 14 (27.5%) who returned at preinjury performance level. Across both groups, over one-third changed their most important sport, shifting toward an individual-based sport.
Conclusion:
At 1 to 2 years after ACLR, female athletes demonstrated no differences in combined MVPA and only a very small reduction in vigorous PA, yet they had higher levels of self-reported knee pain and symptoms, reduced knee function in sports, lower quality of life, and poorer objective knee function compared with matched controls.
Participation in regular physical activity (PA) is a key modifiable risk factor for the prevention of chronic disease, disability, and mortality worldwide. 50 In youth, PA is instrumental in stimulating cardiac health, bone and musculoskeletal development, and psychological well-being.24,33 Sports are a primary source of PA engagement for youth. However, sports-related injuries are the leading type of injury in this population, 15 and evidence suggests that injury rates are rising. 29 The knee is among the most commonly injured joints, with anterior cruciate ligament (ACL) rupture beingone of the most devastating knee injuries for a young athlete.22,28 The potential long-term consequences of ACL rupture include recurrent injury and early-onset osteoarthritis, 7 which affects younger adults with a history of injury and is characterized by chronic pain and disability. 6
Return to sports (RTS) is often cited as a key goal by injured athletes 19 and is considered a marker of successful injury recovery by clinicians and researchers. 27 However, just over half of athletes make a return to competitive sports 1 year after ACL reconstruction (ACLR). 2 While an abundance of literature has examined factors that influence RTS after ACLR,1,14 much less is known about PA participation, which includes active transport, occupational demands, and household activities, in addition to sports and recreation participation. 35 Furthermore, RTS or self-reported PA data do not provide an objective measurement of PA amount or intensity to facilitate comparison with PA guidelines. Current Canadian PA guidelines recommend 60 minutes per day of moderate or vigorous PA (MVPA) for children and adolescents (aged 5-17 years) and 150 minutes per week for adults (aged ≥18 years).40,41
The effect of previous ACLR on objectively measured PA has been examined in only a few previous studies conducted by 1 research team.3,26 In the first study, the authors found that college-aged adults with previous ACLR spent less time in objectively measured MVPA than did matched healthy controls without a history of knee injury. 3 In the second study, they found that female participants who had undergone ACLR were less likely to meet PA guidelines than were young male and female participants without ACLR. 26 These findings support the hypothesis that individuals who have sustained an ACL rupture, particularly female patients, would be at risk of less PA in the future.
The current study aims to build on this previous work by examining objectively measured PA in female athletes at a younger age range and at a closer time since surgery compared with the previous studies. The transition from adolescence to adulthood is a critical period for promoting PA. 38 Furthermore, the period of 1 to 2 years after surgery is when many individuals attempt to RTS and may still be in contact with rehabilitation providers, making this an opportunity for intervention if needed.
The primary objective of this study was to determine if female youth and young adults who have had ACLR differ in amount of objectively measured MVPA as compared with healthy matched controls 1 to 2 years after reconstruction. We hypothesized that female youth and young adults who have had ACLR in the previous 1 to 2 years would have less MVPA than would healthy matched controls. The secondary objective was to examine differences between groups across a variety of health outcomes including body mass index (BMI), sports participation, patient-reported health outcomes, and physical function. We hypothesized that the ACLR group would report lower levels of sports participation, patient-reported health outcomes, and physical function.
Methods
Study Design
This study involved a cohort of 102 female youth and young adults aged 15 to 23 years: 51 who had undergone ACLR in the previous 1 to 2 years (injury group) and 51 without a previous knee injury (control group), matched by age and previous sports background. Sample size was based on the following: (1) an a priori estimation of being able to detect a clinically meaningful difference in MVPA (7.5 min/d) between matched injury and control groups, which was based on pilot data from 7 days of accelerometer wear in youth and young adults 3 to 10 years after knee injury (n = 14 matched pairs) from the University of Calgary (power = 0.80; α = .05).5,48
Ethical approval was granted by the University of British Columbia’s Behavioural Research Ethics Board (H16-01938). At study entry, all participants completed informed consent or assent (accompanied by parental consent if <16 years of age) and a health screening tool (Physical Activity Readiness Questionniare, revised 2002).
Participants
Injury group inclusion criteria at recruitment included female sex, age between 14 and 23 years, and unilateral primary ACLR for a sports-related knee injury in the previous 1 to 2 years. Participants were excluded if they had a previous ipsilateral or contralateral ACLR. For the control group, inclusion criteria included female sex, age between 14 and 23 years, and no previous sports time loss or medical consultations attributed to a knee injury. Each participant with an injury had a control participant matched by age (date of birth within 1 year) and previous sport (primary sport and competitive level). For both groups, exclusion criteria at the time of recruitment included pregnancy, any musculoskeletal injury sustained in the past 3 months that resulted in missed sports participation, the inability to speak and understand English, or any systemic disease (eg, cancer, heart abnormalities) or neurological disorder (eg, head injury, cerebral palsy).
Participants with previous ACLR were recruited from 11 orthopaedic surgeons in the Greater Vancouver region as well as through study information distributed by collaborators (Figure 1). Potential participants were identified from surgical reports within their medical records by medical office assistants at their clinics and mailed an invitation letter. Within 2 weeks, follow-up telephone calls were made to inquire if the letter was received and to confirm interest. To recruit controls, each participant with an injury suggested a teammate from her previous sports team at the time of knee injury. When this was not possible, a matched control was recruited through distribution of study information by collaborators.
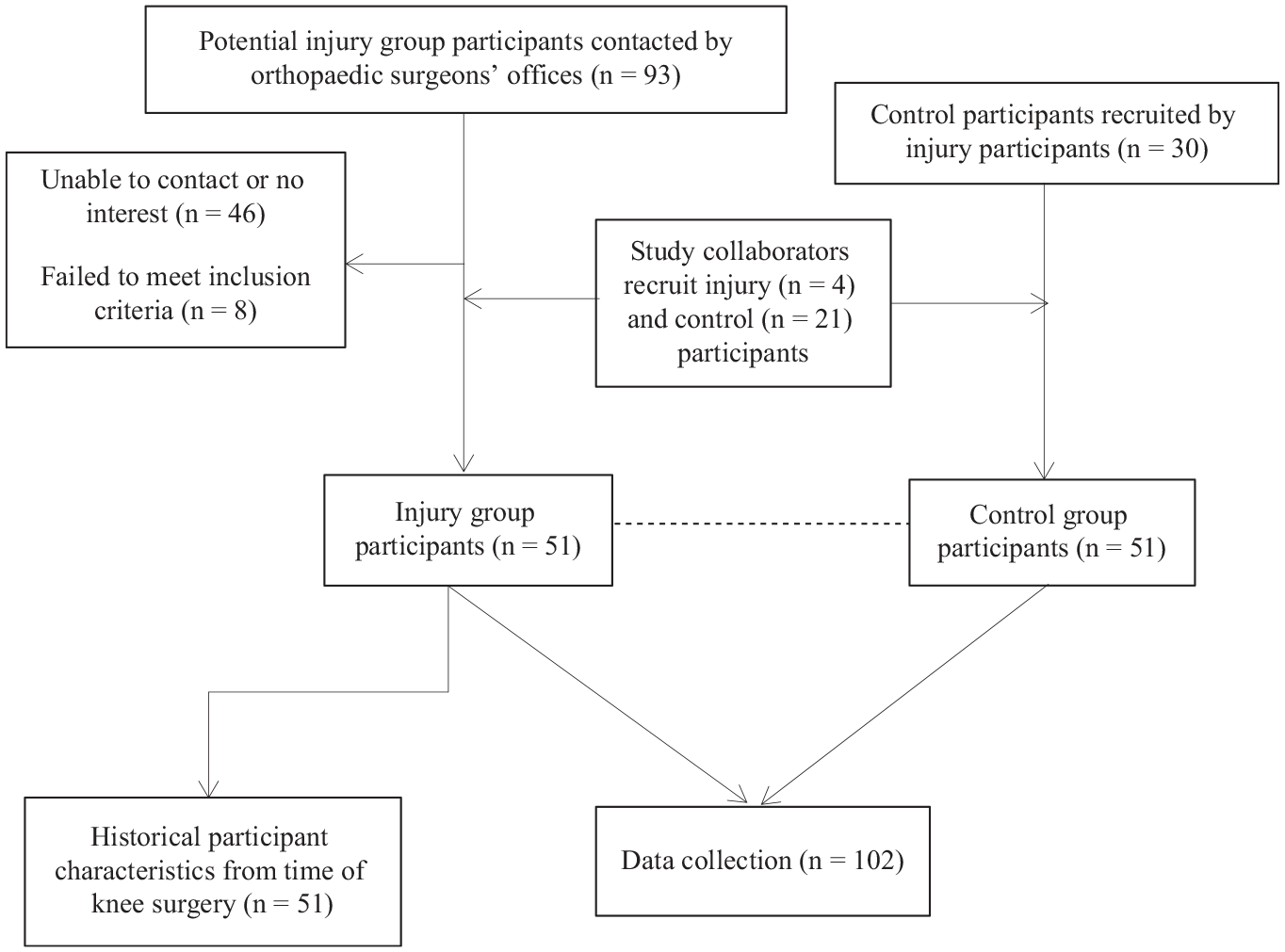
Participant recruitment and data collection.
Data Collection
After informed consent and enrollment, available ACLR information from the time of surgery was obtained from medical records (eg, age, time from injury to surgery, surgical details, anthropometrics [height, weight]). All data were collected at a single in-person session, with the exception of accelerometry. Data collection included the following:
Study-specific questions: participant characteristics, injury details, past and present PA participation, RTS details
Anthropometric measurements: height (in centimeters) and weight (in kilograms)
Patient-reported health outcomes: Tegner activity level, 36 Knee injury and Osteoarthritis Outcome Score (KOOS), 34 Knee Self-Efficacy Scale (K-SES), 18 Anterior Cruciate Ligament–Return to Sport After Injury (ACL-RSI) scale, 45 Tampa Scale for Kinesiophobia (TSK-11) 49
Physical function tests: triple single-leg hop (TSLH) 31 and 1-leg rise (OLR) 39
At the end of the session, participants were given an accelerometer to wear for 13 consecutive days, after which it was returned to the investigators by mail or picked up in person.
Accelerometry: PA Outcomes
Participants were fitted with a triaxial accelerometer (GT3X; Actigraph) on the right anterior superior illiac spine using an elastic belt at the level of the illac crest. Accelerometers are recognized as the gold standard for measuring PA in field settings 16 and have been used in young active populations. 3 The accelerometer did not share any information with participants that could influence their PA. Participants were instructed to wear the device under clothing during all waking hours for 13 days. A valid day required a minimum of 10 hours of wear time.30,42 To be included in multivariable analyses, participants needed to have a minimum of 4 valid days, including 1 weekend day, as this was the same criteria applied in most recent Canadian population-based accelerometry studies of adults and youth.11,12
A number of strategies were employed to promote accelerometer adherence. Participants received a logbook to record accelerometer wear time and nonwear time (ie, swimming, bathing, or sleeping) to stimulate self-monitoring. 44 Written instructions, reminders, and a tip sheet were included in the logbook. Participants had the option to receive automatic text message reminders at individually specified times over the wear period, a strategy previously found to increase wear time in adolescents. 4 At the data collection session, an example of accelerometry data output was shown to participants as another tactic to promote greater accountability. 44
The accelerometer was preset to filter nonhuman motions, with recording restricted between 0.25 and 2.5 Hz. Data were collected in raw acquisition mode and subsequently processed and analyzed using ActiLife software, the proprietary software associated with Actigraph accelerometers. Monitor nonwear time and total wear time were estimated and validated using recommendations of Choi et al, 10 and the digitalized acceleration signal was converted into 1-minute epochs with an activity count for each epoch.
During data reduction, PA was classified into minutes of light, moderate, and vigorious PA based on validated cut points (light, 100-2019 counts; moderate, 2020-5998 counts; vigorous, ≥5999 counts). 42 A sensitivity analysis was conducted by repeating the primary analysis using different validated youth cut points (light, 101-2295 counts; moderate, 2296-4011 counts; vigorous, ≥4012 counts) for participants who were <18 years of age.17,43
PA outcomes obtained from the accelerometers included mean minutes per day of light PA, moderate PA, vigorious PA, and MVPA. Meeting Canadian PA guidelines was examined, and participants were assigned to groups dichotomized as yes (meeting the guidelines) or no (not meeting the guidelines). To calculate weekly PA, the mean number of minutes per day for each participant was multiplied by 7 to account for the varied number of valid days among participants.
Anthropometric Measurements
Anthropometric measurements were assessed to calculate BMI using a medical scale (model 869; seca) with weight recorded to the nearest 0.1 kg and a stadiometer (model 217; seca) with height recorded to the nearest 0.1 cm. BMI was examined as continuous and categorical variables. For participants between 14 and 19 years of age, BMI was converted into age- and sex-specific percentiles using US reference data: underweight (<5.0th percentile), normal weight (5.0th-85th percentile), overweight (≥85th percentile), and obese (≥95th percentile). 9 Participants ≥20 years old were classified by accepted adult standards: underweight (BMI <18.5), healthy weight (18.5-24.9), overweight (25.0-29.9), and obese (≥30.0). 23
Patient-Reported Health Outcomes
All study participants completed the Tegner Activity Scale 36 and KOOS. 34 Only the injury group completed the ACL-RSI, 45 K-SES, 18 and TSK-11. 49 Details on the psychometric properties of these outcomes are available in Appendix 1 (available in the online version of this article).
Physical Function Tests
Each participant completed the TSLH 31 and OLR. 39 A description of the procedures for these tests is in Appendix 2 (available online).
Statistical Analysis
Descriptive statistics were summarized by group and reported as frequency (percentage) and mean (SD) or median (range), as appropriate by data distribution. Available participant characteristics were summarized for the injury group.All continuous variables were examined for normality (Shapiro-Wilk test) and homogeneity of variance when necessary. In the case of missing data, the participant and matched control were removed from that specific analysis. The median (range) and mean within-pair differences (95% CI) were calculated for the following outcomes: light PA, moderate PA, vigorous PA, MVPA, KOOS (5 subscales), TSLH, and OLR. The minimal clinically important difference for the KOOS was considered as follows: Pain, 6; Symptoms, 5 to 8.5; function in Activities of Daily Living, 7 to 8; function in Sport/Recreation, 5.8 to 12; knee-related Quality of Life, 7 to 7.2. 34
The assumptions for linear regression were evaluated through examination of residual plots and Q-Q plot: Y values are independent and a linear function of X; homoscedasticity indicates constant variance; and for a given x, y/errors are normally distributed. A multivariable linear regression (95% CI) was done, accounting for clustering by pair; assessing the association of previous knee injury (exposure) with MVPA (outcome); and including coefficients for age, total wear time, time since injury, and BMI. The value for time since injury for control participants was considered the same as that for the matched participants, reflecting an equivalent knee injury–free period. Regression analyses began with the full model. Using a backward stepwise elimination approach, each variable was individually removed from the model to see its effect as a potential confounder between the primary exposure variable and the outcome. Collinearity was checked for all continuous variables. An interaction term between BMI and group (injury or control) was examined. The most parsimonious model was kept as the final model. As a sensitivity analysis, a multivariable linear regression analysis between injury group and MVPA (with BMI as a covariate) was repeated including only injured participants (and their matches) who had also sustained concurrent meniscal injury (n = 24 matched pairs).
For the secondary objective, in a similar model-building strategy to that just described, separate multivariable linear regression models (adjusted for clustering by pair) were used to assess the association between group (injury or control) and each of the following outcomes: BMI, TSLH, and OLR, with covariates as appropriate (eg, time since injury, age). To adjust for multiple comparisons, a significance level of .01 was used (alpha = .05/5). All statistical analyses were performed using SAS Version 9.4 (SAS Institute).
Results
Participant recruitment is outlined in Figure 1. Participant characteristics at entry into the cohort are summarized by group (injury or control) in Table 1. Median age of participants was 17.8 years, varying from 14.6 to 22.6 years. In addition to ACL rupture, 24 (47.1%) participants in the injury group sustained concurrent meniscal tears. Nearly two-thirds of ACL ruptures were described as noncontact. At data collection, it had been a median 1.7 years (range, 1.1-7.3) and 1.1 years (range, 1.0-2.0) since injury and surgery, respectively, for participants in the injury group. All participants in the injury group attended physical therapy after knee surgery, although the duration and number of treatments varied considerably.
Participant Characteristics at Baseline Recruitment Into Cohort a (N = 102)
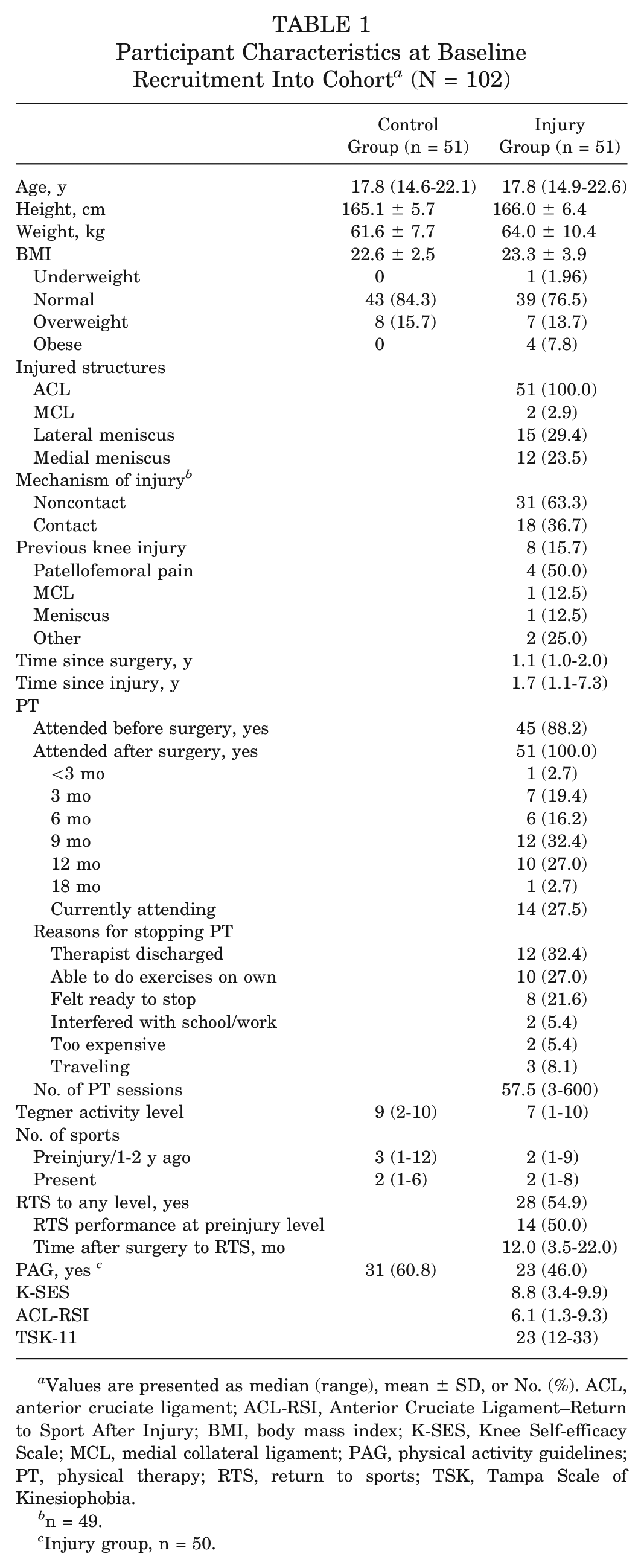
Values are presented as median (range), mean ± SD, or No. (%). ACL, anterior cruciate ligament; ACL-RSI, Anterior Cruciate Ligament–Return to Sport After Injury; BMI, body mass index; K-SES, Knee Self-efficacy Scale; MCL, medial collateral ligament; PAG, physical activity guidelines; PT, physical therapy; RTS, return to sports; TSK, Tampa Scale of Kinesiophobia.
n = 49.
Injury group, n = 50.
Available participant characteristics from the time of ACLR are presented in Table 2 for the injury group. Participants had a median age at the time of surgery of 16.9 years (range, 13.4-21.6) and a mean BMI of 21.7 (SD, 3.2).
Available Participant Characteristics From Time of Anterior Cruciate Ligament Reconstruction (n = 51)
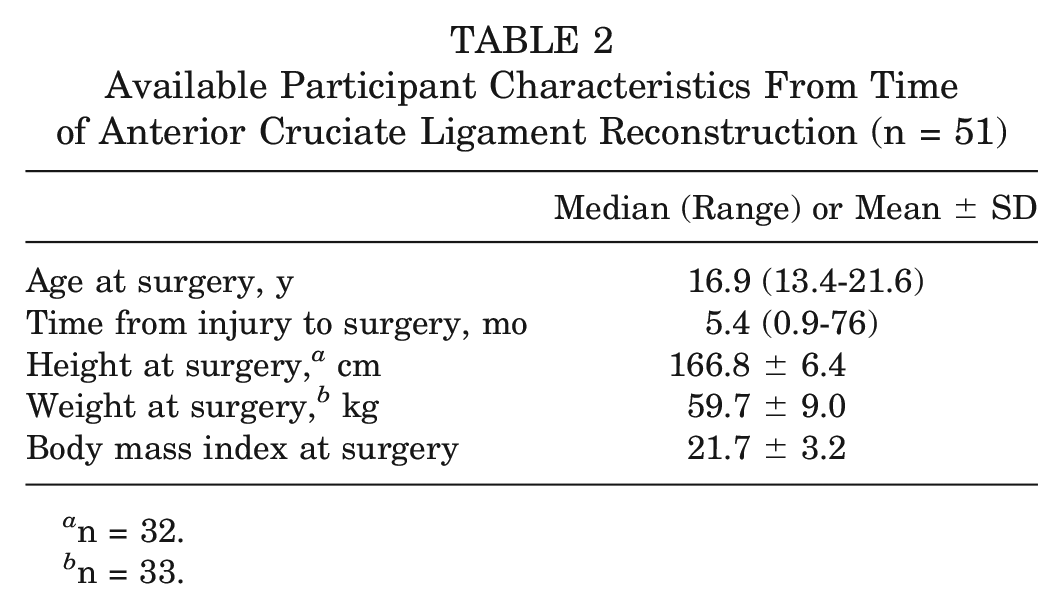
n = 32.
n = 33.
Participants reported being previously engaged in a variety of sports for a minimum 1 hour per week (before ACL rupture/1-2 years earlier), with the most frequent being soccer, basketball, and volleyball. Present-day sports participation had changed for both groups, with 48% and 25% decreases in the number of participants who played soccer in the injury and control groups, respectively. Among those in the injury group, 54.9% reported a different “most important sport” from preinjury, as opposed to 19.6% of participants in the control group.Furthermore, more participants chose to engage in individual sports, such as strength training (increased >3-fold in the injury group) and aerobic exercise at the fitness center (nearly doubled for the control group). Figure 2 summarizes team and individual sports played at both time points by group (before ACL rupture/1-2 years earlier). Additional sports participation details are available in Appendix 3 (available online).
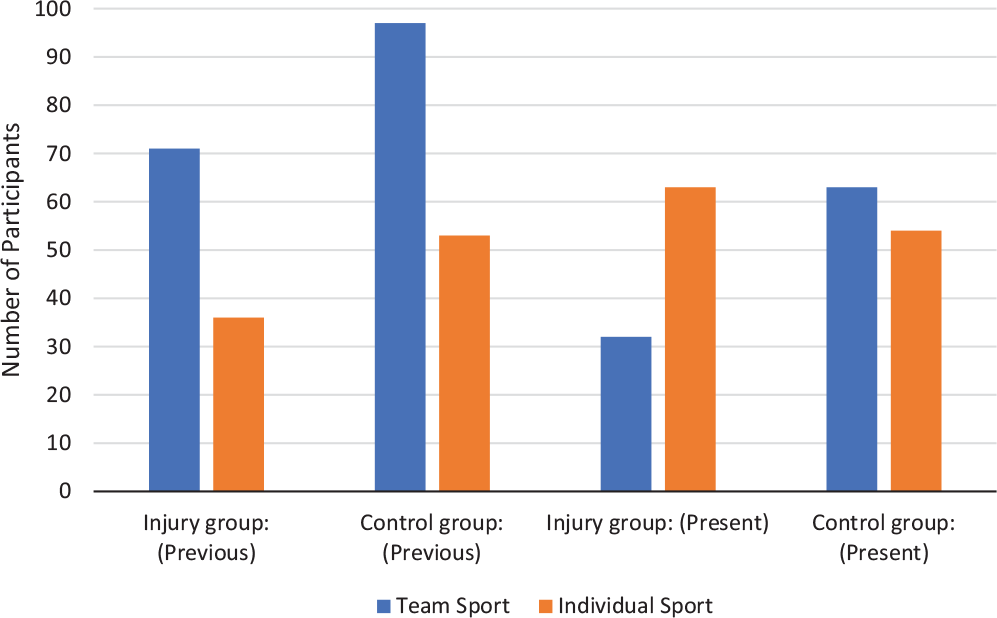
The number of team and individual sports for both groups: previous (injury group, preinjury; control group, 1-2 years earlier) and present day.
The median Tegner activity level was 9 (range, 2-10) for the control group and 7 (range, 1-10) for the injury group.In the injury group, 55% of participants reported that they had returned to sports, and of these, 50% stated that they had returned to the same performance level as before the knee injury and that this took a median 12 months (range, 3.5-22.0). Adult or youth PA guidelines, as appropriate, were met by 60.8% and 46.0% of participants in the control and injury groups, respectively.
Descriptive details and mean within-pair differences for participants’ PA, KOOS, and physical function tests are presented in Table 3. The mean matched-pair difference for mean minutes per day of vigorous PA was significantly lower in the injury group (mean difference, −1.22; 95% CI, −2.40 to −0.04), whereas no difference was found for other PA intensities.
Physical Activity, Patient-Reported Outcome Measures, and Functional Performance Tests by Study Group and Mean Within-Pair Differences a (N = 102)
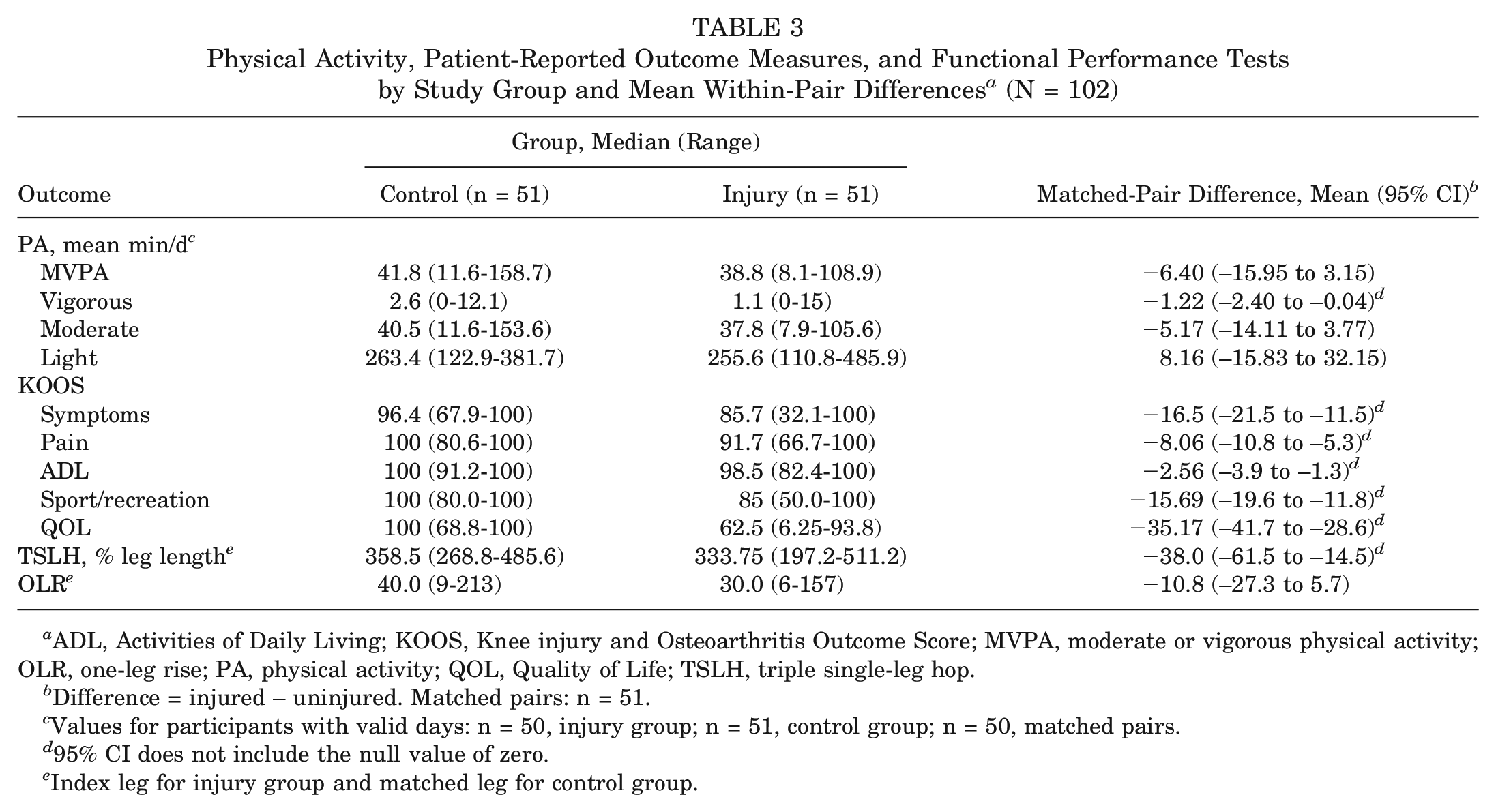
ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MVPA, moderate or vigorous physical activity; OLR, one-leg rise; PA, physical activity; QOL, Quality of Life; TSLH, triple single-leg hop.
Difference = injured – uninjured. Matched pairs: n = 51.
Values for participants with valid days: n = 50, injury group; n = 51, control group; n = 50, matched pairs.
95% CI does not include the null value of zero.
Index leg for injury group and matched leg for control group.
The injury group had significantly poorer KOOS outcomes on all 5 subscales while meeting the minimal clinically important difference for 4 subscales, with the exception of Activities of Daily Living. The injury group also had a significantly lower TSLH distance than did the control group.
Among the 102 participants, 98 (96.1%) met the a priori requirement of a minimum 4 valid days (including 1 weekend day), resulting in 47 matched pairs to include in the multivariable analysis. There was no significant association between group (injury or control) and mean minutes per day of MVPA, while controlling for BMI, total wear time, time since injury, and age (Table 4). Results of the sensitivity analysis examining mean minutes per day of MVPA in the subgroup of participants who sustained a concurrent meniscal injury (and their matched pairs) were not significant (mean matched-pair difference, –8.10; 95% CI, −23.98 to 7.78). Results of the sensitivity analysis that repeated the primary objective with validated youth cut points for MVPA were essentially unchanged from the original analysis (coefficient for injury group, –4.40; 95% CI, −14.18 to 5.38).
Associations Between Previous Knee Injury and MVPA and Other Health-Related Outcomes: Multivariable Linear Regression (n = 51 Matched Pairs) a

Values represent coefficient (95% CI). BMI, body mass index; MVPA, moderate or vigorous physical activity; OLR, one-leg rise; TSI, time since injury; TSLH, triple single-leg hop; TWT, total wear time.
Control group used as reference vs injury.
Matched pairs, n = 47.
Index leg for injury group and matched leg (left or right) for control group.
95% CI does not include zero.
For the secondary objectives, multivariable examination of other health-related outcomes showed that the control group had a significantly better performance on the TSLH than did the injury group while controlling for time since injury (Table 4).
Discussion
This study examined PA and other health outcomes in female youth and young adults, a distinctive group at high risk of knee injury and consequently at elevated risk of poor long-term joint problems (ie, early-onset osteoarthritis). The unique study design with age- and sport-matched control participants facilitated a comparison of health outcomes with peers. The main finding of this study was contrary to the original hypothesis, as we did not find a significant difference in MVPA between female youth and young adults who had ACLR in the previous 1 to 2 years and healthy matched controls. The size of the point estimate for the difference in vigorous PA between groups (1.22 minutes) suggests that this is likely not clinically relevant. However, other important findings from secondary outcomes provide evidence that at 1 to 2 years after ACLR these female patients have noteworthy deficits including more self-reported knee pain and symptoms, lower self-reported knee function in sports, reduced quality of life, and poorer physical function (measured via the TSLH) as compared with their matched uninjured counterparts.
The main finding is in contrast to that of a recent investigation measuring objective MVPA in adults with previous ACLR, which found that they had significantly less MVPA than their matched controls had. 3 However, the mean MVPA performed by these adults was substantially higher across both groups (injury, 78.34 min/d; control, 94.16 min/d) than that in the current study involving female youth and young adults (injury, 38.8 min/d; control, 41.8 min/d). Additionally, the previous study included adults up to 5.5 years since ACLR, much longer than the 1 to 2 years in the current study. Conversely, a recent study involving youth and young adults 3 to 10 years after knee injury did not find a difference in self-reported PA between those with a previous knee injury and matched controls. 47
Given the paucity of studies that have objectively measured PA in this population, these results could be considered encouraging to clinicians and public health professionals by suggesting that female adolescents are remaining as physically active as their peers in the early years after ACLR. In fact, the amount of MVPA found per day in this cohort is comparable with the results from recent population-based accelerometry studies of Canadian children and youth. 11 The Canadian Health Measures Survey reported that girls aged 12 to 17 years averaged 40 minutes (95% CI, 35-45) of MVPA per day. 11 However, Canadian women aged 20 to 39 years reported smaller amounts of MVPA, with an average of 24 min/d. 12
The results of this study highlight the importance of distinguishing between the evaluation of RTS and the broader concept of PA participation. Only 54.9% and 27.5% of injury group participants reported that they had returned to sports and had returned to their previous performance levels, respectively. These numbers are on par with those of previous systematic reviews that have summarized RTS at 1 year after ACLR.2,15 Observed in isolation, these statistics suggest a dire situation for sports participation after ACLR. However, the objectively measured PA results in the current study are in contrast to the negative RTS levels reported by participants and provide evidence that RTS and PA should be treated as separate constructs.
The detailed descriptive data on sports played by participants in the current study suggest that many participants from both groups changed the sports in which they engaged over the previous 2 years, with many shifting from team-based sports (eg, soccer) to more individually oriented sports (eg, running). This behavior directly supports the theory that many youth and young adults change sports owing to available sports opportunities and evolving interests as they progress through teenage years regardless of injuries.37,38 Aligned with the current study is the finding that PA that can be performed outside of a structured context, such as jogging, cycling, and skiing, is more likely to be tracked from youth to adulthood. 25 An overemphasis on RTS, especially the same sports and at the same competitive level, may distract clinicians from encouraging overall healthy PA participation. This is even more critical to consider when a young individual is considering returning to a pivoting sport, where there is an increased risk of recurrent injury, 46 such as meniscal or chondral damage, which could then accelerate development of osteoarthritis. 32
Despite the positive findings regarding PA, the KOOS results from the participants in the injury group suggest far-from-optimal health, with 4 of the 5 subscales meeting minimal clinically important difference for lower scores as compared with results from the control group.The control group’s KOOS outcomes were similar to norms for young active individuals. 8 If the injury group participants are experiencing pain and other symptoms, this could have a negative influence on their PA in the years to come. The poorer quality of life found in the current study aligns with a systematic review that found reduced quality of life, as measured using the KOOS, in individuals >5 years after ACLR as compared with population norms. 20 Poorer quality of life was associated with revision surgery, meniscal injury, and severe osteoarthritis. Future studies are needed to investigate how these self-reported outcomes may influence PA behaviors in the coming years.
The current study has a number of strengths. Few studies have examined objectively measured PA after knee injury, with none focusing on female youth and young adults at this critical period of 1 to 2 years after reconstruction. Accelerometry measures all domains of PA and facilitates a more accurate and comprehensive understanding of PA than does self-reported PA, which is subject to reporting and recall bias. This study had exceptionally high accelerometer adherence, with a mean of 15 hours of daily wear time and with 96.1% of participants providing >4 days of valid data. Height and weight were objectively measured to facilitate the most accurate BMI calculation.
There are also some important limitations to consider when interpreting the results from this study. Our sample size calculation was based on pilot data from 14 matched pairs from a similar cohort, although the current study had larger variability in PA participation. Consequently, it may have been underpowered to detect a true difference in MVPA; however, given the novel aspects of the study design and outcomes, this preliminary study provides a suitable foundation for future work. Furthermore, despite best efforts to recruit an unbiased representative sample of participants, those who chose to participate may have been higher functioning and more physically active compared with those who chose not to participate. However, selection bias was minimized by recruiting participants directly from multiple orthopaedic surgeon offices. The use of wearable devices in this study could have caused participants to modify their usual PA (Hawthorne effect), although limitation extends to both groups. Noteworthy, the device that we used did not provide any information about their activities. The lead author (A.M.E.) did communicate to participants that we were looking to examine their usual PA participation and that it was not a competition between groups. Measurement bias attributed to nonblinding of the assessor to the study group (injury or control) may have occurred during the measurement of height and weight as well as with the evaluation of physical function tests. Given the scope and resources available for this study as part of a doctoral dissertation, it was not feasible to have blinded assessors. This potential bias was minimized by using a calibrated medical scale and taking multiple measurements for physical tests. Some of the patient-reported health outcomes applied in this study have not been formerly validated in youth—namely, the TSK-11 49 and OLR. 39 However, the KOOS, 34 TSLH, 31 ACL-RSI, 45 and K-SES 18 have been extensively used in this age group.There are many external factors that could influence PA after ACLR in adolescent female patients. While this study focused largely on intrapersonal factors, future work may be done to consider how broader influences, such as school or work environment or sociocultural environment (eg, program availability, social norms), affect individuals with a history of ACLR. Last, the generalizability of study results should be limited to female youth and young adults after ACLR and not considered representative of all individuals with previous knee injury. Importantly, female youth represent a distinctive subgroup that warrants this unique examination given their elevated risk of knee injuries 21 and osteoarthritis. 13
Clinical Implications
The main results of this study are encouraging in that female youth and young adults who have had ACLR appear to be attaining MVPA in amounts similar to those of their peers 1 to 2 years after surgery. However, they are doing so while reporting significant knee pain and symptoms, lower function in sports and recreation, and reduced quality of life and demonstrating lower physical function than are those who have not had knee injuries. The discrepancy seen between reported RTS and PA participation highlights that clinicians need to expand conversations with patients beyond RTS to discuss goals, interests, and future plans for PA, especially for individuals who express less interest in RTS. Education should include promoting healthy PA to foster long-term joint health.
Conclusion
This study did not find a significant difference in MVPA between female youth and young adults in the 1 to 2 years after ACLR and their matched uninjured peers. However, they did have deficits across self-reported health outcomes, including pain, symptoms, and quality of life as well as reduced physical function. The current results should be interpreted with caution, given the small sample size, and the study should be considered preliminary to inspire further work in this area. In the future, researchers must consider examining a broader range of facilitators for and barriers to PA in female patients after ACLR. PA should also be examined beyond the 1 to 2 years after reconstruction in this subgroup, especially given the presence of poor self-reported health outcomes that have the potential to negatively affect future PA participation if not specially addressed and improved.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211002530 – Supplemental material for Effect of Anterior Cruciate Ligament Rupture on Physical Activity, Sports Participation, Patient-Reported Health Outcomes, and Physical Function in Young Female Athletes
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211002530 for Effect of Anterior Cruciate Ligament Rupture on Physical Activity, Sports Participation, Patient-Reported Health Outcomes, and Physical Function in Young Female Athletes by Allison M. Ezzat, Mariana Brussoni, Louise C. Mâsse and Carolyn A. Emery in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors acknowledge the recruitment efforts of the 11 orthopaedic surgeons who contributed to this study and the use of space and facilities for data collection that was generously provided by Fortius Sport and Health, North Shore Sports Medicine, and West Richmond Community Centre. Last, thanks to the participants themselves for their enthusiasm for the study and for assisting in additional recruitment efforts.
Submitted June 8, 2020; accepted December 18, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.M.E. was funded through the Canadian Child Clinician Scientist Program. M.B. and L.C.M. received salary support from the BC Children’s Hospital Research Institute. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.