
Abstract
There is an increasing awareness that the inclusion of quality of life as an outcome measure is important in ensuring a client-centred and holistic assessment. This review outlines the benefits of quality of life as an outcome measurement in the field of prosthetics. It introduces the key concepts and challenges in the definition and assessment of quality of life post-amputation, including the relative advantages and disadvantages of adopting generic, disease/condition specific, dimension specific and individualized measures of quality of life. In conclusion, the review delineates and recommends issues and guidelines for consideration when undertaking quality of life research and assessment. A co-ordinated approach by practitioners in the field of prosthetics is necessary to ensure the inclusion of quality of life as an outcome measure and to ensure its measurement in a standardized and rigorous manner.
Introduction
In the field of prosthetics, there is an increasing acknowledgement by practitioners, clinicians and therapists of the need to measure the outcomes of their practice (Billock 1996; Hoxie 1996; Otto 2003; Polliack and Moser 1997; Segedy 2005). According to Szabo (2001) the goals of assessing health outcomes are to improve the quality of care, the quality of health, and thus ultimately the quality of life (QoL) of patients. As the aim of providing people with more effective body functioning is central to the fitting of a limb prosthesis most outcomes research is concerned with ensuing physical adjustment (e.g. +Dudgeon et al. 2005; Pezzin et al. 2000). However, function should not be considered in isolation from more general aspects of the person's QoL (Callaghan and Condie 2003). To concentrate solely on physical indicators belies the complexity of the individuals' amputation experience. Indeed Sullivan (2003) states that “the most complete and meaningful assessments of health status are now seen to include the perspective of the patient”. Indeed, a burgeoning literature evidences the influence of psychosocial variables (e.g. coping, social support, body image) on prosthetic rehabilitation and post-amputation adjustment (Desmond and MacLachlan 2006b; Donovan-Hall et al. 2002; Gallagher 2004; Gallagher and MacLachlan 1999, 2000b, 2001, 2004; Hanley et al. 2004; Horgan and MacLachlan 2004; Jensen et al. 2002). Thus, truly capitalizing on the current rate of technological development in prosthetics requires attention not only to the physical and technical factors which play a fundamental role, but also the social and psychological issues facing those ultimately using the technology.
In 1997, Polliack and Moser identified QoL as one of four categories of prosthetic outcomes, in addition to clinical/biomechanical evaluation, patient satisfaction, and resource utilisation. Despite this endorsement and although QoL assessments are now widely applied as clinical research outcome measures, QoL assessments are rarely implemented in routine clinical practice and there is a notable absence of guidance regarding QoL assessment in the field of prosthetics. Indeed, the scope, emphasis, suitability and applicability of the variety of instruments used in QoL assessment generally, remains controversial (Andresen and Meyers 2000). The aims of this review are, therefore, to outline a rationale for routine QoL assessment, to introduce key concepts in the definition and assessment of QoL post-amputation and to describe a variety of issues that should be considered when undertaking QoL research and assessment.
Benefits of QoL as an outcome measurement
QoL measures are not intended to supplant existing outcome measures associated with prosthetic use but rather to supplement them through more holistic assessment of the impact of a prosthesis on the individual's life. Higginson and Carr (2001) outline eight potential contributions of QoL measures in routine clinical practice. They can be used to identify and prioritize problems and issues of clinical relevance; facilitate communication; screen for potential problems as some issues, particularly psychological and social issues, can be overlooked unless specifically asked about; facilitate shared clinical decision making; identify preferences; monitor changes or response to treatment; and train new staff. They can also be used in clinical audit and in clinical governance. Additionally, QoL measures are increasingly included in clinical trials to demonstrate intervention-related changes over time (Cramer 2002). For example, if two prosthetic interventions result in similar functional benefits, a more favourable QoL impact for one intervention could influence the prescription recommendation.
QoL is also important in terms of the recent publication of the World Health Organisation's International Classification of Functioning, Disability and Health (ICF) (2001) which emphasizes the dynamic intersection of environmental factors and individual characteristics in shaping the disability experience. Disability within the ICF serves as an umbrella term for impairments, activity limitations and participation restrictions. ‘Impairment’ refers to disablement at the organ or system level, for example, limb loss (World Health Organization 2001). According to Heinemann (2005) the measurement of activities assesses the degree to which people can independently perform daily tasks like walking upstairs, whereas the measurement of participation assesses the degree to which individuals are socially integrated, productive and involved in the community. QoL is, therefore, considered an outcome measure at the participation level in terms of the person's real life experiences and, as such, can highlight potentially negative effects of an intervention (Liddle and McKenna 2000). For example, intervention at an impairment or activity level may interfere with participation in life activities due to time in therapy and fatigue. Measures at the impairment or activity level may not show such effects, but QoL measures have the potential to do so.
Definition of QoL
Definition of QoL has proven contentious and despite the proliferation in this field there is still no consensual definition or gold standard of measurement. The dominant conceptualization characterises QoL as a multidimensional construct encompassing physical, psychological and social functioning dimensions which are subjectively evaluated (Kuijer and de Ridder 2003). The World Health Organization defines QoL as an individual's perceptions of their position in life, in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is a broad ranging concept affected in a complex way by the person's physical health, psychological state, level of independence, social relationships, their relationship to the salient features of their environment (WHOQOL Group 1993, 1994) and their spiritual, religious and personal beliefs.
Definitional diversity is a major challenge facing QoL research (Rapley 2003). Most definitions acknowledge the multidimensional and subjective nature of QoL, yet neither the number nor variety of dimensions are agreed (Rapley 2003). Lack of consensual definition, and indeed the failure of many researchers to make explicit the QoL definition to which they subscribe, is a major shortcoming of QoL research. Furthermore, the absence of definition renders difficult assessment of the appropriateness of QoL measures implemented, reduces comparability between studies and consequently limits the development of a robust evidence base.
In health care settings it is argued that it is neither practical nor appropriate to assess all that is meant by QoL. Health related quality of life (HRQoL) concerns aspects of a person's life that are associated with illness, accidents and treatments (Guyatt and Jaeschke 1990). Schipper et al. (1996) describe the four main components of the HRQoL construct as (1) physical and occupational functioning, (2) psychological state, (3) social interaction and (4) somatic sensations or symptoms. Although the HRQoL construct potentially reduces confounding variables, producing more focused and reliable measurement, HRQoL may provide an artificially and unnecessarily narrowed perspective. As illustrated by the exemplar domains above, spiritual and economic status are generally not incorporated into HRQoL domains. Yet McGee (2004) reports that the ability to earn a reasonable income, financial demands of health care itself, and ability to live independently in a safe and healthy environment may all be influenced by illness and health interventions and therefore should not be excluded.
Challenges in QoL measurement
Selecting an appropriate measure of QoL
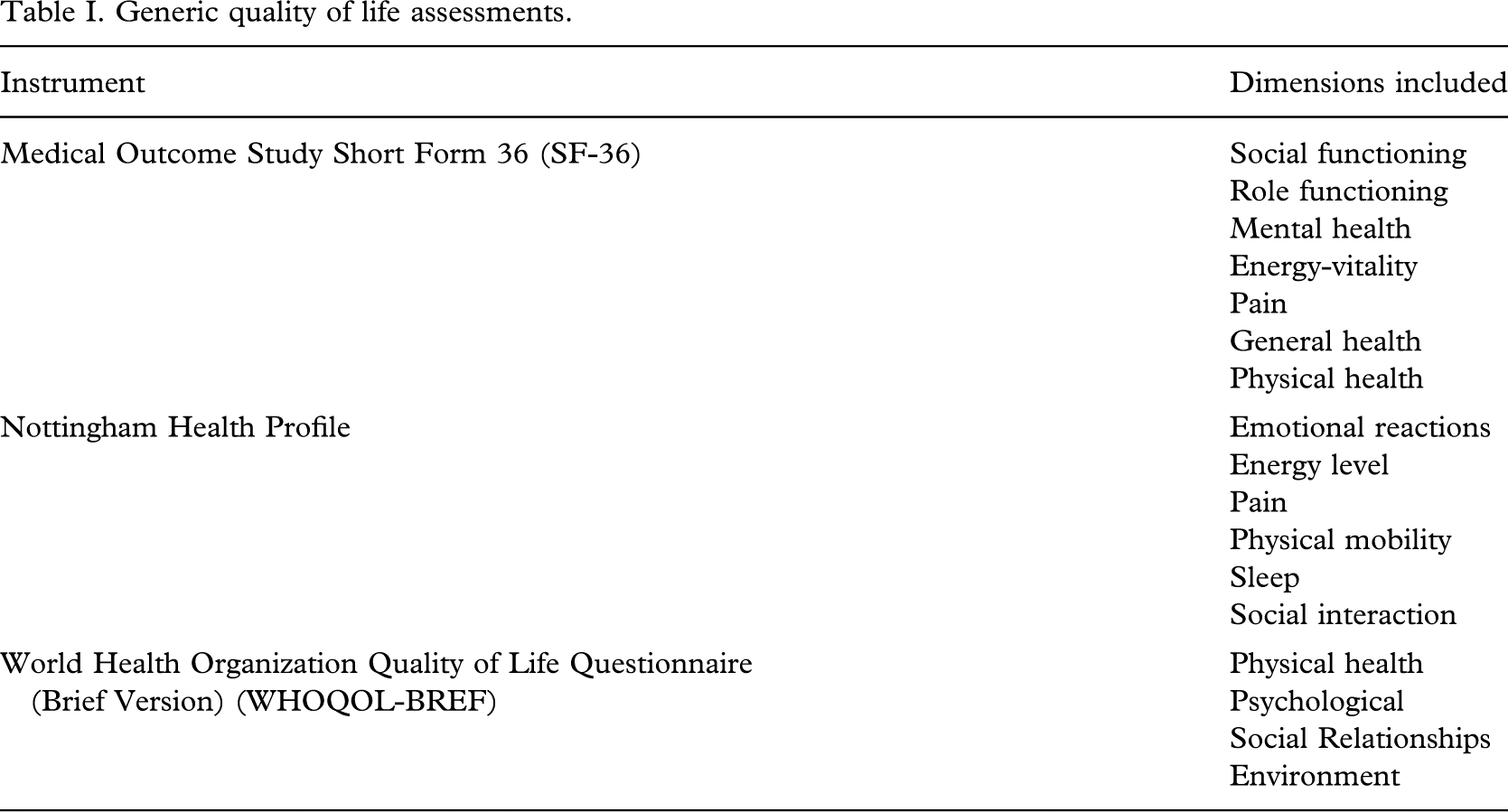
Generic measures of QoL typically assess multiple health domains and can be used in the general population and across different patient populations (Garratt et al. 2002). Designed to be applicable across diseases or conditions and treatments or interventions, generic measures differ in terms of the number and focus of the subscales and items they include (McGee 2004), see Table I. A variety of these assessments have been used in investigations of QoL among people with amputations e.g. the SF-36 (Dougherty 1999, 2003; Hagberg and Branemark 2001), the NHP (Demet et al. 2002; Demet et al. 2003) and the WHOQOL (Gallagher and MacLachlan 2004).
Generic quality of life assessments.
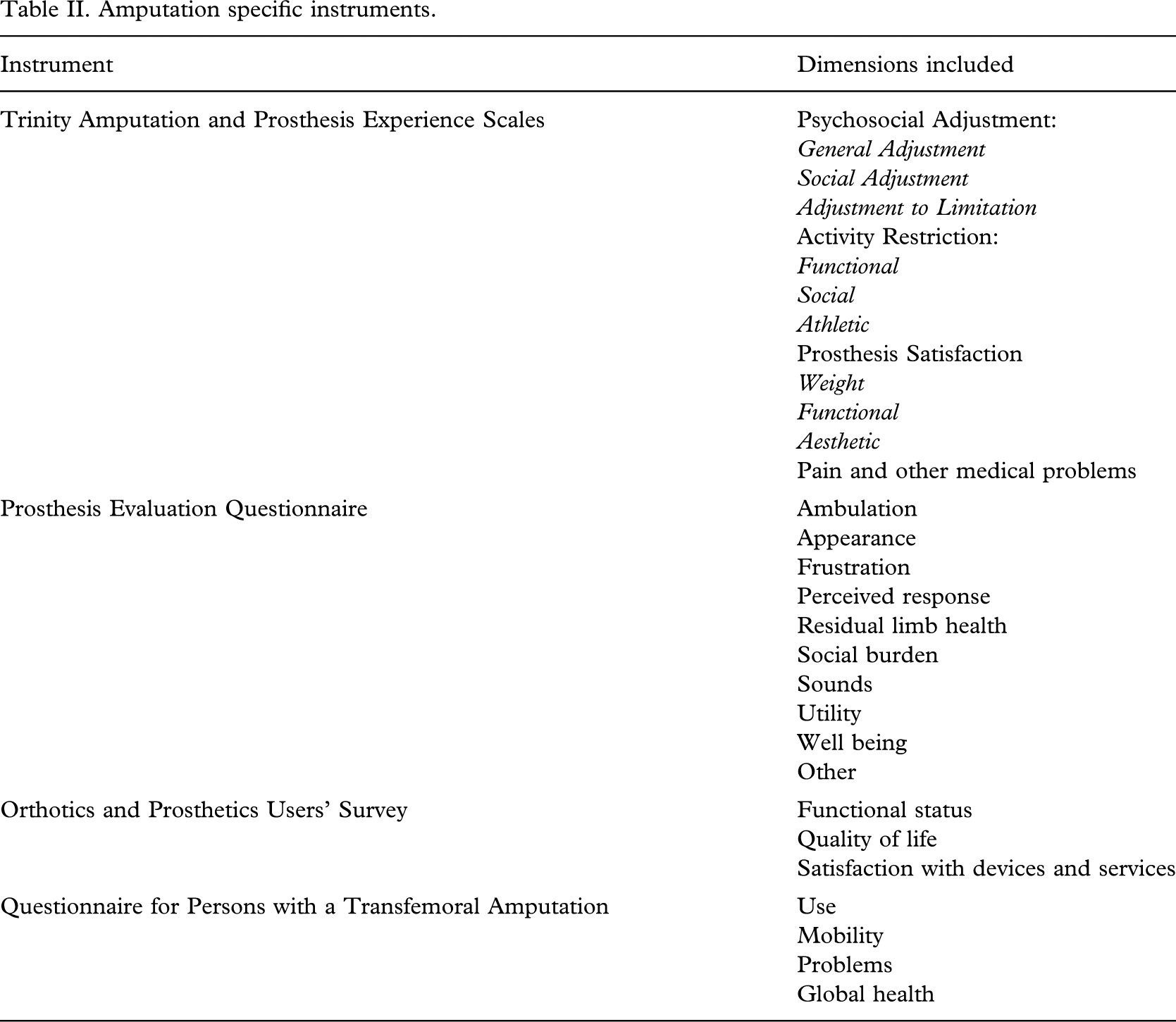
Disease or condition specific measures of QoL include aspects of health that are relevant to particular health problems and may measure several health domains (Garratt et al. 2002). These instruments are intended to be sensitive to change in aspects of life considered most affected by a condition and its treatment. Within the field of prosthetics, condition specific QoL measures include the Prosthesis Evaluation Questionnaire (Legro et al. 1998), Trinity Amputation and Prosthesis Experience Scales (TAPES) (Gallagher and MacLachlan 2000a; Gallagher and MacLachlan 2004), the Orthotics and Prosthetics Users' Survey (OPUS) (Heinemann et al. 2003) and the Questionnaire for Persons with a Transfemoral Amputation (Q-FTA) (Hagberg et al. 2004). Like generic assessments, these instruments differ in their development, focus, structure and psychometric properties (Table II).
Amputation specific instruments.
Dimension specific measures focus on a particular component of QoL such as psychological well-being, pain, vitality, physical function, and cognitive functioning. Arguably, the most widely researched dimensions in the context of amputation are physical functioning (e.g. Davidson 2002; Pohjolainen and Alaranta 1991), pain (e.g. Jensen et al. 2001; Nikolajsen et al. 1997) and affective distress (predominantly depression) (e.g. Desmond and MacLachlan 2006a; Whyte and Niven 2001). Within these dimensions numerous different measures have been used with varying results. For example, symptoms of depression amongst individuals with amputations have been assessed using the Hospital Anxiety and Depression Scale (Zigmond and Snaith 1983), the Centre for Epidemiological Studies Depression Scale (Radloff 1977) and the Beck Depression Inventory (Beck et al. 1988, 1961).
Individualised measures of QoL allow respondents to nominate and weight the importance of aspects of their own lives thus acknowledging the relative and variable nature of QoL across individuals. Examples, include the Schedule for the Evaluation of Individual Quality of Life (SEIQoL) (McGee 1991; O'Boyle et al. 1992), its briefer direct weighting procedure (Hickey et al. 1996), and the Patient Generated Index (Ruta et al. 1994). These individualised assessments are based on Calman's (1984) definition, that is “Quality of life measures the difference, or the gap, at a particular period of time, between the hopes and expectations of the individual and the individual's present experiences”. Individualized instruments address the specified concerns of the individual patient rather than imposing an external, potentially less individually relevant standard through administration of a fixed, predetermined set of questions.
In the SEIQOL, individuals nominate the five aspects of their lives (not necessarily health related) which most contribute to their overall QoL at the time of assessment. McGee (2004) notes that research has shown that health is not always reported as an important aspect of QoL, even in samples with chronic health conditions (Clarke et al. 2001), that the SEIQoL is more sensitive to change than generic or illness-related measures (O'Boyle et al. 1992) and that QoL, using an individualized measure such as the SEIQoL, can remain high in patients in palliative care settings (Waldron et al. 1999). Unlike the SEIQoL, the PGI (Ruta et al. 1994) was developed to measure HRQoL. The PGI acts as an individualized disease-specific outcome measure when used with the inclusion of the sentence ‘think of the different areas in your life, or activities in your life that have been affected by your condition’, in the instructions. The PGI has been used with individuals with lower limb amputations (see Callaghan and Condie (2003) for additional information).
Utility measures were primarily developed for economic purposes and consequently are of less relevance in the clinical practice. Their aim is to assess the value of health or other interventions in terms of a combination of increased QoL and length of life (McGee 2004). The assumptions underlying utility measures, as outlined by Koch (2000), include the fact that: life quality is based solely on the presence or absence of physical conditions deviating from those of the normal population; future life quality does not incorporate the potential role of social values or context but relies only on the person's current physical condition; a person with a physical disability cannot have a positive QoL. Criticisms of oversimplification, inherent discrimination against older people and people with disabilities, and the questionable validity of utility measures spurred the development of alternative QoL assessments (Liddle and McKenna 2000).
Generic versus condition-specific measures of QoL
According to Cella and Nowinski (2002) both generic and condition-specific measures of QoL play a role in QoL assessment with appropriate choice of measures dependent on consideration of the relative advantages and disadvantages of each in the context of the purpose of the study. The broad applicability of generic QoL questionnaires allows comparisons across different diseases and conditions and across interventions and also with ‘healthy’ people. Generic instruments capture a wide range of QoL domains. However, in doing so, some of the detail can be lost. Cramer (2002) notes that generic instruments are developed for general populations and do not focus specifically on the impact of a particular disease or condition, and are thus less likely to detect and respond to small but clinically important changes over time or related to interventions. Conversely, because of their specificity and the provision of finer and more precise detail, condition-specific QoL measures cannot include elements of the broader QoL picture, are limited to particular groups of people and cannot be used to compare groups. The main advantage of condition-specific measures is the immediate and overt relevance to both people with the condition and clinicians. Clearly generic and condition-specific measures of QoL are not necessarily mutually exclusive but rather can serve to complement each other.
Individualized versus disease specific measures of QoL
A primary challenge in measuring QoL is upholding its subjectivity and uniqueness to individuals. Stenner et al. (2003) indicate that the more a researcher emphasises subjectivity, together with the fact that this subjectivity is structured by social factors such as class, gender, age and cultural identity, the less meaningful generic or condition-specific measures of QoL become. Carr and Higginson (2001) raise questions about the ability of pre-established measures with pre-selected domains of QoL to be truly patient centred and representative of the individual's QoL. In addition, the importance that individuals attach to each domain of QoL will differ depending on a myriad of variables including the individual's expectations and aspirations, their own belief system, age, gender, education, environment, marital status, etc. (Carr and Higginson 2001). As a result, to truly assess an individual's QoL, it is important that a weighting system is employed. This system of identifying and weighting personally relevant domains of QoL increases the likelihood of the measure being responsive to change because what is being measured is important in the life of the individual (Carr and Higginson 2001).
Individualized measures also offer an opportunity to study ‘Response shift’ (Sprangers and Schwartz 1999); a phenomenon used to explain how individuals who experience periods of continuing difficulty, such as declining health status, fail to evidence a reduction in subjective QoL that would be expected by objective standards (Carver and Scheier 2000). The working definition of response shift is a change in the meaning of one's self-evaluation of a particular construct (McGee 2004), in this case QoL. Sprangers and Schwartz (1999) propose that response shift can take three forms: a change in the respondent's internal standards of measurement (recalibration), a change in the respondent's values (the relative importance of aspects of the variable under consideration), or a redefinition or reconceptualization of the variable (McGee 2004). A combination of these changes may also occur. The use of individualized measures advocate and support the notion that disability does not in and of itself result in diminished QoL (deLateur 1997). Finally, and perhaps most importantly, individualized measures appear relevant and clinically meaningful to both clinicians and patients and as a result can facilitate shared decision-making and goal and priority setting. For these reasons, increasing emphasis is being placed on individualised measures such as the PGI and the SEIQOL.
However, individualized measures are not without limitations. Some people have difficulty understanding the system of direct weighting, thus limiting their use as self completed questionnaires (e.g. Macduff and Russell 1998). Individualized measures are also dependent on respondents volunteering domains of QoL important to them. However, some domains, e.g. related to mood or sexual functioning, may be less likely to be spontaneously volunteered. Additionally, it is assumed that people spontaneously identify multiple domains of QoL and track their progress in these domains, but there is no evidence base for this assumption. Wright (2000) also highlights the possibility that people may have unrealistic expectations of interventions that will need to be accommodated. Furthermore, the interpretation and analysis of data are complex (Carr and Higginson 2001). Indeed, Dijkers (2003) identifies the main disadvantage of individualized measures as burden both on the respondent and administrator.
Assessing QoL measures
QoL is a complex, abstract, and multidimensional concept that is difficult to define and perhaps even more difficult to measure (Rapley 2003). However, the apparent elusiveness of the QoL concept should not detract from its importance or prevent standardized and rigorous measurement. In this concluding section some guidelines are offered for consideration when undertaking QoL assessment.
At the outset a clear statement of the definition of QoL underpinning the research, should be provided. This definition together with information on the sample, outcomes of interest and research aims (e.g. clinical trial, evaluating change in groups with a specific disease or condition etc.) should influence the selection of an appropriate QoL measure(s) assessing domains pertinent to the definition adopted, the sample being researched and the research question. The choice of an appropriate QoL instrument also depends on the characteristics of the target audience (e.g. age, cognitive ability, culture, language, etc.) and the setting in which assessment will take place (e.g. private or open area, noise, etc.). Instrument selection should be informed by comprehensive review of literature and research in the field to identify existing measures appropriately and successfully used previously for similar purposes. Candidate measures should be reviewed in light of the above criteria, but also in terms of their psychometric properties. Psychometric properties essential for QoL measures in clinical practice include the instrument's validity, reliability, responsiveness and interpretability. (For a review of these psychometric properties see Scientific Advisory Committee of the Medical Outcomes Trust (2002)). Arguably, a more co-ordinated effort needs to take place to establish and review the psychometric properties of QoL instruments to be used with people wearing prosthetics.
Meyers and Andresen (2000) highlight the importance of reviewing the time reference period assessed in the instrument. Standard research instruments typically incorporate items requiring respondents to make general statements about their health in the “past six months”, or “past 4 weeks”, or even “past 3 – 6 days” (Meyers and Andresen 2000). While such questions may be meaningful to most respondents, they are arguably less meaningful for those who experience dramatic health status changes over short time periods e.g. relapsing remitting MS or Parkinson's disease. In addition, such questions are problematic as they fail to account for the short-term memory loss or distortion experienced by individuals with TBIs, strokes or mental illness (Meyers and Andresen 2000). Consideration of the time reference periods and the implications for those who experience unstable conditions is a critical element in selecting appropriate assessments. Fitzpatrick (2000) contends that a primary impediment to the use of QoL measures in clinical practice is the lack of intuitive meaning and familiarity provided by the scores derived. For instance, at what point does a problem become severe or what constitutes a meaningful change in QoL scores before and after an intervention? Consequently, when reviewing QoL measures investigate whether data is presented in useful forms that can be incorporated into practice. Finally, the burden, that is, the time, effort and others demands that the QoL measure may impose should be seriously considered (Scientific Advisory Committee of the Medical Outcomes Trust 2002).
Conclusion
Incorporating the patient's perspective is a central component in rehabilitation and assessing QoL is an important aspect of this endeavour. Consideration of the relative advantages and disadvantages of the available QoL measurement options best drives choice of instrument (Cella and Nowinski 2002). A combination of measures may also be appropriate. Overall, a co-ordinated approach by practitioners in the field of prosthetics is necessary to ensure the inclusion of QoL as an outcome measure and to ensure its measurement in a standardized and rigorous manner.