
Abstract
This cross-sectional descriptive study was initiated to investigate the relationship between physical activity and perceived quality of life in a lower-limb amputee population. The objective was to show which aspects of physical activity were most strongly linked to quality-of-life factors in this special patient group. The outcome measurements were two questionnaires: a section of the Trinity Amputation and Prosthetic Experience Scales (TAPES) and the World Health Organization Quality-of-Life Scale (WHOQOL-Bref). The former measures activity restriction and has Athletic, Functional, and Social subscales. The latter includes Physical, Psychological, Social, and Environmental domains, and measures the individual's perception of their quality of life. The two questionnaires were sent by post to 75 male and female participants with either trans-tibial or trans-femoral amputation who were receiving prosthetic care from a Glasgow-based rehabilitation and mobility centre and who met the inclusion criteria. All participants were over 18 years of age (mean age 66 years). In total, 25 participants returned the questionnaires—a response rate of 33%. According to analysis, 8 of the 12 relationships found were statistically significant. There was a very strong correlation between scores on the social elements of each questionnaire. The correlations between scores on the functional and athletic elements of the TAPES questionnaire and scores on the social element of the WHOQOL-Bref questionnaire were less strong. Our findings support the need for greater acknowledgement by healthcare professionals involved in the care of those with amputation about the importance of the patient's social relationships with friends and family. Education about the importance of increasing and maintaining a level of physical activity conducive to health benefits should be implemented within a supportive sociable environment for the patient with lower-limb amputation.
Introduction
Amputation is one of the major causes of permanent disability. In addition, amputation can often be associated with anxiety, isolation, and depression, which may change the social and free-time activities of the person with lower-limb amputation.
The use of physical activity to prevent and treat disease is an ancient concept, yet only recently has scientific evidence become available to support its many benefits. It is known to be important for healthy individuals, as it increases longevity of life and promotes a sense of psychological wellbeing. Equally, those who face physical or psychological challenges, or a combination of these, can benefit from physical activity as advocated by many international health communities (World Health Assembly 2004).
A profile of the lower-limb amputee population
General activity trends in the elderly have shown that an increase in physical activity improves health-related quality of life. What then is the situation for the lower-limb amputee?
Some 82.9% of those with lower-limb amputation in Scotland have lost a limb due to peripheral vascular disease, with 38.6% of this group having undergone amputation due to diabetes (Callaghan et al. 2001). Another important factor is the average age of the lower-limb amputee population; the Scottish amputee population is predominantly elderly, with around 80% of primary amputees over 60 years of age and more than 20% over 80 years of age (Condie et al. 1996). Davies and Datta (2003) reported on those attending a sub-regional English limb centre, where trans-tibial amputation accounted for 50.5% and trans-femoral amputation accounted for 49.5% of the vascular or diabetic cases (87.5% of the total amputee population). These demographics give an indication of the low preoperative activity levels likely in this group, and suggest that postoperative activity levels may also be reduced. Pell et al. (1993) found that physical mobility was the only independent factor that significantly affected quality of life in amputees as measured by the Nottingham Health Profile, when the amputees were compared with their non-disabled counterparts. On the basis of this novel research, one can speculate that creation of preoperative and postoperative personalised activity programmes will ultimately reduce the incidence of amputation by the reduction of metabolic disorders such as diabetes.
This background, and an apparent dearth of publications on the combined participants of physical activity and quality of life, led to the initiation of this study.
The purpose of the study
This aim of this study was to determine the relationship between quality of life and restriction of physical activity in people with lower-limb vascular amputation. Our hypothesis was that the higher the physical-activity level of a person who had undergone vascular amputation, the greater would be their perception of their quality of life.
Methods
A cross-sectional, mixed-methodology study was conducted with a group of lower-limb amputees in 2006. A cross-sectional design was chosen so that information regarding the prevalence of physical activity and scores representing the quality of life of the population could be collected.
Participants
Participants were adult men and women who had unilateral trans-tibial or trans-femoral lower-limb amputation and who were successfully fitted and ambulatory with a prosthesis. The lower age limit was 18 years. There was no upper age limit. Ethical approval was received from both hospital and university committees. Details of suitable possible participants were sourced from hospital notes so that a random selection could be made from this cohort. All attended the West of Scotland Mobility and Rehabilitation Centre, Southern General Hospital Trust, Glasgow, UK, for prosthetic care. In total, 75 participants were selected from those living in five postal-code areas of west-central Scotland. In order to produce a homogenous sample, adult patients who had lost their limb due to peripheral vascular disease (with or without accompanying diabetes) were selected. This was done so that the sample population would have similar physical-stamina levels, based on their previous pre-amputation pathology status. Participants with bilateral amputations were excluded for this reason. Only those who had been discharged for more than 2 years following amputation were selected.
Postal communication was sent to these 75 participants. The communication contained several items: a covering letter (explaining the purpose of the mailing and an invitation to participate); a detailed Participants Information Sheet (that made clear the purpose of the study and how to complete the questionnaires); a consent form; two questionnaires; and a low-value beverage voucher for redemption at the tea bar of their local prosthetic clinic. A prepaid postage envelope was also included for the return of the consent form and questionnaires. A reminder letter was sent to each participant 1 week after the initial mailing in order to encourage return of the questionnaires. Participants were asked to return the completed questionnaires within 3 weeks of receiving the initial correspondence. In order for analysis and compilation of demographic information to occur, each questionnaire was marked with coded identification specific to each participant. This ensured confidentiality throughout. All of the participant demographic and questionnaire response data were coded, input to SPSS® Version 12 software, checked, and analysed.
The measurement tools
In order to measure physical activity, a section was extracted from the Trinity Amputation and Prosthesis Experience Scales (TAPES). The TAPES were originally developed as a multi-dimensional assessment of adaptation to lower-limb amputation and prosthesis use (Gallagher and MacLachlan 2000, 2004). The Activity Restriction section was used, in which limitations of physical activity were distinct. This ensured that a range of possible activities was covered whilst excluding items not relevant. There are three Activity Restriction subscales, with four questions in each subscale. Therefore, 12 questions were answered in total. The questionnaire was short and simple to use, taking no more than 5 min for the participants to complete and for the researchers to score.
The three Activity Restriction subscales were Athletic, Functional, and Social. Some of the 12 items in the Activity Restriction section were based on items from the Short Form 36 (SF-36) Health Survey (Ware et al. 1993). The Athletic Restriction subscale covers activities that involve more dynamic physical effort; for instance, sport and recreation and running for a bus. The Functional Restriction subscale covers rudimentary functional tasks, such as climbing one flight of stairs. The final subscale, Social Restriction, addresses social activities such as visiting friends and working on hobbies. Items on the Activity Restriction subscales are scored on a 3-point scale ranging from 2 (limited a lot) to 0 (not limited at all). Each subscale consists of 4 items and, hence, subscale scores range from a minimum of 0 to a maximum of 8, with higher scores indicative of greater limitation.
Analyses have revealed that the TAPES questionnaire had high internal consistency (alpha-reliability coefficients ranged from 0.72 to 0.94) and good face, construct, content, and predictive validity (Gallagher and MacLachlan 2000, 2004). However, similar analyses have not been carried out on individual subscales of the questionnaire. The questionnaire has been used to measure outcomes in those with both upper-limb and lower-limb amputations (Desmond and MacLachlan 2005).
In order to measure quality of life, the World Health Organization Quality-of-Life Scale (WHOQOL-Bref) self-administration questionnaire was used. The World Health Organization (WHO) defines ‘quality of life’ as an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. The primary importance of this questionnaire is to discover the individual's perceptions. Perception is a broad-ranging concept affected in complex ways by the person's physical health, psychological state, personal beliefs, social relationships, and relationships to salient features of their environment.
The WHOQOL-Bref is a comprehensive research instrument containing 26 items rated on a 5-point Likert scale. A maximum score of 5 indicates a perception of a high quality of life, while a minimum score of 1 indicates a perception of a poor quality of life. Four domains comprise the following items: Physical Health (7 items); Psychological Health (6 items); Social Relationships (3 items); and Environment (8 items). The remaining two items, at the beginning of the questionnaire (coded Q1 and Q2), ask specifically about the participant's rating of their quality of life and satisfaction with their health. Cronbach's alpha values for each of the four domain scores range from 0.66 to 0.84, demonstrating moderate-to-good internal consistency. Test–retest reliabilities range from 0.66 for physical health to 0.87 for environment. In addition, the domains were integral to the assessment of quality of life, indicating good content validity. Because of its brevity, it is ideal for use in large-scale surveys, and in some clinical situations (e.g. palliative care) where use of a longer questionnaire is not practicable (WHOQOL Group 1993, 1998). Both questionnaires are included in Appendices I and II.
Data analysis
Each of the three subscales of the Activity Restriction section of TAPES and each of the four domains of the WHOQOL-Bref instrument were summarised using appropriate descriptive statistics. Summary statistics were calculated (mean, standard deviation, etc.). As a result of the non-normality of several of these scores and the small sample size, the nonparametric correlations between each of the subscales and each of the domains were assessed using Spearman's Rank correlation. The level of significance was set at 0.05 for all tests. All analysis was performed on SPSS® Version 12.
Results
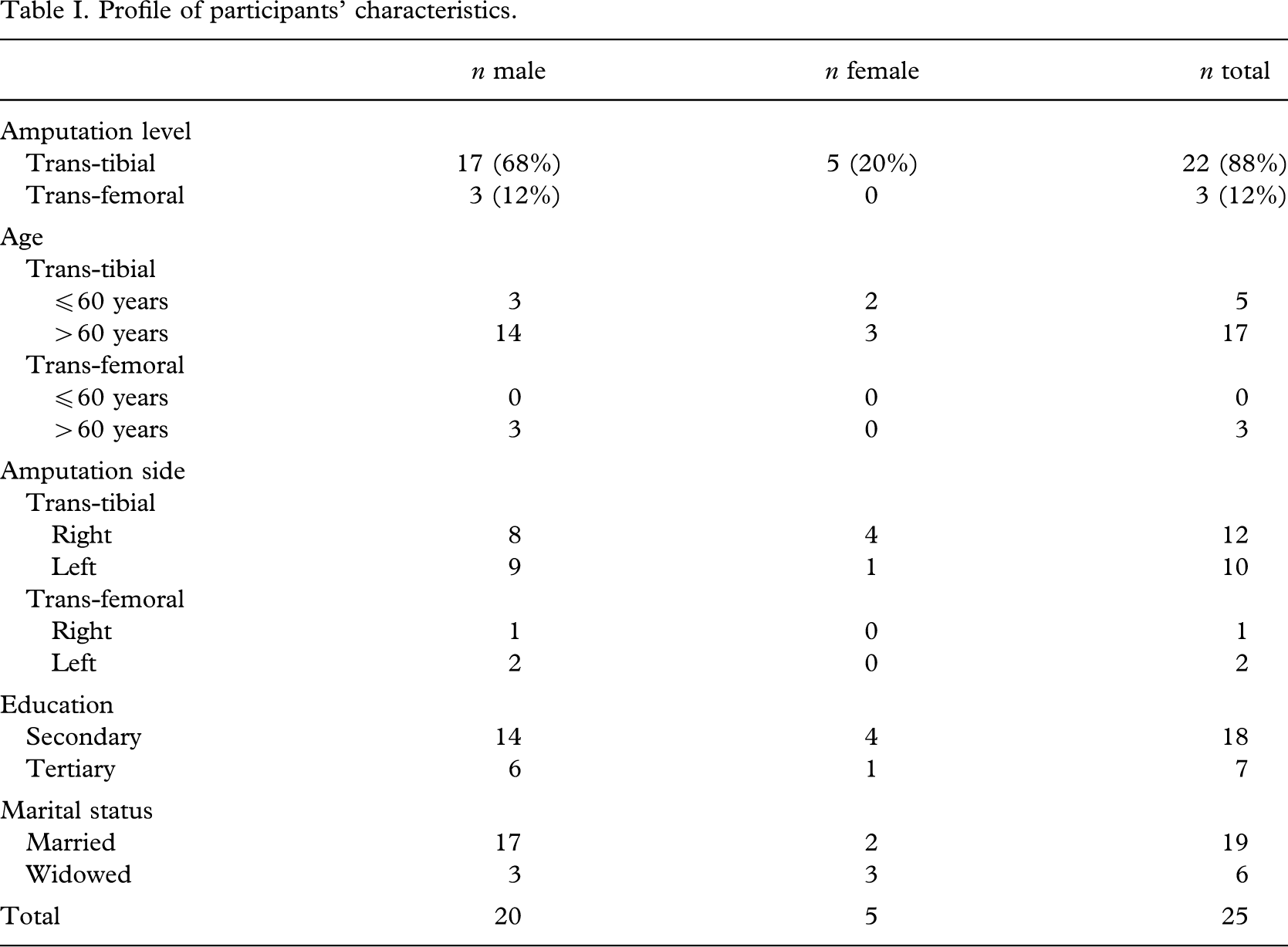
In total, 26 of the 75 invited participants returned the questionnaires. One questionnaire was discarded because of incomplete data. Therefore, 25 of the 75 questionnaires were analysed, the return rate being 33%. Table I details the participants' profiles.
Profile of participants' characteristics.
For the TAPES subscales, the highest mean score was achieved on the Athletic subscale (7.24, SD = 0.88) and the lowest on the Social subscale (3.44, SD = 2.50). For the WHOQOL-Bref, the lowest mean score was achieved in the Physical domain of (56.32, SD = 18.70), and highest in the Environmental domain (72.20, SD = 15.19). Summary statistics are presented in Table II.
Summary statistics for the questionnaire subscales and domains.
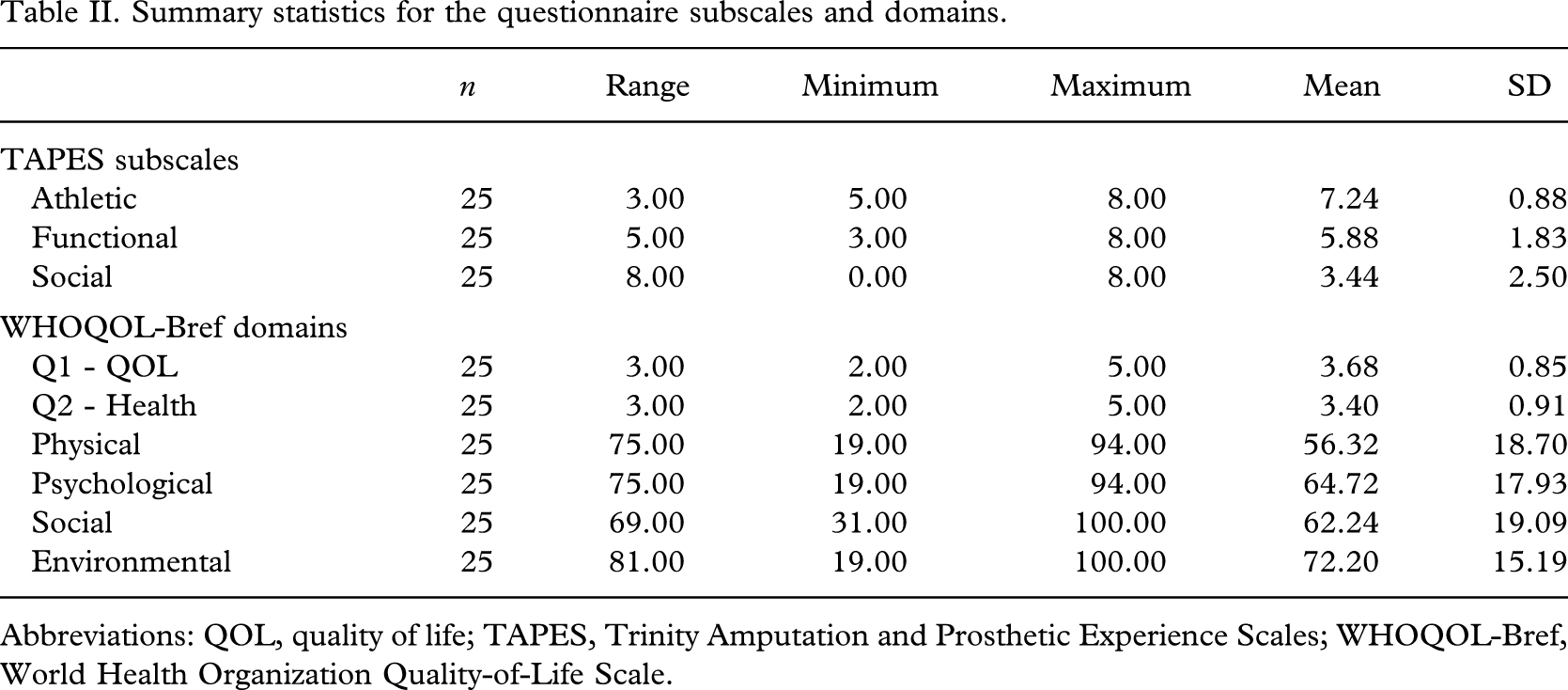
Abbreviations: QOL, quality of life; TAPES, Trinity Amputation and Prosthetic Experience Scales; WHOQOL-Bref, World Health Organization Quality-of-Life Scale.
The relationships between the TAPES subscales and WHOQOL-Bref domains were investigated and all results are shown in Table III. Eight of the 12 relationships were statistically significant. The negative sign on all correlations reflects the fact that a higher score on a TAPES subscale indicates more restriction, and hence less physical activity, whilst a higher score in a WHOQOL-Bref domain indicates a perception of better quality of life. Therefore, a large negative correlation indicates a strong positive relationship between level of physical activity and perceived quality of life. There was a significant relationship between scores in the Physical domain of WHOQOL-Bref and all scores on three subscales of TAPES. There were significant relationships between scores in the Psychological and Social domains of WHOQOL-Bref and scores on the Functional and Social subscales of TAPES, and there was a significant relationship between scores in the Environmental domain of WHOQOL-Bref and scores on the Social subscale of TAPES. Only scores on the Social subscale of TAPES had a relationship with scores in all four WHOQOL-Bref domains. Scores in the Environmental domain of WHOQOL-Bref were significantly related to scores on the Social subscale of TAPES only.
Nonparametric correlations (rs) between scores on questionnaire subscales and domains.
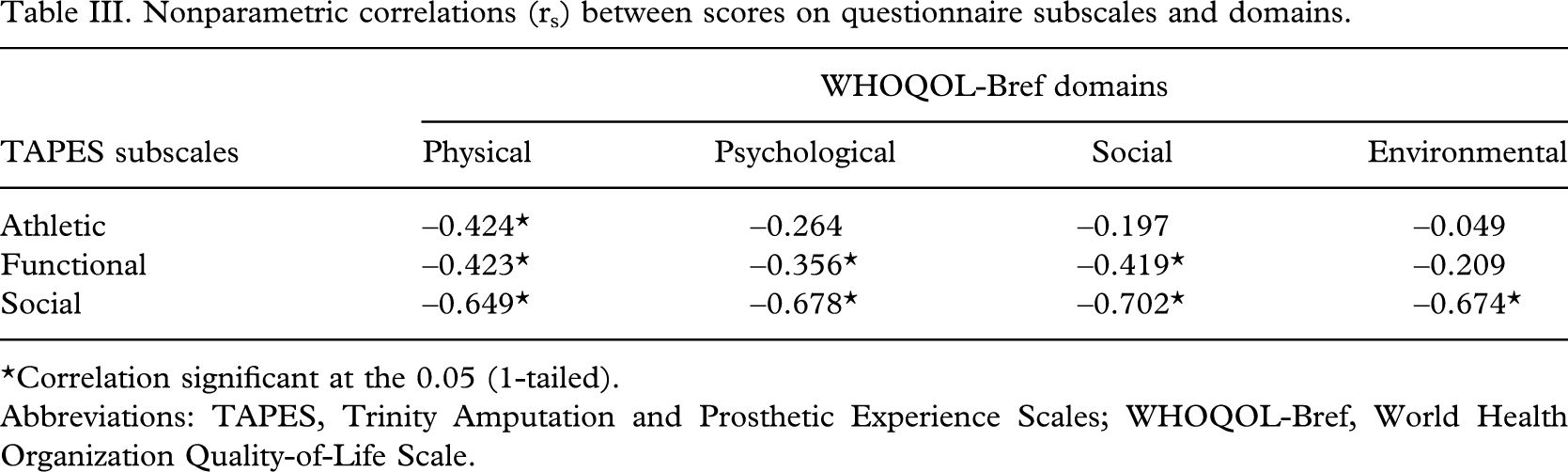
∗Correlation significant at the 0.05 (1-tailed).
Abbreviations: TAPES, Trinity Amputation and Prosthetic Experience Scales; WHOQOL-Bref, World Health Organization Quality-of-Life Scale.
Discussion
This investigation was initiated with the hypothesis that if participant achieved higher scores on the Activity Restriction subscales of TAPES, they would also achieve lower scores in the WHOQOL-Bref domains. There was indeed a statistical correlation between scores on certain TAPES subscales and scores on certain WHOQOL-Bref domains. On the basis of previous research stating the strong relationship between reaching recommended levels of physical activity and the accompanying perception of increased quality of life (Brown et al. 2004; Leinonen et al. 2004), the authors expected a strong correlation between scores on the Athletic and Functional subscales of TAPES and scores in the Physical domain of WHOQOL-Bref. These correlations were found; however, whilst statistically significant, they were weak (Athletic rs = –0.424, p = 0.017; Functional rs = –0.423, p = 0.018). There are clearly other factors in this amputee population, such as gender, age, and amputation level, that influenced the physical outcome.
Interestingly, there was no relationship between scores on the Athletic subscale of TAPES and scores in the Psychological, Social, or Environmental domains of WHOQOL-Bref. This suggests that the participant group failed to acknowledge any participation in functional activity at a high level, thinking more in terms of a level of function based around necessary activities of daily living. Indeed, many of the respondents commented that the athletic items were totally irrelevant to the functional aspects of their lifestyle. For example, being able to carry out vigorous activities like running, lifting heavy objects, or participating in strenuous sports was not considered important. This could be due to their pre-amputation pathology or their age, and one has to ask whether a different questionnaire might elicit more relevant answers in this population group.
Scores on the Social subscale of TAPES showed the strongest relationships with scores in all of the WHOQOL-Bref domains. Predictably, the strongest negative correlation was between scores on the Social subscale of TAPES and scores in the Social domain of WHOQOL-Bref. On the basis of these findings, it is suggested that individuals place higher importance on social standing and friendships with family and friends than on physical ability. It seems that, during the ongoing post-amputation rehabilitation process, accomplishing and maintaining social integration is valued much more highly than being physically active or even personal psychological wellbeing. This is certainly supported by the great success of amputee support groups such as The Murray Foundation (www.murray-foundation.org.uk). This group's creation of a Hospital Visitor Scheme and a Visitor Support Network has proved an invaluable aspect of patients' immediate post-amputation rehabilitation. It is also acknowledged that members of the rehabilitation team try to prepare the amputee patient for the important reintegration into social life as part of their ongoing therapies.
At the core of our findings is the desire of an older, less-active patient group to seek comfort, gain confidence, and maintain social standing by prioritising relationships rather than a level of physical functioning they cannot relate to. As the results of this study showed a weaker-than-expected relationship between physical activity and quality of life, future research could investigate the reasons for this finding. We can offer some possible explanations. The amputee in postoperative rehabilitation does not necessarily always receive one-on-one gait training in an in-patient or out-patient physiotherapy department, and may only receive prosthetic rehabilitation. In group rehabilitation, the amputee can benefit from social interaction, during which they can seek guidance and information from their contemporaries' personal experiences. However, it may also be possible that important physical educational and information dissemination is lost without positive one-on-one reinforcement over several weeks with a therapist. This possibility is supported by the results of a pilot study that evaluated the effect of exercise consultation on promotion of physical activity in people in Scotland with Type II diabetes. By conducting a consultation with the experimental group of participants, and by providing the control group with an informational exercise leaflet, it was shown that “exercise consultation is more effective in stimulating exercise behaviour change in the short term than a standard exercise leaflet currently used to promote physical activity in people with Type II diabetes” (Kirk et al. 2001).
Another issue is the preoperative training of amputee patients. This issue is of vital importance in order for successful rehabilitation after surgery to occur. Improvement in self-esteem can help the patient in the postoperative rehabilitation process, and so preoperative assessment can be regarded as a keystone of the rehabilitation process. Formalised liaison with the prosthetic clinical team that examines as many aspects of care which the patient can expect could be carried out before amputation.
This work clearly differs from similar, worthy studies carried out by the notable Dublin-based authors mentioned previously. Gallagher and MacLachlan (2004) were interested in the aspects of the prosthetic experience that were most strongly associated with quality of life. Their findings support the claim that TAPES can be used to evaluate quality of life. Although we used the same questionnaires, this work specifically extracted the areas of physical activity and quality of life and examined what the person with lower-limb amputation perceived as important. The relationship between physical activity and quality of life was also examined, with the aim of making recommendations for the tailoring of current prosthetic rehabilitation programmes to include more personal physical activity in a group setting. Further work is intended in order to elicit a change in recommended practice.
Both the TAPES and WHOQOL-Bref questionnaires initially seemed ideally suited to the study design, which required the use of postal questionnaires. The instructions were easy to understand, the questions clear and concise, and assistance to complete the questionnaires was not required. Combined, the questionnaires took an average of 13 min to complete by the participants and around the same time for the researchers to score.
The WHOQOL-Bref measurement tool has been used in studies that investigated such diverse conditions as lower back pain (Horng et al. 2005), rheumatoid arthritis (Taylor et al. 2004), and spinal cord injury (Jang et al. 2004) and is clearly adaptable. It was considered important not to use a disease-specific or disability-specific measure so that the value of the concept of normal quality of life was not diminished. This approach has been advocated by Wade (2003) and, as Andresen and Meyers (2000) explain, “most studies using generic HRQOL [health related quality of life] tools are of groups with specific impairments rather than heterogeneous groups of people with disability.”
The number of participants initially selected was reasonable, but the response rate was lower than the authors expected. In some research studies, a response rate of 25% or higher is considered good, while in others it is acknowledged that response rates of over 75% are possible by adopting specific techniques. These include supplying another copy of the questionnaires in the reminder communication or including an enticement on the envelope—for example, a comment suggesting to participants that they may benefit if they open it (Streiner and Norman 1995; Edwards et al. 2003).
Participants with trans-tibial and trans-femoral amputation were invited to participate in order to obtain as large a sample size as possible. Because only 12% of the respondents had the trans-femoral level, this did not influence the results greatly. The assumption was that those with trans-tibial amputation would not have the same physical activity levels as those with trans-fibial amputation. However, it was anticipated that the response rate may be poor and a distribution of physical activity levels was desirable.
The purpose of the study was not to examine comparisons between people with trans-tibial and amputation and those with trans-femoral amputation, but rather selection was made from these two groups in order to increase the sample size of those who shared the aetiology criteria. Comorbidity was not recorded, as the sample was not large enough to take this factor into account statistically as a covariant representation of the sample.
Caution should be taken when extrapolating the results of this study to other populations, since the participants were all recruited from a specific western Scotland locale. Further research could encompass nationwide participant groups in order to achieve more general findings. In addition, a larger sample size could enable examination of the possible effects of gender, age, location etc.
Future research will draw on populations with the same level of amputation and, therefore, similar functional abilities and expectations, and steps will be taken to produce a higher response rate.
Conclusions
This study examined the relationship between physical activity and quality of life in an amputee population. A weaker-than-expected relationship between the two was observed. Healthcare professionals should understand the value the amputee patient places on their relationships with family, friends, and those in their peer group. A social-support network is important to them. This study supports increasing physical activity in this patient group, so long as social interaction is not compromised. Ways of encouraging increased daily physical activity of a kind conducive to health benefits and combining this with peer-group interaction should be investigated. Creating and positively reinforcing awareness within the rehabilitation team about the importance of the amputee patient's reintegration into social networks is paramount and should not be overlooked.
Footnotes
Acknowledgements
Thanks to Mr Brian Callaghan for his helpful comments gratefully received in the preparatory stages of the study, to the prosthetic team of Otto Bock (UK), WestMARC, Southern General Hospital Trust, Glasgow for their invaluable assistance in participant selection for the study, to the participants who were involved, and to Anne Slater for her tireless work on page design and layout of the mailing documentation.
Appendix I. World Health Organization Quality-of-Life Scale (WHOQOL-Bref)
Please keep in mind your standards, hopes, pleasures and concerns. We ask that you think about your life
You should circle the number that best fits how much support you got from others over the last two weeks. So you would circle the number 4 if you got a great deal of support from others as follows.
You would circle number 1 if you did not get any of the support that you needed from others in the last two weeks.
The following questions ask about
The following questions ask about
The following questions ask you to say how
The following question refers to
Did someone help you to fill out this form
How long did it take to fill this form out?