
Abstract
Background: It is important to measure the functional capabilities of a prosthesis in order to make informed decisions when prescribing a limb.
Objectives: To measure the functional of a range of commercial single degree of freedom hands to act as baseline comparisons for the newer multi-axis hands.
Study Design: Form-board and self-timed tasks.
Method: Repeated measures with a single subject using a validated assessment tool. The test measured the function of three conventional, single axis, powered hands, controlled by five different myocontroller formats. One transcarpal device was also tested.
Results: When controlled by the same type of two channel myoelectric controllers (proportional voluntary opening, voluntary closing) the overall functional scores were similar for all similar types of hand, with a maximum score of 94 out of 100. The smaller transcarpel hand had a score of 84. Only when a more limited single channel three state controller was used was the score much lower (81).
Conclusion: All of the hands were of a similar design and were set in a precision grip, but the precision grip did not achieve the highest individual grip score. Additionally, while the Southampton Hand Assessment Procedure (SHAP) score is dependent on the speed of execution of the task, the speed of the prosthesis did not have as great an impact on the score as the other variables.
This study provides comparative data between similar designs of commercial hands. This will allow clinicians to be better informed when they prescribe a device for a user.
Introduction
There is an increasing interest in supporting clinical decisions with evidence of the effectiveness of a prosthesis. 1 – 3 When a clinician wishes to prescribe a hand, they can use their knowledge and experience, but there is a paucity of other reliable sources to assist in this decision. Currently, there are few tools specifically validated to measure the function of a prosthetic hand. 3 – 4
In a systematic approach to development, the designer must understand the requirements of the user and create a specification. They must then be able to measure the resulting design and compare them with the specification. Newer multifunction hands are now being marketed, which have more degrees of freedom and a greater price. So it is important to demonstrate that these increases are warranted. This study is the first stage in a process to address this problem. It aims to measure the function of conventional single degree of freedom myoelectric hands and controllers. This will create a baseline for later studies of the more advanced designs. The hands studied are similar in shape, and it was anticipated that they would all have similar capabilities, separated mostly by the means by which they were controlled.
For this study, the cosmetic qualities of the devices were not studied, only the manipulative function of the hands was measured using the Southampton Hand Assessment Procedure (SHAP). 5
Background to SHAP
SHAP was chosen as it is one of the few assessments which had demonstrated sufficient psychometric merit.3,4 SHAP was designed to assess the function of the hand. It uses a form-board and self-timed tasks, employing abstract objects and simulated activities of daily living (ADLs). The test was designed to be practical, supplying the tester with a number that allows comparison between subjects, over time, and between levels of recovery. 6 It has been shown to have repeatability on normal subjects and some conditions of the hand. 6 – 9 Within the World Health Organization International Classification of Functioning, Disability and Health (WHO-ICF), 10 SHAP assesses factors within the Body functions domain.
The tasks are divided into two sections; abstract objects, to encourage the use of the six standard grips: Tips, Lateral, Tripod, Spherical, Power and Extension, plus 12 ADLs (Figure 1).
11
Each of the grips is given a score based on the difference in time to execute, compared to times recorded by a normal group. The overall score is derived from the individual grip scores with a weighting given to each grasp depending on their relative use in daily activities.
12
The unimpaired population scores above 97.
An example of the SHAP equipment, showing the form-board and one of the simulated activities of daily living (the subject must pour the contents of the carton into the jar). In this example, the right hand is being tested.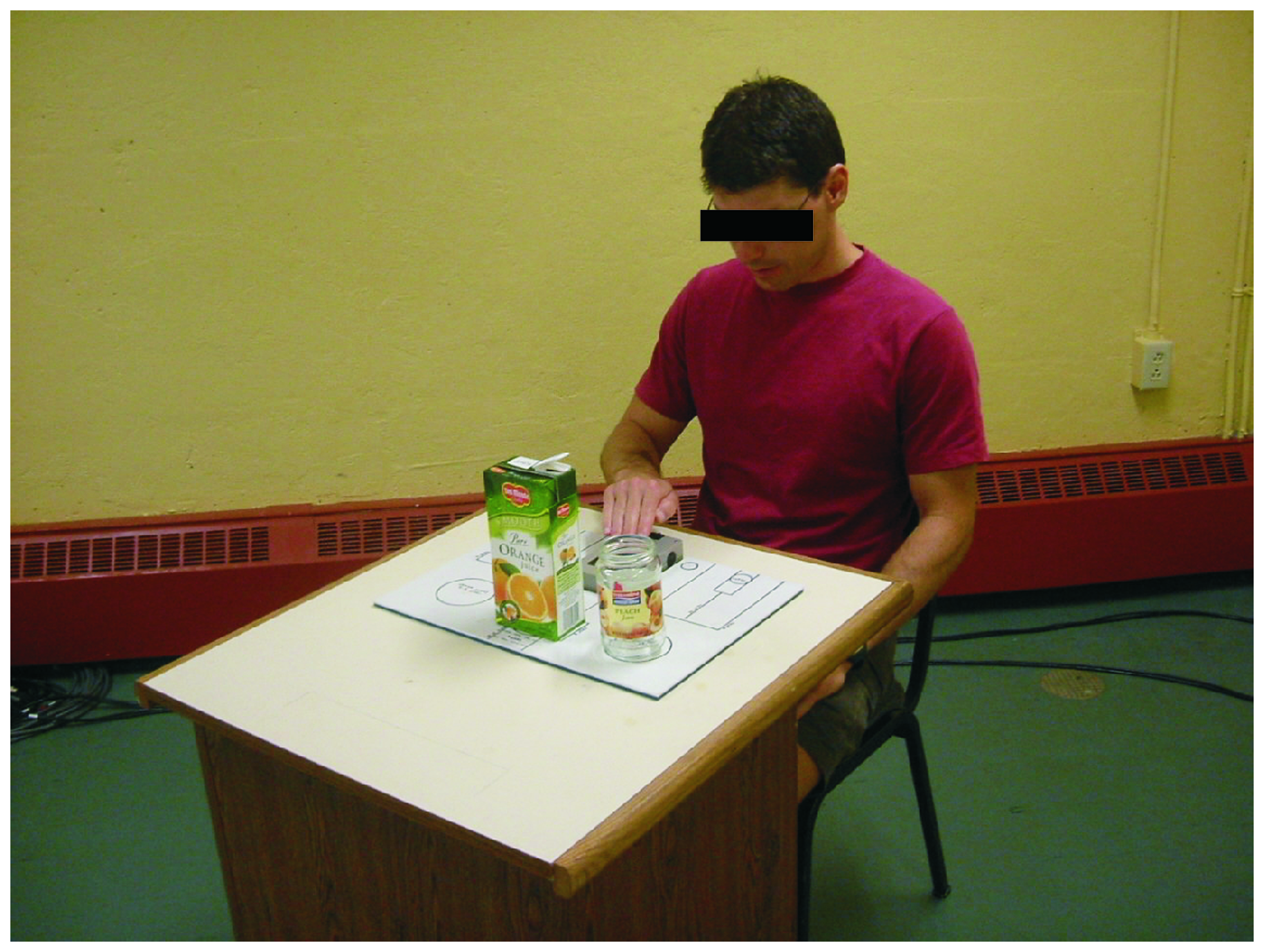
The mechanical design of prosthetic hands
Prosthetic hands are a compromise between many constraints. Pragmatic decisions ensured that the majority of the commercial hands produced before 2005, were very similar in shape. The basic form of the powered prosthetic hand, fitted clinically for the past 50 years, has been a single degree of freedom hand set in one grip (generally tips grip).13,14 While these are widely used, there is little information concerning the designs' functional capabilities. Since 2006 new designs with more degrees of motion have been marketed. While the response to these hands has been positive, it is unknown if the increased complexity has a positive impact on their function. This study is the first stage to attempt to provide evidence in this process. Examples of the simpler hands most commonly fit in Europe and North America were tested to gauge their functional capabilities, this will act as a baseline for later studies.
Modes of control
Hands, programmes and options tested.
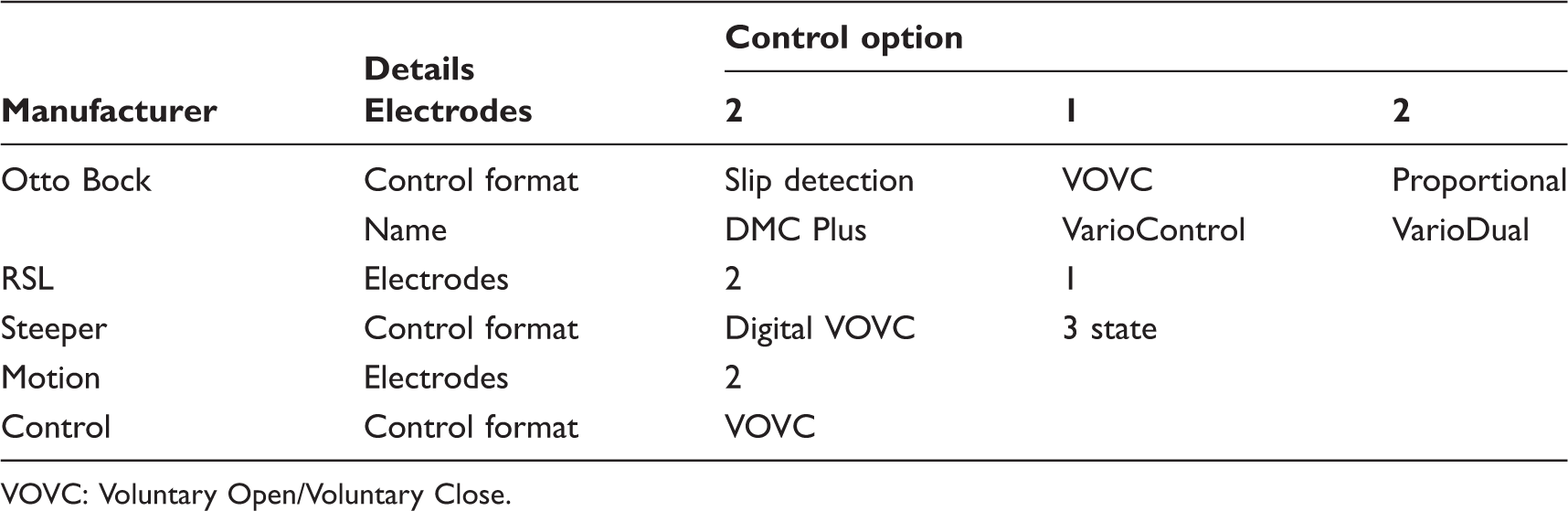
VOVC: Voluntary Open/Voluntary Close.
Since some users may have only one usable muscle to control their prosthesis, single channel controllers have been developed. Some, like the Steeper controller, divide the range of the single muscle into bands: the one corresponding to the lower tension is used to command the hand to close, while the higher tension is used to open the hand. Others, such as the Otto Bock VarioControl, map the proportional tension of the muscle to the degree of flexion, so a relaxed muscle results in a closed hand.
This study focuses on the performance of the earlier generation of myoelectric hands, that typified most devices prior to the launch of the TouchBionics (Livingston, Scotland) iLimb hand in 2005.
Method
Subject
This study aimed to measure the basic functional capabilities of the device alone and attempts to remove the influence of the operator as much as possible. Hence a single user was chosen with repeated measures over a period of time. The relative scores thus emphasize the differences between devices or control schemes.
The subject was the author, who has not lost an arm, but has irregularly used myoelectric control over the past 25 years. He has operated a variety of hands using a custom socket over his forearm. Preparation for this study included general activities with the hands, so basic learning to use the hand was complete. Testing required familiarization to the specific control schemes. SHAP is designed to test the functional capabilities of the subject and the hand. By the use of a single subject inter-subject variations could be reduced substantially. The use of the experimenter allowed many more repetitions of the test to be performed than would be practical or ethical with a cohort of users. Since it was performed by the experimenter on the experimenter no ethical approval was required.
Equipment
The subject was fitted with a splint over the left forearm, extending from the fingers to the olecranon. The prosthesis was positioned over the dorsal surface of the arm and displaced 15 cm distally from it (Figure 2). Otto Bock myoelectrodes were retained over flexor and extensors, in the same manner as a self-suspending socket. The splint was manufactured by the prosthetics team at the Institute of Biomedical Engineering, University of New Brunswick, using conventional materials and techniques. Generally the hand-eye line was similar to that of a routine fitting. The left hand was chosen as it was the subject's non-dominant hand. This was considered appropriate, as the majority of prosthesis users with a single side loss use their prosthesis in a non-dominant manner, irrespective of any natural dominance. SHAP requires the hand being tested to be the leading hand, so used in a dominant manner. Thus a user performing SHAP with their prosthesis would be employing their non-dominant hand in a dominant role. By using the left hand this situation was repeated for this study.
The splint used to retain the prosthesis batteries and electrodes.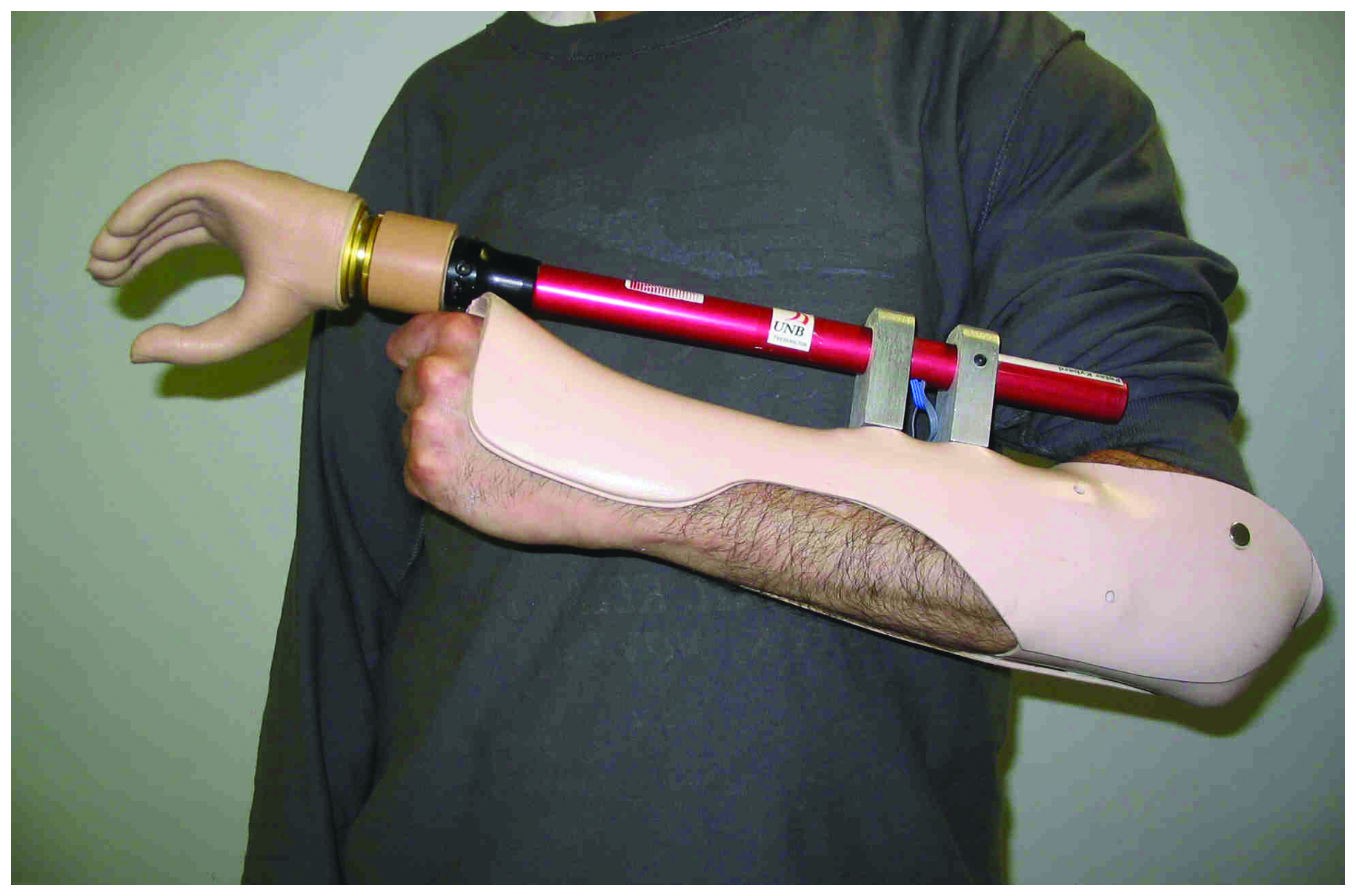
Protocol
The subject was seated at a table, with relaxed shoulders and arms resting on the table, the elbows were at 90°. The form-board with timer was placed directly in front of the subject, approximately 10 cm from the edge of the table. For each task, the subject started the timer, performed the task and then stopped the timer with the same hand.
The test was performed twice a day for 11 successive working days. The first day was used for the adjustment of EMG amplifier gains and familiarization with the hand. The next 10 days were divided into two equal length epochs. Any learning and accommodation would be observed from the difference of these two epochs. The results reported are based on final five days (10 runs). The programme is summarized in Figure 3.
The programme of tests performed on each hand. The hand was tested over 11 days with the data from Day 2 onwards being studied. The chart also shows which statistical test was used with which run.
Hands tested
Hand system design
Three Otto Bock (Duderstadt, Germany) hands were used: SensorHand speed, DMC Hand and Transcarpel (7 3/4”). The SensorHand Speed was set to maximum speed and three different control formats were tested (Table 1). A Motion Control (Salt Lake City, UT, USA) MC Hand was used and the RSL Steeper (Rochester, Kent, UK) hand was tested with two controller formats. The controllers chosen covered the range of formats available from the manufacturers; one electrode, two electrodes, with or without any slip detection. The hands represent those the majority of wearers in Western Europe and North America employ.
Speed of prehension
As the SHAP test is related to the time of execution of the task it was important to measure the speed of movement of the hands. The motion of the fingers was recorded using a Vicon Motion tracking system (Oxford, UK). Markers were placed on the index finger and thumb tips and at the base of the digits over the common pivot. Ten cycles were recorded. The angular velocity was then taken from the Vicon software and the mean of the results calculated. As the fingers quickly achieve full speed, the peak velocities were taken over the majority of each cycle and the mean of 10 cycles calculated.
Data analysis
There was only one subject so there is only one score per condition. The conditions (different hands) where grouped together for the analysis. The Overall SHAP scores of each of the hands were used. Daily order was checked using unpaired t-tests of the first and second run for each day, for the 10 days of both epochs, 10 unpaired t-tests were used. If order was not important these two sets of data should be similar.
Learning effects were checked by using unpaired t-tests between the first epoch, runs three to 12 and the second epoch, runs 13 to 22 (20 overall scores).
A between subject analysis of variance (ANOVA) was used to compare the different overall scores. The independent variables were the hand or controller types (seven instances), the dependent variables were all the overall scores from epoch 2 (70 scores). In all cases, alpha was set at 0.05.
SHAP generates individual grip scores that are used to generate the overall score. Six grips: Tips, Lateral, Tripod, Spherical, Power and Extension. These individual grip scores were normalized against the overall score by dividing the individual grip score by the overall score, to show the scores relative to the overall performance. 6
Results
None of the t-tests for daily order or learning effects was significant (p much greater than 0.05), thus improvements due to practice or daily familiarity were not found.
Overall hand function
The majority of the hands were of a very similar design and they achieved similar overall scores (Figure 4).
Comparison of the overall scores of the five different hands and four different control formats. The hands are ranked in descending order. A star indicates significant difference between the device and its neighbour to the left. This reveals three distinct groups of hands with similar performances. Details of the controller types are provided in Table 1.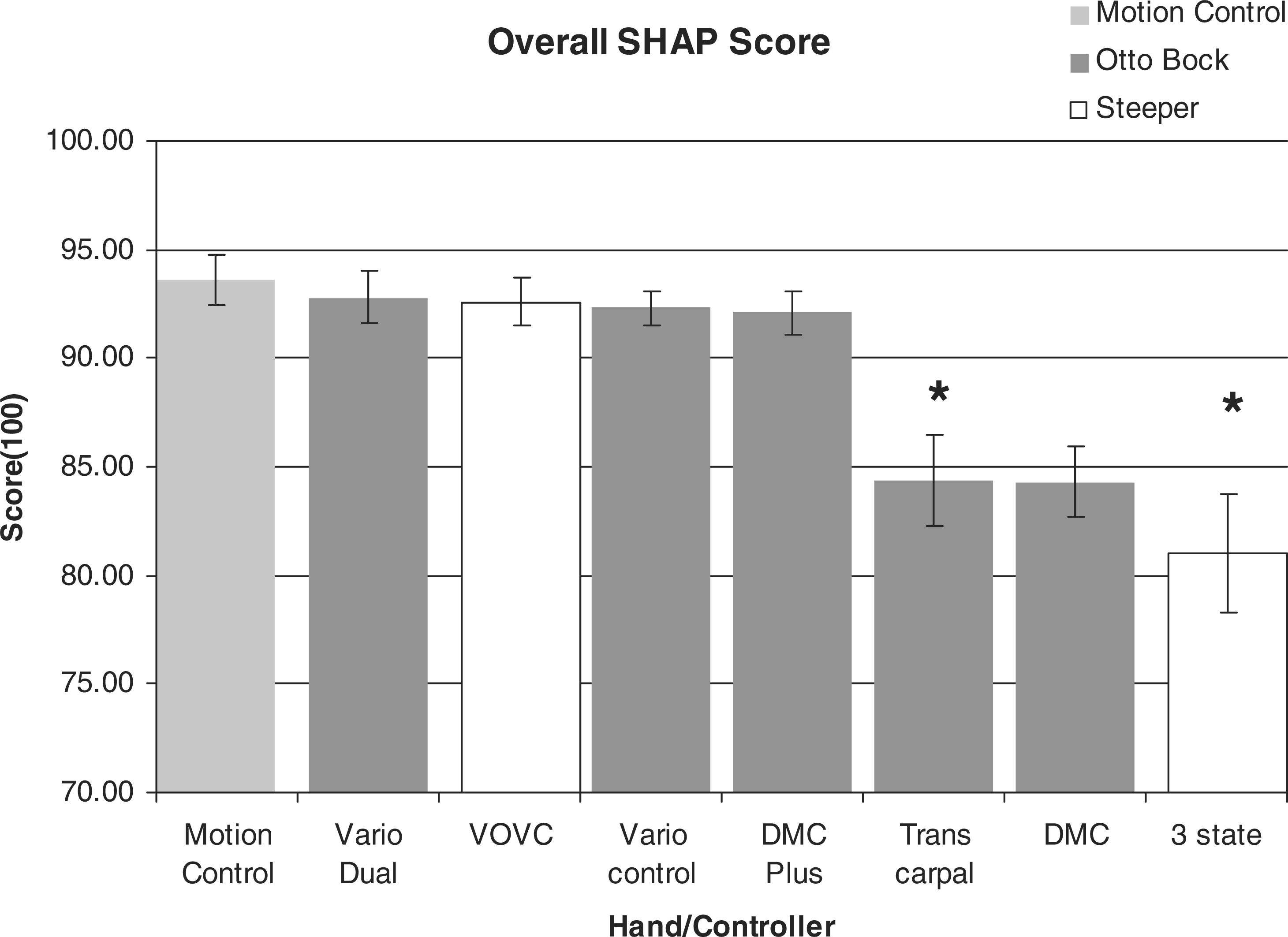
Analysis of the overall scores
The analysis of variance of all of the overall scores showed that they were not all the same population (eight hand/controllers, 10 scores per hand, df = 79, p ≪ 0.05). The hands separate into three groups: the first all have scores over 92 and are similar in shape. The second group contains the short hand design made for transcarpal fittings and the older DMC hand. The last hand which had a significantly lower score was the RSL Steeper hand, controlled with one electrode, three state controller. All the hands were placed in decreasing order of mean overall score, (all scores taken from the second epoch) (Figure 4). T-tests were applied to the pairs at the discontinuities (DMC plus to Transcarpel and DMC to 3 state). Test data were the 10 overall test scores for both hands, in all tests p was much less than 0.05 (Bonferroni correction applied).
Individual grasp function
From the normalized data it is possible to observe which grip is less effective, relative to the overall performance. 6
Using the three different groups identified (above) the different normalized grip scores were compared (Figure 5). In the first (largest) group (Motion Control, Bock VarioDual, Steeper VOVC, Bock Vario-Control and Bock DMC Plus), the grips were arranged in decreasing order of mean score over the 10 tests of epoch 2; Lateral, Power, Extension, Tripod, Tips and Spherical. The Spherical and Tips grips are significantly poorer in performance than the other four grips, which were similar in effectiveness (Student's t-test, was performed on the Tripod and Tips data, two grips, 10 individual scores each grip, five hands p ≪ 0.05, df = 98, Bonferroni correction applied).
Normalized grip scores for the largest group of hands, as defined by their overall mean scores (Figure 4). Each grip score is divided by the overall score to indicate the relative performance of each grip, Tips and Spherical grips are significantly less than the next lowest, Tripod (p ≪ 0.05) indicated by a star (*).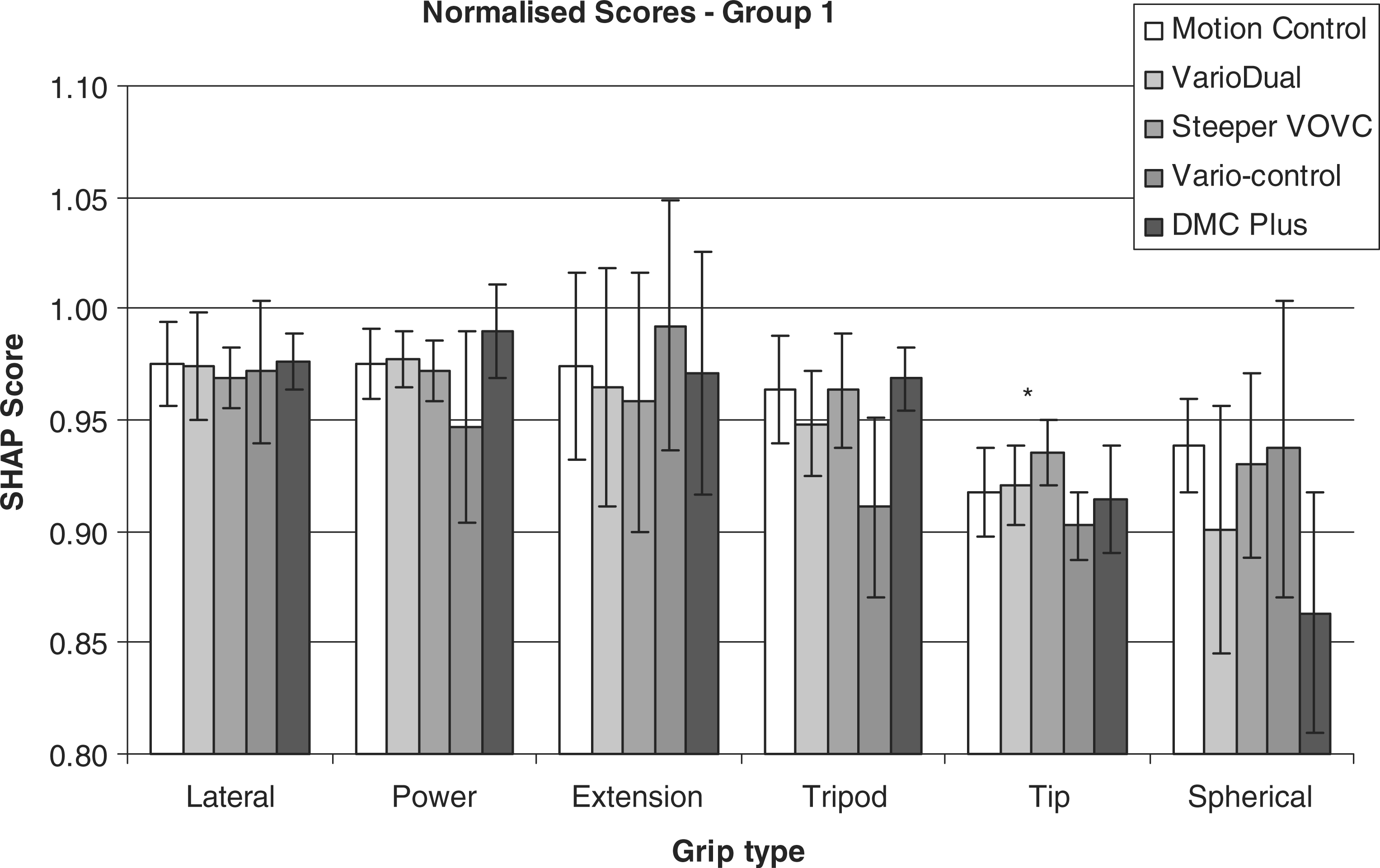
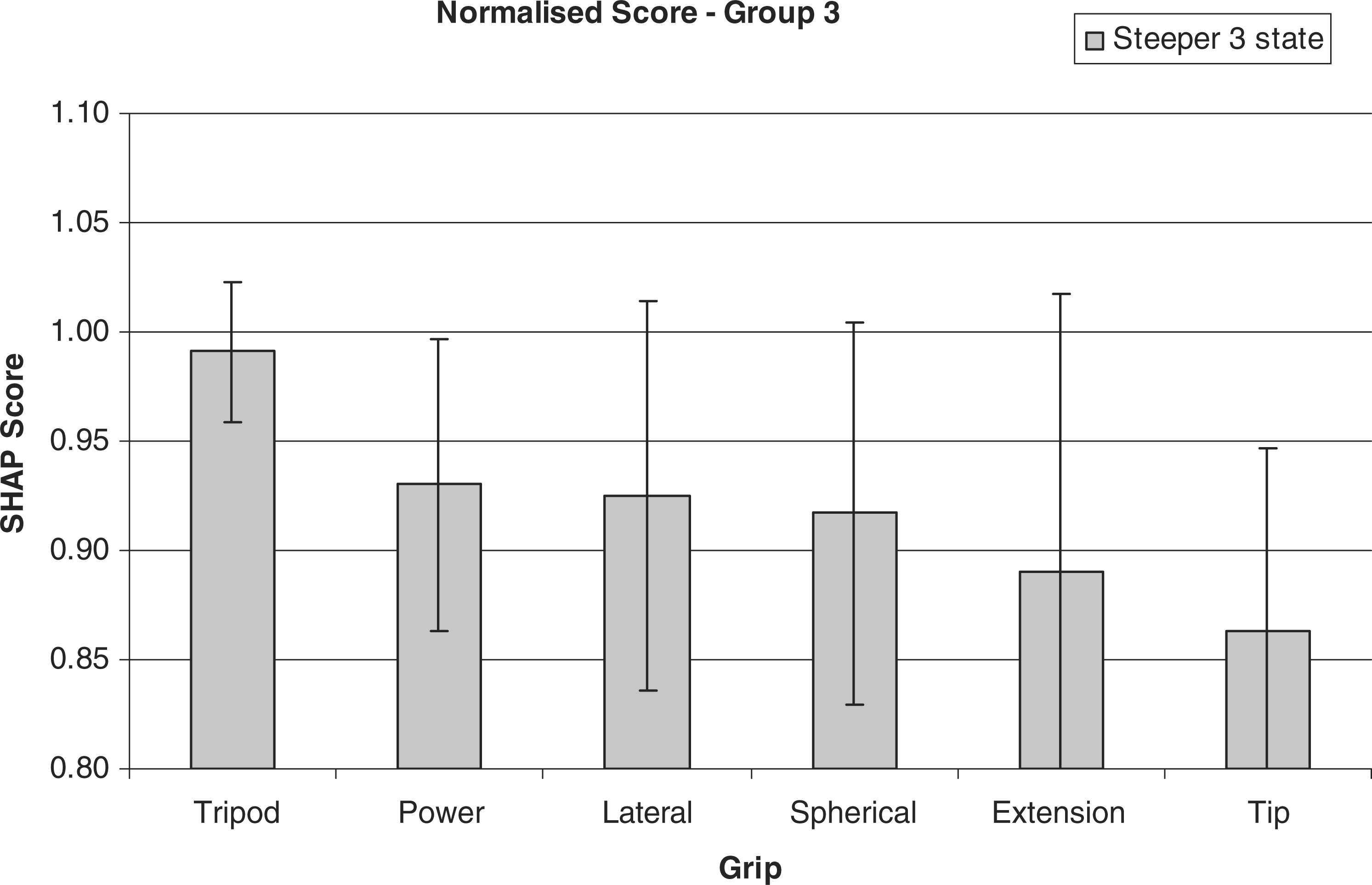
For the second group (Bock Transcarpel and DMC) the Extension Tripod were significantly less functional than Lateral, Power and Spherical plus the Tips grip was less functional still (Figure 6). Again, the grips were arranged in decreasing order of mean score of the 10 tests in epoch 2 and differences identified before Student's t-test were applied to Spherical and Extension (two grips, 10 individual scores each grip, two hands p ≪ 0.05, df = 38) and Tripod and Tip (two grips, 10 individual scores each grip, two hands p ≪ 0.05, df = 38), Bonferroni correction applied each time. For the single RSL Steeper hand with the three state controller, no grip was significantly different due to very large variabilities in the data (Figure 7).
Normalized grip scores for the second group of hands, as defined by their overall mean scores (Figure 4). Each score is divided by the overall score to indicate the relative performance of each grip, Extension, Tripod and Tips grips are significantly poorer in functional performance to the other grips (p ≪ 0.05) indicated by a star (*). Normalized grip scores for the hand with the poorest functional score, as defined by their overall mean scores (Figure 4). Each score is divided by the overall score to indicate the relative performance of each grip. While some have lower scores their variability means there is no significance difference between grips.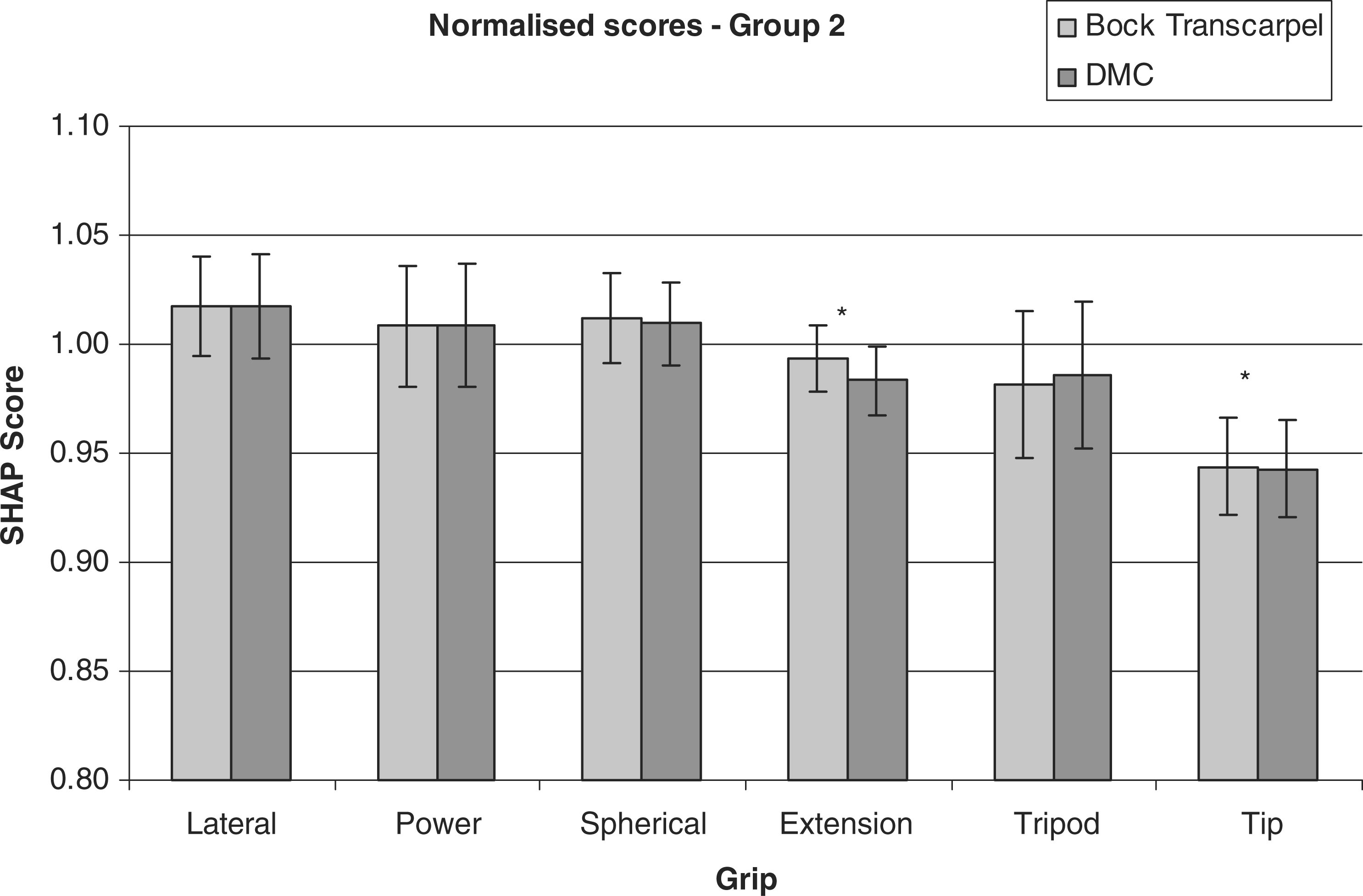
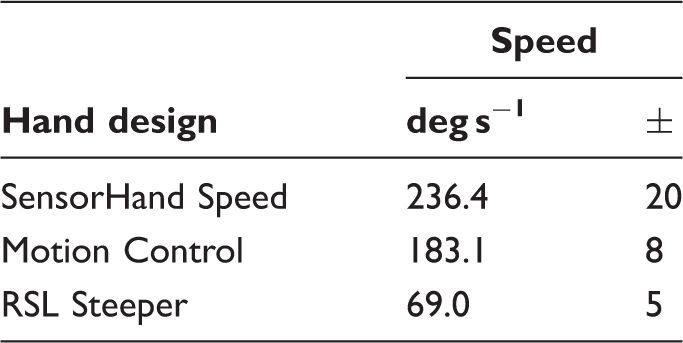
Hand speed
Angular velocities recorded for the three main hand designs.
Discussion
The normal healthy hand shows a score greater than 97 and the reduction in score below that is proportional to the level of function. SHAP was designed to be quick and easy to administer, as a result its competence was designed to be limited to the assessment of the function of the hand alone. All judgements made here are based entirely on this area of hand assessment. SHAP does not make any determination over the bodily compensations required to operate the hand, although it has been shown that use with a motion tracking system can elucidate details of these compensatory motions.15,16
Hand comparison
The hands had similar shape and scores. The smaller transcarpal hand scored lower (84.4), it possessed a smaller gape and so it was harder to pick up the larger objects. The second hand in this less functional group was the DMC, which was a much older hand in design and moved more slowly (84.3). Finally, while the Steeper hand was similar in shape, when using the three-state controller it was much more difficult to use quickly and precisely. Controlling the device was more involved, especially repeated grasping actions, which became slower and harder to perform, hence the hand with this controller achieved a much lower score (81.0), while with an easier 2 channel VOVC it had a score very similar to the other designs (92.6).
The normalized scores betray an interesting finding; that while the hand is set in a grip that should afford good tip prehension, this does not prove to be the case in practice. It is in line with the results reported in Kyberd et al., 6 where the normalized Tips grip for six users of standard Bock DMC hands was lower than the other grips.
The difference in the scores for the SensorHand and other hands was, in part, due to the control format. The SensorHand Speed relies on the force sensors to apply lighter forces on the target. Its minimum grip is still large. So combined with a fast prehension speed, it makes the hand harder to control precisely, forcing the user to repeatedly reapply grip onto some objects before a creating a stable grip.
RSL Steeper Hand – Voluntary Opening/Voluntary Closing
The Steeper Hand was slower in motion and both control formats only used a simple On/Off. While the SHAP score is derived from the time of execution, a slower speed might bring a lower score, but the slower speed also meant that it was easier to control than the very quick Otto Bock, hence the overall scores were very similar (92.6 for the Steeper and a maximum 92.8 for the Bock).
RSL Steeper Hand – three-state controller
This recorded the lowest score (81.0) compared to that of the dual site controller (92.6). This form of control is both harder to achieve and harder to tune to the best performance. The only adjustment possible with the hand was the gain of the EMG amplifier. The control format is superficially similar to that developed by Parker et al. 17 – 19 but it is not the UNB controller. Parker established both theoretical and practical limits on the controller, relating the noise of the signal to the thresholds of all states. This more successful controller allowed adjustment of all the thresholds to find optimal levels in relation to the noise on the EMG signals and thus was easier to master than the Steeper solution.
Hand speed
While SHAP scores depend on the speed of the entire action. Hand function clearly depends on more than rapidity of grasp, and since the speed of the opening of the hand alone does not significantly alter the SHAP score, this suggests that the type of controller has a greater impact than hand speed on the functional performance. Also that SHAP is more than a measure of hand speed alone. While the designs had widely different speeds (the Bock being over three times faster than the Steeper) their overall scores were not significantly different. The speed of motion of the hand has to be reduced considerably before it has an impact on the score, this only occurred with the much older DMC hand. The SensorHand Speed design combines the fastest motion with the strongest grip so that without the finger tip sensors on the hand, it would be very hard to control. It is possible to slow down the hand, but the purpose of this test was to assess the impact of hand speed on the score. For any clinical fitting the speed would need to match the user's capabilities.
Interpretation of results
These results are the relative functional performances of these hands and controllers. When interpreting how a different user would perform with these devices if the subject achieved a higher (or lower) score for one particular hand/controller combination than the subject featured here, then it is likely that the second user would score proportionately higher (or lower) on other hands.
Conclusion
The functional capability of a number of commercial single degree of freedom myoelectric hands was measured using the SHAP. All of the hands measured were of a similar design; single degree of freedom with the fingers set in a precision grip. Similar hands had corresponding functional scores when controlled using comparable control formats. Only when the hand shape or control format were dissimilar was functional score significantly different. While the hands were set in a precision grip it was not the precision grip that achieved the highest score.
Additionally, despite the fact that the test employs a timed element the fastest hand did not score much higher than other hands with similar geometry (94–92), only a very much slower hand scored significantly lower (83). The control format has a greater impact on the overall scores with dual channel voluntary opening, voluntary closing having a greater score than a single channel three state controller (81). Hand size has an impact on the overall score, so that a smaller Otto Bock Transcarpal hand had a smaller gasp aperture and consequently a lower score (84).
Footnotes
Acknowledgements
The author would like to thank Motion Control, Otto Bock and RSL Steeper for the load or gift of the hands under test. The author would also like to thank the staff of the Fredericton Limb centre for their assistance. In addition to the reviewers for their insight and assistance.
Funding
The work was supported by The Canadian Foundation for Innovation, Canada Institutes of Health Research, New Brunswick Innovation Foundation, NSERC (312094-05), Canada Research Chairs Program.
Conflict of interest
The author reports no conflicts of interest. The author alone is responsible for the content and writing of the paper. Support for the work from manufacturers of the prosthesis was to the extent of loan or gift of the hands under test. There was no financial support from any company.