
Abstract
Background: The International Classification of Function, Disability and Health (ICF) has been promoted for use in clinical practice but few articles have demonstrated that it can be used as a sensitive outcome measure, and there has been no published evidence that it can be used for individuals following a lower limb amputation. We developed an ICF-based checklist for individuals who had an amputation.
Objective: To evaluate the feasibility of this checklist in detecting meaningful changes of function and quality of life in persons following an amputation using the ICF qualifiers as an outcome measure.
Study Design: Time series study.
Methods: Twenty patients were rated on the ICF checklist items for four time points; preadmission status, one week post-amputation, on discharge from the acute hospital and three months post-amputation.
Results: Seventeen patients completed the full study, having data collected at each of the four time points. Using the ICF checklist, we could demonstrate a significant functional deterioration immediately after amputation with a gradual improvement in function over the following three weeks consistent with our direct observations of these patients.
Conclusions: The ICF checklist has the potential to be used as an outcome instrument as it appears to have content validity and sensitivity as a measure of changes in patients following an amputation.
Clinical outcome measures based on the ICF potentially improve the ability to record, monitor and benchmark patient and treatment outcomes nationally and internationally. This paper addresses the feasibility of ICF categories and qualifiers when used as an outcome measure and indicates that further development and analysis of the psychometric properties of such measures is warranted.
Keywords
Background
A significant amount of work has been done using the International Classification for Functioning Disability and Health (ICF) in various settings.1,2 Numerous ICF Core Sets have been published for a number of conditions over the last six to seven years.3,4 There are numerous articles regarding the ICF, its applicability in clinical settings and its user friendliness, however, very little research has been published demonstrating that the ICF is practical as an outcome measure in the rehabilitation clinical setting. A paper demonstrating that scales could be developed based on simple clinical ratings of the ICF categories has been published. 5 There are a small number of studies which have utilized the condition-specific Core Sets as outcome measures.6,7 Recently, it was demonstrated that the ICF items were sensitive to changes in patients undergoing inpatient rehabilitation following traumatic brain injury. 8 No papers have been published using ICF categories with qualifiers as an outcome measure. Consideration of the use of the ICF as an outcome measure is relevant in view of endeavours to cross-link the concepts contained in outcome measures used in the rehabilitation of patients following amputation9,10 and also to develop an ICF Core Set for individuals following an amputation. 11 Clinicians are keen to have sensitive and valid outcome measures which can be used more broadly, and not solely in the development of new classifications. There is a need to explore the ICF, its categories and qualifiers as a potential outcome instrument in patients undergoing rehabilitation. The process for this includes choosing relevant categories to make a checklist or an outcome instrument, determining the content validity of the outcome instrument in the first instance and then analyzing the other psychometric properties of the outcome measure and its individual items. Establishing content validity is critical to developing and understanding outcome measures. 12 Validation of face validity, reliability, sensitivity and other psychometric properties are also required before using an outcome instrument to ensure that it will be useful in a broader clinical setting.
A generic ICF checklist was developed in 2002. 13 However, there are concerns regarding its generic nature and lack of specificity for the individual conditions in its clinical application.14,15 There is a lack of evidence for the ICF checklist’s ability to capture functional change following lower limb amputation.
The aim of this pilot study was to evaluate the feasibility of an amputee-specific checklist in detecting meaningful changes in function and quality of life in people following an amputation.
Method
The amputee-specific ICF checklist was created by two experienced clinicians (FK and JX) who have been treating amputees collectively for over 35 years. It was based on the ICF checklist version 2.1a 16 and ICF 2001. As well as this, the clinicians developed a list of some of the main functions and factors felt to be affected by the process of amputation and subsequent rehabilitation and then chose items from the ICF categories which they felt may capture the progressive changes. A list of 25 items was agreed upon as being useful for patients following an amputation as it was expected that these items would change during the patients’ journey through amputation and rehabilitation.
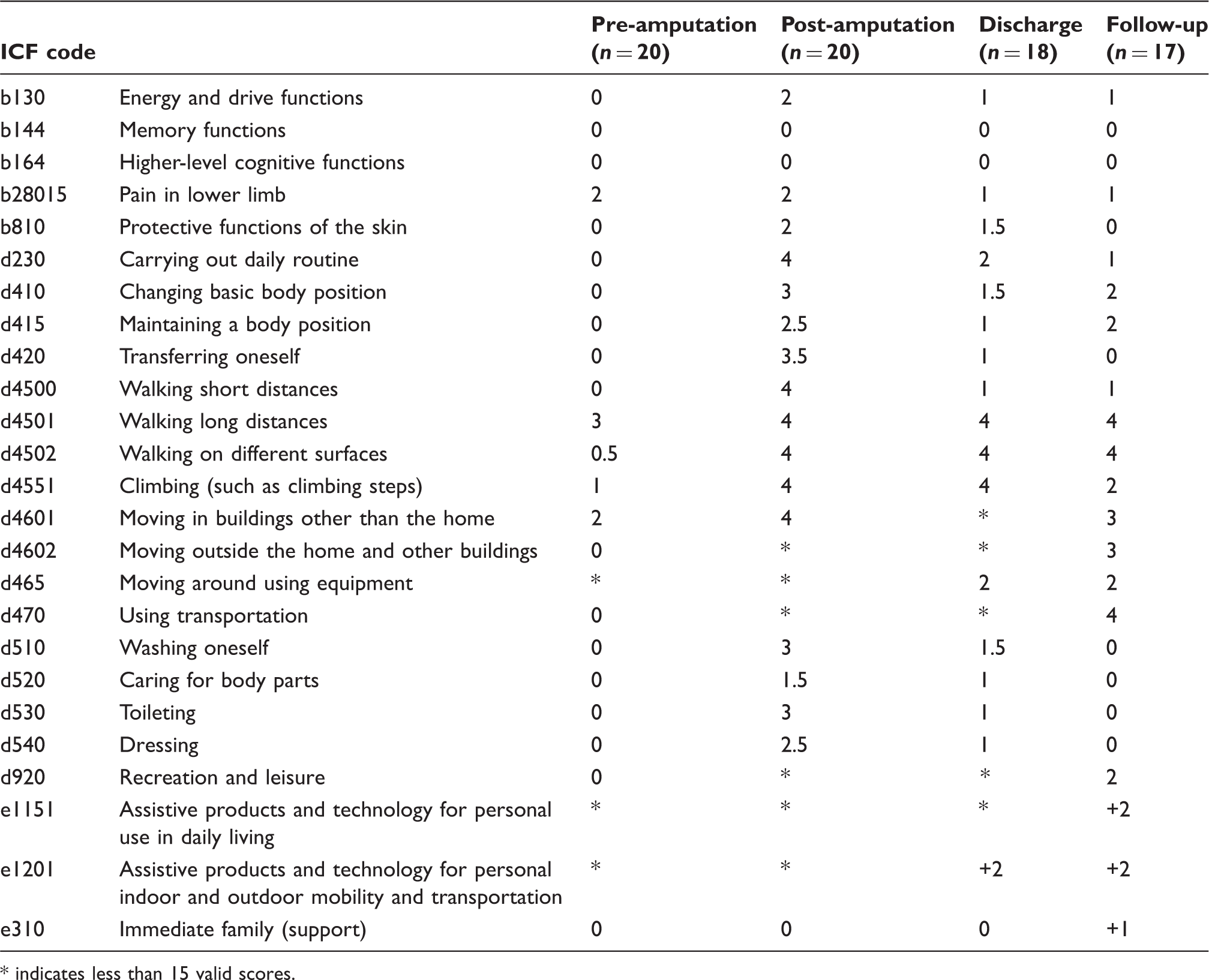
Median ICF qualifier scores at pre-amputation, one week post-amputation, discharge and at three month follow-up.
indicates less than 15 valid scores.
All patients who presented to Liverpool Hospital, a university teaching hospital, for a primary amputation of the lower limb and who were referred to the rehabilitation service were eligible for the study. Patients could be referred to the service before or after the amputation. Those with severe cognitive problems, or those who were unable to follow commands or participate in the rehabilitation programme, were excluded from the study, as major cognitive problems would affect the patients’ ability to cooperate with the programme or to consent. The study was approved by the hospital ethics committee and all patients gave informed consent to participate.
Four time points were determined for data collection
At the initial consultation, a retrospective analysis was performed regarding the pre-admission functional status. This was scored according to the patients’ reported function preoperatively. No verification of the patients’ preoperative functions was undertaken. One week post-amputation, when the patient was rated according to their observed functional status based on physical and functional assessment by various members of the multidisciplinary team. At discharge from the hospital, when the patient was again rated according to their observed functional status based on physical and functional assessment by various members of the multidisciplinary team. At three months post-amputation, when the ICF amputee checklist was rated according to the patient’s self-report obtained by a telephone interview.
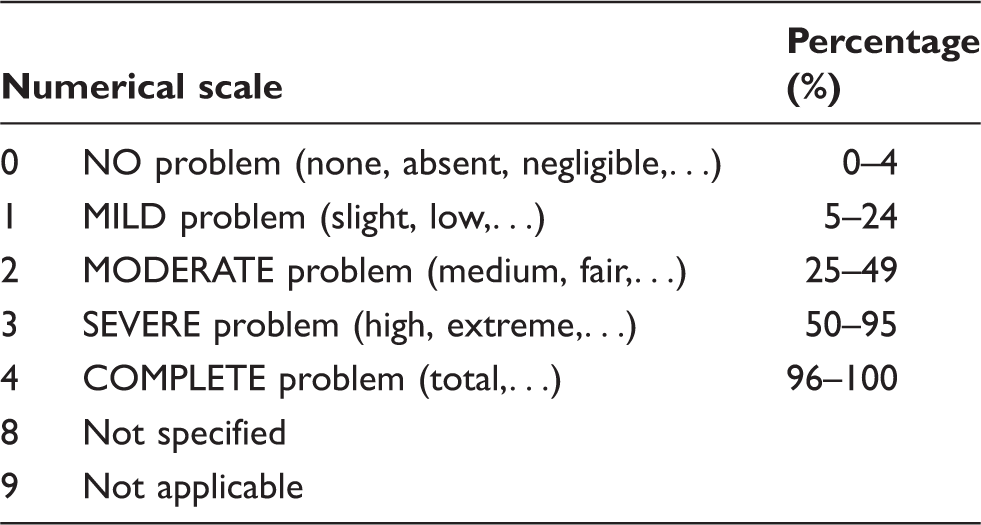
Generic scale of qualifiers.
In the case of environmental factors, these may be positive (facilitators) or negative (barriers). Facilitators are coded with a plus (+) sign, whereas the lack of a plus sign is the code for a barrier.
Analysis of the data was carried out using SPSS V.18 to evaluate significant changes between individual item scores over the period. Non-parametric tests were employed.
Results
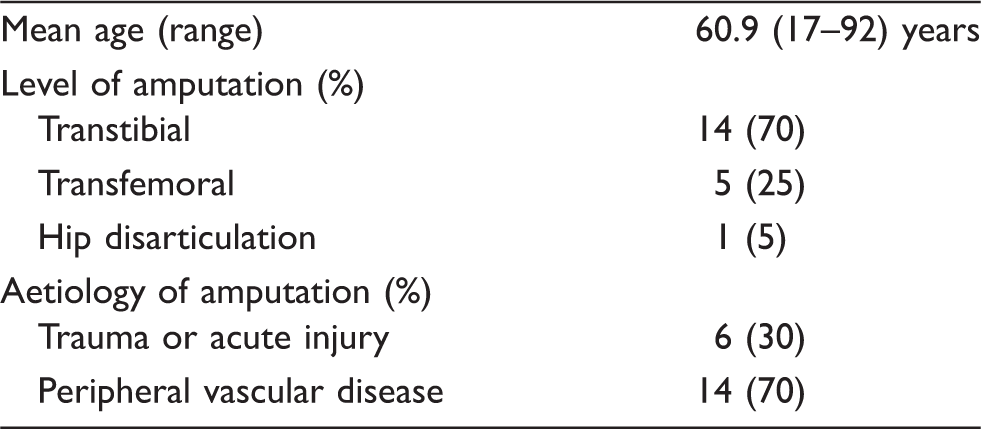
General characteristics of the study cohort (n = 20).
All 20 recruits completed the pre-amputation and post-amputation phase of study. One patient died during the post-amputation hospital stay. One was transferred to another hospital and was lost in follow-up. This left 18 patients who completed the study on discharge from acute hospital. At the three month assessment, one patient was not contactable leaving seventeen patients for whom a full data set was available.
For categories d4601, d4602, d465, d470, d920, e1151 and e1201, a number of patients were scored as not applicable (9) on one or more occasions. Scores of 9 were excluded from further statistical analysis. Following this exclusion, only one patient had valid scores on each of the four time points for category e 1151. The number of patients who had valid scores at each of the four time points for category d4601 was 10; d4602 was 9; d 465 was 7; d470 was 8; d920 was 3 and e1201 was 7. For all the other categories, 17 patients had valid scores at each of the four time points.
The median scores for the four data collection points are summarized in Table 1. Where there were less than 15 patients with valid scores, the median score was not recorded as very small samples would not be meaningful.
The assessment of pre-amputation functional status showed that half of the cohort has moderate to severe leg pain, severe difficulty with longer distance mobility, moderate problem with stair climbing and significant difficulty with mobility outside of the home setting. Most patients scored 9 for moving around using equipment, using assistive products for daily living and mobility as they were independent without aids prior to their admission.
During the first week post-amputation, most of the ICF categories for mobility have a median score of 4 indicative of ‘complete’ disability. For self-care activities, the median score range from 1.5 to 3 indicates a moderate to severe problem. Most patients scored 9 for e1151 and e1201 as they were not yet issued with a prosthesis or walking aids. There were therefore only 4 valid scores for e1151. There were 12 valid scores for scores for item e1201 and the median score of 4 suggests that the use of aids may have been a barrier at this stage, as the patients had not yet learned to use the aids, which is normal at this very early stage of rehabilitation.
On discharge, the basic mobility categories d410, d415, d420 and d4500 were rated as 1, indicative of mild problems. Mobility over longer distances and climbing stairs were severely to completely impaired.
At the three month follow-up assessment, there were no scores of 9 as all the activity, participation and environmental items in this checklist were now relevant to the patient. Eight of the items were scored at 0 suggesting a ceiling effect. Basic self-care activities had improved further and half of the patients had no disability in the activities of daily living. Three ICF categories for outdoor mobility content were still rated as total dependence indicating that there was a need for further rehabilitation to improve these activities. Climbing stairs and moving around outside home scores (median scores of 2 and 3 respectively) demonstrated that improvement of the patient had taken place. Recreation was still moderately restricted. Prostheses and mobility aids were moderate facilitators and family support was a mild facilitator.
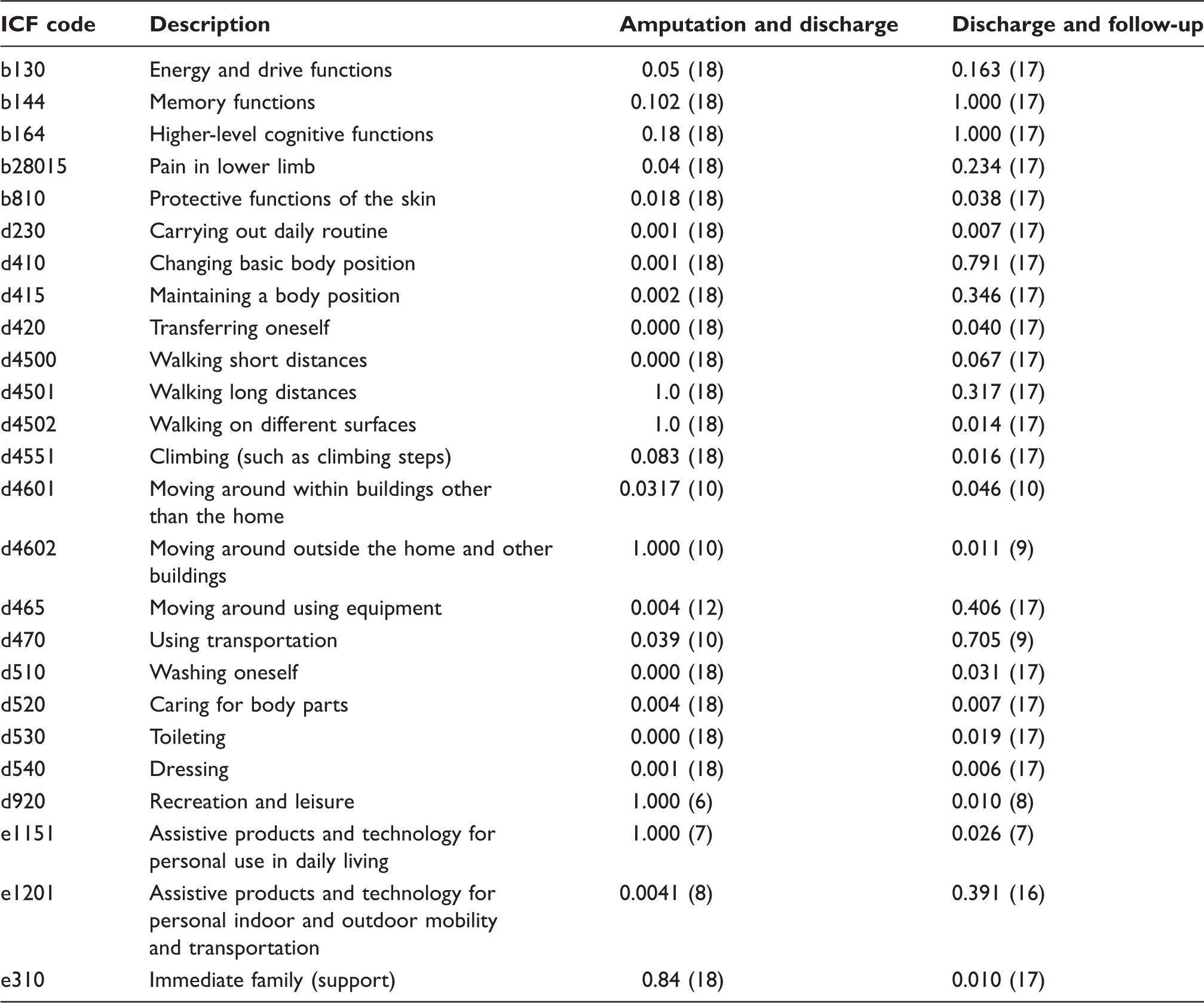
Wilcoxon-signed rank tests between amputation and discharge, discharge and at three month follow-up with the number of paired results in brackets (the significance level is set at 0.05).
Comparing pre- and post-amputation, 19 out of 25 (76%) ICF categories reach statistically significant change (p < 0.05). The items that do not show statistically significant changes are memory functions, higher level cognitive functions, lower limb pain, protective functions of skin, and immediate family support. Assistive products and technology for personal use in daily living were not included in the significance analysis as there were only four valid responses for this category one week post-amputation.
In the comparison between amputation and discharge 15 out of 25 (60%) ICF categories reached statistically significant change whereas 10 items do not cross the threshold of statistically significant change. Those non-significant items are memory functions, higher level cognitive functions, walking long distances, walking on different surfaces, climbing steps, moving around outside the home and other buildings, using transportation, recreation and leisure, assistive products and technology for personal use in daily living and immediate family. Moving around using equipment had 12 paired results, using transportation had 14 paired results, recreation and leisure had 11 paired results and assistive products for mobility had 9 paired results and, even though these items demonstrated significantly significant changes, in view of the small number of patients, caution is advisable in drawing conclusions.
The analysis on discharge and three month follow-up shows that 14 out of 25 (56%) ICF categories reached statistically significant change. These statistical significant items are: protective functions of the skin, carrying out daily routine, transferring oneself, walking on different surfaces, climbing stairs, moving around within buildings other than the home, moving around outside the home and other buildings, washing oneself, caring for body parts, toileting, dressing, recreation and leisure, assistive products and technology for personal use in daily living and immediate family. Table 4 provides an overview of the Wilcoxon-signed rank tests of the data for the study. In this group there were four categories with less than 15 matched pairs of data as indicated by the number in the brackets in Table 4.
Discussion
The ICF has over 1400 categories. Such a large number is cumbersome and challenging to work with in clinical applications. Our pilot study aimed to establish the feasibility of using an amputee-specific ICF checklist for individuals with lower limb amputation as an outcome measure.
Content validity of a measurement system relies on a consensus by experts that the system is doing what it is supposed to be doing. In this study, we considered that the items in the scale were suitable for and did reflect relevant categories of change in patients undergoing rehabilitation after lower limb amputation.
In view of the age and aetiology of the patients it is not surprising that many had significant disability in outdoor mobility including stairs, walking outdoors and walking long distances prior to admission. The high prevalence of moderate pain prior to the amputation correlates with the prevalence of peripheral vascular disease in this group of patients.
On the acute post-amputation assessment, all the items related to self-care activities and mobility demonstrated a significant decline from the pre-morbid state reflecting the functional limitations the patients had after their amputation. The median score on self-care activities, transfer and mobility increased by two to three points, indicative of a progression to moderate to severe disability, most marked in mobility. These changes are not unexpected due to the impact of anaesthesia, surgery, the underlying pathological condition requiring amputation, the acuity of patients one week post-amputation and a component of disability secondary to deconditioning in the perioperative period. The categories of cognitive and memory function did not change and would not be expected to change. Study exclusion criterion effectively excluded persons with severe memory and cognitive problems from the study and with the exception of patients who develop acute delirium perioperatively, we would not expect changes in these categories. However, it is likely that altered memory and cognitive function could affect the rehabilitation progress and therefore including this in an amputee outcome measure might be warranted, but further analysis and a larger sample would be required to make any more definitive conclusion.
The Wilcoxon-signed rank tests on pre- and post-amputation shows statistically significant significance in the majority of the selected ICF categories, again with the exception of memory, and higher cognitive functions as well as pain and immediate family support. The reason for lack of changes in pain probably reflects the high prevalence of pain prior to amputation in the vascular patient.
The functional changes between one week post-lower limb amputation and discharge from hospital, reflect the fact that after the initial significant decline in function, there are marked improvements by the time of discharge. These improvements were evident clinically in this sample of patients and reflected in the ICF scores. There are improvements in pain, self-care (washing, toileting and dressing) and mobility (changing body position, transferring and walking short distances). Generally, these categories improved the median score by one to two points. The most dramatic improvement is in walking short distances, improving from complete problem to mild problem. This is indicative of the emphasis on basic mobility over shorter distances in early rehabilitation. All these improvements in these domains reached statistical significance. The domains which did not reach statistically significant change for improvement were higher level mobility, such as outdoor mobility, walking long distances, walking on different surfaces, climbing stairs, walking in places other than home, using transportation, leisure and recreation. This is expected as most patients with an amputation in our unit would be discharged when they could manage self-care activities and mobility around their home independently and safely after any necessary home modifications had been completed. Their subsequent outpatient prosthetic rehabilitation programme would address the higher levels of mobility and community participation, such as leisure and recreation. The statistical analysis for the change on the median score for prosthesis use has not reached statistical significance because of a number of invalid scores which requires further investigation. Partly this could be explained by our local clinical practice patterns, where most prostheses are fitted on an outpatient basis. This meant that many patients were scored 9 (not applicable) and could not be included in the statistical analysis. The reason for family support not reaching statistical significance is unclear. It is possible that our sample is too small and lacks statistical power or that our sample has more subjects with a limited family support network on discharge. Further investigation of the family support network is required to explore this fully.
In the three month follow-up, we see at least half of the subjects have no difficulty in self-care. The statistical analysis for these categories shows further significant improvement in self-care activities. Most of the outdoor mobility items such as walking on different surfaces, climbing stairs moving around within buildings other than the home, moving around outside the home and other buildings, using transportation and recreation, which did not show significant changes on earlier assessment, start to improve significantly as these aspects of the patient are addressed in the outpatient rehabilitation programme. It is expected that with ongoing prosthetic rehabilitation, the patient with an amputation would continue to improve their community mobility and participation. All these changes are consistent with the normal expectations of progress in a patient undergoing successful rehabilitation after lower limb amputation. It would be beneficial to have a six-month review to determine if further improvements have taken place. The changes of prosthetic use and family support might now also become statistically significant as a facilitator for amputees living in the community.
We acknowledge the limitation of a small sample size but, even with such a small sample, only two of the selected categories (memory and higher level cognitive functions) do not show any significant change. The remaining 23 selected ICF categories demonstrate statistically significant changes at various stages. These changes are not uniform but vary depending on the progress of the individual with amputation suggesting that the 23 categories are appropriate for an amputee checklist and enhance the scale by having different levels of floor and ceiling effects. The impairments and disabilities detected by the checklist appear to peak at acute post-amputation and undergo a general pattern of progressive improvement initially in self-care functions and basic indoor mobility and later on in outdoor and community mobility and community participation after a latency of two to three months post-amputation. There is also room for further improvement in the community and higher mobility items.
In view of the number of categories which show significant change which conforms to conventional expectations after lower limb amputation and participation in rehabilitation, we consider that our ICF checklist for persons following a lower limb amputation has content validity for measurement of change in the patient over the course of their progress through their rehabilitation. Further analysis could be utilized to check for redundant items. Additional items or an increase in the range of the items to make a broader outcome measure could be considered.
While we could correlate the ICF scores at post-amputation and discharge with actual patient function and parameters, this was not possible for the retrospective pre-amputation scores and the follow-up scores which were determined by telephone interview. It would be difficult to match the pre-amputation scores with actual patient function directly but this could certainly be organized for the follow-up scores by direct observation of the patient activity by a member of the rehabilitation team. This could be done in a more definitive study.
This study did not attempt to determine which ICF categories should be included in a definitive ICF checklist/Core Set for persons with and amputation but whether using such a checklist/Core Set as an outcome measurement tool in its own right would be feasible. Based on the findings of this study we are optimistic that a well chosen and balanced checklist/Core Set could be used as an outcome instrument, but further work needs to be done.
While we have established the content validity of this ICF checklist using ICF qualifiers, further testing to determine other aspects of validity and reliability needs to be undertaken to develop a valid clinically useful ICF-based outcome measure. Comparison with other measures of function and quality of life after amputation would be necessary.
Conclusion
Our pilot study with a self-developed 25-item amputee-specific ICF checklist demonstrates clinically meaningful changes in individuals following lower limb amputation in a small sample, suggesting the feasibility of using it as an outcome measurement. These changes are domain and temporal specific and support the development of an ICF-based clinical tool. Further studies to fully explore the psychometric properties of ICF-based outcome measures are required.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.