
Abstract
Background: As part of the process of improving prosthetic arms, it is important to obtain the opinions of the user population.
Objectives: To identify factors that should be focused on to improve prosthesis provision.
Study design: Postal questionnaire.
Methods: The questionnaire was sent to 292 adults (aged 18 to 70 years) with upper-limb loss or absence at five centres (four in Europe) Participants were identified as regular attendees of the centres.
Results: This questionnaire received a response from 180 users (response rate 62%) of different types of prosthetic devices. Responses showed that the type of prosthesis generally used was associated with gender, level of loss and use for work (Pearson chi-square, p-values below 0.05). The type of prosthesis was not associated with cause, side, usage (length per day, sports or driving) or reported problems. The findings did not identify any single factor requiring focus for the improvement of prostheses or prosthetic provision.
Conclusions: Every part of the process of fitting a prosthesis can be improved, which will have an effect for some of the population who use their devices regularly. There is, however, no single factor that would bring greater improvement to all users.
Introduction
Information concerning the use of prosthetic limbs and user satisfaction is difficult to obtain objectively, but is worth attempting to elicit. The user perspective may cover all aspects of the device from prosthesis control, appearance and reliability to the delivery of service. All players have a particular perspective based on their needs and experience. The opinion of the user is essential, but is only part of the picture.
Among the methods to obtain information, the questionnaire is limited in scope but effective in gathering aspects of the process. Properly designed, it can elucidate information about users’ concerns and opinions and gain an idea of their needs. An aspect that is difficult to address is the limited numbers of respondents who may contribute to the results. Any single centre has a narrow perspective based on local demographics. Many surveys reported in the literature are based on a single centre, making the numbers so small. 1– 4 So much so that Davidson in 2002 5 was able to claim that “Nearly all studies of upper limb prosthesis use performed since a study by Kay and Peizer used relatively small samples of between 20 and 60 amputees”, (this refers to a paper published in 1958 6 ). While this might overemphasize the limitation in numbers (e.g. in 1994 Burger 7 polled 414 from the centre in Ljubljana), the point is well made, that statistically sufficient numbers are hard to come by. A disadvantage of smaller surveys is that if sub-groups are considered separately the numbers become too small to be significant. A solution to this limitation is to use the same survey in more centres.
The largest reported questionnaire survey was by Aktins, 8 and was sufficiently large that the author created specific questionnaires for different user sub-groups, namely body-powered devices, electric limbs and those with bilateral loss, each being treated as a separate group while retaining statistical validity. Despite being a long questionnaire, Atkins achieved a good response rate above 60% in all categories. One limitation of the Atkins survey was geographic: while the US market is larger than most, cultural differences between American users and others were not explored. Interpreting the results of a particular survey for other regions has to be undertaken with caution. Davidson’s questionnaire 5 was described as ‘based on’ Atkins’s work, but any differences were not reported. Possible differences may be based on the fact that the USA does not possess a state-based health system, so that some respondents of the Atkins survey may have depended on charities to provide their prostheses. In contrast, much of Europe as well as Australia, where Davidson’s survey took place, is state based, and responses regarding the sort of service received may be different from those of users who are self-financed or supported by a charity.
The present survey, while not as large as the Atkins survey, is of sufficient size to generate distinct groups for more detailed analysis. It also obtained responses from users of different countries and healthcare provisions, giving a broader perspective. It is based on the first part of a survey originally devised to investigate the opinions and concerns of users in the United Kingdom and Italy under the EU-funded Technology for the Disabled and Elderly (TIDE) project initiative MARCUS (Manipulation and Reaction Control under User Supervision TP-150) in 1994. It was also employed in 1998 in the EU project Totally Modular Prosthetic Arm with high Workablility (ToMPAW, DE-420), and in 2006 it was offered to users attending the limb clinic in Fredericton, New Brunswick in Canada. The data presented here represent a set-point for the opinions and wishes of the user population at the time these surveys were conducted, which occurred before newer technologies entered routine use.
To be sure that any device design is acceptable to its target population, it is important to canvas their opinions. In the rehabilitation field, user consultation is particularly important lest users believe that the service is being done to them rather than for them. This survey was part of a process to ensure that this consultation took place.
The aim of the work was to produce a simple questionnaire that was easy and quick to answer, and this choice was supported by a high response rate compared to other surveys in the literature (62% against 10% to 50%). 9 Details of the individual surveys as well as a more detailed review of the literature prior to these surveys are provided elsewhere. 10,11 This paper focuses on the information revealed when the data from multiple centres is brought together. In this way it is hoped to obtain responses more generally applicable and less tied to local variations in population or provision.
While the individual surveys were conducted at very different times in different centres, the basic provision of prostheses had not changed as radically as it may in the near future. Therefore, analysing this data was seen as an opportunity to compare different centres before changes took place, and record a point against which future comparisons can be made. Keeping the same questionnaire facilitated more straightforward comparison, as it is more difficult to compare results of different surveys than results of the same survey conducted at different times. A more standardized approach to monitoring outcomes is required to allow easier exchange of information. Moves are afoot to develop this approach further, 12 and newer ideas for assessing the fit between rehabilitation technology and users 13 are likely to deliver more precise tools in the future.
Method
The survey was carried out at four fitting centres in Europe (Oxford, Edinburgh, Göteborg and Stockholm) and one in Canada (Fredericton). A description of these centres is available in the appendix. More details of the initial design are available elsewhere. 10 Local ethical clearances were received at each of the sites.
Objectives
The purpose of the survey was to obtain basic data on the population of active users of artificial arms, identify areas of concern, and enable recommendations to be made on the direction of research and development in arm prosthetics. This study is to be used as a point of reference for future arm development as more sophisticated prostheses become more widely available.
Design
The questionnaire was designed to be read and answered easily and quickly. The first section used closed questions and could be answered by ticking boxes or filling in simple answers. The second section (not detailed here) comprised longer open-ended questions. The survey focused on the user’s viewpoint and enabled participants to name aspects of most concern to them. The questionnaire was designed after interviews with a small sample of patients who routinely attended the Oxford prosthetic arm clinic. Modifications were carried out after discussions within the team. A brief pilot phase was initiated during which the questions were presented orally to a number of clinic attendees and their responses used to hone the questions. Ten questionnaires were then posted to individuals along with a covering letter and a prepaid return envelope. This pilot study gained a 50% response rate and indicated that no substantive changes were required. The survey was then conducted.
Procedure
The survey was distributed via the post and a single reminder was sent out. When used outside Great Britain, the questions were translated into Swedish and the English version checked for a North American audience.
Sample
The individuals surveyed were chosen by the clinical team at each centre. Participants were adults defined as ‘frequent users’ of their devices 10 who had attended the clinic regularly according to their attendance and repair profile (clinic visits or work conducted on their limb in the preceding 18 months). Individuals were contacted by letter detailing the purpose of the survey and questionnaires were returned in pre-addressed envelopes. The numbers of responses received from each centre were Oxford 54, Edinburgh 36, Göteborg 47, Stockholm 29 and Fredericton 15.
Analysis
Initial analysis of the data showed greater similarities among different centres than along national lines, so that it was most appropriate to pool the data for analysis. The analysis used the Pearson chi-squared test. The test looked for factors that were divergent from an even distribution, i.e. if an attribute was seen in 20% of respondents overall, one fifth of users in each category should have this attribute. Significant deviation from this frequency would imply that the factor was important in the use or provision of the devices. All subsequent inferences of significance represent divergence from the expected level.
Results
Population
Basic survey population data with percentages in brackets (some percentages round away from 100%).
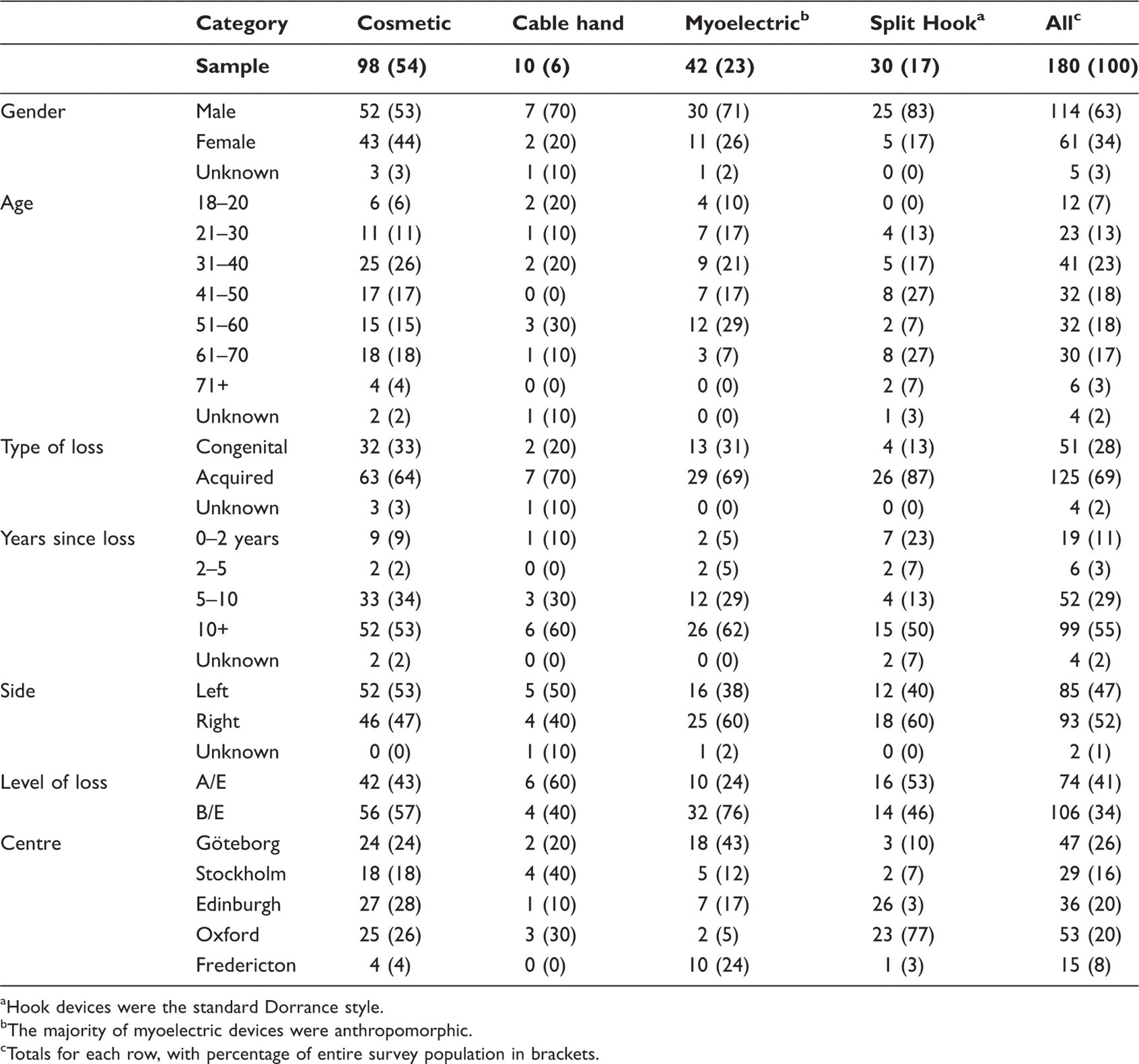
Hook devices were the standard Dorrance style.
The majority of myoelectric devices were anthropomorphic.
Totals for each row, with percentage of entire survey population in brackets.
Data on prosthesis use with percentages in brackets (some percentages round away from 100%).
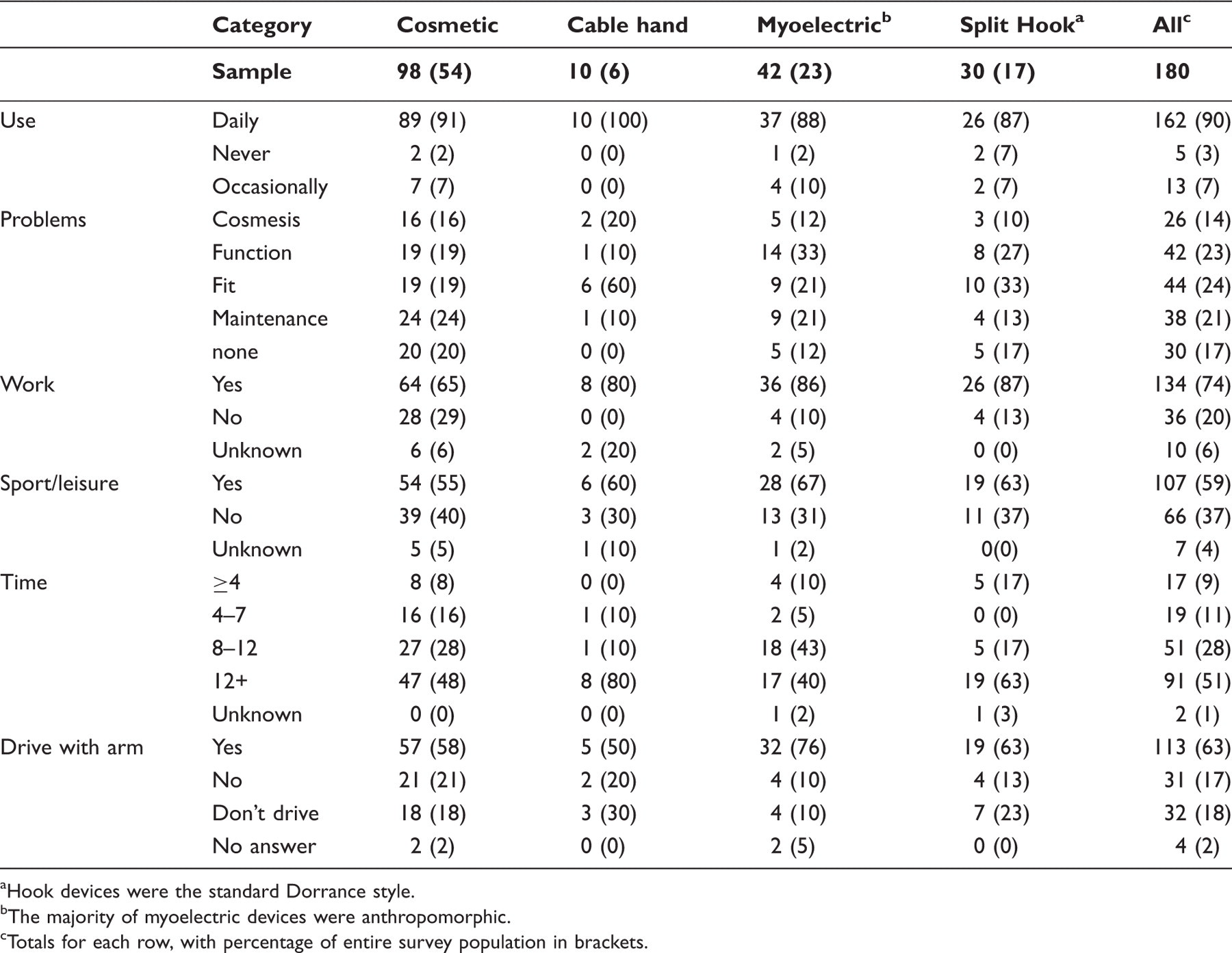
Hook devices were the standard Dorrance style.
The majority of myoelectric devices were anthropomorphic.
Totals for each row, with percentage of entire survey population in brackets.
Analysis
Results of Pearson chi-squared test on the findings of the questionnaire.
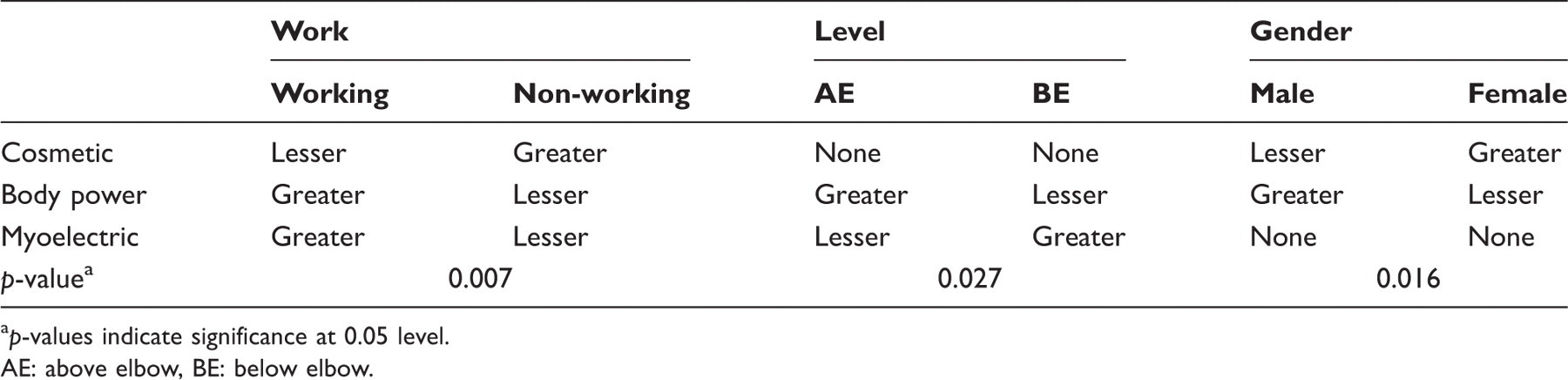
p-values indicate significance at 0.05 level.
AE: above elbow, BE: below elbow.
There was a bias towards cosmetic devices for female users, towards split hook devices for males and against split hook devices for females (Pearson chi-square = 10.26, p-value 0.02). There was also a non-significant bias in use of body-powered hands (7 males versus 2 females).
Similarly, prosthesis type was associated with the level of loss of the individual (Pearson chi-square = 9.14, p-value = 0.03). However, cosmetic prosthesis use did not vary significantly with level of loss. The use of myoelectric prostheses was significantly lower for the above-elbow level but significantly higher for below-elbow loss. Conversely, the use of split hook prostheses was significantly higher for absence of the upper arm and lower for forearm loss.
Finally, there was a significantly higher use of cosmetic hands among users who did not work. For those who did work, split hooks and myoelectic hands were more often reported (Pearson chi-square = 12.08, p-value = 0.01).
Discussion
The population was generally mixed, representing users of different types of prosthesis. Non users were excluded from the population by the recruitment method. Information on why prostheses are not used is valuable, but different methods need to be employed to elucidate this data. 14 Other surveys have defined users as active in various ways, perhaps the most controversial being Roeschlein, 15 who defined an ‘unsuccessful’ user as one who ‘did not use a prosthesis, or wore a prosthesis for cosmesis without using it in a functional manner’. The present authors disagree with the implication that a non-actuated prosthesis is not useful to the wearer or serves an entirely passive role.
Comparative demographics
Comparison of population statistics between current questionnaire and earlier surveys with sample sizes greater than 60.
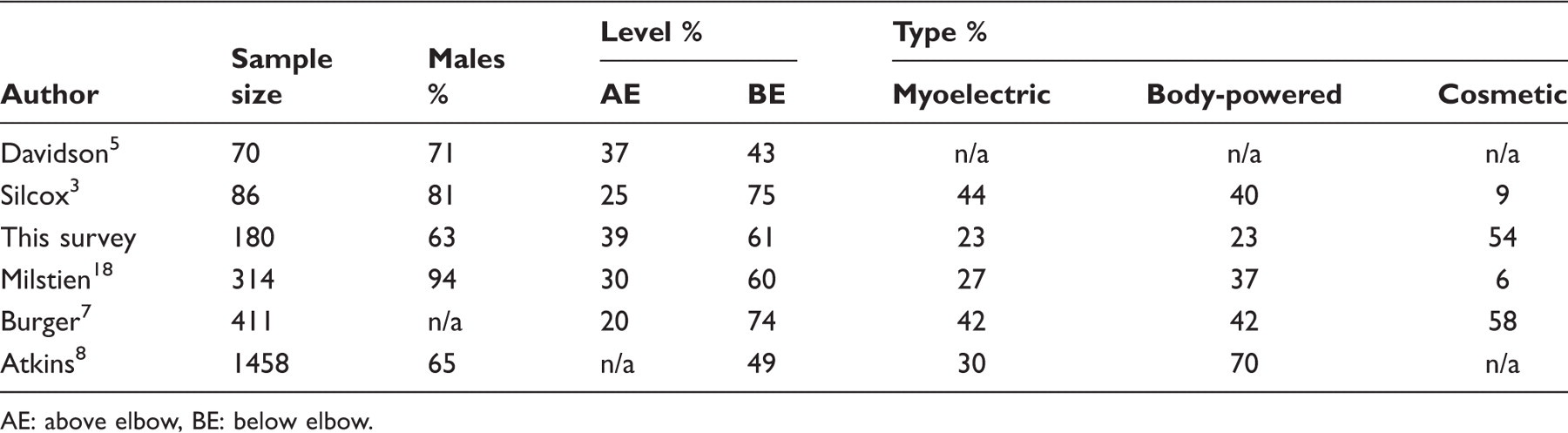
AE: above elbow, BE: below elbow.
Gender
There was a greater number of males than females in the survey population, which may indicate that males undertake more hazardous activities. However, other studies have reported an even greater bias towards males, e.g. Milstien (94%) and Silcox (81%), 3,18 although general limb-absent population statistics seem to be more evenly spread, such as in the Oxford centre population (68%). 19
Statistically, females showed a bias towards cosmetic devices and away from actuated ones, while the male population tended more towards hooks and other cable-operated devices.
Level of loss and prosthesis type
An association between level of loss and type of prosthesis has been observed more generally. 20 As with all aspects of prosthetic provision, any choice must take many factors into account. With a need for a longer prosthesis, these choices are more sharply defined. There is a trade-off between how effective the residuum is alone at assisting in manipulation, and how much poorer a shorter residuum is at supporting a heavy, multi-joint arm. The shorter the residuum, the poorer the leverage for moving the limb. Additionally, the requirement for more joints (whether powered or unpowered) increases cost and mass while reducing the chance of the limb being light enough to carry or reliable enough to be useful. So while the person with the longer absence will need more function from their prosthesis, they may choose lighter, more robust body-powered solutions, (where proprioceptive feedback from the cable can assist in limb control) or they may reject active solutions altogether in favour of the lightest prosthesis, such as an entirely passive lightweight arm with limited but effective function.
Problems reported
One of the most interesting associations not observed is the users’ perceived problems with their devices. Despite written remarks stating that individuals who favoured purely cosmetic or purely functional terminal devices had no interest in any other quality, it cannot be observed from this data that cosmesis was the greatest focus of those with specifically cosmetic devices (Table 2) or that those with active terminal devices were solely interested in function (around 30% for active hands and 19% for cosmetic devices). Appearance seems to have some importance to those with non-anthropomorphic devices, and function for those with non-active hands. While each category requires some interpretation; as ‘cosmesis’ is likely to incorporate the appearance of non-anthropomorphic devices and ‘maintenance’ may mean the reliability of the device or the level of service given to the individual client, no comments to this effect were recorded in the open-ended questions. This shows that the aims and requirements of all users are more complex and involved than simple utility, and designers of new prostheses must comprehend this and incorporate it into their design approach.
Additionally, user comments about the problem of cosmetic gloves becoming dirty or damaged could be regarded as either a maintenance or a cosmesis problem. Certainly, in the Kejlaa survey, the majority of reported problems with gloves came from myoelectric hand users, 2 although this was in an era when the majority of gloves were PVC and became permanently stained very easily. A repeat of this survey today might garner different responses.
An important conclusion from this finding is that high profile attempts to improve prosthetic provision 21 tend to dwell most strongly on the appearance and capability of the device (cosmesis and function) but ignore fit and maintenance, categories which are clearly at least as important to users.
Prosthesis usage
There were a number of questions concerning the use of the prosthesis. They aimed to get an idea about how people employ their devices and for how much of the time (Table 2).
Type of prosthesis used
There was fairly strong variation in the type of prosthesis used. While myoelectric hands are controversial in some quarters, there was no proportionate reduction in the use of these devices, such as time of use or employment in sport. It has been argued by James et al. that myoelectric prostheses give no advantage over no prosthesis at all. 22 While the current survey cannot provide much insight into the functional usage myoelectric prostheses, this survey had a broader range of users than the survey by James et al., whose population was a single socio-economic group followed only until adulthood. Users in the current study were adults selected for regular or heavy use of prostheses, some of whom grew up using prosthetic limbs of different designs. Over 50% had experienced limb loss more than ten years previously, and 23% were still users of myoelectric devices, suggesting that myoelectric hands do provide benefits to some wearers. A second difference in this survey population compared to James et al.’s cohort is that limbs were provided by state funding rather than charitable sources, which may influence user perceptions of their provision.
Time of usage
The questionnaire contained two questions about the amount of time the devices were used. The first concerned how often they wore their devices. The majority used the prostheses on a ‘daily’ basis, with 7% saying ‘occasionally’ and very few saying ‘never’. Davidson reported that 31% used their devices ‘a lot of the time’ or more. 5 The current larger sample showed an even greater bias towards full use of the devices, probably because the selection procedure required consistent users, as the original purpose of the survey was to establish the needs of people who used their prostheses, not of those who did not.
A second question asked users to estimate the number of hours per day they wore (rather than used) their devices. More than 79% wore their devices for more than eight hours a day (Table 2), confirming that if individuals wore their prostheses they tended to wear them all day. This is similar to the results when this question was previously considered by the authors, 10,11 and reflects similar data from other surveys. In a survey in the early 90s conducted at Cambridge, 58% indicated daily usage greater than eight hours, 16 a bias also observed in other surveys 2,9,18 (50% to 60%, 77% and 64%, respectively). Only two users reported daily usage below four hours a day, one of whom reported a problem with fit, which may well have limited the use of the limb.
Directed use
The majority of users (65–87%) wore their devices for work, with fewer being cosmetic hand users. By contrast, use during sport was less frequent (59%). While some respondents suggested that they wore their prosthesis at work for the benefit of others, usage during sport was more likely to depend on the device benefiting them during that particular activity.
Finally, the 63% who used their prosthetic device for driving indicated a purely functional concern (although a study in the UK found that users can and do use a cosmetic device for this task 23 ).
Conclusion
This survey of a wide range of persons who demonstrably wear their prostheses on a daily basis showed a broadly homogenous group with few factors biased towards any particular group or prosthesis type. This suggests that the choice of prosthesis is individual and not unduly influenced by specific factors. The largest population of users employed cosmetic devices, followed by similar numbers of myoelectric and body-powered devices. The survey included more males, and the population generally peaked at age 30–40 years but was quite evenly spread. The clinics in general saw far more people with acquired than congenital losses, but there was an even distribution between left and right sides, with more losses at the distal end of the arm.
The recruitment method ensured that the majority of respondents were long-term users who employed their devices for more than 12 hours daily. They used them for work, sport and driving. The most frequent problems were with fit, function and maintenance, although the largest grouping was cosmetic hands, and those self-identified as primary users of cosmetic hands had fewer complaints about the cosmesis of their devices.
Comparison of the data suggested no statistical associations between type of prosthesis and cause, side, usage (time, sports, driving) or reported problems. The only statistically significant associations were prosthetic type with gender, work and level of loss.
These findings could not identify any single factor that deserves greater focus for improvement of prostheses or prosthetic provision. This means that every part of the process can be improved, and each will have an effect for some members of the population that use their devices regularly.
While this study accessed a larger and more diverse population than some other surveys, it is still limited in range and scope. What is required is a much greater standardization in approach between centres and groups. There are now moves afoot within the profession to standardize other aspects of outcome measures, 14 and it is hoped that attempts to measure aspects of consumer use and satisfaction show continued progress.
Footnotes
Acknowledgements
The authors would like to thank Tasmine Husain for her statistical advice, the fitting centres for their contribution in organization and data collection, the participants for their time in answering our questionnaire
Funding
We thank the bodies that funded this work: The European Union Telematics Applications programme (MARCUS, TP-150 and ToMPAW, DE 420) and the Canada Research Chairs programme.
Appendix: Characterisation of fitting centres
The centres involved in the survey were: