
Abstract
Background: Shortly after the Centre for International Rehabilitation (CIR) casting system was demonstrated in Thailand, the Prostheses Foundation (PF) started modifying this system.
Objectives: To make the process suitable for the Foundation’s main activities, namely clinical service at its main workshop, mobile clinics and satellite workshops.
Study design: Clinical trial.
Methods: The development of the PF-modified CIR casting system took nine months, with the final PF-system launched in January 2008. Since then it has been used extensively at the Foundation’s main workshop and also during mobile clinics.
Results: By September 2009, a total of 1030 trans-tibial and Symes prostheses had been made by this system, and the Foundation had trained more than 200 personnel. Personnel training has been widespread and the PF-system is now being implemented at all satellite workshops around Thailand and at a clinic in Acheh province, Indonesia.
Conclusions: Using the PF-modified CIR system has simplified the Foundation’s work.
The PF-modified CIR casting system is demonstrated as the successful method for making of the prosthetic socket. This provides faster and more practical way than the original CIR system which gain the benefit for the amputees who live in the remote area. The PF-modified system can be implemented to other parties who interest as our satellite workshops began to operate this system in their workshops.
Keywords
Introduction
The Prostheses Foundation of HRH the Princess Mother (PF) was established in 1991 with the main objective of providing free prostheses for underprivileged amputees regardless of nationality and belief, using materials produced in Thailand. Since its establishment, the Foundation has striven to improve and update fabrication methods, prosthetic components, machinery and equipment, making these suitable for Thailand while also meeting international standards.
In 2004, Dr Yeongchi Wu and his colleagues at the Centre for International Rehabilitation (CIR) developed the CIR casting system for trans-tibial (TT) prostheses. 1 The system uses the dilatancy principle, a phenomenon whereby the viscosity of certain substances increases with shear rate or pressure. The CIR system uses grains that adhere limitlessly with each other when compressed under negative pressure. Research has shown some advantages of this system over the classic plaster casting system. 2,3,4
The CIR casting system was first demonstrated in Thailand at the Sirindhorn National Medical Rehabilitation Centre (SNMRC) in March 2007. The Prostheses Foundation was impressed with the system and believed it might be appropriate for the Foundation’s activities. It began to modify and redevelop the methods, equipment and corresponding tools to make them suitable for use in mobile units and at the Foundation’s main workshop. Emphasis was placed on the use of local materials manufactured in Thailand. After nine months of testing, the PF-modified CIR casting system was first used at the Foundation’s main workshop on 7 January 2008.
A major activity of the PF is service provision through its mobile units, which are currently organized five times per year. Approximately 150–200 lower limb prostheses per mobile unit are fabricated and delivered to amputees in remote areas of Thailand and neighbouring countries. To be suitable, this system must be capable of handling at least 150 TT prostheses per mobile unit.
After adapting the operating procedure and related instruments, seven training courses were held from May to July 2008 for a total of 137 mobile unit personnel, including physicians, prosthetists and prosthetic technicians. The PF-modified CIR casting system was first used for a TT prosthesis mobile unit in Thailand’s Roi-Et province in August 2008.
Today the PF system is used in the Foundation’s satellite workshops around Thailand and has also been transferred to a workshop in Acheh province, Indonesia. The Foundation has trained personnel including physicians, physiotherapists, prosthetists (ISPO level I), prosthetic technicians (ISPO Level II) and amputees as technicians. In total, more than 200 individuals have received training in the PF-modified CIR casting system, and associated workshops have been provided with the necessary machinery, equipment and tools. In addition, the PF-modified system has been successfully applied to produce prostheses for animals, including elephants and horses.
Methods
Tools
The notable changes in tools from the original CIR casting system are: the casting bag, the number of plastic bags used and the sponge.
The casting bag
In general, the casting process has become easier using the Foundation’s foam casting bag. The number of plastic bags involved is reduced from two to one because the PF-modified casting bag has been designed as a prefabricated semi-closed, two-layer bag system (Figure 1, left).
The PF casting bag (left) compared to the original CIR casting bag (right).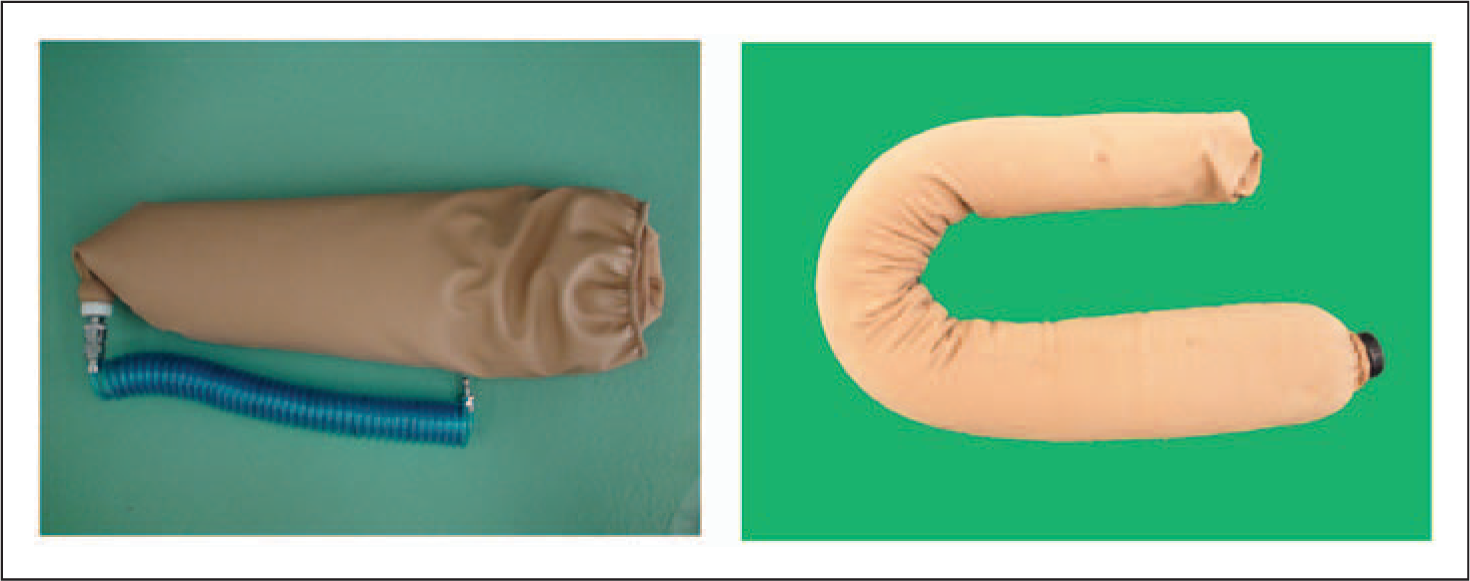
The PF casting bag is open on one side with a polyurethane-coated fabric as the outer layer, an extra-thick nylon stocking as the inner layer, and an elastic band around its opening (Figure 1, left). Compared to the original bag (Figure 1, right), the PF bag is more easily donned which leads to faster impression making. In addition, some original CIR steps were eliminated to streamline the casting process.
The new outer layer of polyurethane-coated fabric replaces the outer plastic bag of the original CIR casting bag and prevents air leaking into the system. Used with a plastic bag and a rubber band, the PF system completely seals the negative casting model.
The inner layer of the bag is made of an extra-thick nylon stocking which can be expanded up to three times its original size in both longitudinal and transverse dimensions, and the pores in the nylon allow the air to be drawn out. Furthermore, the softness of the nylon easily adapts to the shape of the stump, allowing comfort for the amputee during casting.
The bag contains polystyrene foam grains 0.5–1 mm in diameter. The prefabricated vacuum ventilating unit is installed at the end of the casting bag. This feature is an improvement over the original casting bag because it facilitates the use of a vacuum during the casting process.
The PF casting bag is prefabricated in four sizes: small, medium, large and extra large, depending on stump length and circumference. The total length of the bags is 70–80 cm with a corresponding upper circumference around 45–75 cm, depending on bag size.
The plastic bag
The system uses only one plastic bag 0.02 micron in thickness (Figure 2, left), and due to the special design of the PF casting bag, an outer plastic bag is no longer required.
The plastic bag used with the PF-modified casting system (left) and the PF mandrel with the polyurethane sponge (right).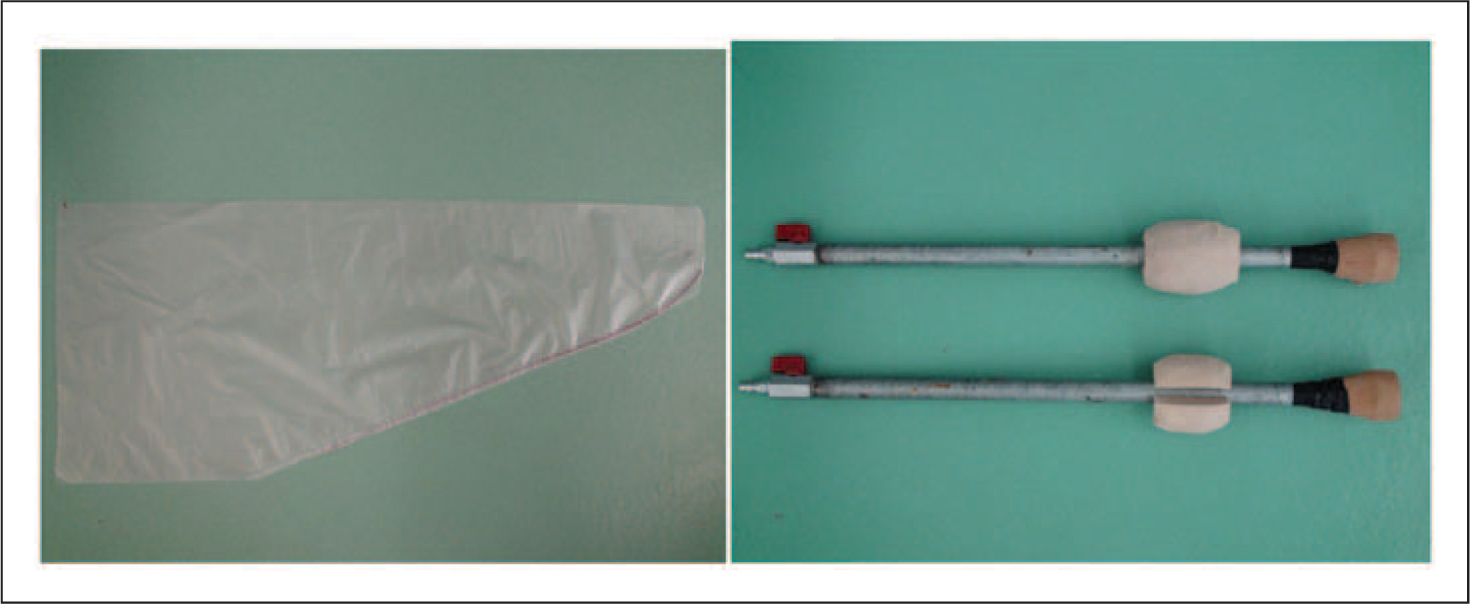
The sponge
The sponge patch used for the original CIR casting system is added on and placed over the popliteal area. With the PF system, a light density polyurethane sponge (specific gravity = 0.27) is used (Figure 2, right). This sponge is still placed over the popliteal area, but it is prefabricated, ball shaped and locked with the mandrel. This sponge allows movement of the sand without deforming the positive model. Sponge displacement no longer occurs with this design, facilitating easier rectification.
Procedures
After measuring the stump dimensions and identifying the bony prominences, the stump is wrapped with a thin plastic cling film. Adhesive foam tapes are cut and pasted onto the bony prominences and possible tender points (Figure 3, upper left). A rubber band is placed and held at mid-thigh level. The PF casting system’s thin plastic bag is donned and then covered by the nylon stocking.
Example of the PF-modified CIR casting procedure: stump identification (upper left), foam bag casting (upper right), making the positive model (middle), front view of the resulting positive model (lower left) and popliteal view (lower right).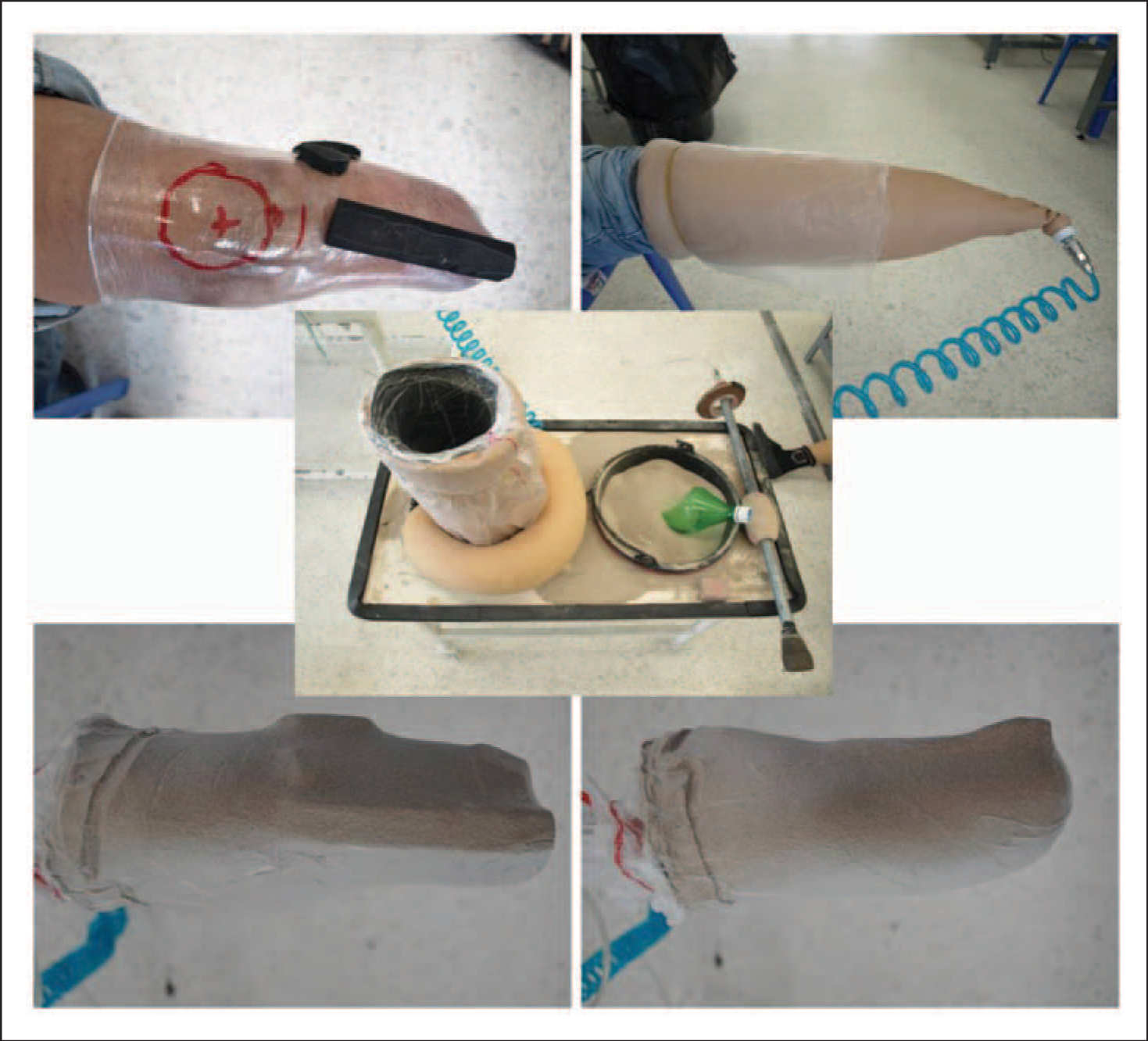
The PF casting bag is rolled over the stump to about 4-5 inches above the femoral condyles. The previously donned plastic bag is then folded down over the casting bag and the rubber band moved down to seal both about 1 inch below the upper trim of the PF casting bag. A vacuum hose with a negative pressure of at least -0.6 atmosphere is then connected to the ventilating unit to extract the air, to solidify the casting bag and form a solid negative model (Figure 3, upper right). Meanwhile, pressure is gently applied by the prosthetist’s hands over the PF casting bag during formation of the negative model until it is solidified. After checking for any discomfort, the negative model is then removed from the stump.
A small amount of silica sand is used to fill the bottom of the negative model. Thereafter, the suction mandrels are inserted together with the polyurethane sponge (Figure 3, middle). The sponge is placed at the level of the popliteal fossa. Next, the negative model is completely filled with silica sand. A base disc is then placed on top of the negative model and the plastic bag rolled up and sealed with the rubber band. The vacuum hose is attached to the mandrel and air drawn out until the positive model has become solid. Following this step, the vacuum hose of the casting bag is released for removal of the casting bag (Figure 3, lower left and lower right).
The positive model is rectified to eliminate any irregularities and to create locks for the supracondylar suspension (Figure 4, upper left), which is the Foundation’s standard prosthetic socket style. The supracondylar suspension is made by tapping the positive model on the medial and lateral sides 1¾ inches above the mid-patellar level to a depth of 2 cm. In accordance with the anatomy, the iliotibial band is spared on the lateral side. Next, the positive model is built up with adhesive foam tape in the popliteal area (Figure 4, upper right) and clay added to fill the gap around the tape (Figure 4, lower left and lower right), to the end of the model. Plastic cling film is wrapped around the model, and one or two layers of nylon stocking then pulled over the positive model. The prosthetic socket is moulded using a bubble vacuum forming method.
Example of the positive model rectification: modification of the supracondular suspension (upper left), modification of popliteal area (upper right), medial view of the resulting positive model (lower left) and popliteal view (lower right).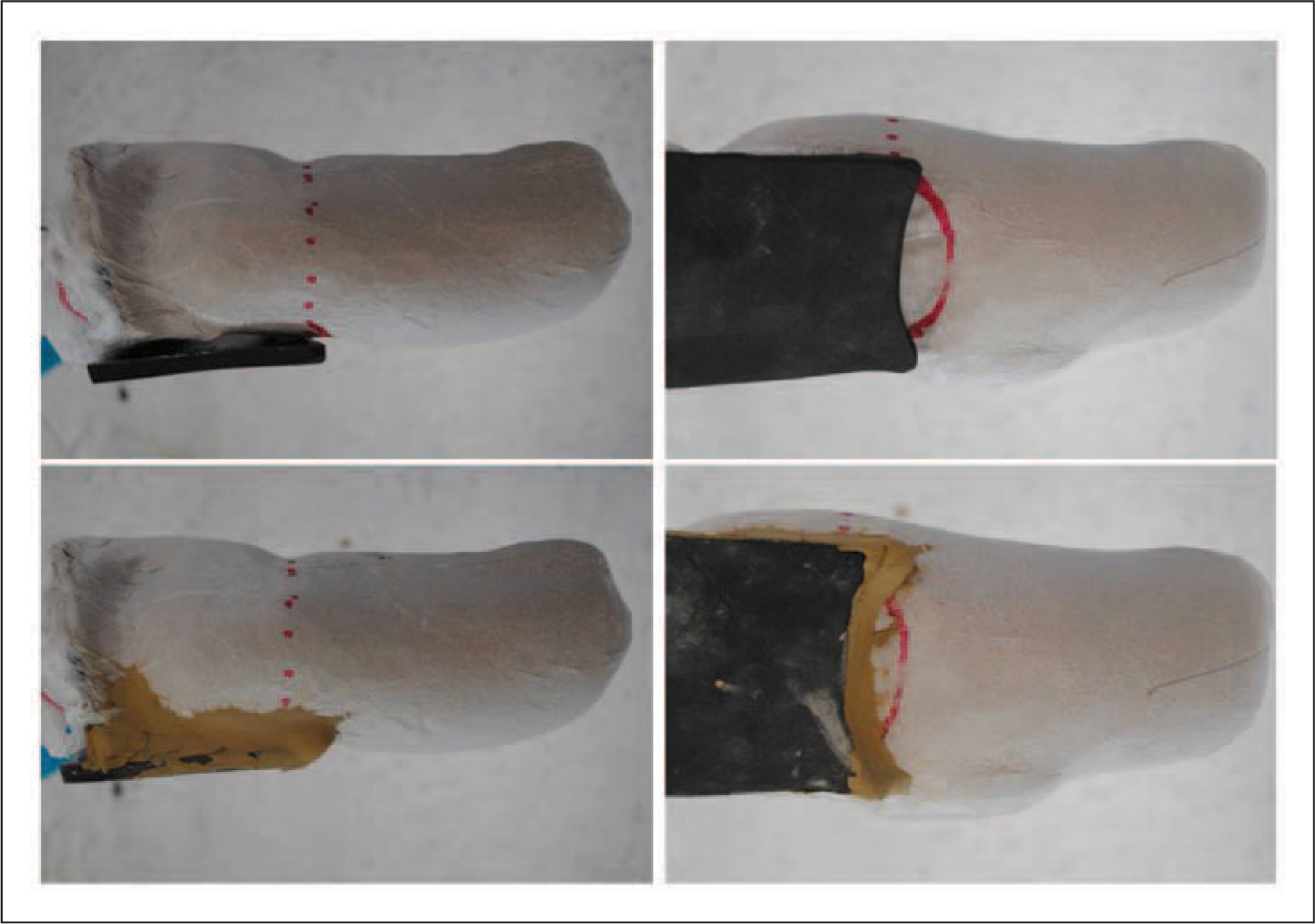
After assembly of the prosthesis, fitting, initial gait analysis and dynamic alignment occur. Once dynamic alignment is completed, a cosmetic cover is fabricated and the final prosthesis delivered to the amputee.
Note: for a Symes socket, the add-on patches are placed around the ankle area and held with the plastic bag and the plastic cling film.
The prosthesis
The trans-tibial (TT) prosthesis is produced using endoskeletal components. A total weight bearing socket is used with supracondylar suspension (Figure 5). The stainless-steel shank, aluminium coupling unit and foot adapter – all machined/manufactured and assembled by the Prostheses Foundation – are used with either the Foundation’s SACH foot (Figure 5, left) or the PF farmer foot (Figure 5, right). The Symes prosthesis is also made using the endoskeletal structure. Like the TT prostheses components, all Symes prostheses components are made by the Foundation.
The Foundation’s endoskeletal trans-tibial prostheses: a cosmetic prosthesis covered with a rigid foam cosmetic cover and an artificial leather skin showing its internal structure (left), and the PF farmer leg (right).
Results
Between 7 January 2008 and 30 September 2009, a total of 1030 TT and Symes prostheses were made using the PF-modified CIR casting system at both the Foundation’s main workshop and its mobile units. Prostheses made at the satellite workshops are not included.
Time monitoring at the main workshop and mobile units revealed that it took on average 100 minutes to fabricate a prosthetic socket using the PF-modified CIR casting system. In contrast, creating a prosthetic socket using the traditional plaster casting method took at least 350 minutes. Normally, an amputee who receives a TT or Symes prosthesis made by the plaster casting method requires two to three visits to the workshop, but with the new method amputees can receive their prosthesis within one day.
Discussion
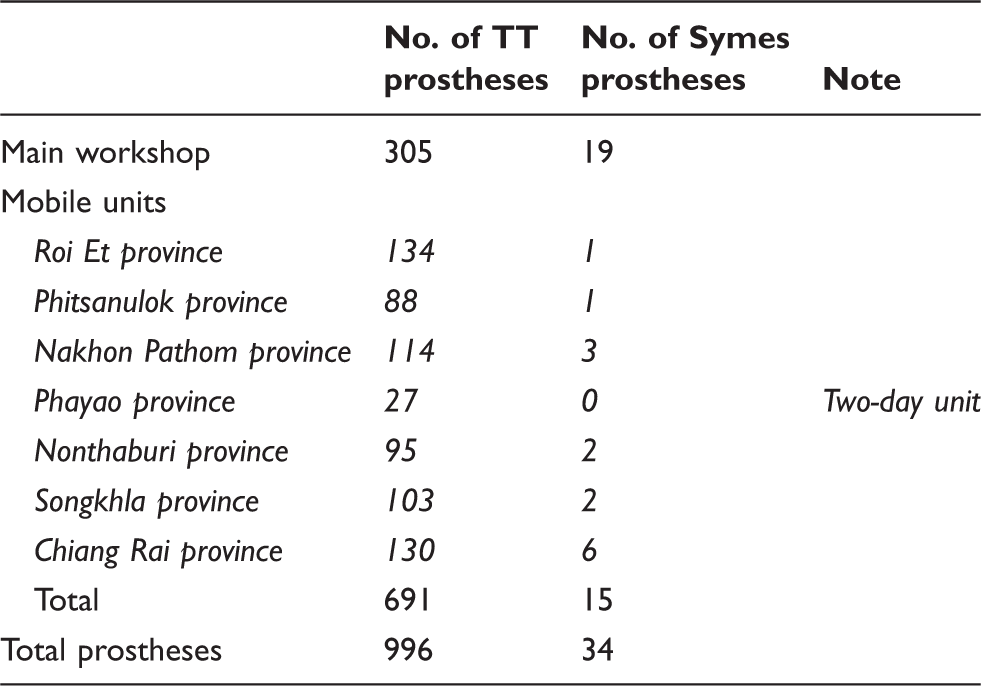
From its release until September 2009, the PF-modified CIR casting system has been used to fabricate 1030 trans-tibial (TT) and Symes prosthetic sockets from both the Foundation’s main workshop and its mobile units. The Foundation’s main workshop produced a total of 324 TT and Symes prostheses at an average of 15.43 per month.
Note: the average number of working days per month is about 15 (14.58) due to national holidays (at least 16 per a year) and mobile unit activity (two weeks each for preparation and operation).
Number of TT and Symes prostheses made using the PF-modified CIR casting system.
The density and position of the sponge are also important because this must not easily collapse during the making of the positive model, but must allow the sand grains to replace its space during rectification. A sponge of polyurethane foam with a specific gravity of 0.2–0.3 is the most suitable. The Foundation ran tests and found that at this density the model’s contour does not deform and is not too difficult to rectify by minimal compression. Moreover, this sponge must be placed with the mandrel at the popliteal area level to allow for sand movement into this area.
When the positive model is rectified, the direction of reduction is upward. This prevents enlargement of the model’s size by sand movement during rectification.
Results from the mobile units show that the PF-modified CIR casting system is applicable to workshops in which many prostheses must be produced in a short time. As the table shows, an average of about 100 prostheses were made within four operating days. This high output was also accomplished through the arrangement and positioning of tools and equipment. Each mobile unit has at least two 96-litre vacuum machines (piston pump type) providing a sufficient partial vacuum for the PF-casting system (–0.6 atmosphere or more). The vacuum tubes are connected and arranged as a circuit to distribute the negative pressure evenly to each working unit in the system. Using this system together with the bubble-forming method allows an amputee to be cast and fitted with a prosthesis on the same day, which is helpful to amputees who live in remote areas.
Production costs of the of prostheses are reduced because most materials used in the process, such as the sand and foam casting bag, can be reused and recycled, which has the added benefit of being environment-friendly.
This article represents an overview of the technical aspects of the experience gained with the PF-modified CIR casting system. In-depth data will be collected and studied in the near future.
This research has been approved by a board committee of the Foundation.
Conclusion
Since introduction of the CIR casting system in Thailand, the Prostheses Foundation has modified this method and developed corresponding machinery and tools (e.g. a workbench, vacuum machine, draping machine, etc.) appropriate for the Foundation’s activities (a large-scale workshop, small-scale workshops and mobile units).
The time taken to manufacture a prosthetic socket was reduced from 350 minutes or more to only 100 minutes apiece. This allows amputees to receive a TT or Symes prosthesis within one day, reducing the amount of time required away from their jobs. Together with the Foundation’s rectification technique, well-fitting prosthetic sockets can be produced.
The PF system is currently used in 16 satellite workshops around Thailand and in a workshop in the Acheh province of Indonesia. Moreover, this system has been applied to fabricate prostheses for animals such as the elephant and horse. Details of these applications will be reported in the future.
After 21 months of usage, the Foundation has concluded that the PF-modified system is a successful method for fabricating sockets for trans-tibial and Symes prostheses customized for the individual patient and produced in high numbers at high quality. The PF-modified CIR casting system has been shown to simplify prosthesis fabrication, and to be applicable to various operations. It is concluded that the modified CIR casting system has more advantages than the classic plaster casting method. Applying this principle, the Foundation is doing further research to develop the CIR casting system for fabrication of the trans-femoral socket.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Acknowledgement
Thanks to Mr Matthew Morrison, CPO who dedicated his time for this article.