
Abstract
Background: The ‘Convention on the Rights of Persons with Disabilities’ (CRPD) requires governments to meet the assistive technology needs of citizens. However, the access to assistive technology in developing countries is severely limited, which is aggravated by a lack of related services.
Objectives: To summarize current knowledge on assistive technology for low- and lower-middle-income countries published in 1995 or later, and to provide recommendations that facilitate implementation of the CRPD.
Study design: Literature review.
Methods: Literature was searched in web-based databases and reference lists. Studies carried out in low- and lower-middle-income countries, or addressing assistive technology for such countries, were included.
Results: The 52 included articles are dominated by product oriented research on leg prostheses and manual wheelchairs. Less has been published on hearing aids and virtually nothing on the broad range of other types of assistive technology.
Conclusions: To support effective implementation of the CRPD in these countries, there is a need for actions and research related particularly to policies, service delivery, outcomes and international cooperation, but also to product development and production.
The article has a potential to contribute to CRPD compliant developments in the provision of assistive technology in developing countries by providing practitioners with an overview of published knowledge and researchers with identified research needs.
Keywords
Introduction
Assistive technology is adapted or specially designed technology for improving the functioning of people with disabilities. 1 The Convention on the Rights of Persons with Disabilities (CRPD) entitles its beneficiaries with rights to assistive technology to ensure their full and equal enjoyment of all human rights and fundamental freedoms. 2 However, access to assistive technology is limited in many countries. 3 – 8 The World Health Organization (WHO) estimates that in low- and middle-income countries only 5–15% of people requiring assistive technology have access to it. 9 Less than 3% of the hearing aids needed in these countries reach there. 10 Estimates indicate that 0.5% of a population need prosthetic and orthotic devices and 1% need wheelchairs, but these needs are far from being met. 11 – 13 Trends in functional limitations among the elderly indicate an increased need for interventions such as assistive technology. 14
The situation is aggravated by the fact that assistive technology is often supplied without considering the need for associated services. 15 In general, these include individual assessment, selection, fitting, training and follow-up to ensure safe and efficient use. These services often have a significant impact on the outcome. In addition, accessibility of the environment is a prerequisite for using certain types of assistive technology. 16 – 19 Incompatibility with the environment may result in assistive technology being abandoned. 20 Provision of substandard wheelchairs without clinical services, training of users and long-term possibilities of local maintenance and repair has been criticised and can result in dangerous scenarios for users. 13
From the viewpoint of the medical model of disability, assistive technology might be seen as correcting the ‘shortcomings of an individual’, while from a social model perspective it is considered an enabler that reduces barriers in a ‘disabling environment’. 21 Stressing the freedom of individuals to make their own choices, which is also to be respected in this field, the CRPD acknowledges that assistive technology can be used both for improving body structures and functions and for improving activities and participation by reducing barriers. 1,2
Compliance with the CRPD requires that assistive technology be equitably available, accessible and affordable irrespective of gender, age or impairment. To achieve this, governments and other signatories need to carry out measures related to policy, legislation, research, development, production, training, information, use and cooperation. 22
The objectives of this review were to present an overview of current knowledge on assistive technology for low- and lower-middle-income countries and to provide recommendations that facilitate the implementation of CRPD-compliant measures.
Method
Without language restriction we searched for literature published in 1995 or later in the web-based databases AMED, CINAHL, PubMed, Sociological Abstracts and Web of Science on 22 June 2009. The search terms ‘assisti* device*’, ‘assisti* technolog*’, ‘braille*’, ‘hearing aid*’, ‘low vision aid*’, ‘orthos*’, ‘prosthes*’, ‘self-help device*’ or ‘wheelchair*’ were used in combination with ‘developing countr*’, ‘less resourced’, ‘low income countr*’, ‘poverty’ or ‘technology transfer’. The reasons for including only articles published in 1995 or later were that two comprehensive reviews of rehabilitation of people with amputations and prosthetics in developing countries were published in 1996 23,24 , and that the authors did not have access to all earlier articles.
Studies that were carried out in low- and lower-middle-income countries, as defined by the World Bank based on 2007 gross national income (GNI) per capita, or that addressed assistive technologies for such countries, were included. Literature reviews, case studies, papers published in non-peer-reviewed supplements, conference proceedings and studies on accessibility measures, dental prostheses and devices requiring surgical procedures for fitting were excluded.
We searched the reference lists of selected articles and included those that met the selection criteria. Relevant articles known to us but not found by the strategy above were included. A complementary search on 9 March 2010 was carried out in AMED, CINAHL, PubMed and Web of Science for the same time period using ‘prosthet*’ or ‘enabling technol*’ in combination with the second group of search terms.
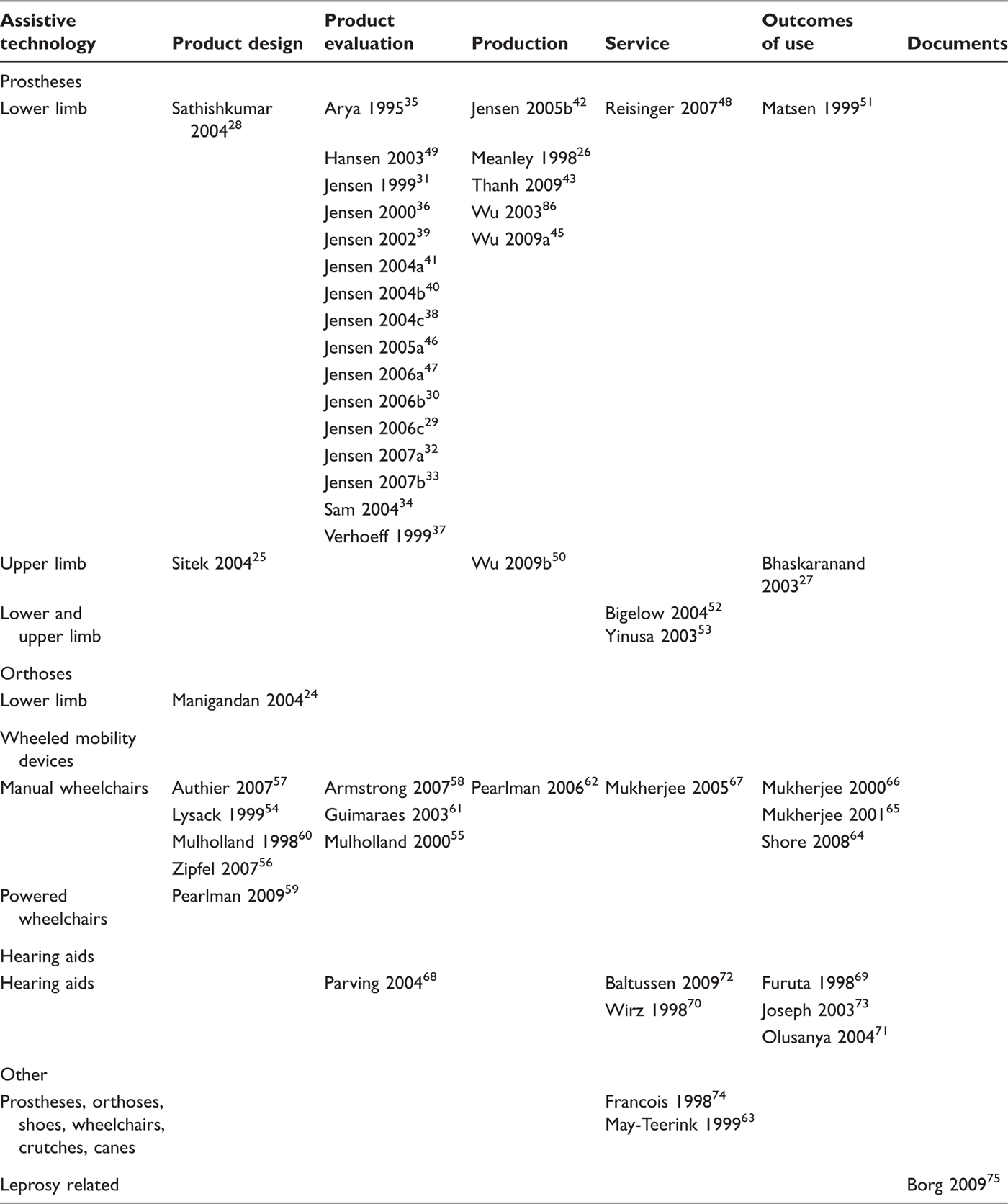
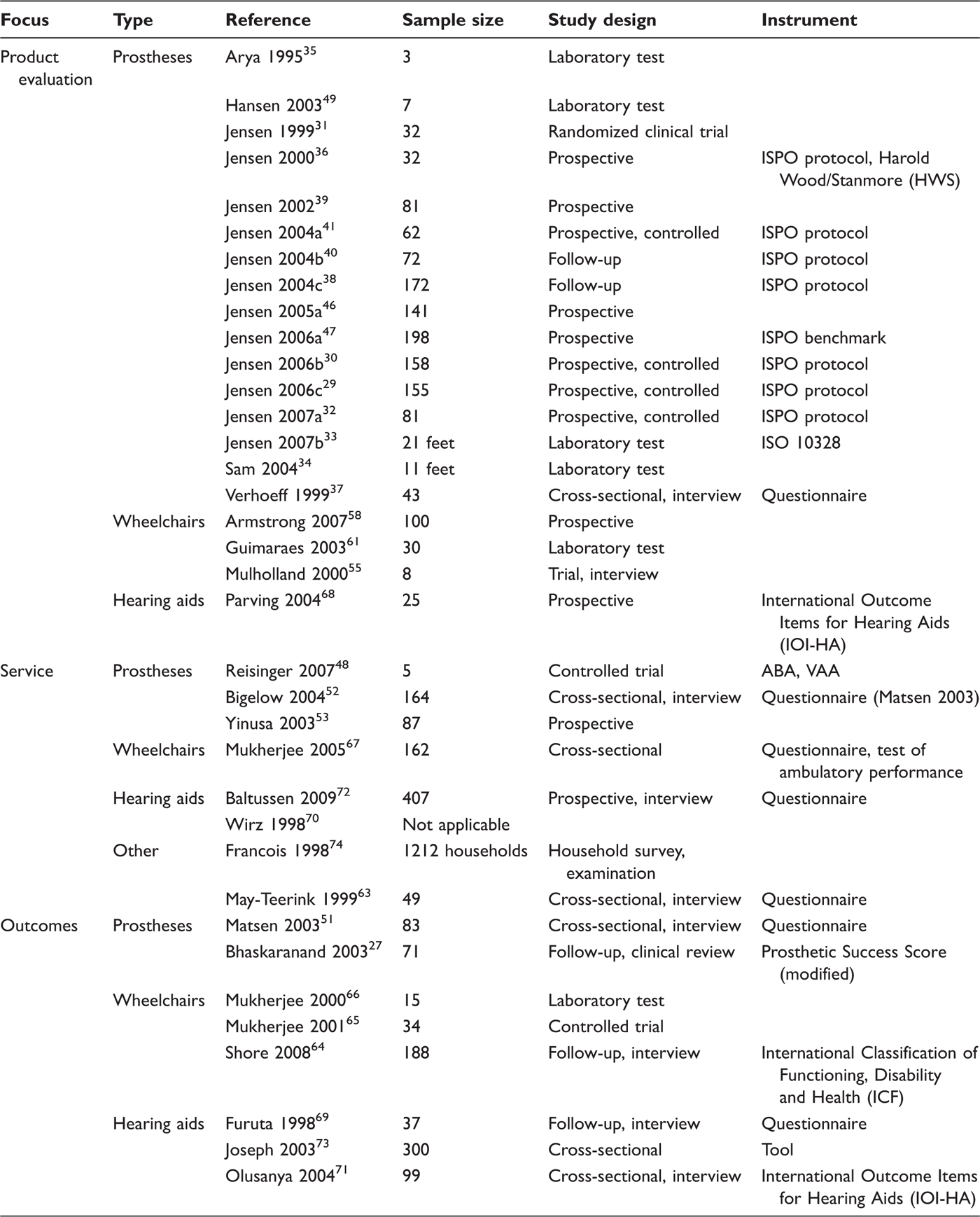
Identified articles were categorized based on the type of assistive technology and the focus of study. Six focus areas were used: product design, product evaluation, production, services, outcomes of use, and documents. As the studies covered various assistive technologies and impairments, and differed greatly in focus, each with its preferred research methods, a complete evaluation of the strength of the evidence was not carried out. However, sample size, study design and instrumentation were compiled for studies on product evaluation, services and outcomes of use.
Results
The initial search yielded a total of 49 articles and the complementary search yielded an additional three articles. Among a total of 52 included articles, 11 were published 1995–1999, 21 were published 2000–2004, and 20 were published in 2005 or later.
Included studies by type of assistive technology and focus of study.
Details of studies on product evaluation, services and outcomes of use.
The main findings according to type of assistive technology are summarized in the following.
Prostheses and orthoses
Different designs of arm and leg prostheses and leg orthoses have been described and evaluated. They should be functional, affordable, durable, easy to fabricate and repair, adaptable to local materials, and culturally acceptable. 25 – 28
An adjustable, temporary, femoral socket prosthesis has been described in the literature and was claimed to be cost-effective. 29
Various foot designs have been evaluated in field contexts and in laboratory settings. 30 – 36 The feet showed wide variation in durability, with two VI models considered to be low-cost, durable, locally manufactured feet. 31 However, out of 21 foot models commonly used in the developing countries, none passed mechanical testing according to ISO standards. 34 There are variations between feet in terms of shock-absorbing capacity, gait performance and mass. 35,36
Prosthetic systems for people with leg amputations have been evaluated. The ICRC polypropylene system for trans-tibial prostheses was reported to be an attractive and durable solution, while two other systems performed unsatisfactorily. 37 – 40 TATCOT resin-wood and ICRC polypropylene trans-femoral systems provided what was considered clinically and technically acceptable, while the outcome of another system was unsatisfactory. 41,42 Poor outcomes are attributed to inadequacies in the construction, material and socket fit, and in the training of involved personnel. 39 – 41
Arm prostheses should preferably be of light weight. 26
Suggestions to improve production capacity include enhancing the productivity, efficiency and quality of services, and increasing the number of prosthetists through training programmes. 13 Different methods to meet the needs for cost- and time-efficient fabrication of sockets have been developed. The CIR casting system using micro polystyrene beads contained in a thin bag appears to provide a better fit than plaster of Paris casting and sand-casting. 43 – 46 To measure the quality of leg prostheses a benchmark has been developed. 47,48
A comparison of three systems for á priori alignment indicated that all of them have the potential for application in outreach prosthetic services. 49 Building alignment into a prosthesis without special hardware has been suggested for developing countries. 50
A fabrication process for making low-cost trans-radial sockets using recyclable plastic soda bottles has been described in the literature. The sockets can be used for stump care or incorporated with terminal devices. 51
People in Vietnam were relatively satisfied with prosthetic treatment although their leg amputations led to departure from previous careers, inability to perform rigorous physical activities and difficulties with social interactions. 52 A study of the situation of people with amputations in Haiti revealed that only one quarter of 164 interviewees had ever had a prosthesis due to inaccessibility and unaffordable services. Existing workshops were limited in their scope of services due to insufficient supplies and inadequately trained personnel. 53 Delay in fitting of upper limb prosthesis seemed to have no correlation with successful rehabilitation. 28 However, poor prosthetic services can lead to unsatisfactory results. 54 Discrepancies in care between demographic groups and between different regions have been noted. 52,53
Wheeled mobility devices
Detailed designs of manual and powered wheelchairs developed for various purposes have been reported, sometimes along with their evaluation. 55 – 60 Wheelchairs need to be affordable, rugged and suited to manoeuvring over diverse terrain, and should meet the individual’s safety, functional, social, geographical and cultural needs. 58,61 To improve safety and comfort, a low-cost wheelchair cushion with better pressure distribution than a foam cushion has been designed. 62 Involving end users in design and evaluation is crucial. Function and quality of life are paramount and should not be overtaken by technical issues. 56
Collaboration between countries in designing and testing wheelchairs has been documented. 57 Reports indicate that the transfer of technology is difficult. 55,57,60
Considering the need for wheelchairs, the problems in their provision are enormous. As a complement to charities and local small-scale manufacturing, increased large-scale domestic production and import may be necessary if supply is to meet demand, maintain high sustainability and achieve maximum impact. 63
The use of mobility devices such as wheelchairs, crutches and canes improves mobility, health and quality of life, and users with better mobility seem to get better opportunities. 64,65 In developing countries quality of life may be a more important consideration in the provision of assistive technology than increased independence. 61 Physiological outcomes of wheelchair use indicate that arm-crank propulsion is useful for long-distance rides while hand-rim propulsion is suitable for short-distance ambulation. 66,67
To reduce negative effects of wheelchair use and high abandon rates, it is important that users are properly assessed. 68
Hearing aids
Low-cost hearing aids meeting WHO requirements are produced, although they are not readily available to everyone in need. Solar-powered hearing aids have been developed to reduce the need to replace batteries. 69 – 71
Aural rehabilitation seems to be feasible and effective in enhancing activity and participation for people with hearing impairments. 72 Estimates in India indicate that both passive screening and fitting of hearing aids at the tertiary care level, and active screening and provision of hearing aids at the secondary care level, are cost-effective. Active programmes were slightly more costly but were able to achieve a higher coverage. 73
Community-based rehabilitation (CBR) has been suggested as an effective strategy to reach children with hearing impairments. 71
The International Outcome Inventory for Hearing Aids (IOI-HA) is considered to be a valuable tool to measure outcome of hearing aid use. 72 Hearing aids offer their users high satisfaction and improved functioning. 69,72 Regular use of a hearing aid has a positive impact on the language performance of students. 74
Other issues
With the exception of those requiring lower limb prostheses, a survey in Afghanistan revealed that the majority of people with disabilities were not equipped with the necessary assistive technology. 75 Findings from Uganda indicate that lack of economic means is a primary barrier to assistive technology. 64 Gender differences in access to assistive technology based on financial and cultural factors have been reported. 52,64,75 Not only women but also children were less likely to access assistive technology. 75 The potential of assistive technology to facilitate the activities and participation of people affected by leprosy seems not well utilized. 76
Discussion
Despite being valuable sources of information, conference reports and recommendations, WHO guidelines (e.g. references 10–12 and 77–79) and reviews and overviews (e.g. references 13, 23 and 80–82) were not included in this review, as the intention was to take stock of current, peer-reviewed and published scientific evidence.
An average annual publication rate of about 3.5 articles during the studied period indicates that research on assistive technology in low- and lower-middle-income countries has received very little attention. The scarce literature is dominated by product-oriented research on leg prostheses and manual wheelchairs. Less is published on hearing aids and virtually nothing is published on the broad range of other types of assistive technology and related issues. Thus, there is a general lack of evidence to support effective implementation of the required assistive technology measures of the CRPD, which has been pointed out elsewhere. 83
Reasons for the lack of evidence may be sought not only in limited funding. Actors in this field have focused on developing and implementing strategies to meet at least a fraction of the need for assistive technology rather than publishing in peer-reviewed journals. With few exceptions the scientific community, donors and development organizations have not given priority to this type of research in the past. However, there is a chance that this will change as compliance with the CRPD requires assistive technology research and technical and economic cooperation between countries. To support the human development of people with disabilities, who are overrepresented among the poor yet overlooked in development strategies, 84 the scientific community needs to provide evidence that guides governments and organizations in their efforts to provide assistive technologies, as these can be an effective means to health, education, work and participation in family and community life. 83
The included articles report positive outcomes of assistive technology use in specific areas (e.g. health, mobility and education) and in general areas such as activities, participation, functioning and quality of life. Activities, participation and functioning are defined in the International Classification of Functioning, Disability and Health. 1 There is less consensus on quality of life, as this varies among individuals and their perspectives. 85 This is also reflected in the articles, although none defines quality of life. One article uses quality of life to mean independence in performing activities, level of pain and ability to transport multiple or large objects, 61 while another article associates it with level of difficulty in carrying out tasks. 65
Provision of assistive technology is not about isolated activities such as design or supply of products, or delivery of services. Although research addressing separate components of provision is necessary, there is a growing need for research that applies a system perspective to guide the development of holistic strategies for cost-efficient provision. Countries that are sincere in their attempts to comply with the CRPD will find themselves in a situation where they need to implement measures to ensure the provision of assistive technology at national level. Without a holistic, national plan it is likely that inequitable access will prevail, with significant differences between people living in different locations or having different impairments, and that available resources will not be utilized optimally, as parallel systems to serve people with various needs may be developed or maintained. Also international cooperation – whether economic or technical – needs to support national plans in a coordinated fashion.
With reference to a recent definition of ‘appropriate wheelchair’, appropriate assistive technology should meet the user’s needs and environmental conditions; provide proper fit and support; be safe and durable; be available in the country; and be obtained, and services sustained, in the country at the most economical and affordable price. 12 For many ‘affordable’ means at no cost. 86 However, as already pointed out, safety and function should never be compromised.
Based on the findings and the discussion above, the following recommendations are made to facilitate implementation of the required CRPD measures:
As there are variations in access to assistive technology across genders, ages and disabilities, these perspectives should be considered in the planning, implementation and evaluation of activities. Evidence to guide development of effective policies and legislation is needed as such evidence is scarce. Research and development on design, evaluation, production and use of assistive technologies are still required, particularly in areas not already addressed, e.g. for cognitive and visual impairments. Research on assistive technology to facilitate work and education is required from a human rights perspective as well as to reduce poverty. Research is needed to guide the development of cost-effective strategies that ensure assistive technology is equitably available, accessible and affordable. Opportunities to use CBR in this regard should be explored and documented. To prevent a lack of adequately trained personnel to staff new services, suitable training programmes need to be developed. To guide the utilization of available resources, good quality studies of outcome and cost-effectiveness are greatly needed. Development of strategies and methods for effective international cooperation would facilitate implementation of the CRPD. To comply with the CRPD requirement of undertaking or promoting assistive technology research, governments are recommended to develop indigenous research capacity. Countries that lack necessary resources may consider cooperating regionally or in partnership with established research centres as part of international cooperation. This may generate new and innovative ideas in a field seemingly dominated by researchers from well-resourced settings. Mechanisms to monitor government compliance with the CRPD regarding assistive technology, including research and international cooperation, should be developed and implemented.
Acknowledgments
The authors are most grateful for the reviewers’ thoughtful and constructive comments.
Funding
This work was partly funded by the Swedish International Development Cooperation Agency (SIDA).