
Abstract
Background:
Evidence-based recommendations are lacking for prosthetic and orthotic services in low- and lower-middle-income countries.
Objectives:
The aim of this study was to compare and synthesise findings related to experiences of prosthetic and orthotic service delivery in Tanzania, Malawi, Sierra Leone and Pakistan from the perspective of local professionals.
Study design:
This is a qualitative inductive study.
Methods:
A total of 49 associated prosthetists/orthotists and prosthetic/orthotic technicians participated in individual interviews. The second-order concept analysis was applied to the data.
Results:
Four common themes emerged: low awareness and prioritisation of prosthetic and orthotic services; difficulty managing specific pathological conditions and problems with materials; limited access to prosthetic and orthotic services; and the need for further education and desire for professional development. A further theme was unique to Sierra Leone: people with disabilities have low social status.
Conclusion:
Local professionals felt unable to deliver high-quality prosthetic and orthotic services. Prosthetic and orthotic education needs to be adjusted to various countries’ regulations to be recognised as allied health professions. Rehabilitation and prosthetic and orthotic service delivery need to be further integrated in low- and lower-middle-income countries’ regular health systems to increase effective person-centred rehabilitation and to address governments’ low awareness and low prioritisation of prosthetic and orthotic services.
Clinical relevance
The results can inform international guidelines and curriculum development for associate prosthetist/orthotist education to better prepare graduates for the clinical scenario and attempts to improve prosthetic and orthotic service delivery programmes in low- and lower-middle-income countries.
Background
To meet the requirements of the Convention on the Rights of Persons with Disabilities (CRPD), 1 the quality of prosthetic and orthotic services in low- and lower-middle-income countries must be improved. Lower-limb prostheses and orthoses and spinal orthoses, on the priority-assistive technology list of the World Health Organization (WHO), 2 have been identified as necessary to maintain or improve an individual’s functioning. These assistive technologies need to be available at a price the community or state can afford. 2 Assistive technology, including prostheses and orthoses, should meet people’s needs, personal goals and preferences. 3 Little research, including outcomes related to the provision of orthotic devices4,5 and related service delivery,6,7 is available from low-income countries. Most studies have been directed towards evaluating specific products.4,8,9 A scoping review confirms the scarcity of research into prosthetic and orthotic services and the education of prosthetists/orthotists in low-income countries. 10 As evidence-based studies are lacking for prosthetic and orthotic service delivery for low- and middle-income countries, recommendations are often based on small groups of international experts where the local professionals have limited representation. Aggregation of findings from several studies that lead to common themes increases the generalisability of the findings, 11 which can be useful in development or updates of international guidelines for education and human resources for prosthetic and orthotic service delivery.12,13 The aim of this study was to compare and synthesise findings related to experiences of prosthetic and orthotic service delivery in Tanzania, Malawi, Sierra Leone and Pakistan from the perspective of local professionals.
Methods
Study design
This is a qualitative inductive study design using the second-order concept analysis to aggregate subthemes 11 that emerged across three qualitative datasets used for previous studies14–16 on professionals’ experiences of prosthetics and orthotics in Tanzania, Malawi, Sierra Leone and Pakistan into themes.
Settings and sampling
Participants were staff responsible for providing prosthetic and orthotic services. In Tanzania, Malawi and Pakistan, participants were associate prosthetists/orthotists whose training involved 3 to 4 years of education and clinical responsibility for patient evaluations and the design and production of prosthetic and orthotic devices. In Sierra Leone, participants were prosthetic and orthotic technicians.12,13 These technical staff have either an apprenticeship-style training or 2 years of formal training with a focus on the fabrication of prosthetic and orthotic devices.
Purposive sampling was used to ensure a broad variety of associate prosthetists/orthotists and prosthetic/orthotic technicians working in different countries representing variation in relation to having a prosthetist/orthotist education in the country or not, history of complex emergency, dominating religion and level of development.
The sample include both sex and different employment situations: private practice, governmental institutions, teaching institutions, international and national non-governmental organisations, the international workforce, people in the process of completing further studies and the unemployed. Data on the participants are presented in Table 1.
Overview of the studies, design, sample and participant characteristics.
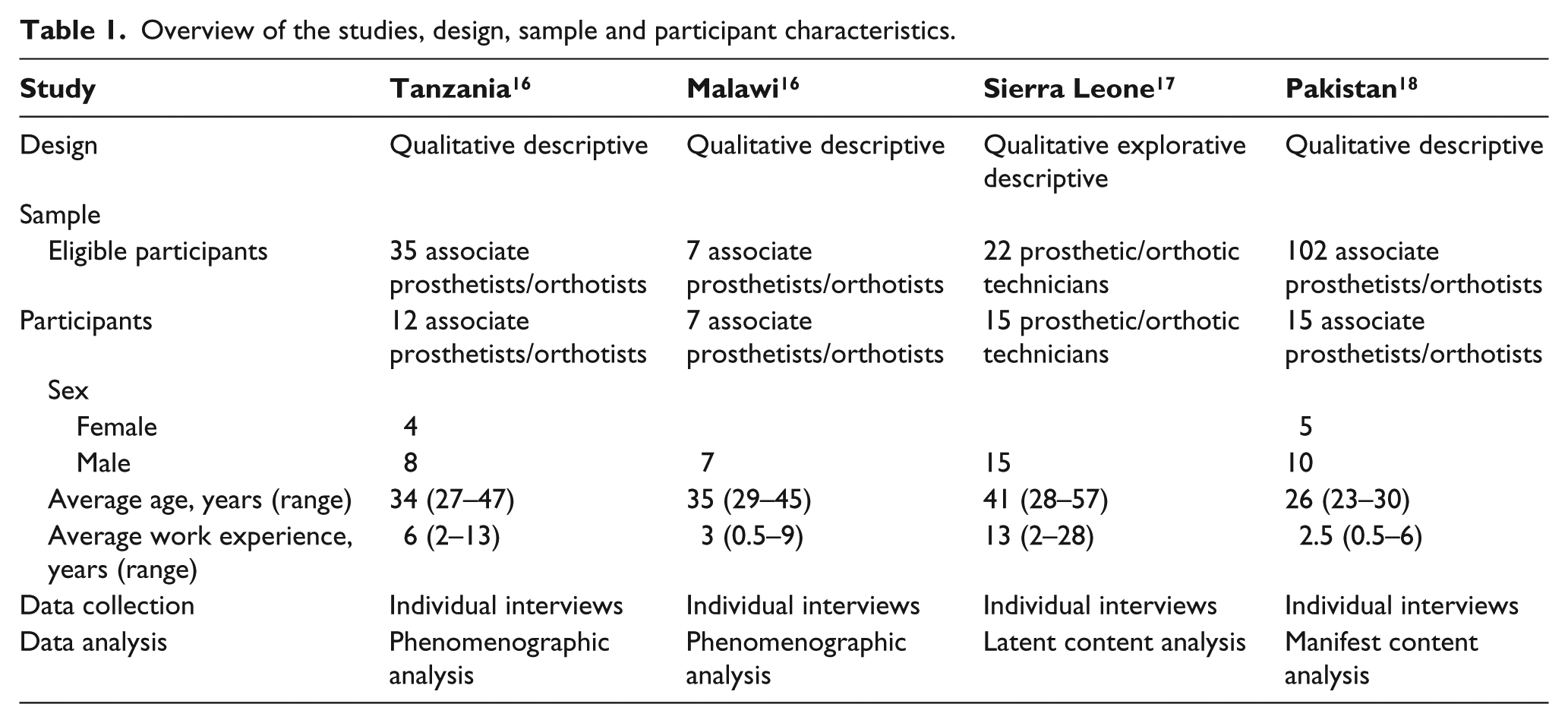
In total, 49 associate prosthetists/orthotists and prosthetic/orthotic technicians participated from Tanzania (n = 12), Malawi (n = 7), Sierra Leone (n = 15) and Pakistan (n = 15) (see Table 1).
Interviews
Individual interviews were conducted in English at the rehabilitation centres where the participants worked. The rehabilitation centres were located within major cities in all countries; in Tanzania and Pakistan, a few centres were also located in smaller cites serving rural areas. An interview guide with open-ended, broad and general questions was used to ensure that participants were encouraged and able to express their full views of the situation.
Data analysis
The qualitative data were analysed for each country. Phenomenographic analysis14,15 was applied to the Tanzania and Malawi data. 16 Qualitative content analysis19,20 was applied to the Sierra Leone 17 and Pakistan 18 data. All datasets had similar research designs, participants, interviewing procedures and data analysis, although phenomenographic analysis was used only for the Tanzania/Malawi study and abstraction level of the content analysis was higher in the Sierra Leone study than in the Pakistan study. The analytical approach in this study was the second-order concept analysis to aggregate 11 subthemes that emerged in the three qualitative datasets used for previous studies14–16 on professionals’ perceptions and experiences of prosthetic and orthotic service delivery in Tanzania, Malawi, Sierra Leone and Pakistan into aggregated themes. Comparisons of similarities and differences and syntheses of the data from all four countries generated aggregated themes. Data were analysed by the author, using Microsoft word.
Results
Prosthetic and orthotic service delivery
Four aggregated themes common to all four countries and one theme unique to Sierra Leone emerged in relation to prosthetic and orthotic service delivery in those countries; subthemes are presented in italics in the text (Table 2).
Common and unique themes in Tanzania, Malawi, Sierra Leone and Pakistan.
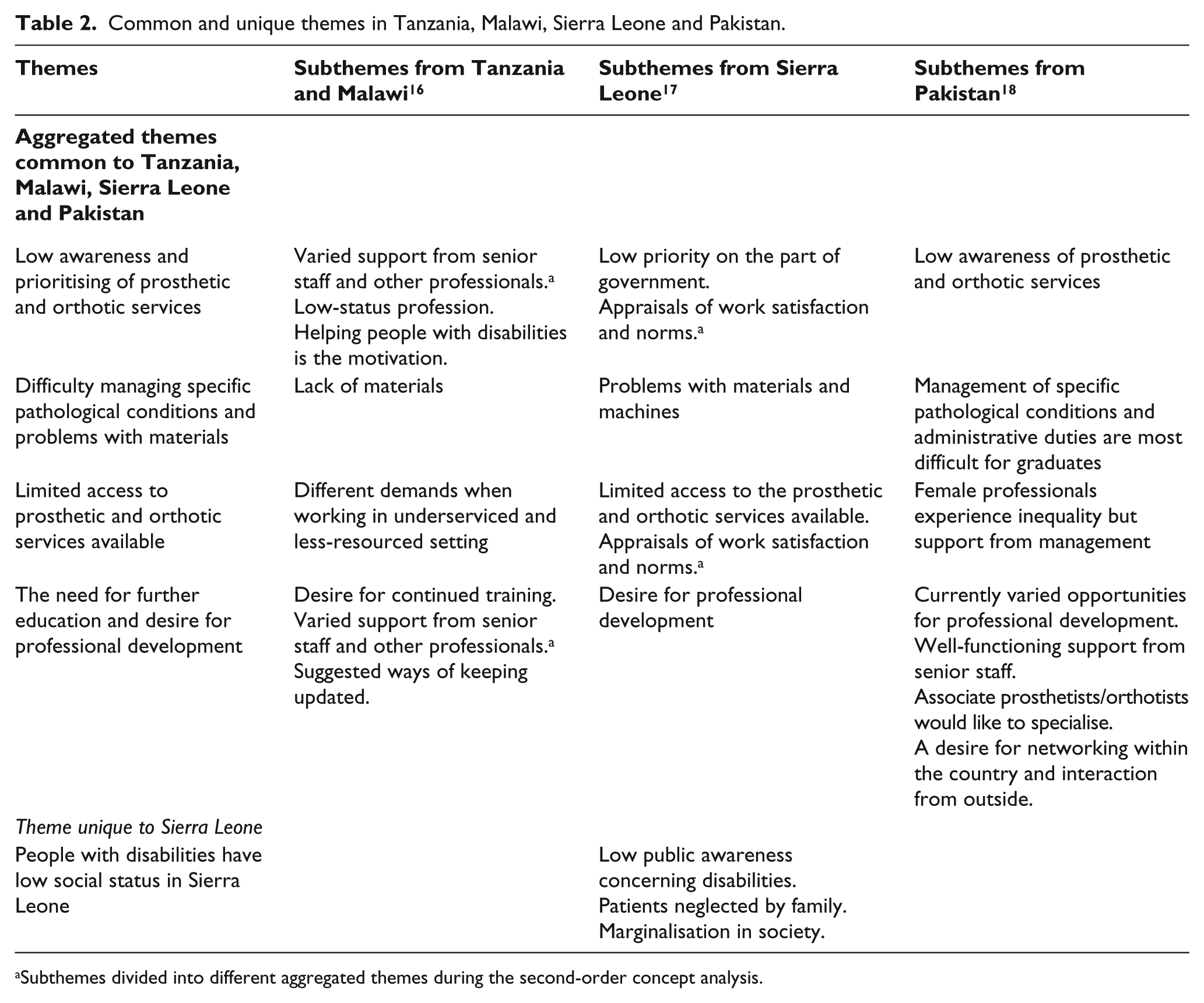
Subthemes divided into different aggregated themes during the second-order concept analysis.
Aggregated themes common to Tanzania, Malawi, Sierra Leone and Pakistan
Low awareness and prioritising of prosthetic and orthotic services
The prosthetic and orthotic professionals who participated perceived that other health care professionals and the general population had poor knowledge about rehabilitation and prosthetic and orthotic service delivery in all four countries. There was low general awareness of the services prosthetic and orthotic workshops could offer, especially in rural areas. Participants called for increased dissemination of information about available services through referral systems, increased availability of community-based rehabilitation workers in rural areas in Sierra Leone, and seminars for health care professionals in Pakistan.
In Tanzania, increased teamwork with support from other professionals and senior staff was perceived as a possible way to improve services for patients. The profession was described as a low-status profession in Tanzania, and Malawian participants reported low salaries, no insurance for work injuries and few employment opportunities. Despite low prioritising of prosthetic and orthotic services in Tanzania, Malawi and Sierra Leone, participants reported that helping people with disabilities is motivating, to fabricate assistive devices facilitate that ability to walk gave them joy and a deep sense of meaning. Participants in Sierra Leone expressed appraisals of work satisfaction, and those who had personal experience of a disability expressed empathy for their patients and were highly motivated to provide the best possible service. They also presented norms that services were distributed unequally between different target groups.
In Sierra Leone, participants experienced a low priority on the part of the government and doubted the government’s ability to independently sustain rehabilitation services that could fully support poor people or to provide funding for appropriate materials or staff with the skills to run rehabilitation centres and empower people with disabilities. Concerns were also raised about charges imposed upon patients for prosthetic and orthotic devices, low salaries for staff and low transparency offered by rehabilitation centre management. The government had taken over parts of the services at the time of the study, but participants expressed the view that non-governmental organisations were needed to provide financial support, materials and assistance.
In Pakistan, there was low awareness of prosthetic and orthotic services, and surprisingly few associate prosthetist/orthotist positions were available in government hospitals. It appears that these institutions mainly employ personnel with no formal education, and participants stressed that trained associate prosthetists/orthotists should provide prosthetic and orthotic services.
Difficulty managing specific pathological conditions and problems with materials
Participants in Tanzania, Malawi and Sierra Leone described lack of materials as an obstacle to delivering services.
In Sierra Leone, participants expressed problems with materials and machines and were not satisfied with the quality of local materials for fabricating prosthetic and orthotic devices. They perceived a need for better machinery and more reliable electricity to provide high-quality service but reported that International Committee of the Red Cross polypropylene technology worked well.
Participants in Pakistan reported that management of specific pathological conditions and administrative duties were most difficult for graduates. Participants felt well prepared to provide appliances to persons with polio or a trans-tibial amputation. Major concerns were expressed about managing cerebral palsy, upper-limb conditions, spinal injuries, complications of diabetes, trans-femoral amputations and evaluating patient outcomes after fitting devices.
Limited access to prosthetic and orthotic services
Participants reported patients’ problems in accessing rehabilitation services in Tanzania, Malawi and Sierra Leone. This mainly concerned patients living in the provinces, but also some who lived locally and could not afford transport to rehabilitation centres.
In Tanzania, participants described different demands when working in underserviced and less-resourced settings. Participants struggled in rural workshops to provide services to long-neglected patients with complex needs. Patients often struggled to pay for assistive devices and travel, and many could not return for adjustments or repairs because they live far away.
In Sierra Leone, participants expressed limited access to the prosthetic and orthotic services available and were hesitant to begin making a device for someone from far away, because they might not be able to come back for a delivery appointment. Outreach services and follow-up programmes were suggested as a means of providing access to services for rural patients. Other participants were especially dissatisfied with the quality of prosthetic and orthotic services delivered by outreach and their limited opportunities to follow up with their patients. Access to services was also limited by hidden fees that poor patients could not afford, as some staff requested extra money from patients to allow them to receive services. Women were often dependent on their husbands for funding for transport and therefore had less access to services than men. Participants emphasised that patients were dependent on their appliances to move, but that some patients could no longer access services because these were no longer free of charge.
In Pakistan, female professionals experience inequality but support from management. Pakistan had female associate prosthetists/orthotists, who acted as good examples, but felt that the profession was still only for men. Some of the male participants agreed that both men and women are needed in the profession, especially since many female patients would feel ashamed if a male prosthetist took a cast of them.
The need for further education and desire for professional development
In all four countries, participants described how they struggled after graduation to provide prosthetic and orthotic services to patients with specific diagnoses. Participants expressed a desire for further training in orthotics and to work towards a bachelor of science or a master’s degree in prosthetics and orthotics to improve services.
In Sierra Leone, the participants had a desire for continued training in elementary prosthetic and orthotic theory. They were satisfied with the on-the-job training they had received from international prosthetic and orthotic experts and the few local associate prosthetists/orthotists with university-level education. The desire for professional development was related to the participants’ wish for better recognition of the profession and improved patient satisfaction.
In Pakistan, participants described varied opportunities for professional development – some of the male participants wanted to work abroad, while the women expressed a desire to return to the Pakistan Institute of Prosthetic and Orthotic Sciences to improve the school and supply the skills and knowledge that are currently lacking.
Participants in Tanzania and Malawi described feeling confident when they started to practice what they learnt after graduation. Participants appreciated well-functioning support from senior staff in all four countries, but it was not always available and participants expressed a desire to have someone to work beside. International exchange programmes, short courses, the Internet, preparing to teach others, discussions with colleagues, and short-term international and national expert support at rehabilitation centres were described as suggested ways of keeping updated.
In Pakistan, the associate prosthetists/orthotists would like to specialise in specific areas, including gait biomechanics, new technologies, orthotics for cerebral palsy and polio, upper-limb prosthetics, spinal orthotics, research and management. Participants had a desire for networking within the country and interaction from outside to facilitate the exchange of ideas.
Theme unique to Sierra Leone
People with disabilities have low social status in Sierra Leone
The participants in Sierra Leone reported low public awareness concerning disabilities and that traditional beliefs tended to underpin understandings of the cause of disability in families of those with a disability and in the general community. Polio was often considered the result of witchcraft, or the will of God, and a child with disability was considered a punishment for the bad behaviour of parents, while amputations are generally assumed to be related to war or accidents. People with disabilities were described as living in poverty and having very limited opportunities in society. Participants reported low societal acceptance of deformities and their concern that people with disabilities did not have access to the services they deserved. Traditional beliefs were seen as a barrier that often delayed patients seeking medical care in favour of traditional treatments. Participants perceived that education about the underlying cause of disabilities could increase societal acceptance of people with disability. Assistive devices were seen as a way to give people with disabilities the opportunity to contribute to society. Participants indicated many disabled children had been neglected by their family to beg on the streets and that most were held in low esteem in their village and sometimes lived in danger. Participants attributed these children’s low status to traditional beliefs about disabilities and the children’s abandonment to their inability to contribute to the household. The neglect of people with disabilities by their families also complicated the provision of rehabilitation services. Participants perceived that families and extended families needed more knowledge about disabilities and they also needed support to take care of family members with disabilities. In general, people with disabilities were marginalised in the society, they were held in low esteem and seen as useless or even evil. Participants expressed their wish that people with disabilities should have access to schools and employment to be able to leave the streets and live in a house and concern that such people were not protected by the law. Skills training for people with disabilities was also suggested to reduce their poverty and increase their access to services.
Discussion
Associate prosthetists/orthotists from Tanzania, Malawi and Pakistan and prosthetic/orthotic technicians from Sierra Leone felt unable to deliver high-quality prosthetic and orthotic services and desired opportunities for professional development. Governments’ low awareness of the needs of people with disabilities and low prioritisation of prosthetic and orthotic services were identified as barriers to providing effective rehabilitation. In Sierra Leone, people with disability needed to be included and supported at different levels within their families and in society in general.
Rehabilitation and prosthetic and orthotic services should be integrated in the health system 21 and be recognised as part of health services. 22 The findings indicate that other health care professionals have poor knowledge of rehabilitation and prosthetic and orthotic service delivery in Tanzania, Malawi, Pakistan and Sierra Leone. Associate prosthetist/orthotist training was seen as low status in Malawi and Tanzania and was poorly recognised in Sierra Leone. This indicates that much work is needed to meet the WHO standard that health care professionals, especially rehabilitation professionals who provide treatment relevant to prosthetic and orthotic services, should have adequate knowledge about prosthetics and orthotics. 22 To facilitate the sustainable inclusion of prosthetic and orthotic services in low- and lower-middle-income countries’ health care and education systems, prosthetic and orthotic education should be aligned with national and international standards for allied health professionals. 22
Prosthetic and orthotic services should be accessible to all who need them irrespective of age or gender, 22 living in rural areas or struggling with poverty. The training and employment of female clinicians is important, especially for the provision of prosthetic and orthotic services for women in Pakistan. 23 A survey of all amputees visiting a rehabilitation centre in Karachi showed that 85% of patients were male and only 15% were female. 23 In the discussion, the authors suggested that this might be because men are the financial providers and are subsequently more exposed to the hazards of traffic accidents and work-related injuries. This could, however, also be partly because female patients do not have equal access to rehabilitation services in Pakistan. Female associate prosthetists/orthotists are needed to treat Pakistani women with disabilities. Records on the graduates from the Pakistan Institute of Prosthetic and Orthotic Sciences showed that only 30% of graduates were women. General employment statistics report that only about 30% of women with degree-level education in Pakistan were part of the workforce, 24 indicating risk that female associate prosthetists/orthotists in Pakistan will stop working after a while to stay at home. Findings from Tanzania indicate that rural settings that have been underserviced for many years require highly skilled prosthetic and orthotic personnel to deal with complex cases made more difficult by extended neglect. Complicated prosthetic and orthotic treatment and care of complex cases should be provided by a multidisciplinary team of professionals with complementary skills. 22 New prosthetic and orthotic service units should therefore be established within, or closely linked to, health and rehabilitation service facilities such as district or referral hospitals. 22 Rehabilitative services are required at different levels of the health system to identify needs and enable referral pathways. 21 Poverty affects access to prosthetic and orthotic service delivery. In Sierra Leone, the government has taken over rehabilitation services and introduced small user fees for prosthetic and orthotic services that were previously provided for free by non-governmental organisations; 25 these new fees were identified as a hindrance for people with disabilities living in poverty in Sierra Leone.
Findings from the local professionals indicate their need for further education and desire for professional development; even the International Society for Prosthetics and Orthotics’ associate prosthetist/orthotist training, corresponding to international guidelines for prosthetic and orthotic education,12,13 was not considered sufficient for providing high-quality services. To provide prostheses and orthoses that facilitate people’s needs, personal goals and preferences 3 requires specialists in the field; shifting the task to less educated personnel25,26 risks reducing the quality of prosthetic and orthotic services. The training of professional staff, regardless of their level of education, needs to be of high quality and centred more on delivering the services people actually need rather than any particular products.
Local staff delivering prosthetic and orthotic services reported having difficulty managing specific pathological conditions. To meet WHO standards ‘[p]rosthetic and orthotic services should be provided by adequately trained professionals’, the training needs to include pathological conditions that prosthetic and orthotic personnel will meet in their clinical work in low-resource settings. 22 In Tanzania and Malawi, professionals struggled with complicated cases and cerebral palsy. In Pakistan, diabetes was reported as the second most common cause of amputation, 27 and local staff reported having very limited knowledge of diabetes. Knowledge about managing diabetic patients who require prosthetic and orthotic devices is important, as low-cost technologies are commonly used and associate prosthetists/orthotists must take care to avoid wounding the patient, which would create further complications and reduced mobility. Prosthetic and orthotic education needs to cover the different types of pathologies that affect people needing prosthetic and orthotic services in each country.
Local professionals in Sierra Leone reported that people with disabilities had low social status. This result is confirmed by Chataika et al. 28 who reported that negative societal and cultural attitudes were perceived as the biggest obstacles to inclusion for people with disabilities in Sierra Leone. Negative attitudes and traditional beliefs were strong, especially in rural areas. Previous findings from focus-group discussions indicated that people with disabilities were seen as the products of witchcraft and sometimes as not fully human. 29 People with disabilities in Sierra Leone have been previously reported to have difficulty accessing education, employment and health care. 30 The findings suggest that difficulty also exists in accessing rehabilitation services. The government of Sierra Leone has shown increased commitment to disability issues by ratifying the CRPD in 2011 31 and by passing the Persons with Disability Act. 32 Despite this progress, those with disabilities continue to face discrimination. The CRPD and the disability act are important changes at the policy level, but for real change, the policies must be put into practice at multiple levels of society.
Conducting secondary data analysis on qualitative studies is emerging in many disciplines but best practice is still not very well defined. 33 It is a limitation that the study only included the perceptions of associate prosthetists/orthotists and prosthetic/orthotic technicians. Other local stakeholders such as users, managers and other groups of health care professionals might have different perceptions that are of importance when making recommendations and should be considered in further studies.
Conclusion
The local professionals in Tanzania, Malawi, Sierra Leone and Pakistan felt unable to deliver high-quality prosthetic and orthotic services. Prosthetic and orthotic education needs to be adjusted to various countries’ regulations to be recognised as allied health professions. Additions of locally relevant curriculum can be considered in associate prosthetist/orthotist education to better prepare graduates for the clinical scenario in their country. Rehabilitation and prosthetic and orthotic service delivery need to be further integrated in low- and lower-middle-income countries’ regular health systems to increase effective person-centred rehabilitation and to address governments’ low awareness and low prioritisation of prosthetic and orthotic services. In Sierra Leone, traditional beliefs about the causes of impairment need to be addressed to allow a rights-based approach to access prosthetic and orthotic services.
Footnotes
Acknowledgements
The author thanks Professor Gerd Ahlström for providing methodological advice regarding conducting a qualitative second-order concept analysis.
Author contribution
L.M. (Lund University, Sweden) was responsible for the study design, data collection, data analysis and writing the paper.
Associate Editor: Stefania Fatone
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was obtained from Kilimanjaro Christian Medical College Ethics Committee of Tumaini University, Tanzania, for data collection in Tanzania and Malawi; Handicap International/New Steps Mercy Ships, Prosthetic Outreach Foundation in Sierra Leone; and the Pakistan Institute of Prosthetic and Orthotic Sciences (PIPOS), Pakistan. Written informed consent was obtained from all participants.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.