
Abstract
A tooth’s center of resistance (Cres) is analogous to any free body’s center of mass (CM). However, unlike a free body, teeth are constrained by the periodontal ligament (PDL) and alveolar bone. In orthodontic literature, Cres is a relatively “fixed” point that “barely” shifts in space, and its estimated location is at the coronal part of the root, as it can change slightly due to alterations in the constrained tissues properties. Despite this, the Cres is mistakenly treated as a fixed point with an approximate location. This oversimplified Cres’ view allowed orthodontists to describe a complete physical theory of various tooth movements, like rotation and translation, by single vectors, even though Cres’ precise location is elusive. The article first demonstrates that only fixed-appliance orthodontics utilizes the three basic physical movement types similar to free bodies, namely translation, tipping, and couple, while removable appliances can utilize only tipping. Therefore, it is evident that fixed appliances can only achieve accurate tooth movement by controlling the Cres location and moving it from the root to the slot center back and forth, as needed. The article argues that controlling the Cres location is the key to achieving the highest treatment success. This contrasts with the relatively lower efficiency of removable appliances, including clear aligners.
Introduction
Since the introduction of clear aligners, the success rate of predicting tooth movements compared to the ClinCheck has averaged about 50%, whereas fixed appliances have achieved 100%.1, 2 Consequently, numerous studies have emerged to explore ways to improve this success rate. Increasing the CA teeth’s grip by the attachments has been the most promising solution in enhancing their efficacy. However, it still falls short of the necessary standard, especially the ABO one. Recently, a growing number of finite element method (FEM) studies have examined various parameters, such as overcorrection and overtreatment, in an attempt to improve efficacy. 3 These studies have not yet provided a definitive clinical solution. Some articles even suggest adding additional aligners with different features, like increased aligners’ rigidity, to potentially enhance treatment outcomes, effectively making each treatment a kind of clinical experiment.
Procedure
The number of CA case reports with phenomenal results detailing treatment paths filled with different clinical recommendations, followed by allegedly supplier demands for similar outcomes, is increasing. Those recommendations come mainly from what we believe are key opinion leaders (KOL) who typically display impressive results. 4 However, we presume these results are achieved in private clinics, where the actual procedures remain unknown, as they are the least rigorous on the randomized controlled trial (RCT) scale.
The late concept of a “learning curve” has recently emerged, suggesting that to achieve good results, a significant number of cases must be treated to accumulate experience, shifting responsibility from manufacturers to treating doctors, as the idiom “but in my hands” revives. 5 Companies claim their treatments are AI-based yet provide no clear information on their data sources and how they are used.
The economic CA chain seemingly disregards the current relatively low treatment success rate, supposedly keeping the patients unaware of the 50% CA outcome efficacy. The number of practitioners and patients continues to rise, partly because aligners are a premium brand, another sociological topic ripe for research.
Despite some improvements in aligners, which companies assert are more effective, results have not dramatically changed in the last 25 years. It looks like history is repeating itself since similar debates relating to FA’ exceptional abilities were confronted with removable appliances back in the first half of the previous century. The main four historical issues included the following:
6
Controlled tooth movement: FA allows precise control over all the direction and magnitude of force applied to teeth. This control is essential for achieving predictable and efficient tooth movement, which is more complex or impossible to achieve with removable appliances that, as well, rely on patient compliance. Continuous vs. intermittent forces: FA can provide continuous forces, which are generally more effective for tooth movement than removable appliances’ intermittent forces. Continuous forces allow for more consistent and predictable orthodontic outcomes. Three-dimensional control: FA offers superior three-dimensional control of tooth movement, including tipping, torquing, and rotational movements. This level of control is sometimes unachievable with removable appliances, which typically offer limited movement capabilities, meaning only tipping versus tipping and torque, the outcome of a couple, by FA. Anchorage control: FA provides better anchorage control, which is critical for achieving desired tooth movements without unwanted side effects, which include intra-arch and inter-arch anchorage, which are more challenging to manage and achieve with removable appliances.
The one parameter, namely, the orthodontist’s ability to fully control the center of resistance (Cres)7–10 location by FA to develop all types of tooth movement, as we see it, is missing from the above list and is what this article will unveil.
Orthodontic Novel Biomechanics
Following indepth research, we found that orthodontic biomechanics of FA, which CA companies attempt to replicate to improve their outcome, are based on some fundamental errors. 9 If known to the orthodontists, it might be that the orthodontic world would have been in a different place. We believe that exposing reality, as we see it, is more important than hiding it.
In order to understand what we mean, we have to go back to fundamental physics, which, insofar as we know, did not change from early Archimedes’ and later Newton’s days. We are sure every orthodontist worldwide is or should be aware of the subsequent facts that, as we see it, lie behind orthodontic tooth movements:
Each free body has a center of mass. If a vector goes precisely through the CM, the body translates, while if it does not, the free body tips around the CM and translates in the vector’s direction. If a couple (two identical forces in opposite directions and different planes) is activated on a free body, it does not matter where the couple is on the body; the outcome is tipping around the CM.
Teeth, in the mouth, are not free bodies. Due to the biological restraint (BRest) of the periodontal ligament (PDL) and alveolar bone (AB), a tooth in the jaw has a Cres analogous to the CM of a free body, with all physical terms and calculations related to that point. The distance between the CM of an extracted single-root tooth (as a free body) located in the apical region of the crown and the Cres of the same tooth while in the mouth, located in the root, is about 5 mm. It means that the BRest forces, with a relatively low Young modulus of elasticity (about 2,000 MPa), 11 move the tooth’s CM from the crown to the root in about 5 mm. As long as there is no change in the tooth, as a free body, shape or weight (if, for example, extracted), the CM is in a permanent point, while the tooth’s Cres, (while in the mouth) is an elusive point due to the continuous metabolism of the AB and the PDL that change its features, and as the appliances in-use, fixed or removable, as will be explained later.
From a physical and biomechanics point of view, the Cres, only while being elusive (unstable) during removable appliances treatment, unlike the CM of a free body, negates the possibility of a single vector passing through the Cres, to develop translation.
Therefore, in orthodontics, the available movements are as follows: while using removable appliances, the only movement that can be accomplished is tipping, since the Cres is elusive, however, while using FA, the appliance can control the Cres location, and therefore it can accomplish all three movements, tipping, torque, and translation. It must be mentioned that unlike a free body, where a vector that does not pass the CM develops translation and rotation, in teeth, the restraint force prevents translation. Therefore, only the rotational movement around the Cres is being expressed.
The answer to why orthodontics needs a couple, if it delivers the same outcome as tipping, lies in the levers’ sizes needed to develop identical movements. In the edgewise appliance, orthodontic couples developed within relatively miniature bracket slot dimensions, as this is the only way orthodontics can create a truly effective, long-term, active couple, as defined in physics. It is valid for edgewise systems, while it is different in the Begg system. 6
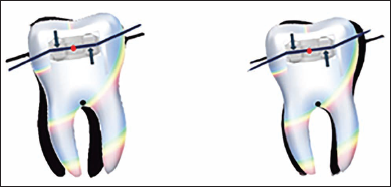
Although CA users claim that couples are a natural part of its biomechanic inventory, we state that no removable appliance can boast this ability, as described above. Does a drawing of two identical arrows in opposite directions on any tooth surface place its rotational center precisely between those arrows? (Figures 1–3). The answer to that question is no, since in biomechanics, every vector should relate only to the tooth’s Cres and not to an imaginary point that moves according to the painter’s (orthodontist’s) wishes. We further believe that in any tooth depiction, the tooth’s Cres location should be as the CM in Physics. Ignoring it might mislead the reason.
An illustration referred to “Orthodontics, Current Principles and Technique,” 2005, by TM Graber, page 1166. According to Sheridan, the two blue vectors, the outcome of two ditches in the CA, develop a more efficient couple than the wire-bracket complex due to a more significant available distance between the vectors in the CA between the vectors then in the bracket. As we see it, this drawing ignores facts related to a couple: if the two blue arrows are equal and precisely in opposite directions, what keeps them identical and in opposite directions, following even minute tooth movement? Why does the appliance “ignore” the Cres (red point), which serves the tooth’s center of rotation and rotates around a point located in the mid-distance between the two arbitrary vectors? If we move the upper arrow gingivally in 2 mm, does it mean the tooth’s rotational point moves accordingly?

An illustration referred to “Principles and Biomechanics of Aligner Treatment” by Nanda, Castroflorio, Garino, and Ojima, Fig. 2.22 page 22. In the figure, where is the center of rotation (COT) of the couple applied to the bracket? Is it amid the bracket or at the natural Cres in the root? As we know from practice, applying a couple at the bracket level in FA moves the root more than the crown. It means that the tooth’s center of rotation is at the center of resistance (red point) amid the bracket (left figure) and not at the biological restraint point (black point), which is between the roots, as we can see in the left figure that the root moves more than the crown, unlike the right figure where the Cres is in between the root, and the root moves as the crown. Does the tooth have two Cres or one?
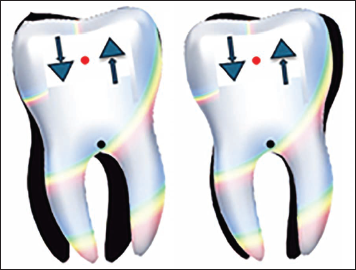
Where is the Crot of the couple applied to the attachments (blue triangular) on the tooth’s crown below? On the left, it is depicted amid the attachments (red point). As the above text explains, the Cres is not a vector location-dependent point. In orthodontics, it depends on the restraint levels of biological bodies in removable appliances and on the physical qualities of the wires and the brackets bonded to teeth in fixed appliances. Therefore, the real movement below is on the left (around the blue point representing the Cres), since the root moves as the crown in the opposite direction.
It seems that redefining the term torque in orthodontics is essential since we found it confusing. The current orthodontic literature, especially the one related to CA, defines every diagonal change in tooth inclination or angulation as a torque change. Andrews (1972)12 defined the orthodontic torque movement as the outcome of a couple, where the apex moves much more relative to the crown’s tip. These were not Andrews’ words; however, they are precisely what he and the profession meant. No other definition is appropriate to describe that orthodontic movement. For example, tipping, although it, as torque, changes the tooth inclination and/or angulation, is far from being orthodontic torque. CS case, the first orthodontist (1895) ever to develop a genuine torque movement in a patient, said, while comparing tipping to torque outcome changes, “What a difference?” 13 The difference is at the movement axis location: in tipping when no external force restrains the tooth, it is always at the natural Cres in the root, and in orthodontic torque, it is about the midst of the FA bracket’s slot, which without any doubt fulfill the movement’s definition. It might sound bizarre, but there is no other way to describe it. As clinicians, we know the clinical significance of torque changes versus tipping changes, and we believe we do not need to add more.
For years, we have known that when performing torque in FA, the tooth’s center of rotation is in the archwire at the bracket. However, we did not realize this involved the Cres movement to this area since any rotation can be expressed only around the Cres of a restrained body as the CM of a free body. (The center of rotation, as described in the literature,9, 10 has nothing to do with the Cres since it relates to the entire treatment movement of the tooth in space and not a momentary movement due to a specific vector). What prevented us, for about a century, from asking this question? Were we really that blind?
We are not sure what the answers are. However, suppose relatively weak restraint forces (about 2,000 MPa) 11 of the AB and the PDL develop the Cres by moving the tooth’s CM about 5 mm apically, we should not be surprised that the restraint forces of the FA’ system, the metal wire, the bonded brackets and the connection to the tooth, which are about 200,000 MPa, 11 can easily move the tooth’s Cres to the wire in the bracket’s slot. 14
The engagement between the metal wire and the bonded bracket builds (or develops) a new mechanical body, and in FA orthodontics, we have to relate to that new body. Can one see a way that can change the traits of RA or CA, and move the Cres to the crowns?
For example, as long as the engagement between the wire and the tooth is active (like following placing a torqued wire in a bracket’s slot), the tooth’s Cres automatically move to the bracket area. Just compare it to the utmost restraint, which means ankylosis, but it is not! (it might be a moving ankylosed unit). However, upon completion of the torque movement, the restraint level previously developed in the bracket decreases. If the orthodontist applied no new torque, the restraint would reset itself to the level where no force is applied, “allowing” the Cres to move back to the root. The 200,000 MPa decreased to only 2,000 MPa during the torque movement. We assume that each orthodontist using the edgewise system felt the restraint forces in his own fingers.
In order to end the biomechanics era, the question raised is, can we use only two movements, tipping and couple, with an equivalent outcome in orthodontics and yet develop all needed movements like tipping, torque, and translation?
The answer lies in explaining the viable, well-known movement—the “walking of a tooth”—in detail to understand the above theory that might enlighten the subject and clarify our opinion.
To explain the superiority of FA over RA, through a physicist’s eyes, we will describe the “walking” from start to finish, highlighting the exceptional capability of FA to achieve excellent treatment outcomes.
One such movement is the ability to close an extraction space between two teeth using a one-time force application by a power chain, resulting in segmental parallelism of the involved teeth.
After an extraction of a tooth (let us say tooth No. 14, the upper right 1st PM) and following the leveling and alignment of the teeth using FA, a relatively rigid round or rectangular archwire is engaged in the system to ensure it does not bend during space closure and does not create high friction that would prevent the teeth from sliding along the archwire. The anchorage is provided by the teeth behind the extracted tooth, 15, 16, and 17 (2nd PM, 1st and 2nd molars).
Pulling back with a relatively heavy power chain from tooth 13 (the upper right canine) toward the posterior anchorage segment causes distal tipping of tooth 13. This tipping movement occurs around the natural, in-root, Cres of tooth 13, while the archwire passing through it at the beginning of the action is not supposed to exert any pressure on its bracket’s slot due to the preliminary leveling and alignment. 6
Once tooth 13 is pressure-free, its natural Cres is located in the root. The distal crown’s tipping of tooth 13 is around the Cres, as it moves the root apex and crown tip in opposite directions approximately equally; the crown moves distally, and the root moves mesially. This movement exerts pressure on the archwire inside the slot of tooth 13, developing a couple.
The couple, in effect, applies pressure to the archwire, increasing the resistance to the sliding as, at the same time, it raises the restraint level of tooth 13 to such a high level that it shifts the tooth’s Cres from its natural, biological root location up to the center of the bracket. The couple builds up as the distally directed power chain force does not stop. When the force stored in the couple exceeds the distal pull force of the tooth by the chain, the couple begins to act, rotating the tooth around the new Cres that shifted due to the restraint from its natural location to the center of the bracket. Indeed, due to its position on the crown, the couple causes the root to move distally, several times more than the crown, mesially, fulfilling the orthodontic torque movement definition.
The couple’s movement continues until the force applied by the chain surpasses the couple’s force, and the archwire in the canine’s slot is released, shifting the Cres back to its root location. The continued force application by the chain will rotate the tooth around its natural Cres, with the root and crown again moving equally in opposite directions, meaning tipping, until a new couple is built in the system, and so on.
The above description is of the combination of couple and tipping in translating the tooth, where the moving Cres qualities in the FA system are the core of this publication. Therefore, there is no need for other movements in orthodontics.
Conclusion
The answer to why the CA efficacy cannot surpass the relatively low efficacy lies in it being a removable appliance and the inability to control the Cres location. To our surprise, the biomechanic-related reasons for that were implanted years ago during the professional discussion between FA and RA followers in the first half of the previous century. However, those reasons disappeared from the orthodontic discourse regarding CA. Many of the parameters related to CA that were and are still in use are not based on physics and belong to nonexisting biomechanics.15, 16 The other answer might be related to the number of lectures, webinars, conferences, and, of course, “publications flood,” that, according to PubMed, more than 12,000 articles in the last 25 years include the words Invisalign or clear aligners, compared to the 8,400 publications in the last 75 years that include the word fixed appliances (480 articles per year versus 112).
The orthodontic torque movement originating from the couple is a movement that, on the one hand, requires the highest possible restraint (200,000 MPa) to move the Cres to the crown so that the axis of rotation is there. On the other hand, it allows for the highest precision in orthodontic treatment results, as the ABO demands for. Since this movement requires clear and precise conditions that no removable appliance, including CA, can achieve, the possibility of increasing the efficiency of CA to match that of FA beyond what has been achieved so far, according to current data, cannot exist in reality.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
There is no patient involvement in the review; therefore, consent is unnecessary.