
Abstract
Objective
To evaluate and assess changes in temporomandibular joint (TMJ), dental, skeletal and soft tissue changes following bimaxillary anchored fixed functional appliance (FFA) treatment of skeletal Class II malocclusion using Magnetic Resonance Imaging.
Methods
The prospective single-arm clinical trial included 15 patients (8 males, 7 females; mean age 15.71 + 1.81years) with Class II Division 1 malocclusion treated with bimaxillary anchored Forsus FRD. Four miniplates were placed bilaterally in maxilla and mandible. Then Forsus FRD L pin module was attached to miniplates without levelling of the arches. Pre-treatment (T1) and post-functional (T2) lateral cephalograms and MRI of TMJ were recorded. A total of 7 parameters were used to assess TMJ in all the 3 planes using MRI. Student’s t-test was carried out to compare pre- and post-treatment-induced changes.
Results
The mandible significantly moved forward (SNB, 3.71 + 0.91°; SND, 3.21 + 1.25°; Pg-OLp, 2.61 + 0.66 mm, p < 0.001) and there was distalizing effect on maxilla (SNA, –0.79 + 0.89°; A-OLp, –0.57 + 0.47mm, <0.001). Mean overjet correction of 4.43mm was achieved, of which 71.8% were skeletal changes. 65% of skeletal changes contributed to molar relationship correction. The forward positioning of mandible seems to be because of condylar and glenoid fossa remodelling, with condyle moving in anterior position within glenoid fossa (3.28 + 2.29) and articular disc moved posteriorly relative to condylar head (2.27 + 1.62°).
Conclusion
Significant skeletal changes and TMJ remodelling were observed with bimaxillary anchored FFA in correcting skeletal Class II malocclusion.
Introduction
Skeletal Class II malocclusion is often characterized by maxillary protrusion, mandibular retrusion, or their combination alongside abnormal dental relationships and soft tissue profile discrepancy. 1 Skeletal Class II due to a retrognathic mandible warrants correction through growth modification by removable or fixed functional appliances (FFAs) in growing individuals. Previous research by Koretsi et al. 2 and Zymperdikas et al. 3 have determined that the correction obtained with these appliances is predominantly dentoalveolar and less skeletal, thus affecting the stability of the results.
With the expanded utilization of skeletal anchorage devices in orthodontics, miniscrews and miniplates have been used previously in conjunction with FFAs with different designs to control the unwanted effects.4–6 However, these designs limited the use of miniplates only on mandibular symphysis and failed to provide substantial evidence to prove the superior skeletal effects attained.7, 8 A recent systematic review 9 also concluded that FFA supported by bi-maxillary anchorage failed to control the proclination of mandibular incisors.
Therefore, it was hypothesized in the present study that anchorage support from both mandible and maxilla would lead to better anchorage control and greater skeletal effects. Since the orthopedic forces applied by functional appliances affect not only the dentition but also the position of mandibular condyle within the glenoid fossa, TMJ remodeling was investigated.
Furthermore, no MRI study has previously attempted to assess the TMJ adaptation following skeletally anchored FFA therapy. Therefore, this study was aimed to evaluate the preliminary changes in TMJ complex and also assess dental, skeletal, and soft tissue changes in the maxillomandibular complex brought about by treatment with bimaxillary anchored FFA.
Material and Methods
The study protocol was approved by the institutional Ethical Committee and is registered under the Clinical Trial Registry. Informed consent was obtained from parents of all subjects at the start of the study.
The prospective single-arm clinical trial was conducted in the Department of Orthodontics and Dentofacial Orthopedics.
Sample Selection
The sample size was calculated based on a significance level of 0.05 and a power of 80%. The power of the study determined that a sample of 13 subjects was required to detect a clinically significant increase in mandibular length with a standard deviation of 0.94 mm and an effect size of 0.7. 5 A final sample of 15 subjects (8 males, 7 females; 15.71 ± 1.81years) was selected among the patients who reported to the department OPD.
The inclusion criteria were (a) skeletal Class II with SNB <78° and SNA = 80°–82°; (b) convex profile giving a positive clinical visual treatment objective (VTO); (c) CVMI stage 4 and 5 (assessed by CVM method using lateral cephalogram 10 ); (d) horizontal or average growth pattern; (e) bilateral Class II/ end-on molar relation; (f) no previous orthodontic treatment; and (g) no clinical signs or symptoms of TMJ disorder. The exclusion criteria were (a) history of TMJ trauma; (b) signs of periodontal disease and (c) systemic disease affecting bone metabolism.
Appliance Design
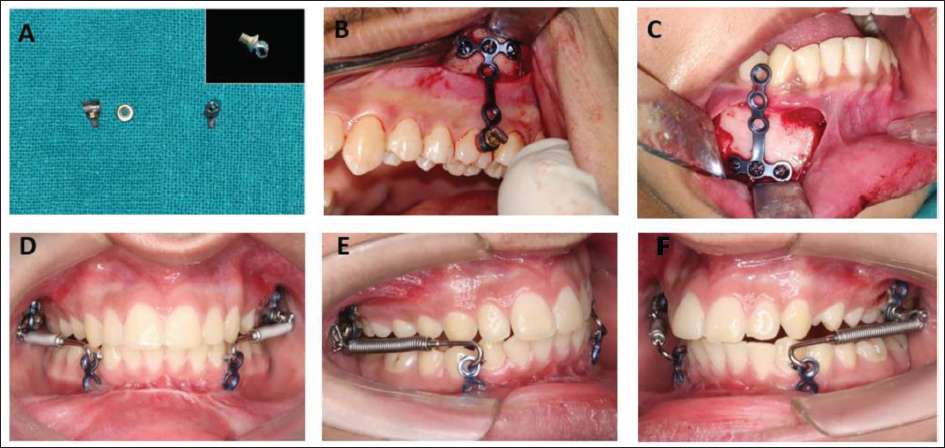
Four “T”-shaped miniplates (S. K. Surgicals Pune, Maharashtra, India) were used as the anchorage plates in maxilla and mandible. For the insertion of Forsus-FRD (3 M Unitek, Monrovia, California, USA) appliance, a headgear tube (0.045 inch) was soldered on the head of S.S. screw (Figure 1a). This screw with the soldered headgear tube was tightened on the last hole of maxillary miniplate with a bolt, such that this screw should come at the level of middle third of the buccal surface of maxillary first molar once the miniplate is fixed on the zygomatic buttress (Figure 1b).
(A) Screw with Soldered Headgear Tube. (B,C) Maxillary and Mandibular Miniplates. (D-F) Intra-oral Photographs with the Forsus FRD.
Methodology
A standardized lateral cephalogram in natural head position and MRI of TMJ with TMJ surface coil for simultaneous imaging of left and right joints were recorded for all the subjects before starting the treatment (T1). MRI scans were taken with patient’s head at right angle to the MRI table. All the surgical procedures were performed by a maxillofacial surgeon under local anesthesia. In the maxilla, two plates were fixed using three 2 × 6 mm screws on right and left zygomatic buttress. Two miniplates were fixed in the region of mandibular canine and premolar bilaterally with three screws (2 × 8 mm). During the surgical procedure, the patient was asked to bite in centric occlusion, and distance was measured from the distal of the headgear tube to distal of the mandibular canine, using the measurement gauge to determine the length of pushrod to be used. A mark was made with a surgical marker to locate the position of the mandibular miniplate during surgery. The miniplates were loaded after 3 weeks of the surgery. The Forsus FRD, L pin module was inserted in the headgear tube attached to the maxillary plate and the mesial hook of pushrod was placed inside the circular hole of the mandibular miniplate (Figure 1 d–f).
The leveling and alignment of the arches was not done before the functional phase, as the Forsus was directly attached to the miniplates. The subjects were observed at an interval of 4 weeks and the appliance was activated by using split crimps (1.5 mm of activation) if required.
The appliance was removed after overcorrected Class I molar and canine relationship was achieved. Standardized lateral cephalogram and MRI-TMJ were recorded (T2) following the pre-treatment protocol. The mean duration of the functional phase was 8.5 + 1.4 months. The same maxillofacial surgeon removed the miniplates under local anesthesia and teeth were bonded with 0.022-inch slot pre-adjusted fixed appliances.
Cephalometric Analysis
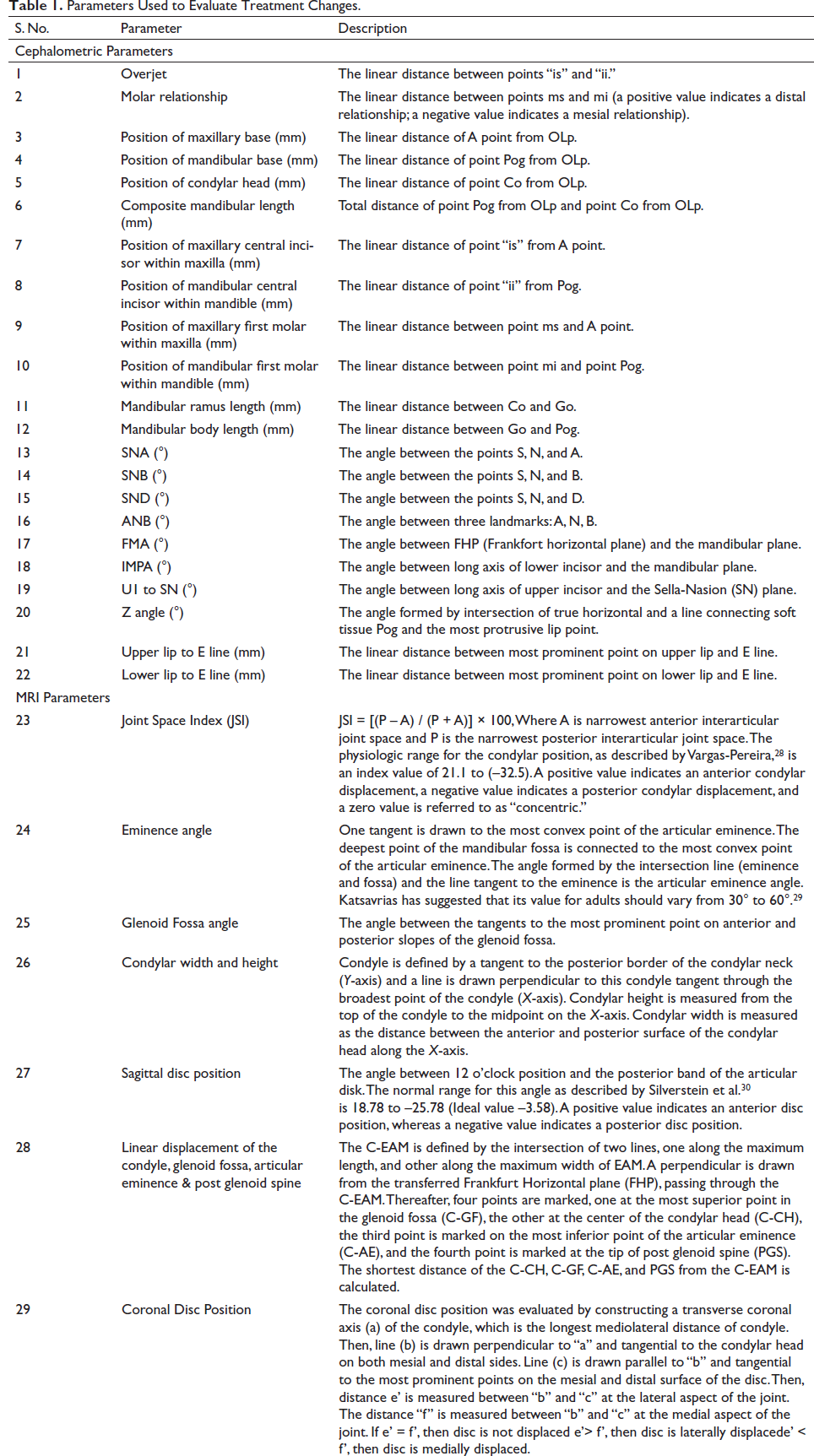
Standardized lateral cephalograms of all the subjects were evaluated using modified Pancherz analysis 11 to assess the skeletal and dental changes by superimposing the tracings (at T1 and T2) on the T-FMN line, with T point as the registration point. Apart from this, variables assessing soft-tissue, incisor inclination, and skeletal divergence were additionally added (Table 1).
Parameters Used to Evaluate Treatment Changes.
MRI Evaluation
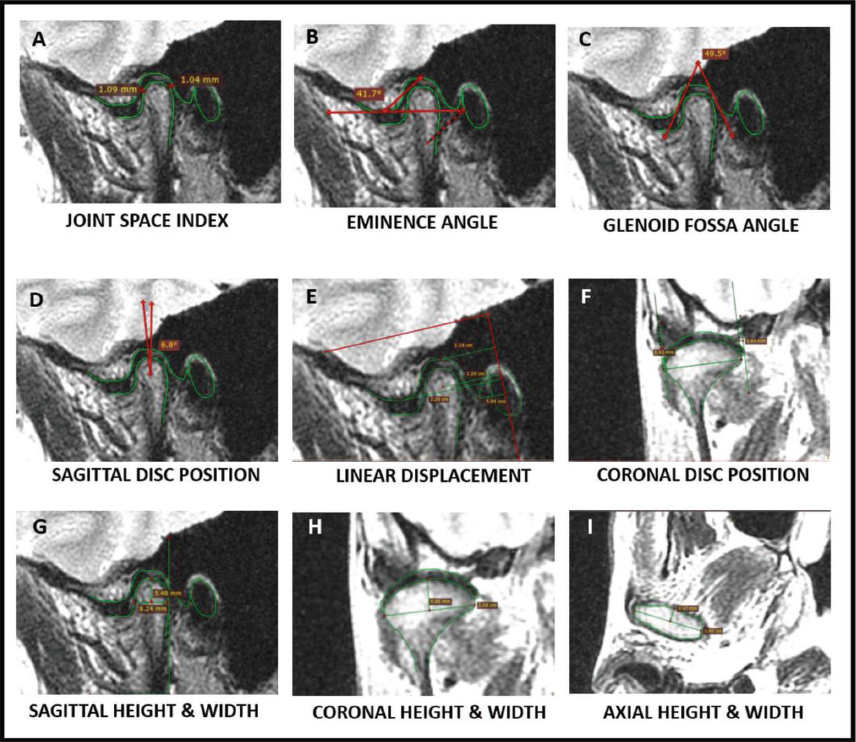
MRI scans of TMJ were recorded with an H Txt VOLMER 3 Tesla (GE, USA) scanner. The images were obtained in maximum intercuspation (closed mouth) and open mouth positions. The MRI protocol included T1 (TR560/TE12.1/FoV 160 × 160 mm) and T2 (TR3000/TE105.9/FoV 160 × 160 mm) weighted spin-echo sequences in coronal, sagittal, and axial planes of 3 mm slice thickness with no interslice gap. Both right and left TMJ were evaluated. All the measurements were done using RadiAnt DICOM viewer 2020.1 software and those sections were chosen that displayed the maximum width of the condyle. The parameters used to evaluate treatment changes are summarized in Table 1 (Figure 2).
Skeletal and Dental Changes Assessed by Modified Pancherz Analysis.
Statistical Analysis
Data analysis was done using IBM SPSS Version 16.0. Quantitative data were expressed as means and standard deviations, while qualitative data were expressed as percentages. Normality of the data was checked by using the Shapiro–Wilk test. Change in the quantitative parameters was assessed for significance using the paired t-test. The analysis of coronal disc position was done using the chi-square test. A p value of <.05 was considered to be significant. All the measurements were repeated twice by the same observer and a second observer after an interval of 1 month, and correlation coefficient values of 0.88–0.92 for intra-rater and 0.91–0.95 for inter-rater reliability were calculated.
Results
Out of 15 subjects, one was excluded due to infection in right mandibular miniplate, accounting for a final sample size of 14 subjects (7 males and 7 females).
Cephalometric Evaluation
Treatment changes of cephalometric measurements, as assessed by paired t-test, are shown in Table 2. The maxillary measurements (SNA, –0.79 + 0.89°; A-OLp, –0.57 + 0.47 mm) exhibited a statistically significant backward movement of maxilla, whereas mandible (SNB, 3.71 + 0.91°; SND, 3.21 + 1.25°; Pg-OLp, 2.61 + 0.66 mm) significantly moved forward. Intermaxillary sagittal relationship improved significantly due to changes in both maxilla and mandible. Also, a significant increase was observed in FMA (0.57 + 0.65°). The angular measurements of upper and lower incisors did not show any significant change, while linear measurements showed a significant backward movement. Facial convexity improved was demonstrated by a change in Z angle (3.57 + 0.76°).
Cephalometric Changes After Bimaxillary Anchored FFA Therapy Assessed by Paired t-test (N = 14).
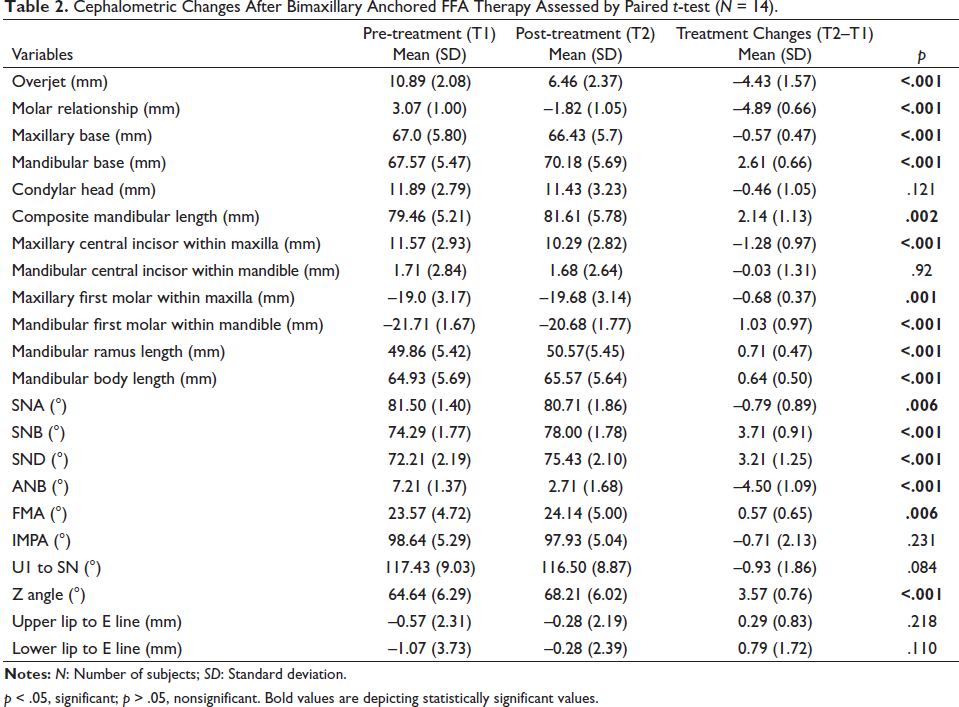
p < .05, significant; p > .05, nonsignificant. Bold values are depicting statistically significant values.
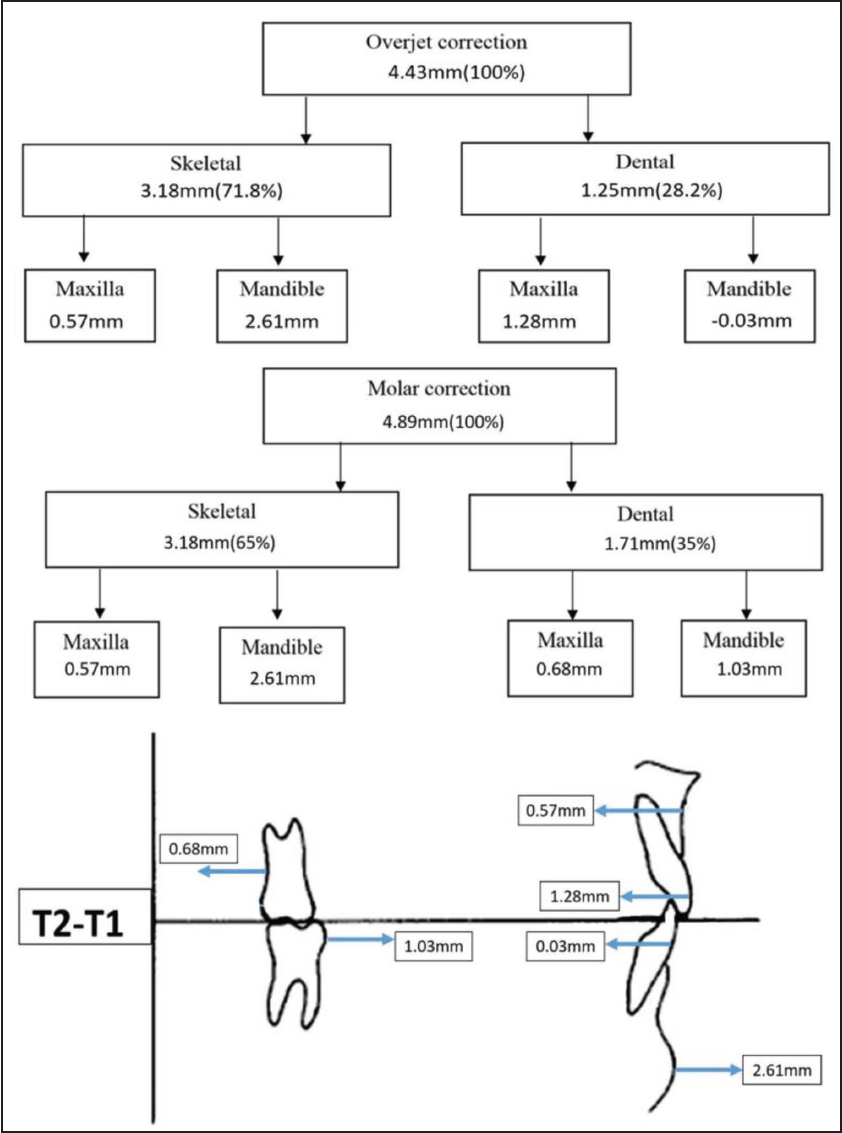
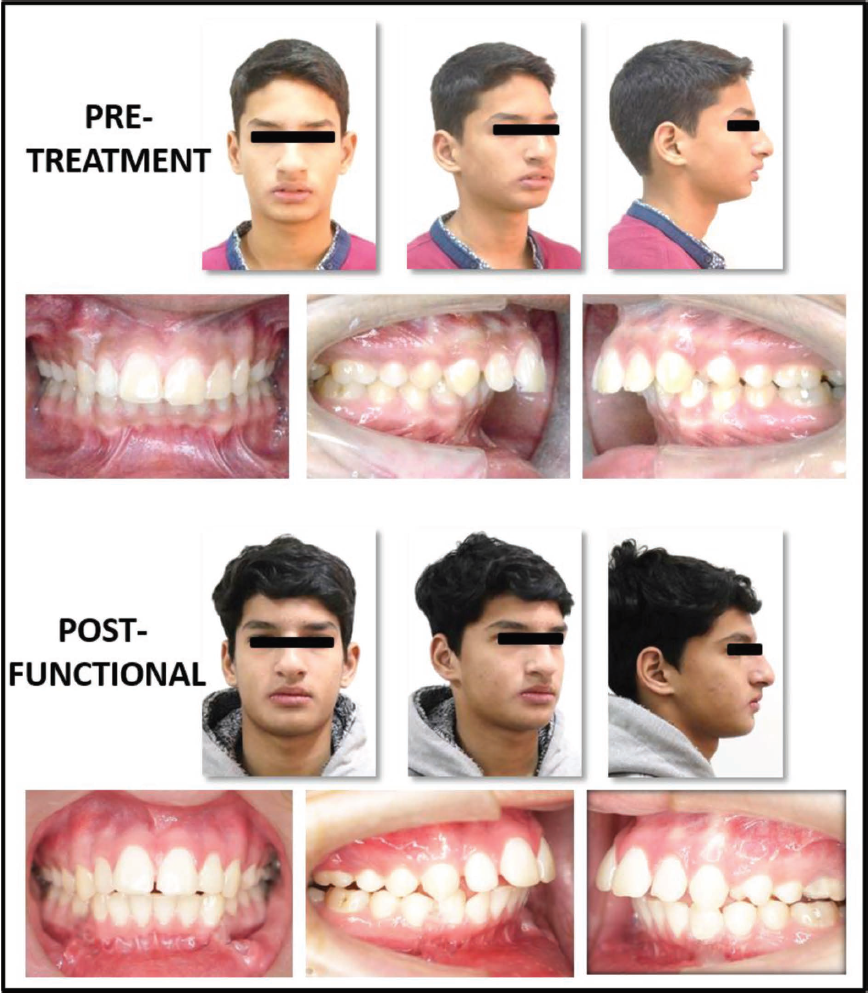
The schematic diagram of maxillary and mandibular skeletal and dental changes assessed by modified Pancherz analysis is displayed in Figure 3. The mean overjet correction was 4.43 + 1.57 mm with a contribution of 71.8% skeletal changes and 28.2% dental changes. The molar relation changed from Class II to Class I, showing correction of 4.89 + 0.66 mm of which 65% was by skeletal changes and remaining 35% was by dental changes. The pre-treatment and post-functional photographs of the patient are depicted in Figure 4.
Parameters Used for MRI Evaluation.
Pre-treatment and Post-functional Photographs of a Patient.
MRI Evaluation
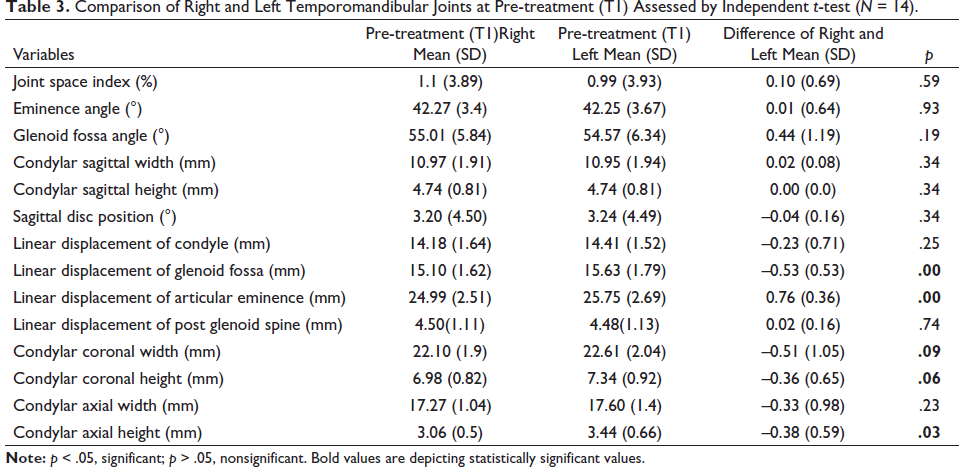
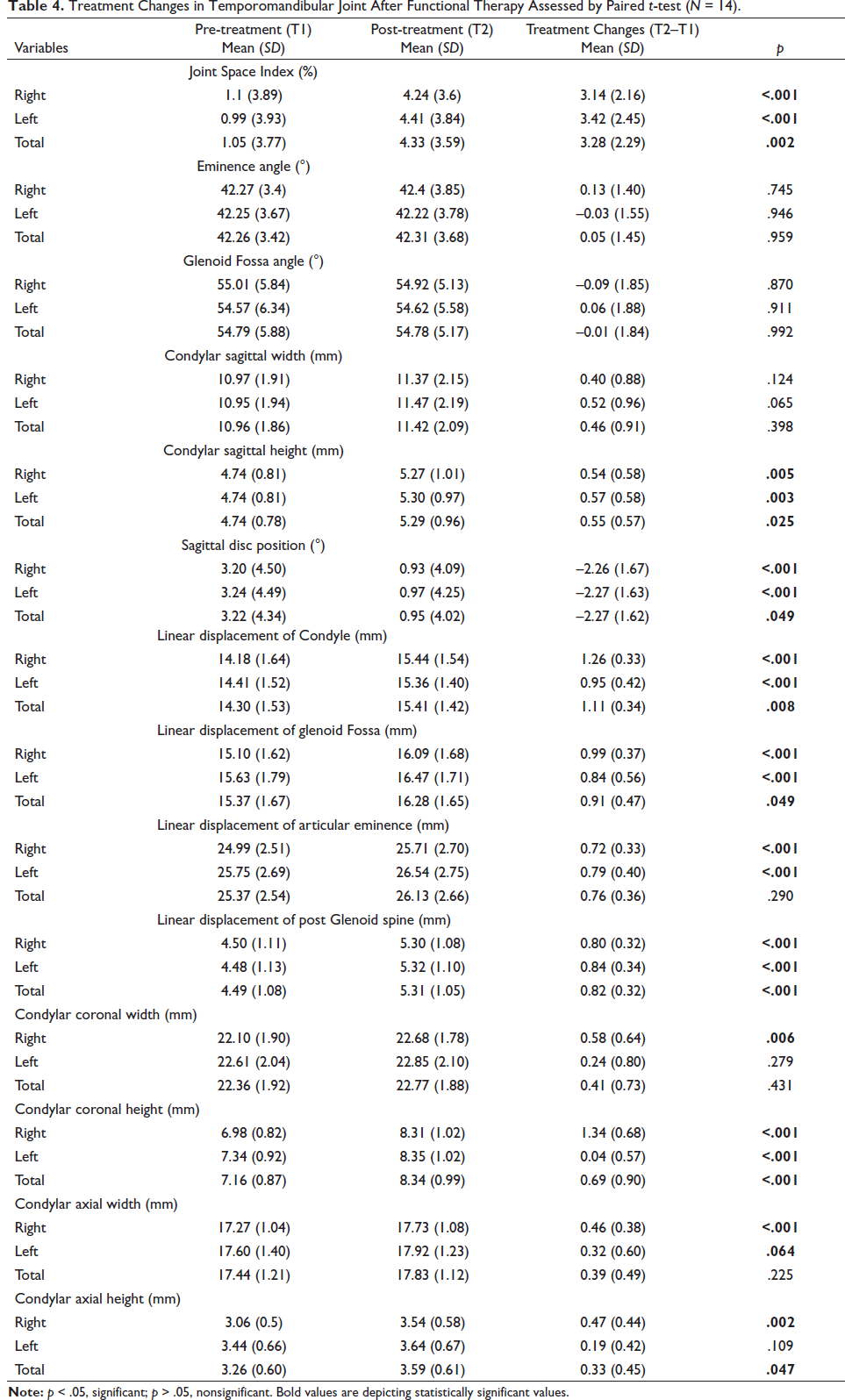
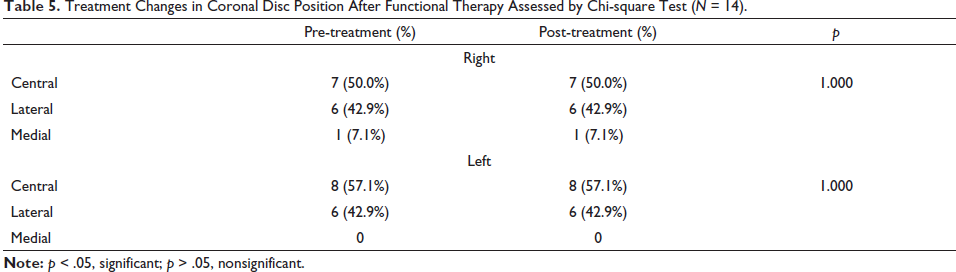
An initial comparison of right and left TMJs at T1 was done by independent t-test (Table 3). All the parameters showed statistically nonsignificant differences (p > .05) between both the joints except for position of glenoid fossa, articular eminence, condylar width and height in coronal section, and condylar height in the axial section (p < .05). Treatment changes in TMJ are shown in Table 4. All the joints showed a statistically significant increase in Joint Space Index (JSI) (3.28 + 2.29), indicating an anterior shift of the condylar position in the glenoid fossa. The significant decrease in posterior band angle (2.27 + 1.62°) indicated a backward movement of the articular disc. A significant forward displacement of the center of condyle, glenoid fossa, and the tip of post glenoid spine was observed. Eminence angle and glenoid fossa angle did not show any significant changes. The condylar height in all three sections exhibited a significant increase, whereas condylar width showed a significant increase in the coronal section of the right joint and axial section of right and left joints. After end of the functional phase T2, coronal disc position did not change relative to the condylar head (Table 5).
Comparison of Right and Left Temporomandibular Joints at Pre-treatment (T1) Assessed by Independent t-test (N = 14).
Treatment Changes in Temporomandibular Joint After Functional Therapy Assessed by Paired t-test (N = 14).
Treatment Changes in Coronal Disc Position After Functional Therapy Assessed by Chi-square Test (N = 14).
Discussion
The correction of skeletal Class II arising due to mandibular retrognathism has been researched extensively over the past decades. The treatment modality varies depending on the age of the patient at the commencement of treatment. The present study aimed at skeletal correction in late adolescents using skeletal anchorage with FFA to limit the dentoalveolar side effects. The design of the appliance fabricated included the application of anchor support from both the jaws unlike the previous studies,5, 6, 12 which had used anchorage only from mandible. As the mandibular repositioning involved adaptive remodeling of condyle and glenoid fossa, MRI was conducted to evaluate and report changes in TMJ, in contrast to the previous studies 13 based on 2D cephalogram.
The commencement of fixed functional therapy without levelling and alignment of the arches was beneficial for the late adolescent subjects nearing the completion of growth. An untreated control group was not included, as it is unethical to leave patients without treatment during late adolescence when favorable treatment effects are expected. In the present study, the included subjects are already in late adolescence, when most of the active growth of craniofacial skeleton is completed. Consequently, it will be highly unethical to leave these subjects without treatment, as it will prevent us from utilizing their residual growth. The only choice of treatment remaining will be a surgical correction of retrognathic mandible, after their growth completion.
Modified Pancherz analysis was used to assess skeletal and dental changes. It is considered as the most suitable method of superimposition in comparison to Ricketts and Bjork method. 14
Maxillomandibular Complex Changes
The analysis revealed greater skeletal effects with bimaxillary anchored Forsus. Overjet showed a significant reduction of 4.43 mm. In agreement with previous studies,5, 6, 13 the overjet correction was a combination of skeletal (71.8%) and dental changes (28.2%). The molar relationship changed from Class II to Class I relation with 65% of skeletal changes and 35% were dental changes. Unal et al. 5 have reported overjet correction with 74% skeletal changes by using only mandibular anchorage. The present study also displayed significant improvement in mandibular position (SNB, 3.71°) and length (2.14 mm), which is similar to the results shown by Kochar et al., 13 who also used bimaxillary anchorage with FFA. There was a clockwise rotation of mandible, which can be explained by the transmission of downward and forward forces of the Forsus appliance, directly to the symphyseal region of the mandible. The appliance had a distalizing force on maxilla (SNA, –0.8°), which is in accordance with the previous study 13 using bimaxillary anchorage.
Regarding maxillary and mandibular incisor positions, no significant change was found after the bimaxillary anchored Forsus therapy. This shows that this modality was able to overcome the biggest disadvantage of the functional appliances, that is, proclination of the lower incisors. Meta-analysis has shown an increase of 7.99° in lower incisor inclination after FFA. 3 While previous studies5, 6, 12, 15 using single jaw anchorage reported retroclination of upper and lower incisors, Elkordy et al. 16 stated that retroclination of the upper incisors creates a lock, restricting the forward growth of the mandible and also applies pressure on the lower incisors resulting in their retroclination. Since the present study uses bimaxillary anchorage, minimal forces were acting on the maxillary dentition due to which there was insignificant change in maxillary incisors inclination, and hence, no change was seen in the inclination of the lower incisors.
The soft-tissue facial profile improved after the Forsus therapy. There was no change in the position of upper and lower lips. This can be attributed to the control in the incisor position, which directly affects soft tissue. Conventional Forsus has resulted in protrusion of lower lips due to flaring of lower incisors. 15
TMJ Changes
The pre-treatment MRIs of a majority of subjects had positive JSI values indicating that condyle was anteriorly positioned within the fossa. After functional therapy, the condylar head shifted more anteriorly within the glenoid fossa with an increase in JSI. The condylar height increased in all three planes after the functional therapy. The right joint showed a significant increase in width in the coronal and axial planes, whereas in the sagittal plane, there was no change in the width. Similar findings were observed by Arici et al. 17 and Elfeky et al., 18 who reported a small increase in condylar dimensions and volume 7–9 months post-functional therapy. These changes are suggestive of condylar growth taking place in the postero-superior direction. On the contrary, Ruf and Pancherz 19 concluded that the condyle gets displaced in a forward direction during treatment but returns to its original position post-functional therapy.
The linear displacement was measured to find out whether the condyle-glenoid fossa complex did actually shift anteriorly from its pre-treatment position. In the present study, it was observed that the center of the condylar head was displaced anteriorly by 1.11 mm along the FH plane.
The center of the glenoid fossa and post glenoid spine also moved anteriorly, indicating a forward remodeling of the glenoid fossa post FFA therapy. These findings are in agreement with those of Kyburz et al. 20 and Gandedkar et al. 21 In contrast to these observations, Kinzinger et al. 22 found no significant differences in the glenoid fossa–condyle relationship before and after treatment.
The contrasting findings can be explained because of the difference in the type of functional appliances used. Furthermore, it has been suggested that semi-rigid FFA (Forsus) should be used for better condylar repositioning post-functional therapy. 20
The pre-treatment position of the articular disc was slightly anterior, as indicated by posterior band angle of 3.22°. The disc was displaced in a posterior direction relative to the head of the condyle after FFA therapy. This posterior displacement of the disc is because of the pull from retrodiscal tissues as stated by Voudoris. 23 The position of the disc did not change with the functional therapy in the coronal section. These findings are similar to those of Kinzinger et al. 24 who reported that the disc shifted posteriorly after appliance insertion and moved to its original position after removal.
The eminence angle and glenoid fossa angle did not show any changes after the treatment, which is in accordance with previous studies.25, 26 However, the annual increase in the eminence inclination is only 1.25°/year 27 ; the functional duration of 8 months may not be sufficient to detect such minor changes.
The greater skeletal effects achieved in the present study can be attributed to the use of anchorage directly from both the jaws. With this modality, we can “jumpstart” with the functional phase, without waiting for levelling and alignment of the arches, and thus, harnessing the growth potential of the late adolescent subjects. Since this treatment modality was successful in correcting Class II in late adolescents and TMJ was capable of growth adaptation, hence, this method helps to evade orthognathic surgery, which remains the only choice of treatment in subjects who are at the end of their growth period.
The limitations of the study are that the findings are based on short-term observations and there was a need for two surgical procedures, for miniplate insertion and removal, making this method invasive in comparison to conventional functional therapy.
Conclusion
The forward positioning of mandible accomplished by the bimaxillary anchored FFA was a result of condylar and glenoid fossa remodeling.
The height of the condylar head increased significantly in all three planes and condylar width showed a significant increase in the axial and coronal planes.
The condyle shifted anteriorly within the glenoid fossa with forward displacement of both the center of the fossa and post glenoid spine.
The articular disc shifted posteriorly in the sagittal plane, whereas coronal disc position remained unchanged.
About 71.8% of overjet reduction and 65% of molar correction was due to skeletal changes, and inclination of lower incisors was maintained.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
The study protocol was approved by the institutional Ethical Committee and is registered under the Clinical Trial Registry (CTRI/2020/01/022858). Informed consent was obtained from parents of all subjects at the start of the study. Trial Registration: CTRI, CTRI/2020/01/022858, Registered 20 January 2020, http://ctri.nic.in/Clinicaltrials/rmaindet.php?trialid=39369&EncHid=70842.68512&modid=1&compid=19
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Scope
This study could not integrate functional and fixed phases, as MRI was required post-functional therapy. However, further studies can prove to be beneficial by combining both the phases, subsequently reducing the treatment duration. Additionally, future studies with long-term follow-ups and a larger sample size are required to determine the stability of the results achieved in the present study.