
Abstract
Background
Mini-screws are valuable devices in orthodontic treatment as they allow effective anchorage. Relocation of a mini-screw may be required due to anatomical limitations.
Objectives
To compare the morphology and surface characteristics of three brands of mini-screws before and after use and to check their viability for reinsertion.
Methodology
Mini-screws of three commercially available brands, Group I: Orlus, Ortholution, Korea, Group II: Absoanchor, Dentos, Korea, and Group III: S.K. surgical, India, were evaluated for the sharpness of their threads and active tip, surface roughness, and surface chemical composition using scanning electron microscope (SEM)–energy dispersive spectroscope (EDS) before and after clinical use.
Results
The sharpness of threads did not differ before and after use in any of the groups. The mean tip deformation values in Groups II and III post-insertion were significantly higher than pre-insertion. The SEM images obtained post-insertion revealed loss of gloss and surface finish with a dull appearance in all groups, but most evident in Group I. EDS analysis post-retrieval shows an increase in the amount of carbon and oxygen in Groups II and III.
Conclusion:
Mini-screw reuse within the same patient is possible if proper recycling is done, and pilot drilling is done to overcome the decreased cutting ability of the tip due to deformation.
Introduction
Orthodontic anchorage can be defined as the resistance to unwanted tooth movement. 1 Treatment planning for every orthodontic case requires that special attention be given to the selection of the anchorage protocol. Different techniques have been devised to increase tooth anchorage, such as extra-oral appliances, transpalatal bars, lingual arches, and intermaxillary elastic. 2 Although these devices are useful to some extent, they have their own limitations and are unable to provide absolute anchorage. 3
Absolute anchorage can be defined as the absence of movement of the anchor unit as a consequence to the reactionary forces applied to move teeth. Anchorage of this kind was only possible by using ankylosed teeth or dental implants as anchors, which relied on bone to inhibit movement. 4 The advent of mini-screws revolutionized the field of orthodontics as they made possible the elusive dream of effective and stable absolute anchorage. Mini-screws or mini-implants are also called as temporary anchorage devices (TADs) as they are temporarily fixed in the bone. Their small size and diameter make their insertion extremely versatile. They have become very popular in routine orthodontics due to their low cost, small dimensions, ease of insertion and removal, and the possibility of applying immediate load, thereby reducing the total treatment duration. They enable a vector of forces that is favorable for certain types of tooth movement, forestall unwanted effects, and improve the control of resultant forces during orthodontic treatment. Hence, they are used for a wide variety of tooth movement.2, 4, 5
An ideal mini-screw material should be such that it exhibits biocompatibility, corrosion resistance and at the same time has sufficient mechanical strength to enable mini-screw insertion and removal as well as the forces to which they are subjected during treatment. 6 The clinical success of the mini-screw implants depends on their stability at the insertion site. The success rate of mini-screws was found to be 80%, 7 which may make their reinsertion unavoidable during various stages of treatment. For example, immediate relocation maybe needed during the insertion process because of anatomical limitations such as proximity of roots, blood vessels, and nerves, as well as lack of primary stability or pain. During treatment, mini-screws inserted between the tooth roots may interfere with the path of tooth movement. 8 Since root proximity significantly increases the risk of mini-screw mobility or failure, 9 secondary failure may occur during the course of tooth movement, eventually leading to a need for relocation. This has aroused the interest of various authors for their reuse. However, if the retrieved mini-screws are to be reused or relocated during treatment, their mechanical characteristics must remain unaltered. 10 Therefore, the objectives of this study were to analyze and compare the morphology and surface characteristics of three commercially available brands of mini-screws before and after clinical use, and to check their viability for reinsertion during the relocation process.
Materials and Methods
Self-drilling orthodontic mini-screws of three commercially available brands were used in this study. They were divided into three groups, Group I: Orlus, Ortholution, Korea, Group II: Absoanchor, Dentos, Korea, and Group III: S.K. surgical, India. Parameters given below were tested for 10 samples of each of the three groups; therefore, a total of 30 mini-screw implants were used.
An approval from the Institution’s Ethical Review Committee was obtained to carry out this clinical study. The patients who volunteered for the study were then randomly allocated to one of the three groups. Written consent was obtained from all patients or their guardians. Patient selection criteria included the following: (a) 18-25 years of age requiring mini-screws as TADs during treatment. Mini-screws were placed in the maxillary buccal posterior segment for a minimum of 6 months of intraoral service time. (b) Good oral hygiene and periodontal status. (c) No history of systemic diseases such as diabetes. Exclusion criteria consisted of: (a) Patients out of the said age range. (b) Poor oral hygiene and periodontal status. (c) History of systemic diseases such as diabetes.
Procedure
The as-received mini-screw samples from each group were first analyzed with a scanning electron microscope (SEM) and energy dispersive spectroscope (EDS) before their clinical use. After which, they were individually rinsed in an ultrasonic bath with distilled water for 15 minutes. All samples were then sealed in individual autoclavable envelopes with identification labels and subjected to one sterilization cycle of 30 minutes at 121°C in the autoclave before their use.
Prior to the placement of the mini-screws, the patients underwent a thorough oral prophylaxis regimen to remove any plaque or calculus, especially near the insertion site. An intraoral periapical (IOPA) radiograph was taken before and after placement to determine the proximity of the anatomical structures to the insertion site and assess the interradicular space available for implant insertion. Once the placement site was determined, the patient was asked to rinse thoroughly for 2 minutes with a chlorhexidine mouthwash, and 0.5 ml of local anesthesia was administered through infiltration.
The mini-screws were placed manually using a specially designed hand driver provided by the manufacturers. During insertion, the screw was kept perpendicular to the bone surface till it was felt to have engaged the bone; following which, the direction was altered to a more apical direction in order to avoid the risk of contacting the roots. 3 Keeping the direction steady, the driver was rotated clockwise in a slow and continuous fashion until an increase in resistance was felt due to the transmucosal collar reaching the periosteal surface. Following insertion, the peri-implant tissues were gently rinsed with sterile saline solution before being loaded. Patients were instructed to maintain good oral hygiene at the implant site and were prescribed mouthwashes along with regular oral prophylaxis.
After successful clinical use, with intraoral service duration of minimum 6 months and no signs of failure such as peri-implantitis or mobility, the mini-screw implants were retrieved by application of counterclockwise torque with the hand driver under the application of a local anesthetic gel. The samples were collected for further examination and stored in a glass vial completely immersed in distilled water. The clinical procedure for the insertion and removal of all the mini-screw implant samples was kept identical and standardized and was performed by the same operator.
Prior to the SEM analysis, the retrieved samples were completely immersed in an ultrasonic bath and subjected to a cleaning cycle of 15 minutes each in an enzymatic detergent, followed by distilled water. This was done to remove any organic debris and fully observe their surface topography under the microscope. They were then individually placed in autoclavable envelopes with identification labels and taken to the lab for testing.
Morphological Evaluation
SEM of all the samples was done at an operating voltage of 15 kV with the mini-screws mounted on aluminum supporting discs using double carbon sided tape. Surface morphology was examined at 30-800× magnification with special attention to the threads and the active tip of implants. Digital images were acquired and analyzed on the ImageJ software. Inter- and intragroup comparisons were done to assess the changes seen in the sharpness of the threads and the active tip before and after clinical use.
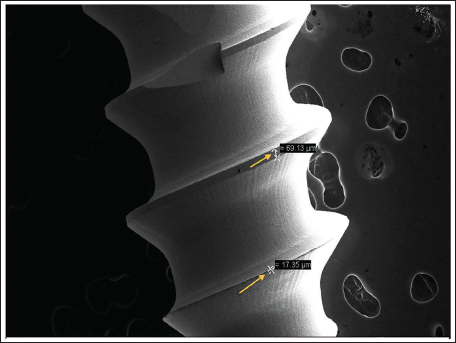
Thread sharpness: Linear measurements were taken at the widest area of each thread tip, and the mean value was taken as the sharpness value for each sample (Figure 1). Increase in the values of the thread widths would indicate blunting and wear of the threads.
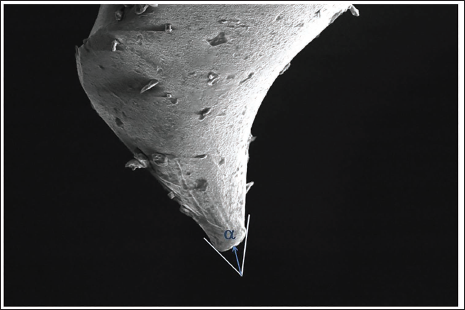
Active tip measurement: The deformation of the tip was measured as alpha value (α). It is the distance between the screw tip and the point of intersection of two tangent lines of the tip margins (Figure 2). Increased α values would indicate greater wear at the tip. The measurements were performed three times for each sample, and the mean value was used for statistical evaluation. 8
Surface roughness: Analysis of various surfaces of the mini-screws was done to investigate any manufacturing defects pre-use, and changes were seen post-retrieval at 30-800× magnification. Surface texture was observed by visual inspection and described in a qualitative manner to compare the groups. 11
Measurement of the Thread Sharpness.
Measurement of Active Tip.
Compositional Analysis
EDS was performed on all the samples to determine the elemental surface composition. The percentage of elements such as titanium (Ti), aluminum (Al), vanadium (V), carbon (C), oxygen (O), calcium (Ca), phosphorus (P), sodium (Na), and potassium (K) were analyzed using the EDS system software, and the values were compared between the groups.
Statistical Analysis
The data on continuous variables are presented as mean and standard deviation (SD), and the data on categorical variables is shown as n (% of cases) across three study groups. The intergroup statistical comparison of means of continuous variables is done using analysis of variance with Bonferroni’s correction for multiple group comparisons. The intragroup statistical comparisons of means of continuous variables are done using paired t-tests in each study group. The underlying normality assumption was tested before subjecting each variable to t-test and analysis of variance (ANOVA). The intergroup statistical comparison of distribution of categorical variables is done using Chi-square test. The intragroup statistical comparisons of categorical variables are done using Wilcoxon’s signed rank test. All the results are shown in tabular as well as graphical format to visualize the statistically significant difference more clearly. In the entire study, the p values less than .05 are considered to be statistically significant. All the hypotheses were formulated using two-tailed alternatives against each null hypothesis. The entire data are statistically analyzed using Statistical Package for Social Sciences (SPSS ver 21.0, IBM Corporation, USA) for MS Windows.
Results
Sharpness of Thread
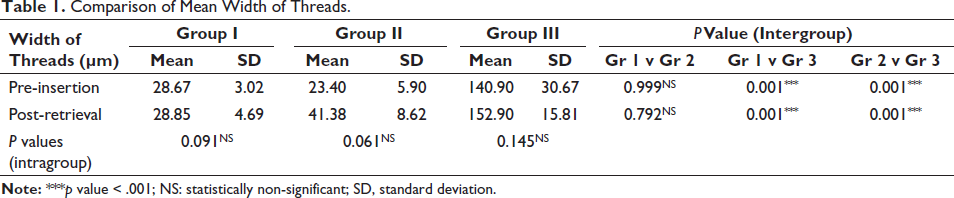
The intergroup comparison of the pre vs post-mean width of threads did not differ significantly between Groups I and II (p value > .05), whereas it was significantly higher in Group III (p value < .001 for both). The intragroup comparison of the pre vs post-mean width of threads did not differ significantly in Groups I, II, and III (p value > .05) (Table 1).
Comparison of Mean Width of Threads.
Active Tip Measurement
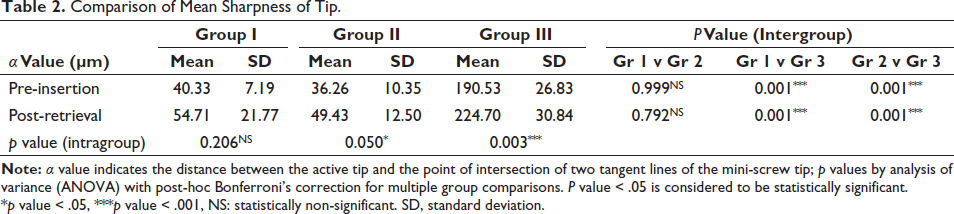
The intergroup comparison of pre-insertion mean α value (Table 2) did not differ significantly between Groups I and II (p value > .05), whereas it was significantly higher in Group III (p value < .001 for both). The intragroup comparison shows that in Group I, the mean pre-insertion α value did not differ significantly compared to mean post-insertion value (p value > .05), whereas in Groups II and III, the mean post-insertion α value is significantly higher (p value < .05 and p value < .01 respectively).
Comparison of Mean Sharpness of Tip.
Surface Roughness
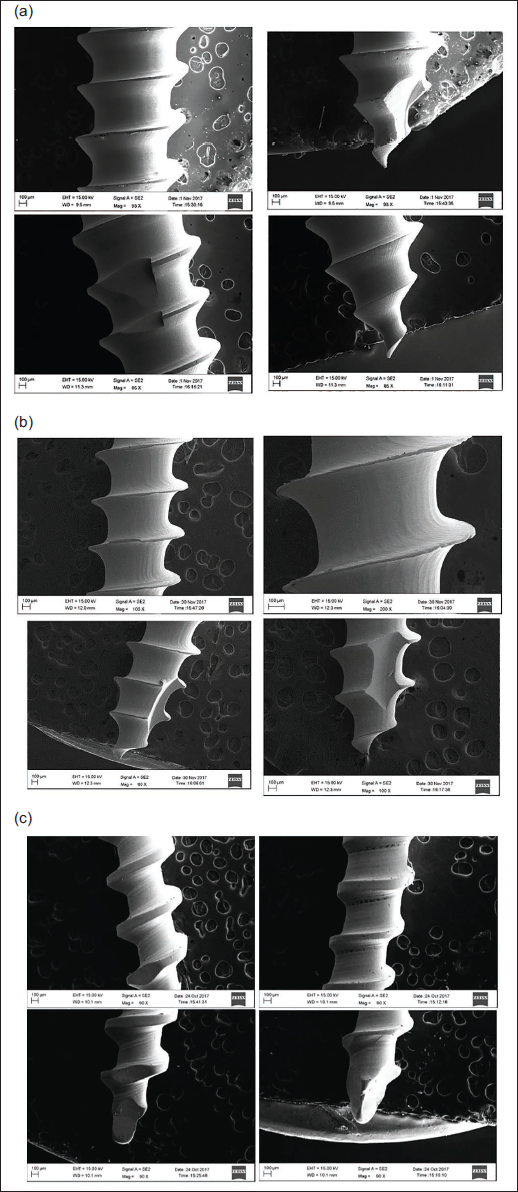
Despite a smooth appearance to the naked eye, the results of the SEM analysis show that in all three groups the mini-screw implants exhibited microscopic surface irregularities and machining defects in the form of grooves, dents, and scratches even before insertion (Figures 3a–c). These characteristics were most evident in Group III, followed by Group II. The surface of Group I mini-screws was the most satisfactory, as they displayed a clear, well-polished surface with minimal surface irregularities of the three groups. Group III mini-screws showed uniform striations between the threads and uneven widths of the threads and screw tip. Despite the surface defects, all the mini-screw implants showed a well-polished, untarnished surface. There was also a special groove that was seen at the active tip in Groups I and II.
(a) Unused Mini-screw Implant Surface of Group I. (b) Unused Mini-screw Implant Surface of Group II. (c) Unused Mini-screw Implant Surface of Group III.
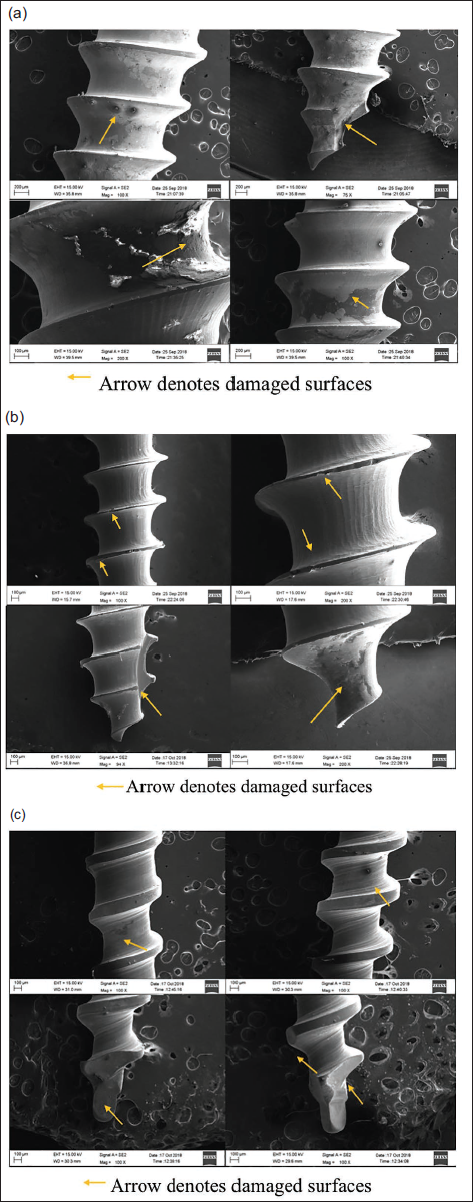
The SEM images of the post-retrieval samples revealed generalized loss of gloss and surface finish, with a consequently dull appearance in all the groups but was most evident in Group I, showing surface staining (Figures 4a–c). These changes were observed in both the head of the screw, which is exposed to the environment of the oral cavity, and the threads of the mini-screws, which are in approximation with the bone. All three groups had some amount of deposits seen scattered over the surface of the mini-screws.
(a) Retrieved Mini-screw Implant Surface of Group I. (b) Retrieved Mini-screw Implant Surface of Group II. (c) Retrieved Mini-screw Implant Surface of Group III.
Surface Chemical Composition
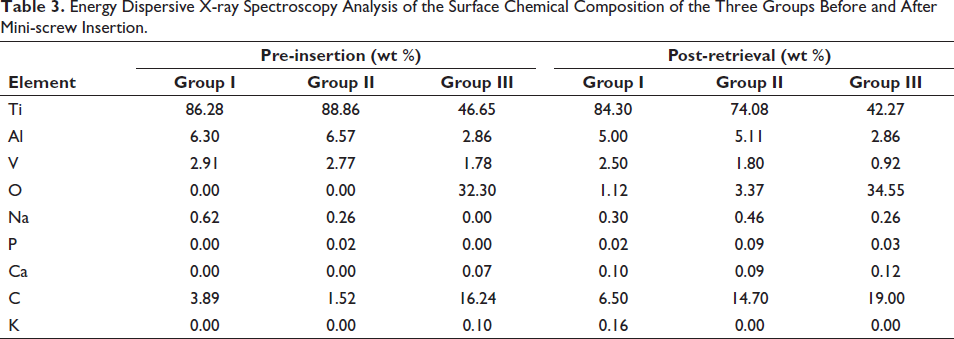
Pre-insertion, all three groups showed titanium, aluminum, and vanadium in their composition (Table 3). Group III displayed the least values for these elements and instead exhibited high oxygen content. Carbon was found in small amounts in Groups I and II and significant amount in Group III. EDS analysis post-retrieval shows an increase in the amount of organic elements such as carbon and oxygen, which seem to mask the peaks of other elements such as titanium. Small amounts of calcium, phosphorus, and sodium were also detected on the retrieved mini-screw implant surfaces.
Energy Dispersive X-ray Spectroscopy Analysis of the Surface Chemical Composition of the Three Groups Before and After Mini-screw Insertion.
Discussion
If the retrieved mini-screws are to be reused or relocated during treatment, their mechanical characteristics must remain unaltered. Between the three groups of samples tested in our study, Groups I and II demonstrated the sharpest pre-insertion tip and thread values (Tables 1 and 2). They also demonstrated the presence of a self-threading groove at the tip, which allows greater ease of placement without pilot hole drilling. 12 Group III showed statistically significant greater pre-insertion mean width of threads and α value compared to the other two groups. However, despite the difference in the sharpness values, the Group III samples did not require pilot hole drilling for their placement.
Post-retrieval, most of the mini-screw samples exhibited notable degree of deformation at the level of the active tip as well as some of the threads. This deformation is likely to be the result of the compressive forces felt at the tip of the screw due to the torque applied during insertion and removal. 13 Deformation at the threads was not statistically significant in any of the three groups (Table 1). This suggests that the overall morphology of the mini-screws remained relatively unchanged after clinical use. However, there was a statistically significant deformation observed in the active tip of the mini-screws of Groups II and III. Similar results were also seen in a study carried out by Yun et al., 10 where four recycled mini-implants showed failure to penetrate into the cortical bone, indicating severe deformation of the tip. Deformation of the active tip poses a hindrance in the reinsertion of retrieved mini-screws, as it hampers the penetration of the tip into the dense cortical bone. Subsequently, higher force levels will be required to overcome this limitation or a pilot drill must be done prior to their reinsertion. However, excessive insertion torque can lead to further tip deformation and possibly its fracture or induce microcracks due to excessive bone compression, whereas pilot drilling may cause problems such as thermal necrosis of the bone, all of which may consequently result in mini-screw failure. 8
Assad-Loss et al. 14 evaluated the design and dimensions of five different brands of orthodontic mini-implants and found that the tip region was the most susceptible area of deformation. Chung et al. 8 and Lu et al. 15 demonstrated significant deformation in the active tips of retrieved mini-implants in their study and recommended that the reinsertion of such mini-implants should be restricted to immediate relocation after primary failure, along with pilot drilling, due to their decreased bone-cutting ability. Mattos et al. 16 found reduced torque resistance in the retrieved mini-implants in their study and hence did not advocate their reuse. In contrast, Noorollahian et al. 17 did not find any adverse alterations in the mechanical properties of used mini-screws in their study and hence suggested their reuse after adequate sterilization.
It is also important to consider changes in the surface finish of the mini-screws as a factor that contributes to their stability and retention. 16 Surface roughness can increase the insertion torque 2 due to increase in the frictional coefficient. This was displayed in a study carried out by Lu et al., 15 where micro implants that were retrieved from the patients showed higher maximum insertion torque values on reinsertion due to the increased surface roughness by irregular deposits. However, roughened surfaces have also shown an increase in implant retention and removal torque. This was observed in a study carried out by Jang et al., 18 wherein mini-implants with an etched surface showed greater removal torque values and enhanced stability. Therefore, it is suggested that increase in the roughness of the mini-implant surfaces will not affect its bone-cutting ability as long as the cutting surfaces remain sharp. 19
Even before use, all three brands of mini-screws showed some amount of structural defects such as grooves, scratches, and striations. This could be the result of the machining process. Machining determines the surface finish of a mini-screw implant as it leads to surface roughness. 12 In our study, Group III images pre-insertion showed the maximum surface roughness compared to the other groups. Although the three groups showed differences in surface finish, they showed comparable clinical performance; therefore, it is not evident how these differences may contribute to the success or failure of the mini-screws. 11
Eliades et al. 20 found morphologic and surface structural alterations in retrieved mini-implants, but no material structural changes in the form of defects or pores were documented. These results are consistent with our study, where neither defects in the form of pores or cracks nor any image suggestive of corrosion could be visualized in the retrieved mini-screws. However, the surfaces showed loss of gloss resulting in a dull appearance. They also showed smoother edges, suggestive of wear during the insertion and removal. These features were also seen in a study carried out by Patil et al. 13 Alterations occurring on the surface are seen more frequently in the body region of the mini-screws because of the increased area of contact with the bone surface, whereas blunting or fracture is seen more commonly on the thread or the tip region, as these areas are thinner and directly subjected to stresses. 13
The surface chemical composition of the mini-screws before and after clinical use was also assessed (Table 3). Titanium was found to be the predominant element in the mini-screw composition of all three groups. Aluminum and vanadium were present in lower amounts, along with traces of other elements. Group III showed the lowest titanium content and a high percentage of oxygen at the surface, which could indicate the presence of a passive film of titanium oxide on the surface. This oxide layer has been found to be beneficial as it is strong, stable, and corrosion-resistant, making it suitable for insertion into tissue or bone. 21
The EDS analysis of the retrieved mini-screws showed a reduction in the weight percentage of the three parent elements. Their presence was masked due to the adsorption of other elements such as carbon, oxygen, phosphorus, sodium, and calcium on the surface of all three groups. Presence of these elements on the screw surface can be attributed to their contact with the oral environment, which consists of biologic fluids such as blood, saliva, and other exudates.8, 13 This was also seen in a study carried out by Yun et al., 10 Patil et al., 13 as well as Iijima et al. 22
If reuse of retrieved mini-screws has to be feasible in clinical practice, a careful recycling process is a prerequisite, which must be able to keep their mechanical and biological characteristics intact. 23 One of the limitations of this study is that this parameter was not investigated. However, several studies have been conducted16, 24–26 to evaluate the effects of recycling, and also new methods of processing the retrieved mini-screws have been developed to enable their reuse. Yun et al. 10 revealed that mini-implants recycled with the combination of mechanical and chemical cleaning procedures produced the best results, with surface conditions similar to the unused samples.
Another limitation of this study was that only the mini-screws placed in the maxillary buccal alveolar bone for en masse retraction were included. However, due to the difference in the cortical thickness and density of the maxillary and mandibular bone, there may be variations in the retrieval characteristics of the mini-screws placed at other anatomical sites. However, this variation was not assessed in our study. Further research with a larger sample size is required to investigate these variations. It would be useful from a clinical perspective to assess the effect of bone densities on the tip and thread sharpness of the mini-screws.
Conclusion
If the retrieved mini-screws show no significant change in their biomechanical properties, only then can their repositioning and reuse within the same patient be considered feasible. In this study, Groups I and II showed the sharpest active tip pre-use, whereas significant deformation of the active tips was noted in Groups II and III post-retrieval. Thread sharpness was not affected significantly after use in any of the three groups. Presence of organic and inorganic deposits was seen on the surfaces of the groups, with high variation among them. No major defects in the form of cracks, pores, or corrosion were seen in any of the groups post-retrieval.
Footnotes
Acknowledgments
The authors gratefully acknowledge that this article is based on a thesis submitted to the M.A. Rangoonwala Dental College and Maharashtra University of Health Sciences, Nashik, in partial fulfillment of the requirements for an MDS degree. This study was approved by the Ethics Committee of the said college.
Declaration of Competing Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
An approval from the Institution’s Ethical ReviewCommittee was obtained to carry out this clinical study. Written consent was obtained from all patients or their guardians.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.