
Abstract
Introduction
Skeletal anchorage devices for the efficient orthodontic treatment mechanics can be placed at various interradicular and extraradicular sites intra orally. However, their placement in the infrazygomatic crest area can broaden the horizon of orthodontic treatment. The bone thickness in the infrazygomatic crest (IZC) area can vary at different heights and insertion angles during the placement of IZC screws between maxillary second premolar and second molar region.
Aims and objectives
The purpose of our study was to evaluate the variation in bone thickness in the IZC area at different insertion angles along the mesiobuccal root of maxillary first molar and at different heights from the crest of the alveolar bone in the apical direction between maxillary second premolar and second molar region using cone beam computed tomography, so as to determine the best possible site where the bone thickness will be maximum that will suit to a particular size of IZC screw.
Materials and Methods
CBCT images of 50 subjects were analyzed by a single observer, the bone thickness in the IZC area was measured and interpreted at different heights from the alveolar crest in the apical direction, that is, 5 mm, 7 mm, 9 mm, 11 mm at six regions between maxillary second premolar and second molar. Bone thickness was also measured at different insertion angles ranging from 55º to 75º to occlusal plane of permanent maxillary first molar along its mesiobuccal root.
Results
The bone thickness in the IZC area was 4.5 mm–3.5 mm, when it was measured at different angles ranging from 55º to 75º to the occlusal plane of maxillary first molar along its mesiobuccal root with maximum bone thickness at 75° with a mean ± SD of 4.56 ± 1.4. Statistically significant differences in bone thickness were found between maxillary first and second molar on both right and left sides at different heights with maximum bone thickness at 11 mm apical from the alveolar crest with a mean ± SD of 2.03 ± 0.76 and 1.91 ± 0.88, respectively, and along the mesial root of maxillary second molar on right and left sides at 11 mm apical from the alveolar crest with a mean ± SD of 2.12 ± 0.80 and 1.95 ± 0.75, respectively.
Conclusions
The best site and safe zone for miniscrew insertion in IZC area is at 7 mm to 9 mm distance from the alveolar crest apically along the mesial root of maxillary second molar and at an angle of 55°–75º to the occlusal plane of maxillary first molar, so as to ensure the adequate stability of the miniscrew and without causing any damage to the adjacent anatomical structures.
Keywords
Introduction
Anchorage planning during the orthodontic treatment is one of the most arduous and challenging task for an orthodontist, inadequate anchorage control during the orthodontic treatment can compromise the orthodontic treatment mechanics which may sometimes result in the failure of the treatment outcome. In addition to the dentition born anchorage various adjunctive anchorage devices have been devised but all have some inherent drawbacks which have been overcome by the introduction of skeletal anchorage devices.1–3
Previously some conventional and traditional adjunctive anchorage devices like headgear, intermaxillary elastics and holding arches; nance holding arch and transpalatal bar were used for anchorage reinforcement but they were having some disadvantages like poor patient compliance of headgear and some undesired side effects of intermaxillary elastics which can cause unwanted rotation of the occlusal plane and extrusion of anteriors, in addition to that, holding arches are not quite effective when used alone or in combination with other anchorage devices.4, 5 Earlier osseointegrated implants were used as skeletal anchorage devices but they were larger in size and undergo osseointegration, so their removal was difficult at the end of the treatment and cannot be placed in small interradicular areas,6–8 after that miniscrews were introduced; however, if the distance between adjacent teeth is small, their placement may cause the inadvertent damage to the roots of adjacent teeth.7–10 The contact of miniscrews with the roots of adjacent teeth is one of the main cause of failure of miniscrews.11, 12 To avoid this damage various extraradicular sites can be employed as best possible sites to obtain absolute anchorage from miniscrews.
In the maxilla among the various possible sites, infrazygomatic crest (IZC) is the most appropriate extraradicular site for miniscrew insertion which can be used for enmasse retraction of anteriors, protraction of posteriors, molar intrusion and distalisation etc.13–18 Infrazygomtic crest is the best possible site for correction of vertical discrepancy as per the literature.13, 15 Anatomically IZC can be located as a palpable bony ridge which is found in between the junction of alveolar ridge and zygomatic process of maxilla. However, there is a variation in the location of IZC in adults and young individuals, in young individuals it can be palpated between second premolar and first molar while as in adults it is palpable above the maxillary first molar. 13 During the placement of miniscrews safety and stability are the primary prerequisites to ensure the efficient treatment mechanics.19–22 This CBCT study was carried out to quantitatively determine the buccal cortical bone thickness in IZC area and also to determine the best possible height and angle of insertion for IZC screws.
Materials and Methods
This study was carried out by analyzing the CBCT records of 50 subjects which were selected randomly irrespective of gender in the age group of 15–30 years from a single ethnic group of Kashmiri population. The CBCT records were analyzed by a single observer and all the CBCT images were taken with a single CBCT unit. This study is an in vitro study that was carried out by analyzing the CBCT records of patients already visiting our department for orthodontic treatment of other conditions as mentioned below in inclusion criteria.
Image Acquisition
CBCT images were taken with NewTom Giano HR 3D CEPH CBCT machine. The CBCT images were taken with the medium field of view (FOV), height — min 1,650 mm (65 in) — max 2,410 mm (95 in), scan time —18 s, 90 kVp, 1–10 mAs (pulsed mode) 0.5 mm focal spot, voxel size (micrometer): minimum slice thickness 75 &μm. CBCT images were generated in all the axial, sagittal and coronal planes and stored in DICOM format.
The study was approved by the ethical clearance committee government dental college and hospital Srinagar, Kashmir. The inclusion and exclusion criteria for this CBCT study are as follows:
Inclusion Criteria
The inclusion criteria are:
Subjects in the age group 15–30 years.
Subjects with fully erupted second molars.
CBCT records of subjects who have undergone CBCT imaging for other indications like impacted canines, supernumerary teeth and assessment of buccal and lingual cortical bone thickness.
No history of previous orthodontic treatment.
Exclusion Criteria
The exclusion criteria are:
Syndromic patients with facial asymmetry and severe openbite.
Patients with cleft lip and palate.
Patients with transverse discrepancy in maxillary arch.
Any impacted teeth in the IZC area.
Any metabolic bone disorder like osteoporosis, etc.
Measurements
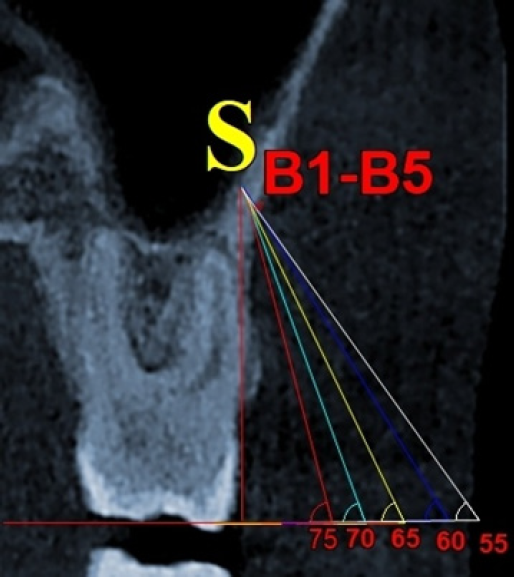
Measurements that were carried out in our study to determine the buccal cortical bone thickness at different angulations in IZC area were done as per by Liou et al. All the sections of a CBCT image, that is, coronal, sagittal and axial slices were oriented in such a fashion that the infrazyogomatic crest was shown along the mesiobuccal root tip point of maxillary first molar. To elucidate the ideal angulation for miniscrew insertion in IZC area measurements were made in the coronal section using NNT viewer software. After image orientation, two types of reference lines were drawn. The plane constructed by the mesiobuccal cusps of maxillary first molars on both sides was chosen as first reference line. A tangent was drawn along the buccal surface of mesiobuccal root of maxillary first molar which was considered as second reference plane. A point named as Sinus point (S point) is formed when the second reference line joins the floor of maxillary sinus (Figure 1). Five different angles of each 5 increments from 75º to 55º to the occlusal plane were drawn in such a manner so that each angular line passes through common S point. The intersection between these angular lines and lateral surface of IZC forms points B1–B5 representing angles 75º–55º, respectively as shown in Figure 1. The distance from points B1–B5 to S point was taken as thickness of IZC at different angles on both left and right sides of the maxillary arch in coronal section.
Coronal Section of a CBCT Image at Maxillary First Molar, Showing Maxillary Sinus Point (S) and Lines (B1–B5) Representing Different Angulations from 75º to 55º, Respectively, Drawn Through Common Sinus Point.
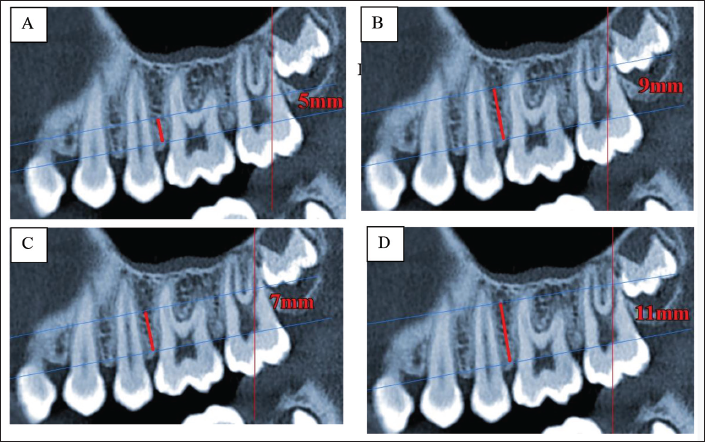
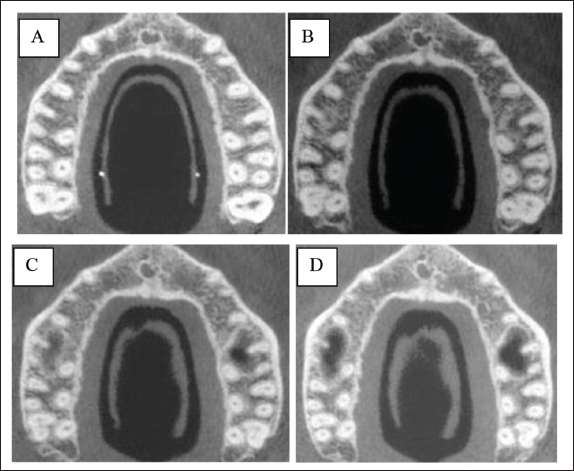
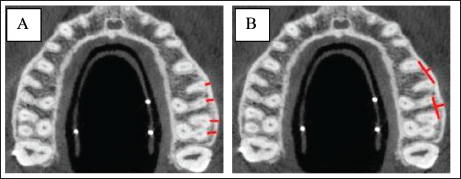
For the measurements that were carried in our study to determine the buccal cortical bone thickness on both sides in IZC area at different heights between maxillary second premolar and second molar, CBCT images were oriented in the sagittal view, the line passing through the alveolar crest bone of the maxillary first molar in the mesiodistal direction was taken as a reference line parallel to occlusal plane of maxillary first molar. Buccal cortical bone thickness was measured in axial slices bucco lingually at the distances of 5 mm,7 mm, 9 mm and 11 mm apically from this reference line (Figures 2A–D and 3A–D). The bone thickness was measured at these four different specific mentioned heights apically from the most prominent point of root bucally to most prominent point of cortical bone bucally over the roots from second premolar to second molar (Figure 4A). The buccal cortical bone thickness between the roots of maxillary second premolar and second molar was measured by drawing a tangent to the most prominent point of roots bucally and then measure the distance from this tangent to most prominent point of buccal cortical bone between the second premolar and second molar (Figure 4B).
Sagittal Views of CBCT Image at Different Heights (A) 5 mm, (B) 7 mm, (C) 9 mm, and (D) 11 mm from the Reference Plane.
Buccolingual Axial Views of CBCT Image at Different Heights (A) 5 mm, (B) 7 mm, (C) 9 mm, and (D) 11 mm from the Reference Plane.
Buccal Cortical Bone Thickness on the Roots of the Teeth (A) and between the Roots of Teeth (B) in Axial Views of CBCT Image.
Statistical Analysis
The recorded data were compiled and entered in a spreadsheet (Microsoft Excel) and then exported to data editor of SPSS Version 20.0 (SPSS Inc., Chicago, IL, USA). Statistical software SPSS (version 20.0) and Microsoft Excel were used to carry out the statistical analysis of data. Descriptive statistical analysis was first done and data were expressed as mean ± SD and standard deviation. Student’s independent t-test was employed for the comparison of bone thickness between right and left sides. ANOVA test was carried out to find the differences in bone thickness at different insertion angles and alveolar bone heights.
Results
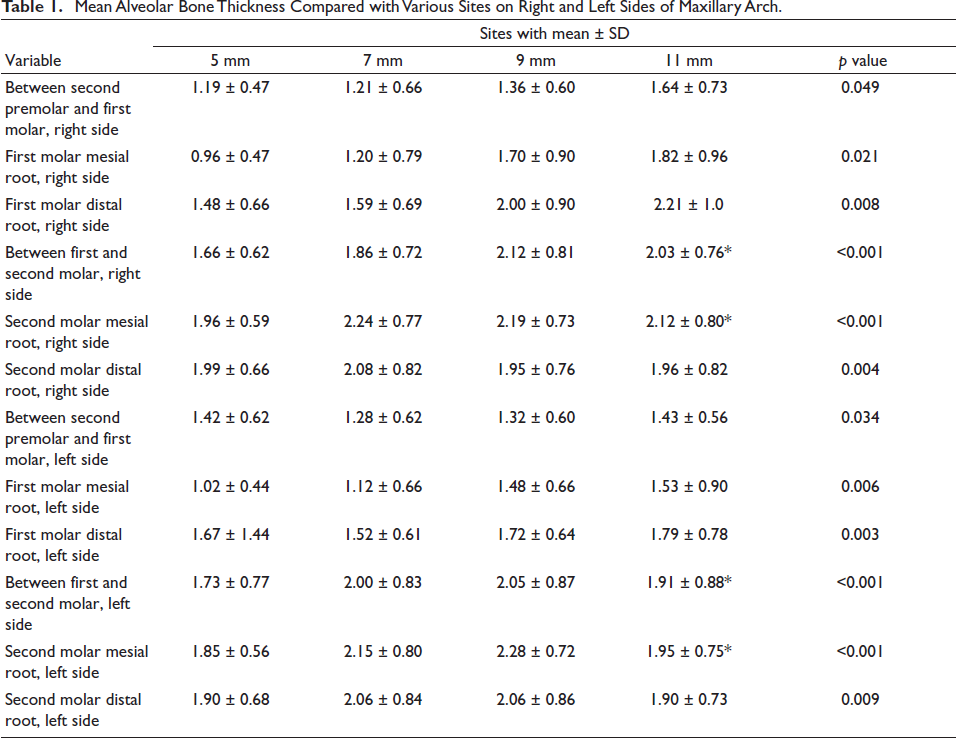
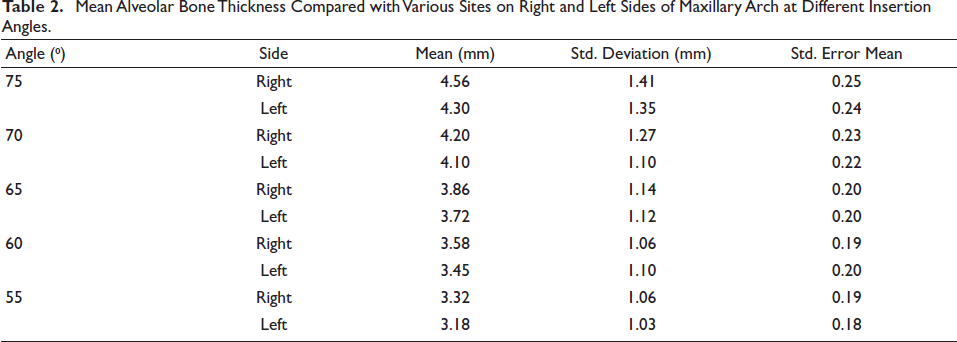
The results are depicted as shown in the following tables: Tables 1 and 2 represent the mean, standard deviation and standard error for the bone thickness at four different alveolar bone heights and insertion angles, respectively. P value was calculated. The bone thickness in the IZC area was 4.5–3.5 mm, when it was measured at different angles ranging from 55º to 75º to the occlusal plane of maxillary first molar along its mesiobuccal root, with maximum bone thickness at 75° with a mean ± SD of 4.56 ± 1.4. Statistically significant differences in bone thickness were found between maxillary first and second molar on both right and left sides with maximum bone thickness at 11 mm apical from the alveolar crest with a mean ± SD of 2.03 ± 0.76 and 1.91 ± 0.88, respectively, and along the mesial root of maxillary second molar on right and left sides at 11 mm apical from the alveolar crest with a mean ± SD of 2.12 ± 0.80 and 1.95 ± 0.75, respectively. The patients were selected randomly irrespective of the gender in the age group between 15 and 30 years, hence the influence of age and gender was not taken into consideration.
Mean Alveolar Bone Thickness Compared with Various Sites on Right and Left Sides of Maxillary Arch.
Mean Alveolar Bone Thickness Compared with Various Sites on Right and Left Sides of Maxillary Arch at Different Insertion Angles.
Discussion
The use of temporary skeletal anchorage devices as anchorage saviours especially in certain complex and difficult malocclusion situations have dramatically increased, and an ample quantity of research on temporary skeletal anchorage devices is increasing and the selection of a particular insertion site for a miniscrew depends on the planned treatment biomechanics, age of the patient, facial profile and anatomy of the adjacent anatomical structures.6, 7, 10, 11, 23, 24 After the selection of a proper insertion site, the miniscrew is initially placed into the cortical bone in a perpendicular direction to the tooth in the keratinized zone at the level of mucogingival junction so as to avoid any soft tissue tissue irritation. Once the cortical bone has been perforated during initial placement of a miniscrew, the angulation should be changed to 50–70° to get the greater surface area of the bone in contact with miniscrews and to avoid any damage to the roots of the adjacent teeth.10, 13 If any inadvertent contact of miniscrew occurs with the roots of the adjacent teeth either during insertion of the miniscrew or during treatment mechanics, it can cause damage to the roots, failure of the treatment and inadequate stability of the miniscrew.10, 25, 26
Infrazygomatic screws were introduced to avoid some drawbacks of traditional mini implants which are commonly inserted in interradicular regions and the placement of IZC screws allows the use of some complex biomechanical procedures.6, 26 IZC screws are wider and larger in dimensions than conventional mini implants. A safe distance of 0.5 mm from the adjacent teeth is recommended during the placement of a miniscrew. 9 During the placement of a miniscrew, it should be placed at a safer distance from roots of the adjacent teeth, so as to achieve the sufficient bone implant contact ratio which is the prerequisite for the stability of a miniscrew. As reported by some studies the best possible site for miniscrew insertion in IZC area is between first and second molar.6, 25, 23 Although, in our study, the maximum bone thickness was found to be at a distance of 11 mm from the alveolar crest apically on both sides, but there are maximum chances of reaching the mucogingival junction and invading the movable soft tissues when the insertion of a miniscrew is done at a height of 11 mm from the alveolar crest apically,26, 27 so the best site of choice in the IZC area should be at the distance of 7–9 mm from the alveolar crest in the apical direction in the region of mesial root of maxillary second molar when measured at different heights from the alveolar crest apically on both right and left sides.
Earlier studies24, 28 evaluated only the thickness of buccal cortical bone at insertion site which is necessary for the primary stability for a miniscrew due to insertion torque, but the total bone thickness in whole area was not evaluated. For a IZC screw with a diameter of 2 mm there should be a minimum bone thickness of around 3mm to ensure the primary stability of a miniscrew and without causing any inadvertent damage to roots of teeth and adjacent anatomical structures. In addition to the bone thickness at different alveolar heights apically, our study also quantified the bone thickness in IZC area at different insertion angles ranging from 55º to 75º to the occlusal plane of maxillary first molar along its mesiobuccal root.
In the present study, we noted the bone thickness of 4.5–3.2 mm in the IZC area when measured at angle of 55°–75° to the occlusal plane of maxillary first molar along its mesiobuccal root, with maximum bone thickness at 75° but the insertion of IZC screws at this angulation is practically impossible because of chances of root damage. The thickness of bone gets decreased as we move farther from occlusal plane. Liou et al., 13 Baungaertel and Hans 6 also reported this in their studies. A bone thickness of 13–17 mm above the occlusal plane and 5–9 mm when measured at an angle of 40°–70° to the maxillary occlusal plane was reported by Liou et al. 6 A bone thickness of 2.49 mm and 2.29 mm was noted, which was measured at a distance of 2 mm and 4 mm above the distobuccal root of the maxillary first molar respectively by Santos et al. 29 Insertion of a miniscrew at an angulation of 75º is practically difficult because of the chances of root damage and bone stripping are quite high, and insertion at an angultion of 40º is easy with less damage to the roots and less chances of bone stripping but the chances of buccal mucosal irritation is high as suggested by Liou et al. 6 So to avoid any mucosal irritation it is recommended to insert the miniscrew at the mucogingival junction in keratinized zone of the gingiva.30, 31 In distalizing the whole maxillary dentition IZC screws are effective as proved by Wu et al. in 2017. 32 Summarizing all these findings, the best possible site for the miniscrew insertion in the IZC region is above the mesiobuccal root of the maxillary second molar at a distance of 7–9 mm above the alveolar crest apically, when inserted at an angle of 55°–75° to the occlusal plane of maxillary first molar.
This CBCT study quantified the buccal cortical bone thickness in IZC region to determine best possible site and safe zone for miniscrew insertion when used for anchorage reinforcement. However in addition to the secure 33 insertion there are other factors which govern the success and stability of these anchorage devices.
Conclusion
The IZC area can be considered as one of the best extraradicular sites for anchorage reinforcement especially in certain complex malocclusions and borderline cases. The best site and safe zone for miniscrew insertion in IZC area is at 7–9 mm distance from the alveolar crest apically along the mesial root of maxillary second molar and at an angle of 55°–75º to the occlusal plane of maxillary first molar so as to ensure the adequate stability of a miniscrew and without causing any damage to the adjacent anatomical structures.
Footnotes
Declaration of Conflicting Interest
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the ethical clearance committee government dental college and hospital Srinagar, Kashmir.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Not applicable