
Abstract
Objectives
To evaluate and correlate the maturation stage of the midpalatal suture, CVM stages, mandibular left second molar mineralization stages of the subjects by CBCT.
Materials and Methods
One hundred subjects (55 males and 45 females) with a mean age of 13.56 ± 4.46 years, were divided into five midpalatal suture maturational stage groups (A to E). Cervical vertebral maturational stages on lateral cephalograms and second molar mineralization stages on orthopantograms from the CBCT images obtained from Carestream CS 9300C 3D system were analyzed and correlation among them were calculated by Spearman’s coefficient of correlation and midpalatal suture maturation stage prediction accuracy estimated with sensitivity, specificity, positive predictive value, and likelihood ratio.
Results
Spearman’s correlation analysis showed a highly significant (p value < .001) and positive correlation between MPS stage and CVM Stage (r = 0.930), MPS stage and mandibular left second molar mineralization stage (r = 0.757), and CVM stage and mandibular left second molar mineralization stage (r = 0.760).
Conclusion
Cervical vertebral maturation stages 1,2, and 3 can be used clinically to predict the midpalatal suture maturation stages A, B, and C, respectively, as their likelihood ratios were more than 10. Second molar mineralization stages had less predictive value for MPS stages.
Introduction
Midpalatal suture (MPS) owns a distinct uniqueness among the structures of the palate. Absolute thorough knowledge encompassing the ossification timing, pattern, and individual variability in the fusion of the MPS, especially in late adolescent and adult patients, is indispensable in decision making, facilitating encroachment toward a more conservative approach such as rapid maxillary expansion alone rather than surgically assisted rapid maxillary expansion. 1
Crowding and posterior crossbite associated with maxillary transverse deficiency can be alleviated by rapid maxillary expansion. 2 Arch perimeter can also be increased by rapid maxillary expansion (RME). 3 RME failure is commonly remarked while treating maxillary transverse discrepancy patients in adult. So, orthodontists should scrutinize mid-palatal suture maturation status in transverse discrepancy cases to ascertain whether the patient requires conventional RME or surgically assisted maxillary expansion. That will reduce the chances of RME failure. Sutural morphology assessment on occlusal radiographs has always been jeopardized by overlaying structures like vomer and the structures of the external nose.4, 5 So, occlusal radiographs are indecisive for surveying the mid-palatal suture area because of high probability of false interpretations.
Cone-beam computed tomography (CBCT) furnishes three-dimensional visualization of the oral and maxillofacial structures at relatively low cost, without superimposition of adjacent structures, with easy accessibility, and low radiation exposure.
The Cervical Vertebral Maturational stage method to figure out skeletal maturation can be accessible on lateral cephalograms, as these radiographs are taken customarily for orthodontic diagnosis and treatment planning without the need of an additional radiograph.6–8 This method is more reliable and reproducible in estimating the pubertal peak and further maturation in skeletal growth. There are studies on dental development as a viable substitute for cervical vertebral maturation index (CVMI) method in prophesying the growth phase. Generally, dental maturation appraisal by the stage of tooth calcification is more certain rather than phase of tooth eruption. Mandibular second molar mineralization stages served as a good predictor of skeletal maturity.9, 10
The main objectives of this study were:
To evaluate and correlate the maturation stage of the mid-palatal suture, CVM stages, mandibular left second molar mineralization stages of the subjects by CBCT. To estimate the prediction accuracy of CVM stages, mandibular left second molar mineralization stages in determining the MPS maturation stages.
In this study, we have evaluated the gender difference in the maturation stage of the midpalatal suture and its relationship not only with cervical vertebral maturational stages but also with mandibular left second molar mineralization stages, which was not the case with previous studies.
Materials and Methods
Sample size was calculated according to the formula n = Z1-α/2 2 pq/E2(q=1–p), where p = prevalence for infinite population, which will be taken as 50%. Z1-α/2 =1.96 or 2 for 95% confidence interval and 80% power. E = acceptable error of deviation. The study was conducted using the 250 pre-acquired, pre-treatment CBCT records, which was done for evaluation of impacted canines, for a longitudinal study in the pedodontics department and for assessing the effectiveness of restorative procedure after obtaining clearance from the institutional ethical committee of the university. From that based on inclusion and exclusion criteria, 100 subjects (55 males, 45 females) were selected for the study from various MPS maturational stages (a–e) on the basis of Angeileri et al. (2013) 1 classification. An approval was obtained from the Ethical Committee of the University before starting the study (Ref. code 95th ECM IIB – Thesis/p. 18).
Inclusion Criteria
Both male and female subjects with age range of 4–24 years.
No prior orthodontic, orthopedic, or surgical treatment in craniofacial region.
No history of bone deformities, bone diseases, and major illness in the past.
Exclusion Criteria
Any radiographic evidence of pathology in maxilla or mandible.
Subjects who had undergone treatment with fixed orthodontic appliance therapy.
Any appliance at the time of examination (previous maxillary expansion may affect suture status).
Cleft lip and palate.
Damage/extorted CBCT 3D acquisitions.
Method
The pre-existing CBCT records were collected from the Department of Orthodontics and Dentofacial Orthopaedics and Department of Oral Medicine and Radiology. At the time of acquisition, these records were taken using the CBCT scanner (Carestream CS 9300C) the scanning parameters of 80 kVp, 4 mA, and scanning time of 11.3 s. CBCT data were transfigured to DICOM (Digital Imaging and Communication in Medicine) format and then imported into Trophy DICOM CS 3D software. Acquired images were then standardized and oriented such that the Frankfort Horizontal Plane was parallel to the floor.
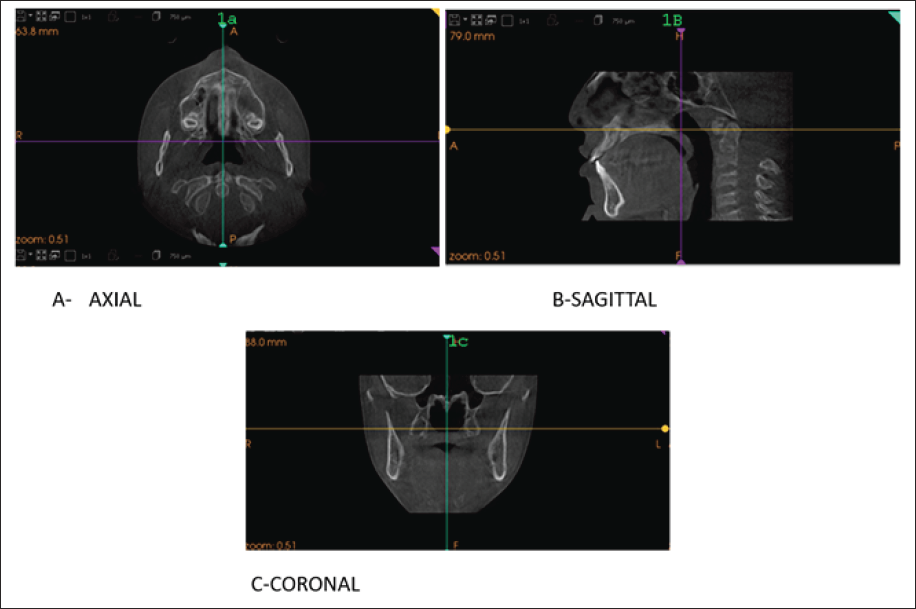
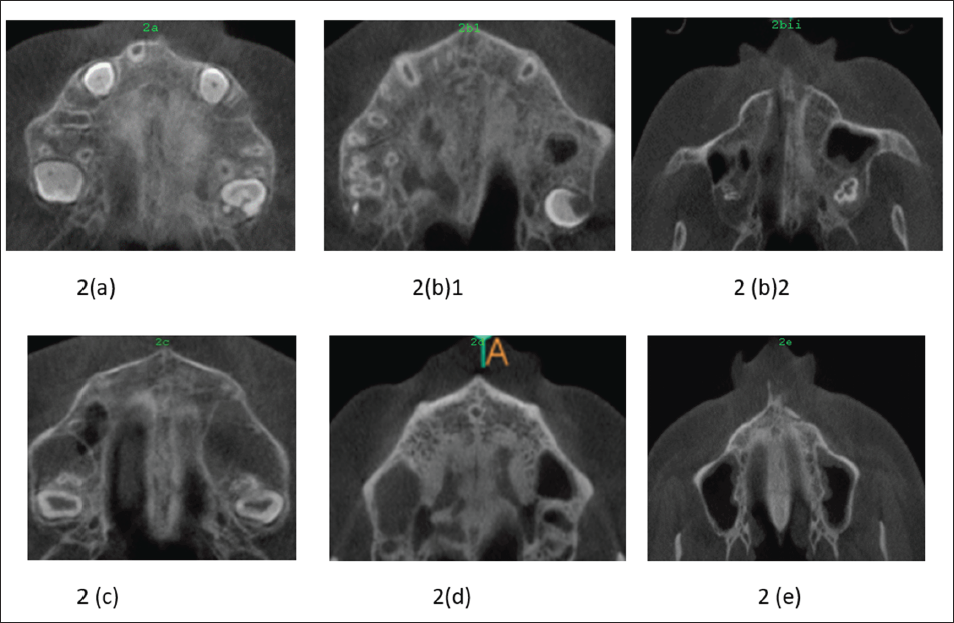
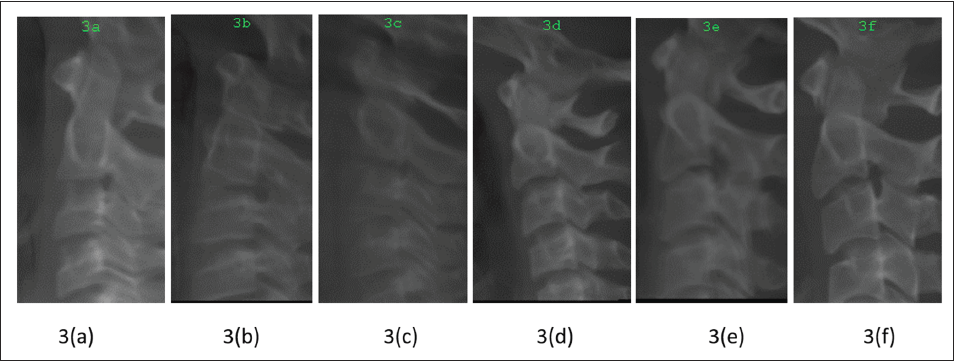
With the Trophy DICOM CS 3D software, maxillary MPS was scrutinized in the axial view of the orthogonal slicing. Midsagittal cross-sectional slice thickness was tuned for better appreciation of the palate and for orientation of the orange line of the analyzing software along with it. The stages of the fusion of MPS were recounted via the scrutiny of these standardized CBCT cross-sectional images in the axial plane on the basis of guidelines by Angeileri et al. (Figure 1a–c). The sutural maturation stage and its accuracy of every particular CBCT radiographic appearance was based on the findings of unique morphology in the fruition of the MPS as elaborated in precursory histologic studies. The radiographic facet of the MPS from initial infancy was speculated as a high solidity area even before sutural interdigitation and fusion. The subsequent illustrative stages of MPS maturation are suggested by Angelieri et al. (Figure 2a–e). With the Trophy DICOM CS 3D software, the 2D images of lateral cephalograms were generated in the sagittal view. The MIP (maximum intensity projection) value was kept at 3.5–4.5 mm and Zoom factor value at 1.5–2.5 for the proper visualization of skeletal structures being appraised and standardized. The cervical vertebrae area was cropped for better visualization to evaluate the exact CVMI stage on the basis of McNamara Staging Guidelines (Figure 3a–f).
Standardized CBCT Cross-sectional Images (a) Axial, (b) Sagittal, (c) Coronal.
(a-e) Midpalatal Suture Maturation Stages.
(a-f) Cervical Vertebral Maturation Stages.
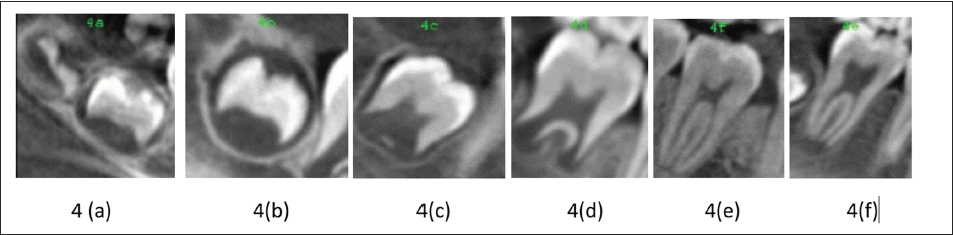
Curved slicing were used to format the 2D image of the orthopantomogram and the mandibular left second molar area was cropped to assess the maturation stage [Modified method of Gleiser and Hunt 9 used by Trakinienė Giedrė (Figure 4a–f)]. Forty images of the cervical vertebrae, 40 images of the MPS, and 40 images of second molar mineralization stages from the same subjects were selected randomly from the total sample and reclassified by the same examiner a month later. A weighted kappa coefficient was calculated for evaluation of the intraexaminer agreement for the CVMI stage and classification of the MPS maturation stage and second molar mineralization stage.
(a-f) Mandibular Second Molar Mineralization Stages.
Statistical Analysis
All the statistical analyses were performed using SPSS 16.0 windows software. The correlations among all the variables were commuted by the Spearman’s correlation test. The relationship among the maturational stages of the MPS and CVM stages and second molar mineralization stages was assessed with an estimate of diagnostic performance—the positive likelihood ratio (LHR), which constitutes sensitivity, specificity, and positive predictive value. A positive LHR of 10 or more for any CVM stage or second molar mineralization stage was considered to be an appropriate indicator for the diagnosis of any of the maturational stages of the MPS.11, 12
Results
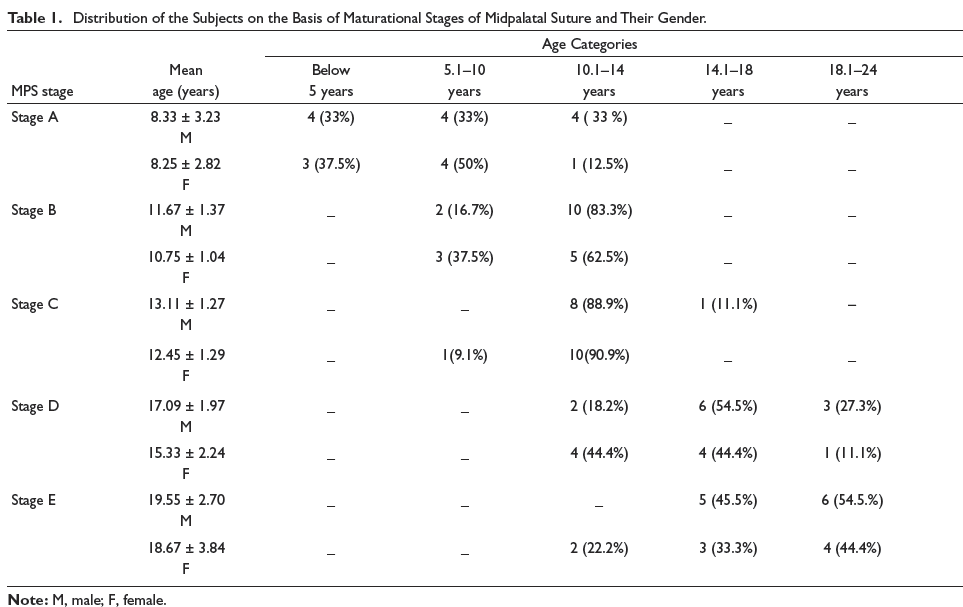
On comparison, the mean and SD of age in female subjects were lesser than that of the male subjects in all the five MPS stage (A to E) groups (Table 1).
Distribution of the Subjects on the Basis of Maturational Stages of Midpalatal Suture and Their Gender.
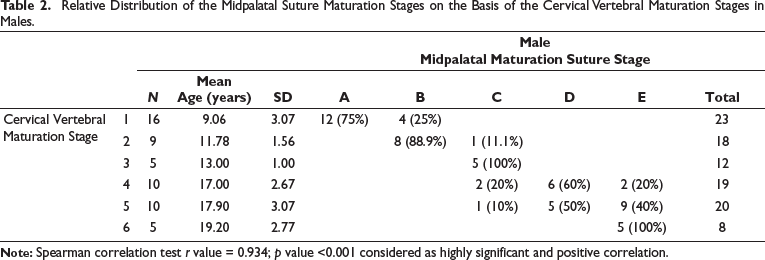
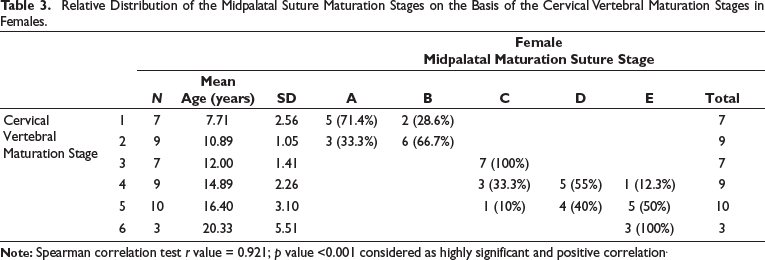
Spearman’s correlation analysis showed a highly significant (p < .001) and positive correlation between MPS stage and CVM stage (r = 0.930), MPS stage and mandibular left second molar mineralization stage (r = 0.757), and CVM stage and mandibular left second molar mineralization stage (r = 0.760). While assessing the relative distribution, highest relation was found between MPS Stage A and CVM Stage 1 (85%); lowest relation between MPS Stage E and CVM Stage 6 was 40%, and relative distribution in males and females is separately shown in Tables 2 and 3.
Relative Distribution of the Midpalatal Suture Maturation Stages on the Basis of the Cervical Vertebral Maturation Stages in Males.
Relative Distribution of the Midpalatal Suture Maturation Stages on the Basis of the Cervical Vertebral Maturation Stages in Females.
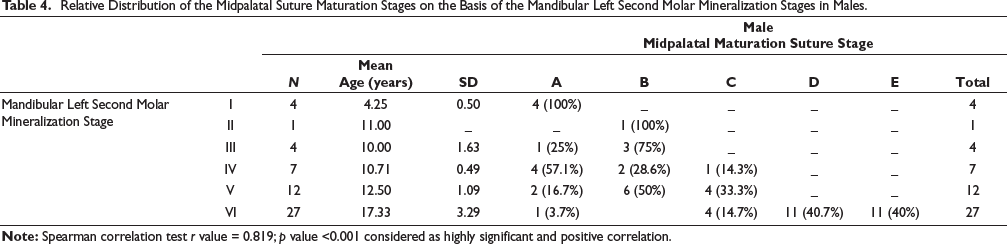
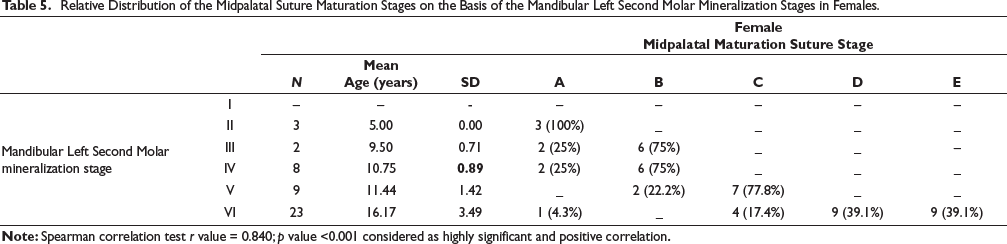
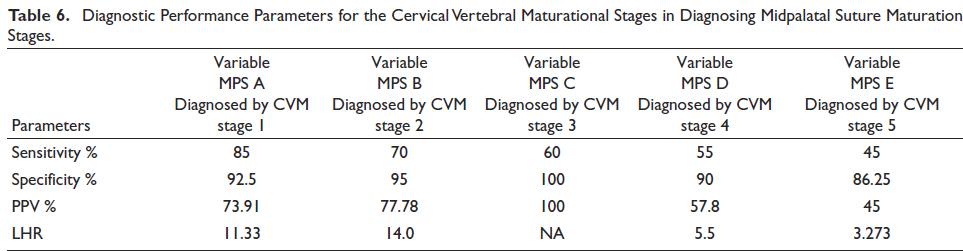
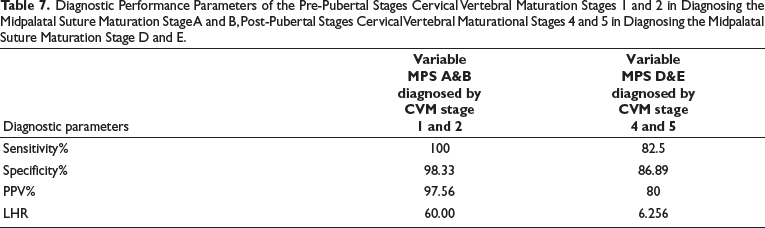
The relative distribution of MPS maturation stages on the basis of the Mandibular Left Second Molar Mineralization stages between males and females is shown in Tables 4 and 5. Skeletal maturity stages in pre-pubertal and pubertal period like CVM Stages of 1-3 had the likelihood ratio (LHR) of more than 10. The LHR for CVM1 to be a MPS Stage A is 11, CVM2 to be a MPS Stage B is 14, and CVM 3 to be a MPS Stage C is more than 10(20-∞). (Table 6). While combining pre-pubertal skeletal maturation stages (CVM stage 1 and 2) in diagnosing the MPS stage A and B, the positive likelihood ratio increased to be 60, sensitivity increased to be 100%, and the positive predictive value also increased to be 97.56%. However, the post pubertal stages such as CVM stage 4 & 5 had the positive likelihood ratio of 6.256 (less than 10) (Table 7).
Relative Distribution of the Midpalatal Suture Maturation Stages on the Basis of the Mandibular Left Second Molar Mineralization Stages in Males.
Relative Distribution of the Midpalatal Suture Maturation Stages on the Basis of the Mandibular Left Second Molar Mineralization Stages in Females.
Diagnostic Performance Parameters for the Cervical Vertebral Maturational Stages in Diagnosing Midpalatal Suture Maturation Stages.
Diagnostic Performance Parameters of the Pre-Pubertal Stages Cervical Vertebral Maturation Stages 1 and 2 in Diagnosing the Midpalatal Suture Maturation Stage A and B, Post-Pubertal Stages Cervical Vertebral Maturational Stages 4 and 5 in Diagnosing the Midpalatal Suture Maturation Stage D and E.
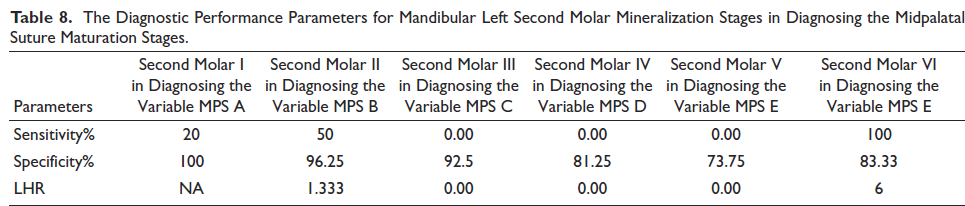
The positive likelihood ratio was found to be less than 10 for all mandibular left second molar mineralization stages. Only mandibular left second molar mineralization stage VI for diagnosing the MPS Stage E had the sensitivity of 100%. But even then, positive likelihood ratio was found to be only 6 (Table 8).
The Diagnostic Performance Parameters for Mandibular Left Second Molar Mineralization Stages in Diagnosing the Midpalatal Suture Maturation Stages.
Discussion
Midpalatal suture is the most influential structure facilitating expansion of maxilla in young individuals. Prior to its ossification, application of any force of a higher magnitude than that required for tooth movement promotes the separation of MPS via stretching of the collagenous fibers followed by formation of a new bone and true increase in its transverse dimension. Conversely in adults, the closure of MPS and circum maxillary sutures increase the complexity of expansion by countering the separation of palatine bones, and are not individualistic being enclosed within other maxillary skeletal articulations, specifically zygomatic buttressing.13, 14
The timing of the closure of the MPS has specially intrigued the practitioners due to its variability and relative uncertainty. It has conflicting literature in the past. Great disparity existed among individuals. Besides contrast in the degree of closure between sutures, variations also exist between different parts of the same suture. 15 Revelo evaluated the MPS with the help of occlusal radiograph 16 . The two-dimensional occlusal radiograph is confounding due to the overlay of the vomer and other external structures of the nose.
The method of MPS maturation classification by Angelieri et al. 1 of is chosen because of its simplicity, reproducibility, and accuracy in making the clinical decision. This morphological classification method pictures the progress of MPS density, which was forecasted to be the possible explanation for resistance to maxillary expansion in adult patients. Cervical vertebral maturation method is clinically most often used to evaluate the skeletal maturation.
Maturational changes can be observed from birth to full maturity. 17 McNamara’s Staging Guidelines 8 (2018) were chosen because of its lucidity, feasibility, improved intraobserver and interobserver reliability, and relevance of the CVM method to everyday clinical practice. In this study, we used CBCT-generated lateral cephalograms, as CBCT provides a dependable estimation of cervical vertebral maturation to assess the pubertal growth spurt. There are studies on dental development as a feasible switch for CVM method in predicting the growth phase. Dental maturity judgment has the edge of being a simple procedure as can be carried out on panoramic radiographs, which are routinely used for various purposes and on intraoral radiographs, which cause minimal irradiation to the patient. Generally, dental maturation evaluated by the stage of tooth calcification is more definite rather than phase of tooth eruption. The mineralization staging of second molars is done by the modified method of Gleiser and Hunt 9 used by Trakinienė Giedrė, 10 which was simplified from 10 to 6 calcification stages. Mandibular second molar was chosen, as its mineralization stages served as a good predictor of skeletal maturity according to previous studies. The pre-pubertal growth spurt was associated with crown formation to the cementoenamel junction of the lower second molar. For recognizing the post-pubertal development period, the second molar’s root canal closure had the highest value. 18
In our study, MPS stage A was observed up to 12 years of age in both males and females. MPS stage B was presented up to 14 years in boys, but in females, stage B was observed in 12 years. The closure of MPS (Stage D) started in 14 years in males but just in 12 years in females. These findings were supported by the findings of the studies performed by Valdiva et al. 14 and Tonello et al. 19
Spearman correlation analysis showed a highly significant and positive correlation between MPS stage and CVM stage advocating that improvement (increase or decrease) in one may be directly associated with improvement (increase or decrease) in other. These findings were consistent with the findings of study done by Angelieri et al., 5 Jang et al., 20 and Lee et al. 21
Highest sensitivity was found in pre-pubertal stages such as cervical vertebral maturation stage 1 and 2 for diagnosing MPS A and B, respectively. Skeletal maturity stages such as CVM stages 1, 2, and 3 had the likelihood ratio of more than 10, for MPS stage A, MPS stage B, and MPS stage C, respectively. This indicates that CVM stages 1, 2, and 3 can be used as a reliable indicator for predicting MPS stages A, B, and C, respectively. Whenever likelihood ratio increases more than 10, there is probability of the disease to be present, which is more than 50%. So, we can clinically use them. For other stages, the likelihood ratios were less than that of 10 and hence cannot be used for the purpose. This finding is contradicted to the study done by Angelieri et al., 5 which had likelihood ratio of 16 (more than 10) for diagnosing MPS stage D&E by CVM stage 4 and 5. Our subjects were also presented in CVM stage 6. That may be the reason behind reduced likelihood ratio.
Mandibular left second molar mineralization stage had highly significant positive correlation with CVM stage and MPS stage suggested that second molar also can be used to predict the MPS mineralization stage. MPS fusion (MPS stage D and E) started after mandibular molar mineralization stage VI. But the likelihood ratio was found to be less than that of 10 for all dental mineralization stages. So, second molar mineralization stage cannot be used clinically for predicting the MPS maturation stages.
Further studies and researches are necessary to place an emphasis on the 3D evaluation of MPS, the number of sample in each group has to be increased substantially, and importance should be given in homogeneity of the samples. Further studies using the CBCT regarding the maturational status of the MPS should include the MPS density and its importance in expansion.
Conclusion
Cervical vertebral maturation stages 1, 2, and 3 can be used clinically to predict the MPS maturation stages A, B, and C, respectively, as their likelihood ratios were more than 10.
Post-pubertal stages like cervical vertebral maturation stages 4, 5, and 6 less likely predict the authentic maturational status of the MPS.
Second molar mineralization stages had less predictive value for MPS stages, as their likelihood ratios were less than 10.
Cervical vertebral maturational stages are better than second molar mineralization stages to predict the MPS maturational stages.
Author Contributions
The principal investigator Naveen Munusamy conceptualized the study and drafted the manuscript. Pradeep Tandon formulated the methodology and was the head of the department. Dr. Gyan Prakash Singh validated the research findings and helped in providing essential resources. Dr. Amit Nagar wrote, reviewed, and validated the manuscript. Dr. Gulshan Kumar Singh curated the research data. Dr. Ranjit Kumar Patil assisted in securing resources and contributed to data curation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
An approval was obtained from the Ethical Committee of the University before starting the study (Ref. code 95th ECM IIB – Thesis/p18).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.