
Abstract
Introduction
Assessment of midpalatal suture maturation is critical to the success of the maxillary arch expansion.
Aim and Objectives
To find the correlation between the midpalatal suture maturation and facial growth pattern in the age group 15-25 years using cone beam computed tomography (CBCT) and the corresponding lateral cephalogram.
Methods
Sixty (60) patients in the age group 15-25 years with lateral cephalogram and CBCT records were evaluated. The sample was divided into three groups according to their growth pattern. Palatal suture maturation was classified into stages “A” to “E.” Based on the above data, the correlation of sutural maturation and growth pattern was evaluated. The chi-square test and Fisher’s exact test were used for group comparisons of categorical data. Statistical significance was kept at p < .05.
Results
Stage of mid-palatal suture maturation was “C” in 23.3%, “D” in 51.7%, and “E” in 25%, with none in stages “A” and “B,” indicating that obliteration of midpalatal suture starts by 15 years age. A statistically significant association was found between growth pattern and suture maturation stage (p = .041). In the 15-18 years subgroup, 9% of vertical growers and 45.5% of horizontal growers were in stage “C.” Echoing the same trend, only one patient (5%) with a horizontal growth pattern was in stage “E” as against nine (45%) with a vertical growth pattern in the 15-25 years sample.
Conclusion
Obliteration of midpalatal suture starts with the formation of bony bridges along the suture by 15 years of age in all growth patterns. Vertical growers had faster midpalatal suture maturation compared to horizontal or average growers, with no correlation between gender and midpalatal suture maturation stage. Horizontal growers in the age group 15-25 years can be subjected to conventional/skeletally anchored maxillary expansion without resorting to the use of CBCT for evaluation of midpalatal suture maturation.
Keywords
Introduction
Maxillary expansion is a common treatment modality to correct transverse discrepancy and gain space. Conventionally, it opens the midpalatal suture in a triangular shape, but the new technique of miniscrew-assisted rapid palatal expansion (MARPE) offers a minimally invasive parallel suture opening option.1–3 The feasibility of the suture to split, the appliance to be utilized, and the amount of force required depends on the calcification/maturation stage of the suture. Assessing the stage of suture maturation entails the radiographic evaluation of the calcification status of the midpalatal suture for formulating a treatment plan.
Various researchers have evaluated midpalatal suture maturation and given their interpretation based on histological and microradiographic studies. In 1975, Melsen described infantile, juvenile, and adolescent stages of morphological development after assessing autopsy samples. 4 In 1977, Persson and Thilander studied stained autopsy samples and discovered individual variations in the degree of midpalatal suture maturation. 5 In 2007, Korbmacher et al. used micro-computerized tomography (micro-CT) to study suture morphology and concluded that suture morphology is independent of age. 6 In 2013, Angelieri et al. conducted an assessment of midpalatal suture maturation stages using cone beam computerized tomography (CBCT) and classified them from “A” to “E” with increasing levels of maturation. 7
Our institutional data over the last 5 years shows that the 15-25 years age group is the most common age group seeking corrective orthodontics, and addressing transverse discrepancy in this group requires consideration of midpalatal suture maturation. The introduction of skeletally anchored expansion techniques has increased the scope of non-invasive expansion depending on suture maturation; its evaluation holds the key to the success of the procedure and device selection.
Subjecting a patient to CBCT to classify the stage of midpalatal suture maturation in decision-making entails exposure to higher levels of radiation and the availability of this diagnostic modality. Lateral cephalograms are taken routinely for orthodontic diagnosis and treatment planning. Co-relating facial growth patterns from lateral cephalogram, with midpalatal suture maturation level, can be highly beneficial in selecting appropriate maxillary expansion modality without exposing patients to high doses of radiation or in scenarios with the non-availability of CBCT. Not many studies have correlated suture maturation with the growth pattern of an individual, underlining the importance of the present study. 8 This study aims/endeavors to correlate suture maturation across different growth patterns in the mixed Indian population in the age group 15-25 years to facilitate the choice of expansion modality using CBCT and the corresponding lateral cephalogram in the selected sample.
The objectives were:
To find differences in suture maturation in average, horizontal, and vertical growth pattern patients between age groups 15-18 and 19-25 years. To evaluate any gender variation in suture maturation across three groups.
Methods
Institutional ethical committee approval was taken for the conduct of the study. This study was a record-based descriptive study using CBCT images and the corresponding lateral cephalograms. The study records were taken from the archives of the Department of Orthodontics & Dentofacial Orthopaedics.
The CBCT images, taken in natural head position using the NewTom Cone Beam 3D imaging system, with a minimum field of view of 11 × 5 mm, were analyzed in the number needed to treat (NNT) integrated software platform. The midsagittal cross-section was used sagitally, and suture maturation was assessed parallel to the palatal plane [anterior nasal spine (ANS)–posterior nasal spine (PNS)] in the central cross-sectional slice between the nasal and oral cavity, as shown in Figure 1.

Mid-sagittal Cross Section Used to Assess Suture Maturation Parallel to Palatal Plane (ANS-PNS).
Inclusion criteria:
Availability of diagnostic quality lateral cephalogram and CBCT. Age between 15 and 25 years.
Exclusion criteria:
Patients with syndromic conditions, cleft lip and palate, or a history of trauma. History of previous orthodontic treatment.
Using the variables of facial growth and maturation stages in CBCT by Angelieri et al. and the correlation between growth pattern and rate of skeletal and dental maturation by Verulkar et al. 9 study as standard norms, significance alpha level of 0.05%, power of study of 80% (ß = 0.20), error margin of 5%, and an effect size of 0.31 were used to calculate the sample size using G*Power software (version 3.1.9.7). A sample size of 60 participants was calculated.
The sample was divided into three groups of 20, each according to growth pattern, that is, horizontal, average, and vertical growth pattern. The sample was further subdivided based on age: 15-18 and 19-25 years and gender, respectively.
The cephalometric parameters used to assess the growth pattern were—Frankfurt mandibular plane angle (FMA), gonial angle, sella nasion (SN)—gonion gnathion (Go-Gn) angle, basal plane angle, Bjork analysis, and Jarabak’s ratio. After assigning patients to respective growth pattern groups, midpalatal suture maturational stages were assigned based on Angelieri et al. CBCT classification into stages A, B, C, D, and E as illustrated in Figure 2.7, 10
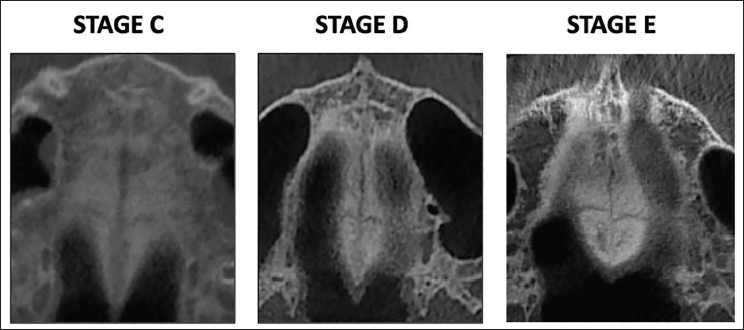
Midpalatal Suture Maturation Stages as Seen in the Present Study.
Statistical Analysis
Data compilation was recorded in MS Excel spreadsheet program and analyzed using Statistical Package for Social Sciences (SPSS) (IBM Corp) for Windows, version 23.0. Associations between age, gender, growth pattern, and midpalatal suture maturation stage were calculated using Fisher’s exact test and chi-square test. Group comparisons for continuously distributed data were made using the independent sample “t” test when comparing two groups. The chi-square test was used for group comparisons of categorical data. In case the expected frequency in the contingency tables was found to be <5% or >25% of the cells, Fisher’s exact test was used. Statistical significance was kept at p < .05.
Results
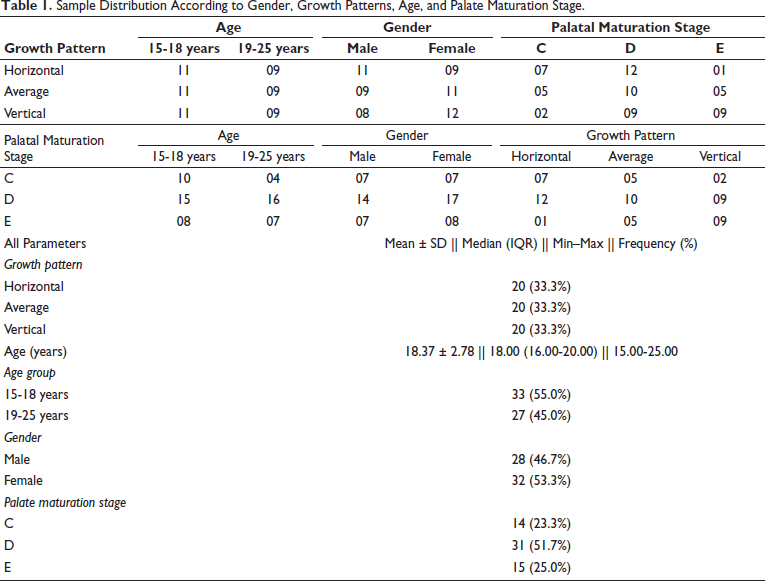
The sample size of 60 was equally divided into three groups of 20, each with average, horizontal, and vertical growth patterns. In each subgroup; 11 (55%) were in the age group of 15-18 years and nine (45%) in 19-25 years. This ensured an equitable distribution of the sample. 46.7% were males and 53.3% were females. The stage of midpalatal suture maturation was “C” in 23.3% of patients, “D” in 51.7%, and “E” in 25%. In the representative sample, no patient had suture maturation stage “A” or “B,” indicating that in the age group 15 years and above, the calcification of midpalatal suture has begun. This data is tabulated in Table 1.
Sample Distribution According to Gender, Growth Patterns, Age, and Palate Maturation Stage.
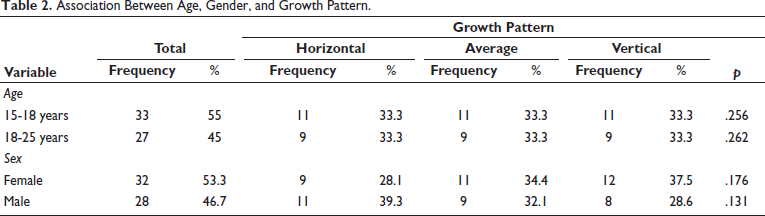
No statistically significant correlation was found between the growth pattern of an individual and age/gender (p > .05) as shown in Table 2. With increasing age, the level of suture maturation increased, with the proportion of patients in stage “C” reducing and stage “D” increasing across all growth patterns.
Association Between Age, Gender, and Growth Pattern.
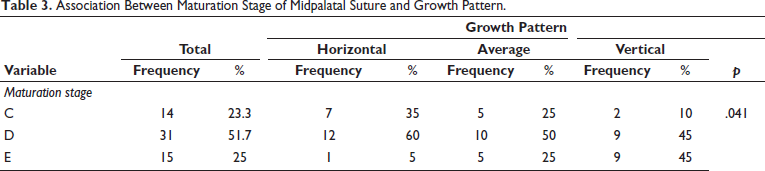
A statistically significant association was found between growth pattern and stage of midpalatal suture maturation (p = .041). 35% of the horizontal growers were in stage C as against 10% of the vertical growers indicating early closure of midpalatal suture in vertical growers. A reverse trend was seen with stage “E” suture maturation, with 45% vertical growers and 5% horizontal growers attaining stage “E.” This co-relation is summarised in Table 3. The proportion of individuals who are vertical growers attained a palatal maturation stage “E” at a higher rate than average and horizontal growers, indicating a relatively faster rate of skeletal maturation in vertical growers. On analysis of the subgroups 15-18 and 19-25 years, a similar trend of vertical growers having an earlier skeletal maturity was observed.
Association Between Maturation Stage of Midpalatal Suture and Growth Pattern.
In the 15-18 years subgroup, 9% of vertical growers and 45.5% of horizontal growers were in the stage “C.” The maturation trend consistency was found in patients with stage “E” maturation, with one (9%) patients in horizontal growth pattern as against 05 (45.5%) in vertical growth pattern.
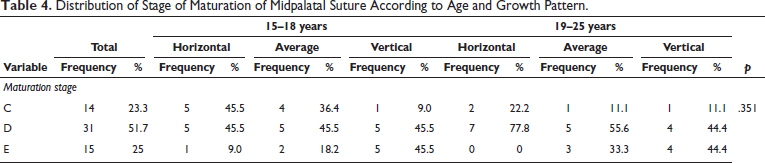
In the 19-25 years subgroup, the midpalatal suture of none of the patients with horizontal growth patterns had attained stage “E” with 22.2% in stage “C” and 77.8% in stage “D” while 44.4% of vertical and average growers had reached stage “E” of midpalatal suture maturation. Out of the 16 stage “D” patients in this age group, 44% were horizontal growers, 31% average, and 25% were vertical growers. These results further shown in Table 4 corroborate the trend of vertical growers having earlier midpalatal suture closure.
Distribution of Stage of Maturation of Midpalatal Suture According to Age and Growth Pattern.
Discussion
The stage of midpalatal suture maturation is an essential guide in the decision-making process of maxillary expansion appliance selection. The maxillary expansion is being used for more than 150 years, with the first documented case of maxillary expansion dating back to 1860 2 and documented maxillary expansion of 15 mm in animal experiments. 11
Maxillary expansion can be slow or rapid depending on the age and treatment requirement, with different expansion protocols laid down for each. As a broad guideline, during deciduous and early mixed dentition, maxillary expansion can be accomplished with light forces using a removable jackscrew expansion appliance or fixed slow maxillary arch expansion techniques like nickel–titanium (NiTi) palatal expander, quad helix, W-arch, modified titanium molybdenum alloy (TMA) transpalatal arch, and so on.12–14 During late mixed dentition or early adolescence, rapid maxillary expansion (RME) can be carried out using bonded or banded appliances like hygienic rapid expander (HYRAX). The dilemma usually is present in the age group 15-18 years in the choice of appliance and above 18 years whether non-surgical expansion can be achieved or not. Earlier, in late adolescence and adulthood, the reliable mode of maxillary expansion was surgically assisted rapid maxillary expansion (SARME). But, with the evolution of bone-anchored expansion devices, the ambit of non-surgical expansion has increased, and MARPE has gained greater acceptance.1, 3 There are individual variations in suture maturation, irrespective of age, 3 which can alter the choice of expansion appliance.
After assessing CBCT scans of 140 subjects ranging from 5 to 58 years of age, Angelieri et al. classified midpalatal suture maturation stages from A to E, corresponding to increasing levels of interdigitations and calcification of midpalatal suture. As per their study, skeletal effects would be expected during maxillary expansion in stages A, B, and C.7, 10 In stage D, radiopacity in the posterior palate indicates fusion of the midpalatal suture in the palatine bone, while in stage E, the entire maxillary midpalatal suture is ossified. In stages B and C, expansion can be carried out with slow expansion appliances or bonded/banded RME appliances, respectively, while skeletal anchorage-based appliances like MARPE are recommended for patients in stage D. In stage E, palatal suture might not open with non-surgical modalities.
To decide the appliance and protocol of maxillary expansion, the patency of the midpalatal suture needs to be ascertained. The occlusal radiographs have been used traditionally for this assessment, 15 but superimposition of adjacent structures like vomer and nose in midpalatal area precludes accurate assessment from occlusal radiographs. 16 CBCT has been found to be highly reliable in assessing the stage of midpalatal suture maturation, as thin CBCT slices provide accurate assessment along all three planes of space. But, CBCT exposes patients to high radiation and necessitates the availability of this diagnostic modality. Thus, finding a correlation between facial skeletal patterns using lateral cephalogram and suture maturation can assist as a decision-making tool without exposing patients to high radiation doses.
In this study, a statistically significant association was found between growth pattern and stage of midpalatal suture maturation (p = .041). The absence of any patient in suture maturation stages “A” and “B” in this study indicated that by the age of 15 years, obliteration of midpalatal with the formation of bony bridges along the suture had started.
In the present study, stage “E” was found in 60% of the vertical growers compared to 7% and 33% in horizontal and average growers, indicating early closure of midpalatal suture in vertical growers followed by average. In the 15-18 age group, the horizontal, average, and vertical in stage “E” were 3%, 6%, and 15%, respectively, while in 19-25 were 0%, 11%, and 15%. In horizontal growers, only one patient was found in stage “E” in the 15-18 years age group. Thus, in the age group 15-25, horizontal growers’ maxillary expansion can be undertaken with conventional RME till 18 years and with MARPE till 25 years, with conviction, without using CBCT to assess mid-palatal suture.
In the age group 15-18 and 19-25 years, 30.3% and 14% of patients, respectively, had suture maturation in stage “C” with only 03% of vertical growers. These individuals can be treated with banded/bonded RME technique. With an increased proportion of stage “D” and “E” in vertical growers above 15 years of age, banded/bonded expansion should be planned cautiously, as dental tipping can further worsen the facial balance and compromise periodontal health. No significant gender variations were found across the growth patterns and suture maturation as shown in Table 5.
Distribution of Stage of Maturation of Midpalatal Suture According to Gender.

Literature is replete with studies that correlate the dental or skeletal maturation of individuals using various dental and skeletal maturity indicators.9, 17–19 But, there is an inadequacy of studies correlating growth patterns with mid-palatal suture maturation, 8 and there is no such study in the mixed Indian population. The findings of the CBCT study conducted by Oliviera et al. 8 found that dolichofacial patients have a delayed rate of midpalatal suture maturation. The results of this study were at variance with our study, which found early palatal suture maturation in vertical growers compared to the horizontal group. The variance can be due to a heterogenous study sample in their study with the age group divided into less than and more than 30 years of age, which has low clinical relevance as the majority of patients seeking orthodontic treatment are in the lower age group.
Gottimukkala et al. 19 and Verulkar et al. 9 studied the correlation between dental and skeletal maturity and growth patterns. Both studies assessed the skeletal age of people of Indian ethnicity using skeletal maturity indicators like the Cervical Vertebrae Maturation Index (CVMI) from lateral cephalograms, hand-wrist radiographs, and dental age using the Demirjian index on orthopantomogram. They concluded that individuals with horizontal growth patterns showed delayed dental and skeletal maturation when compared with average and vertical growth pattern individuals.8, 19 Although they did not study the maturation of midpalatal suture, their results in terms of skeletal maturation are in consonance with our study.
Prlic et al. 20 compared the level of skeletal maturation in 146 Caucasian patients with various growth patterns between the ages of 12-18 years. They concluded that vertical growers have a delayed rate of skeletal maturity as compared to horizontal and average growers, which is at variance with the conclusion of the present study and similar to the study of Oliviera et al. 8 on the Caucasian population.8, 20 Thus, there might be a variation in the maturation of Caucasian and Indian populations in terms of growth patterns. In addition, many studies have also concluded that subjects with vertical growth patterns had earlier dental maturation than horizontal growers.21, 22
The present study will help the clinician in choosing the appropriate modality for maxillary expansion according to the growth pattern of an individual without using high radiation investigation modalities like CBCT in all cases.
The small sample size is one of the limitations of this study, but the matched sample size in all three groups adds to the strength as well. The matched sample helped in a better assessment of the midpalatal suture maturation across the three patterns. Further, since variations are evident in growth patterns and maturation in reported Indian and Caucasian population studies, more studies on different ethnic groups will be valuable in collating a wider database.
Conclusion
Maxillary expansion is a frequently performed procedure in orthodontic treatment. The choice of treatment modality is dependent on the stage of midpalatal suture maturation. This study found that in the 15-25 years age group, the palatal suture maturation stages across all three growth patterns were “C” to “E,” and maximum sutures in the vertical growth pattern had reached stages “D” and “E” in both, 15-18 and 19-25 year age subgroups. The findings of this study prove that maxillary suture maturation is early in vertical growers, followed by average and horizontal growers. There is no correlation between gender and the midpalatal suture maturation stage. In the age group 15-18 years, maxillary expansion can be carried out in horizontal/average with conventional and 19-25 horizontal growers with MARPE technique without resorting to CBCT. In vertical growers 15-25 years and average growers 19-25 years, diagnosis and appliance choice can be augmented with CBCT.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
CBCT and lateral cephalograms were accessed from the departmental archives. Ethical approval was granted by the Institutional Ethical Committee vide No. 024/ADCRR/IEC/2022.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
NA; the study being CBCT- and lateral-cephalogram-based retrospective and descriptive in nature. No patient photographs or personal descriptions were involved in the study.