
Abstract
Introduction
Various skeletal and dental factors help in predicting the mandibular third molar eruption, but the reliability of these factors may vary within subjects with different growth patterns. Thus, the present study aims to analyze these parameters for the lower third molar eruption in subjects with different facial growth patterns.
Material and Methods
The study was conducted on 120 pre-treatment lateral cephalograms and orthopantomograms of the subjects who were equally divided (based on the SN-GoGn angle) into three groups: normodivergent, hypodivergent, and hyperdivergent. The groups were further subdivided into impacted and erupted subgroups based on mandibular third molar eruption status. Nine radiographic parameters were compared between the impacted and erupted subgroups, using the independent Student’s t-test, to check their association with mandibular third molar eruption in different growth patterns.
Results
Beta angle was significantly different in the erupted and impacted subgroups in all three groups (with p <.05). The retromolar space and alpha angle was significant in hypodivergent group (p <.01) and the gamma angle was significant in the hyperdivergent group (p <.01).
Conclusion
Among all the parameters that were analyzed for the third molar eruption, only the beta angle was significantly related to the third molar eruption in subjects with all three different growth patterns.
Introduction
The mandibular third molar is the most frequently impacted tooth after the maxillary third molar. 1 The prevalence of third molar impaction varies from 16.7% to 68.6%. 2 The initial appearance of third molars on the radiograph can be seen from 5 to 16 years of age and its eruption is around 18–24 years. 3 The tooth has a mesial and lingual angulation during its development; therefore, for its normal eruption, it must change its angulation and become upright. Richardson, in the year 1978, stated three ways in which impactions of the tooth could occur: (a) the tooth became upright but not sufficient enough to permit its eruption, (b) the tooth did not change its angulation, and (c) the tooth underwent reverse angulation. 4
Awareness about the eruption status of third molars is of great significance to orthodontists in planning the treatment and also for the stability and maintenance of the dentition in the long run, as there has been a constant debate on the role of lower third molar in the late mandibular incisor crowding. And, for predicting the eruption status of the tooth, it is paramount to know about the factors that influence its eruption. Many skeletal and dental factors help predict the eruption of third molar, such as the retromolar space (RMS), 5 mandibular length, 6 third molar angulation, and the direction of condylar growth. 7 Bjork et al., 7 in 1956, found that the space for the mandibular third molar is diminished if the direction of the growth of the condyle is vertical. He also stated that the growth of the mandibular condyle in a vertical direction is linked with decreased resorption on the anterior border of the mandibular ramus. 7 So, it could be said that different growth patterns influence the eruption of the mandibular third molars.
In a previous study done by Jakovljevic et al., 8 certain skeletal and dental radiographic factors were studied in relation to different anteroposterior malocclusions and in different age-related groups, but these parameters have not yet been studied in different vertical malocclusions. Thus, the present study aims to analyze these skeletal and dental parameters for the lower third molar eruption in subjects with different growth patterns. The secondary objective of the study is to determine the percentage of lower third molar eruptions in different anteroposterior malocclusions.
Material and Methods
The study was conducted on 120 pre-treatment records (lateral cephalograms and orthopantomograms) of the subjects who reported to the Department of Orthodontics and Dentofacial Orthopaedics for orthodontic treatment in 2019–2020. An approval certificate from the ethical research committee of Baba Jaswant Singh Dental College, Hospital and Research Institute was obtained for the study.
The inclusion criteria for the subjects and their radiographs were that the subjects should be 18 years or above, have no history of orthodontic treatment, have no history of extractions, and the radiographs should be of good quality. The subjects with incomplete records or dentofacial deformities were excluded from the study.
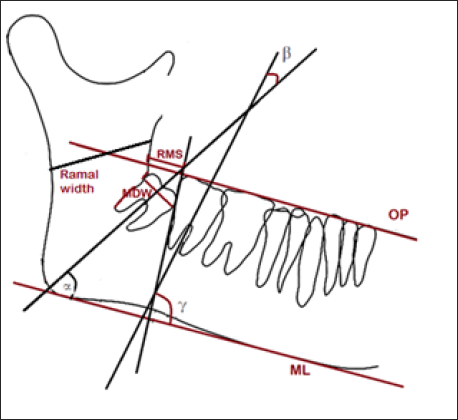
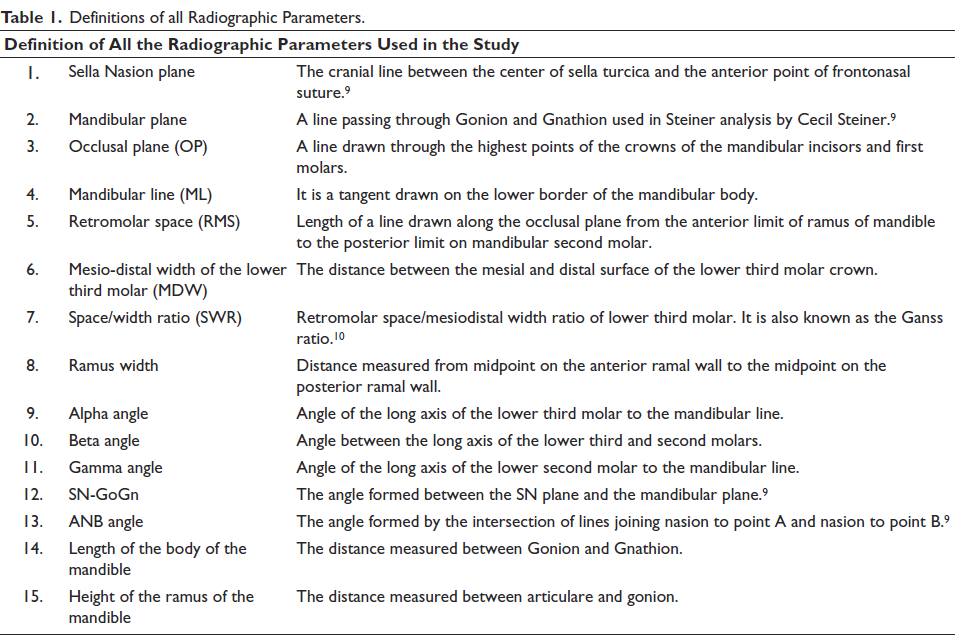
Nine radiographic parameters were evaluated, out of which RMS, mesiodistal width, space/width ratio (SWR), ramal width, alpha, beta, and gamma angles were evaluated on the OPG (Figure 1), and the length of the body of mandible and height of the ramus of mandible was measured on the lateral cephalogram (Figure 2). The definitions of all radiographic parameters are mentioned in Table I.
Linear and Angular Measurements on OPG.
Linear and Angular Measurements on Lateral Cephalogram.
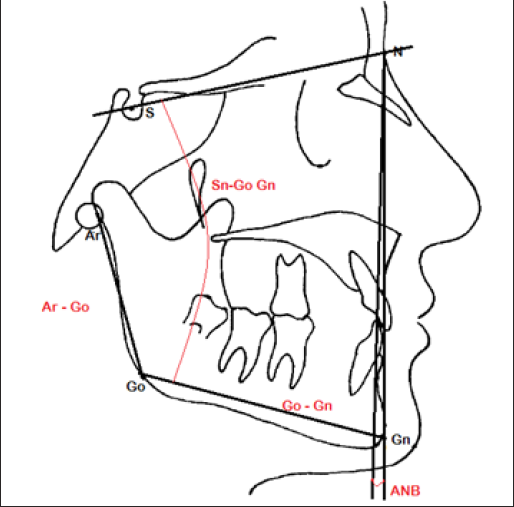
Definitions of all Radiographic Parameters.
The lateral cephalograms were used to allocate the subjects based on the SN-GoGn angle into three groups: Group I Normodivergent (SN – GoGn 27˚–32˚), Group II Hypodivergent (SN – GoGn <27˚), and Group III Hyperdivergent (SN – GoGn >32˚), with the number of subjects being 40 in each group. The SN-GoGn angle was used because the two points, Sella and Nasion, move only a minimal amount whenever the head deviates from the true profile position. 9 The sample size for the study was calculated using the formula:
N = [(Zα) 2 *σ 2 ]/e 2 = (1.96) 2 *(7.3) 2 /(2.7) 2 = 28 per group at 95% confidence level.
(The sample size was calculated by taking reference from a previous study done by Jakovljevic et al. 8 Their article aimed to analyze various skeletal and dental parameters for the lower third molar eruption in subjects with different anteroposterior malocclusions and in different age-related groups. Our study aimed to analyze various skeletal and dental parameters for the lower third molar eruption in subjects with different vertical malocclusions in adults).
The three groups were further subdivided into two subgroups, one with impacted and the other with erupted third molars. The third molars were considered erupted if they reached the level of occlusal plane, drawn on the OPG; otherwise, impacted.
The linear and angular measurements were compared between the impacted and erupted subgroups to see if the parameters were significant enough to predict the mandibular third molar eruption. The study’s secondary objective was to evaluate the percentage of the third molar eruption in different anteroposterior malocclusions. So, the parameters were also studied in Class I, II, and III malocclusions for which the subjects were divided based on the ANB angle.
Statistical Analysis
The software used to formulate the results was the SPSS 22.0 for Windows (SPSS Inc., Chicago, USA) and the level of significance was set at p <.05. Independent Student’s t-test was used in the study to check different parameters for their role in the eruption/impaction of third molars in the erupted and impacted subgroups. Univariate logistic analysis was used to determine statistically significant predictors for mandibular third molar eruption. The study used the chi-square test to find the difference between erupted and impacted third molars in different anteroposterior groups.
To check the reliability, 15 subjects were randomly chosen, and the radiographs were retraced and analyzed by the same operator after 15 days. The same operator recorded three skeletal and five dental parameters and the reliability of the data was checked using the intraclass correlation coefficient reliability index.
Results
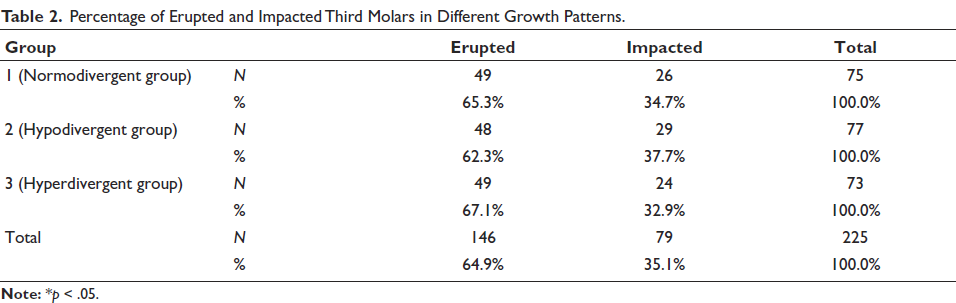
A total of 225 mandibular third molars in 120 subjects (76 females and 44 males) were evaluated. The mean age of the subjects in the normodivergent, hypodivergent, and hyperdivergent groups was 20.85, 20.15, and 20.47 years. The results showed a higher intraclass correlation coefficient (between 0.880 and 1.000), indicating good reliability. Out of the total 225 third molars evaluated, the hypodivergent group had the highest number of impacted molars, while the hyperdivergent group had the least (Table 2).
Percentage of Erupted and Impacted Third Molars in Different Growth Patterns.
All the parameters were assessed for their association with eruption/impaction of the mandibular third molar in the total sample (Table 3) using Student’s t-test. It was noted that only the RMS and alpha and gamma angles were significantly increased in the erupted subgroup and beta angle was significantly increased in the impacted subgroup.
Comparison of the Linear and Angular Measurements Between Impacted and Erupted Subgroups in the Total Sample and the Normodivergent (Group 1), Hypodivergent (Group 2), and Hyperdivergent (Group 3).
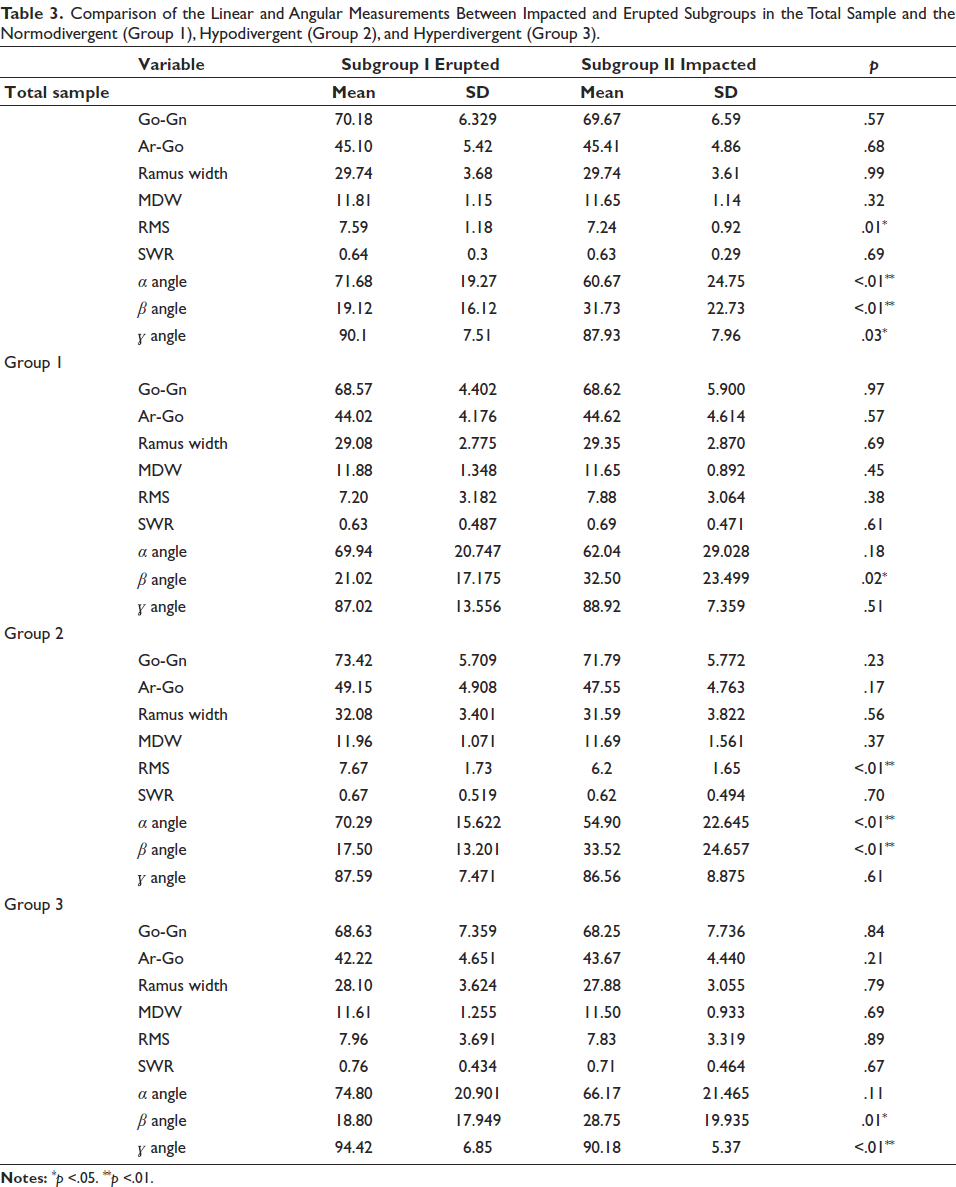
On assessment of the skeletal and dental parameters in the normodivergent group, it was seen that only the beta angle was significantly different in the erupted and impacted subgroups (Table 3). On assessment of the skeletal and dental parameters in the hypodivergent group, the results showed that the RMS and the alpha angle were significantly increased in the erupted subgroup, while the beta angle was significantly decreased in the same subgroup (Table 3). On assessment of the skeletal and dental parameters in the hyperdivergent group, the results showed that the gamma angle was significantly increased, and the beta angle was significantly decreased in the erupted subgroup (Table 3).
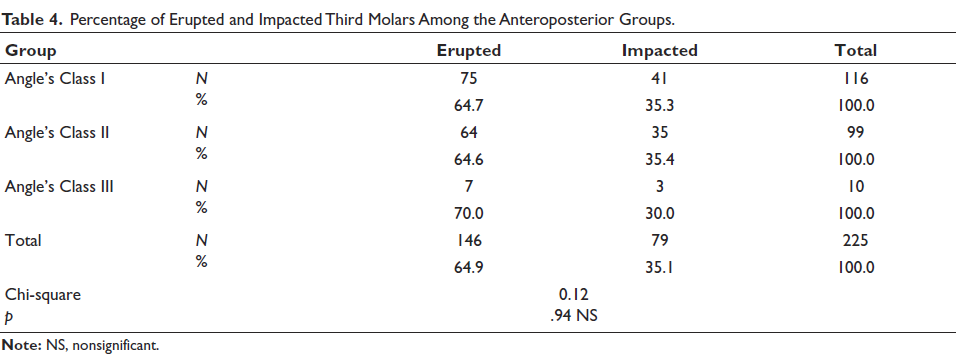
For evaluation of the number of erupted and impacted third molars within the anteroposterior groups, the results showed that the percentage of erupted and impacted third molars was 64.7% and 35.3% in Class I, 64.6% and 35.4% in Class II, and 70% and 30% in Class III malocclusion, but the result was not statistically significant (Table 4).
Percentage of Erupted and Impacted Third Molars Among the Anteroposterior Groups.
Discussion
The eruption of the mandibular third molar depends on a variety of factors. The influence of facial growth pattern on third molar eruption has been under observation since Bjork reported that a reduced space for the mandibular third molar is seen when the growth of the condyle is vertical. 7 Behbehani et al. 11 established that a reduced jaw angle measured at 18 years of age was more commonly linked to third molar impaction. 12 Erdem et al. 13 stated that the chances for mandibular third molar eruption were higher in patients with a vertical facial growth pattern, while Datana et al. 14 concluded that the eruption or the impaction of the lower third molar was independent of the vertical growth pattern of the individual. So, it can be said that the growth pattern of an individual might influence the eruption process of mandibular third molars. Hence, this study was conducted to analyze the effect of various radiographic predictors in a sample divided on the basis of facial growth patterns.
When the skeletal parameters in the total sample were compared between the erupted and impacted subgroups, our results showed that the mandibular length, ramus height, and ramus width were not significant enough to predict the third molar eruption. Ross Kaplan 15 observed similar findings and suggested that the length of the mandible was not reduced in cases with impacted third molars. However, Richardson 16 stated that a reduced mandibular length might lead to reduced RMS, thus causing third molar impaction. Behbehani et al. 11 also reported that a decreased mandibular length might increase the risk of third molar impaction. When the above skeletal parameters were evaluated within different growth pattern groups, the results were similar.
When the linear dental parameters (RMS, mesiodistal width of the third molar, and space width ratio) in the total sample were compared between the erupted and impacted subgroups, the RMS was significantly more in the erupted subgroup, while the increase in mesiodistal width and SWR was not significant. Hattab et al. 17 reported similar results, as they found significantly reduced RMS in the group with impacted third molars. In contrast to our study, Tsai 18 observed that the mesiodistal dimension of the mandibular third molar was found to be a significant factor determining the eruption of the tooth. The above difference could be due to the fact that the pattern of growth, the development of the jaws, and the size of the teeth are likely to vary among different populations and races. Another study by Kaur et al. 19 also reported a wider mesiodistal dimension of the mandibular third molar in the impacted group, which could be due to the difference in the method of measurement of the dimension between both the studies (clinical versus radiographic).
When the significance of the RMS was to be seen within different growth patterns, it was observed that the RMS remained significant in relation to the eruption of third molar only in the hypodivergent group.
When these angular parameters in the total sample were assessed in the erupted and impacted subgroups, it was seen that the alpha, beta, and gamma angles were significantly different between the two subgroups. Our results showed that the mandibular third molars were more upright (alpha angle) in the erupted group as compared to the impacted one. Similarly, Behbehani et al. 11 also concluded that an increased mesial angulation of the third molar is a significant risk factor for third molar impaction. Artun et al. 20 also stated that more than 40⁰ angulation of the third molar to the occlusal plane at the end of orthodontic treatment is a potential risk for third molar impaction. The present study revealed that the angulation between the long axis of the third and second molar (beta angle) was significantly reduced in the erupted group compared to the impacted one. A similar significant decrease in beta angle was reported by Jakovljevic et al. 9 and Uthman. 21 The association of third molar eruption and beta angle could be due to the fact that an upright angulation of the second and third molars causes less consumption of the RMS leading to the eruption of the third molar.
Only the beta angle was associated with the third molar eruption in all three groups, while the alpha angle was significant only in the hypodivergent group and the gamma angle was favorable in the hyperdivergent group. This different degree of association of these angles in different growth patterns could be the fact that the second and third molar’s direction of eruption varies within different mandibular growth patterns.
When the number of erupted and impacted third molars was studied in different anteroposterior malocclusions, it was seen that a higher percentage of the third molar eruption was seen in Class III malocclusion. However, this difference was statistically insignificant. The findings of our study were in concordance with Jain and Valiathan, 22 while Jakovljevic et al. 8 reported increased eruption in skeletal Class III cases.
Out of the total investigated radiographic parameters in the total sample, for their association with third molar eruption, a significant difference was found in RMS and the angular measurements. The correlation of RMS and alpha angle with the third molar eruption was reduced in the normodivergent and hyperdivergent groups. When the gamma angle was evaluated, it was significant only in the hyperdivergent group.
The present study shows that the role of certain radiographic parameters varies in different growth pattern groups. As the third molar eruption forms an integral part of orthodontic treatment planning, for a stable orthodontic treatment in various growth patterns, certain radiographic predictors should be considered.
As the present study was a cross-sectional study, a longitudinal study would be more insightful to study the parameters that are significant enough to predict the third molar eruption status in subjects with different growth patterns.
Conclusion
The conclusions of the study are as follows:
Out of the nine studied parameters, the RMS, along with the angular measurements (alpha angle, beta angle, and gamma angle), was significantly related to the third molar eruption.
The RMS was significant in third molar eruption only in the hypodivergent group.
When angular parameters were studied in different growth patterns, only the beta angle had a significant influence on the third molar eruption in all three groups, while the alpha angle was not significant in the normodivergent and hyperdivergent groups and the gamma angle was not significant in normodivergent and hypodivergent groups.
There was no significant difference in third molar eruption in different anteroposterior skeletal classes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Ethical Research Committee of Baba Jaswant Singh Dental College, Hospital and Research Institute, Ludhiana, Punjab, India.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.