
Abstract
Objective
To assess the diagnostic accuracy and reliability of orthopantomogram (OPG) compared to cone beam computed tomography (CBCT) in evaluating the mandibular buccal shelf anatomy, with specific emphasis on the proximity to the inferior alveolar nerve canal (IANC), across various skeletal malocclusions and vertical growth patterns.
Methods
A cross-sectional study with a retrospective design was conducted using OPG and CBCT images of 90 patients obtained prior to treatment, stratified based on skeletal malocclusion into Class I, II, and III groups (n = 30 each), and further subdivided based on facial divergence (hypodivergent, normodivergent, hyperdivergent). Linear measurements extending from the cementoenamel junction (CEJ) to the superior margin of the IANC were obtained at eight predefined anatomical landmarks. Independent t-test and one-way analysis of variance were used for data analysis, considering P < .05 as statistically significant.
Results
OPG and CBCT measurements showed no statistically significant differences across all malocclusion and growth patterns (P > .05). A consistent decrease in CEJ to IANC distance from the mesial CEJ of the first molar to the distal CEJ of the second molar was observed, most pronounced in hyperdivergent individuals. Class III hypodivergent subjects exhibited the greatest bone height (21.19 ± 1.28 mm), whereas Class II hyperdivergent individuals showed the lowest bone height (15.68 ± 1.72 mm), indicating a closer proximity of the IANC.
Conclusion
OPG is a reliable alternative to CBCT for buccal shelf assessment, offering reduced radiation exposure and cost. Anatomical variations across skeletal and vertical growth patterns significantly impact screw placement safety, emphasizing the need for individualized site selection based on malocclusion and divergence patterns.
Keywords
Introduction
Within the spectrum of temporary anchorage devices (TADs), bone screws placed in the buccal shelf region have emerged as a prominent and dependable skeletal anchorage source, particularly in cases necessitating en-masse distalization to address Class III malocclusion. The introduction of buccal shelf bone screws has facilitated a transition from surgical to nonsurgical treatment approaches, significantly broadening the envelope of discrepancy.1, 2
The posterior mandibular area distal to the second molar is considered the preferred site for buccal shelf bone screw placement, where the cortical bone is sufficiently thick to provide optimal primary stability.3, 4 However, anatomical variations among individuals and different skeletal malocclusions necessitate individualized site selection. The orientation of the bone screw must be carefully assessed to maximize engagement and to limit the potential for soft tissue damage.5–8
The primary stability achieved by bone screws placed in the buccal shelf region depends on several anatomical and biomechanical factors, including bone density and cortical bone thickness. Additionally, the anatomical pathway of the inferior alveolar nerve canal (IANC), which varies across different facial divergence patterns and skeletal malocclusions, also influences stability.9–12
Radiographic assessment is essential for determining the ideal placement site and viability of potential distalization. While cone beam computed tomography (CBCT) offers a detailed three-dimensional (3D) evaluation, it is primarily an ancillary diagnostic tool and is not routinely performed for all orthodontic patients due to its high cost and increased radiation exposure.7, 8, 13 Utilizing CBCT solely for site determination unnecessarily exposes patients to additional radiation.14, 15 In contrast, orthopantomograms (OPGs) are commonly used in clinical practice as a standard imaging modality. However, being a two-dimensional (2D) radiographic tool, OPGs may have limitations in accuracy. 16 If the site selection can be effectively determined using OPG, it would simplify the site determination in routine orthodontic practice.
Therefore, the present study aims to evaluate the reliability and accuracy of OPG-based measurements for determining buccal shelf bone screw placement sites in comparison to CBCT. By analyzing variations in the position and proximity of the IANC among different skeletal malocclusion groups with varying growth patterns, this study seeks to establish a clinically applicable framework for precise and efficient site selection, ultimately optimizing treatment outcomes in contemporary orthodontic practice.
Materials and Methods
Research Design and Sample Size
A retrospective cross-sectional methodology was followed, with participant selection based on purposive sampling criteria. With the approval of the ethics committee, the research investigated the pretreatment CBCT scans and OPG of 90 patients. All CBCT and OPG scans, though retrospective, were originally acquired under a standardized protocol. To ensure minimized variability, patients were oriented in natural head position, with the Frankfort horizontal plane aligned parallel to the floor and the midsagittal plane maintained perpendicular to it. The reporting of this study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 17 guidelines for observational research.
The samples were stratified into three equal groups based on skeletal malocclusion and further subdivided according to varying degrees of facial divergence for comparative analysis (N = 30, n = 10).
The sample size estimation was carried out based on the formula outlined below:
where
Based on this equation, a sample size of 90 would allow the determination of the effect of independent variables on the proximity to the inferior alveolar canal.
The exclusion criteria for this study comprised individuals with a history of extraction of the mandibular second and first molars, prior orthodontic therapy, tipped lower first and second molars, presence of implants or pontics in these regions, prior orthognathic surgical intervention, any periodontal pathology, diagnosed congenital syndromes, unerupted teeth, facial or mandibular asymmetries, supernumerary teeth, expanded cystic follicles, or other relevant pathological conditions involving the region under evaluation.
The subjects were categorized into three skeletal malocclusions using a composite evaluation of four cephalometric angular measurements: ANB angle, Yen angle, Beta angle, and W angle. Classification was performed as follows:
Class I: ANB angle (0°-4°), Yen angle (117°-123°), Beta angle (27°-35°), and W angle (51°-55°). Class II: ANB angle >4°, Yen angle <117°, Beta angle <27°, and W angle <51°. Class III: ANB angle <0°, Yen angle >123°, Beta angle >35°, and W angle >55°.
Further, the groups were subdivided according to the facial divergence patterns considering the mandibular plane angle and Jarabak ratio. The samples were divided into normodivergent (32 ± 5°, Jarabak ratio = 62%- 65%) (n = 10), hypodivergent (≤27°, Jarabak ratio > 65%) (n = 10), and hyperdivergent (≥37°, Jarabak ratio < 62%) (n = 10) groups.
CBCT and OPG Evaluations
A 3D volume scanner (Genoray Papaya 3D+, South Korea) was used to obtain CBCT data. The acquired datasets were stored in Digital Imaging and Communications in Medicine (DICOM) format. The DICOM data were processed to generate 3D reconstructions for measurement with CS 3D Imaging software (version 3.10, Carestream Health Inc., NY, USA), and the digital OPGs were analyzed on the Triana software (version 2.4, Genoray Co., Ltd.).
All the measurements were conducted on an HP Pavilion 15 all-in-one display monitor under controlled lighting and acoustic conditions. To ensure consistency and reduce potential measurement bias, image orientation followed a standardized protocol. The sagittal plane was adjusted to pass through the center of the alveolar process, maintaining parallelism with the mesial roots of the mandibular first molar and extending distal to the second molar. The axial plane was aligned at the level of the furcation regions of the mandibular first and second molars. The coronal plane was oriented parallel to the long axis of the mandibular molars and was established with reference to the axial and sagittal planes. All measurements were subsequently performed on standardized coronal sections and curved slicing in CBCT scans and on OPG by a single examiner at the below-mentioned sites.
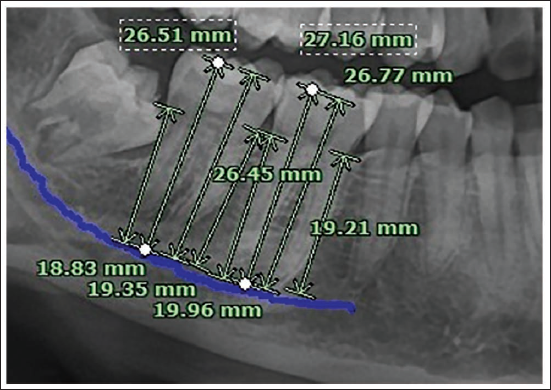
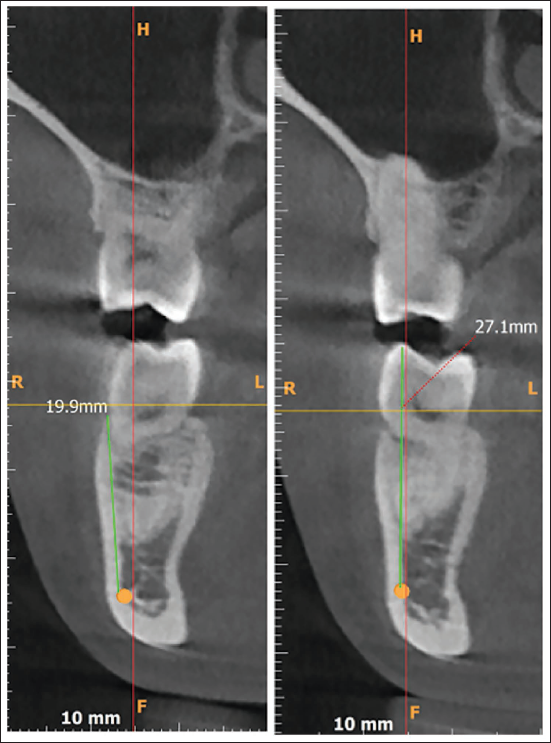
The spatial positioning of the IANC was evaluated. The IANC was digitally traced using a tracing tool in the software. The proximity to the inferior alveolar nerve was assessed by measuring the distance from the cementoenamel junction (CEJ) to the highest point of the IANC (Figures 1 and 2).
Proximity to Inferior Alveolar Nerve Canal Measured from Cementoenamel Junction to the Superior Most Point of Inferior Alveolar Nerve Canal on Orthopantomogram.
Proximity to Inferior Alveolar Nerve Canal Measured from Cementoenamel Junction to the Superior Most Point of Inferior Alveolar Nerve Canal on Cone Beam Computed Tomography.
Eight locations were chosen to make the measurements:
Mesial CEJ of first molar Distal CEJ of first molar Mesiobuccal cusp tip of first molar Distobuccal cusp tip of first molar Mesial CEJ of second molar Distal CEJ of second molar Mesiobuccal cusp tip of second molar Distobuccal cusp tip of second molar
The measurements obtained from the mesiobuccal and distobuccal cusp tips (Locations 3, 4, 7, and 8) were recorded to evaluate the presence of any significant molar tipping or inclination differences. Their primary purpose was to support the study’s exclusion criteria and minimize potential bias by ensuring that variations in molar angulation do not influence the overall findings.
Statistical Analysis
Statistical analysis included descriptive measures with an independent t-test applied to assess differences in measurements between CBCT scans and OPG images. Variations in proximity to the IANC across different groups were analyzed using one-way analysis of variance (ANOVA). A P value of less than .05 was considered statistically significant, and all analyses were executed using Stata 17 software (Stata 17, StataCorp LLC, College Station, TX, USA).
Results
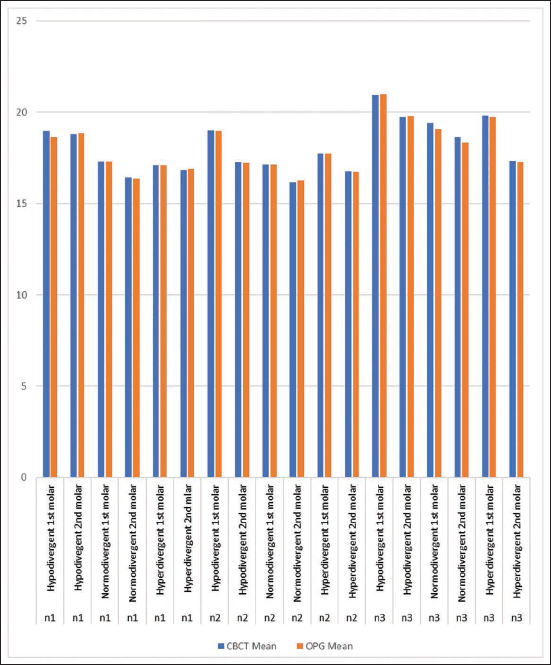
The intergroup comparison between CBCT and OPG measurements showed that none of the differences were statistically significant (P > .05) across all skeletal malocclusions and facial divergence patterns (Figure 3).
Comparison of Mean Measurements Between Cone Beam Computed Tomography and Orthopantomogram Across Different Skeletal Malocclusion and Vertical Growth Patterns.
An incidental finding was observed in all skeletal malocclusions and growth patterns: as measurements progressed from the mesial CEJ of the first molar to the distal CEJ of the second molar, the mean values decreased, indicating an increasing proximity of the IANC to the root apices as we progress distally in the posterior region. This pattern was most pronounced in hyperdivergent individuals, highlighting their increased anatomical risk for nerve encroachment. For instance, in Class I hyperdivergent subjects, the values decreased from 17.46 ± 1.17 mm at the first molar mesial CEJ to 16.10 ± 2.20 mm at the second molar distal CEJ, with a P value of .01. Similarly, in Class II hyperdivergent individuals, the values declined from 17.27 ± 1.50 mm to 15.68 ± 1.72 mm (P = .05). In the Class III hyperdivergent group, the measurements reduced from 18.96 ± 2.02 mm to 16.88 ± 3.68 mm (P = .05). These consistent findings across all malocclusions emphasize that the posterior mandibular region in hyperdivergent individuals is at increased risk of proximity to the IANC, necessitating cautious site selection for bone screw placement.
Intragroup Comparison
Class I Malocclusion
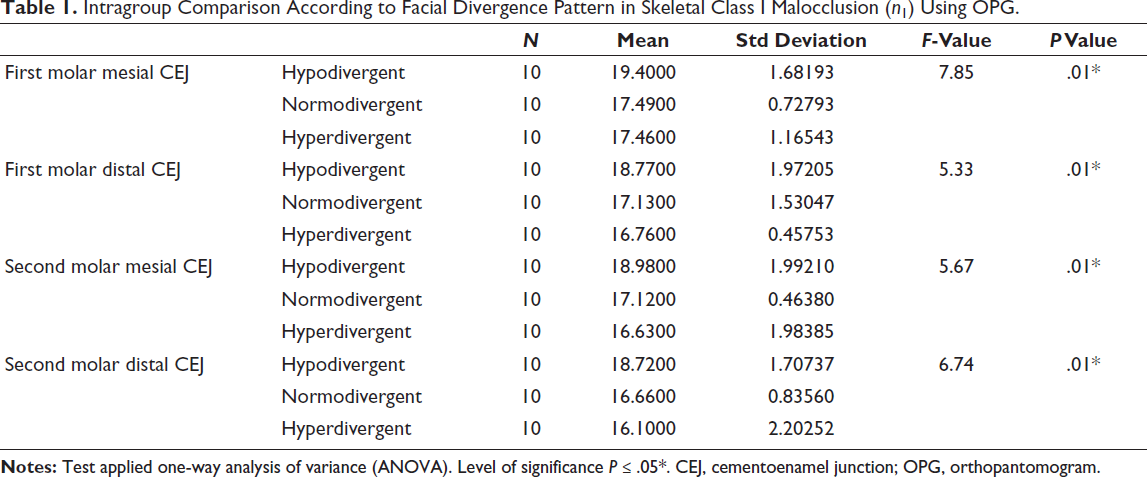
Among individuals with Class I malocclusion, those with a hypodivergent growth pattern demonstrated increased values, ranging from 19.40 ± 1.68 mm at the first molar mesial CEJ to 18.72 ± 1.71 mm at the second molar distal CEJ (P = .01). Normodivergent individuals showed moderate values, decreasing from 17.49 ± 0.73 mm to 16.10 ± 2.20 mm (P = .01), while the hyperdivergent group displayed the lowest bone heights to IANC, reducing from 17.46 ± 1.17 mm to 16.10 ± 2.20 mm (P = .01) (Table 1).
Intragroup Comparison According to Facial Divergence Pattern in Skeletal Class I Malocclusion (n1) Using OPG.
Class II Malocclusion
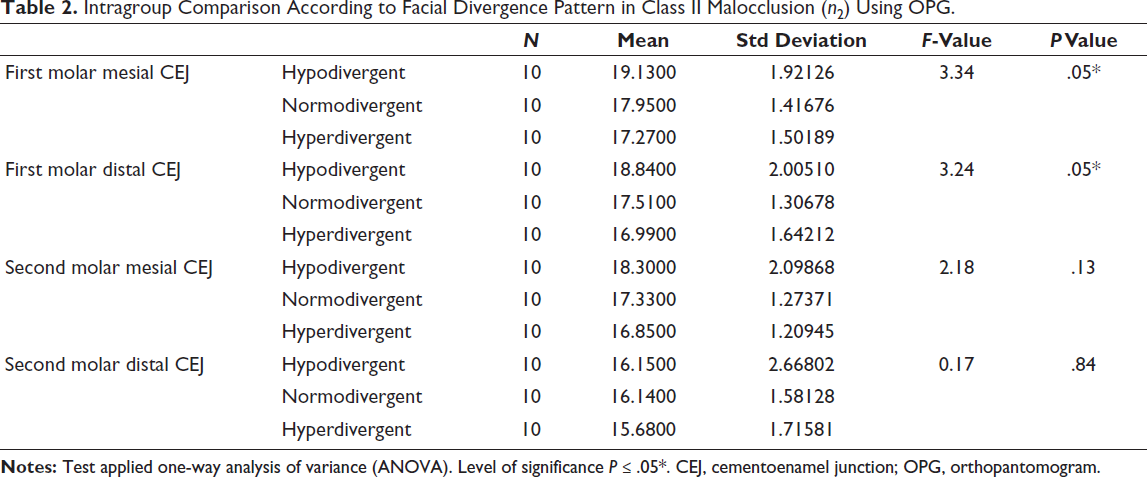
In Class II subjects, hypodivergent individuals again demonstrated the highest values, with bone height reducing from 19.13 ± 1.92 mm at the first molar mesial CEJ to 16.15 ± 2.67 mm at the second molar distal CEJ (P = .05). The normodivergent group showed a decrease from 17.95 ± 1.42 mm to 16.14 ± 1.58 mm (P = .05), while the hyperdivergent group presented the lowest values, reducing from 17.27 ± 1.50 mm to 15.68 ± 1.72 mm (P = .05). These findings highlight the increased risk of IANC proximity in Class II hyperdivergent, making them the least favorable for buccal shelf screw placement (Table 2).
Intragroup Comparison According to Facial Divergence Pattern in Class II Malocclusion (n2) Using OPG.
Class III Malocclusion
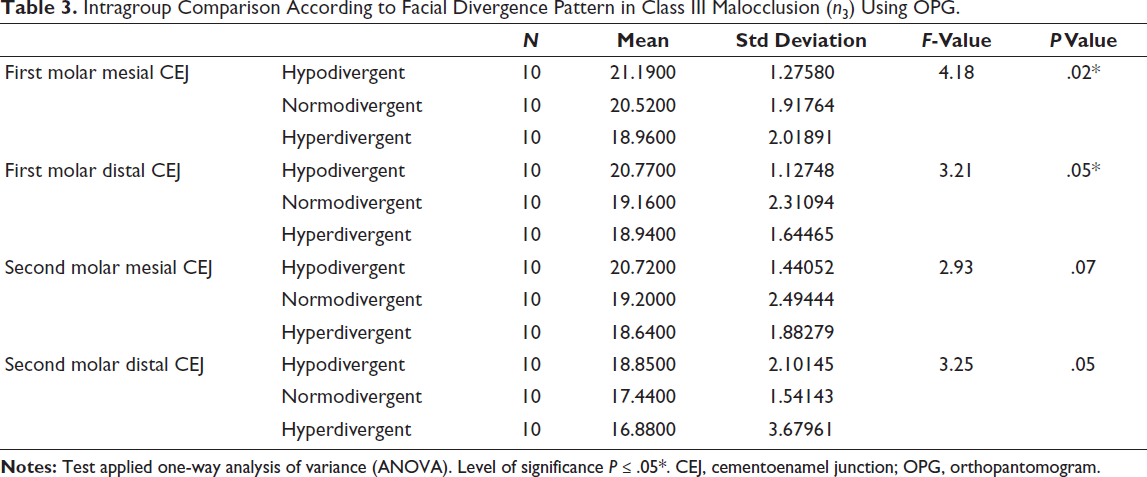
Individuals with Class III malocclusion exhibited the highest bone height values among all skeletal malocclusion groups, particularly in the hypodivergent category. In these individuals, the bone height declined from 21.19 ± 1.28 mm at the first molar mesial CEJ to 18.85 ± 2.10 mm at the second molar distal CEJ (P = .02). Normodivergent individuals showed a reduction from 20.52 ± 1.92 mm to 17.44 ± 1.54 mm (P = .05), while the hyperdivergent group demonstrated values decreasing from 18.96 ± 2.02 mm to 16.88 ± 3.68 mm (P = .05). This confirms that Class III hypodivergent individuals possess the most favorable anatomical dimensions for bone screw insertion, while Class III hyperdivergent individuals require cautious planning due to closer IANC proximity (Table 3).
Intragroup Comparison According to Facial Divergence Pattern in Class III Malocclusion (n3) Using OPG.
Intergroup Comparison
In intergroup comparisons, significant differences (P < .05) were identified in bone height to the IANC across different skeletal malocclusions within the same vertical growth pattern. Among hypodivergent individuals, the highest bone height to IANC was found in Class III malocclusion (21.19 ± 1.28 mm), followed by Class I (19.40 ± 1.68 mm) and Class II (19.13 ± 1.92 mm), suggesting that hypodivergent Class III individuals offer the most favorable anatomical conditions for safe and effective placement of buccal shelf bone screws. Conversely, within the hyperdivergent group, the lowest bone height was observed in Class II malocclusion (15.68 ± 1.72 mm), indicating a closer proximity of the IANC to the CEJ and a potentially higher risk of neurovascular complications. Slightly higher values were recorded in hyperdivergent Class I (17.46 ± 1.17 mm) and Class III (18.96 ± 2.02 mm) individuals, reinforcing that hyperdivergence, particularly when combined with Class II skeletal patterns, poses the challenging anatomical scenario for bone screw placement.
Discussion
Skeletal anchorage has revolutionized orthodontic treatment by providing reliable solutions for complex malocclusions. This approach is particularly beneficial in the management of borderline Class III malocclusion, where skeletal and dentoalveolar discrepancies necessitate the distalization of mandibular dentition to establish a more harmonious sagittal intermaxillary relationship and optimize occlusal function.
Utilization of buccal shelf bone screws is a preferred method for achieving mandibular distalization. The buccal shelf region offers an advantageous location for extra-alveolar bone screw placement due to its favorable osseous quality, high bone density, biomechanical advantages, and minimal risk of failure.
The selection of the most suitable insertion site for buccal shelf bone screw placement and viability of distalization in Class III cases can be evaluated utilizing an array of imaging modalities, including CBCT and OPG. 19
The dearth of literature appraising the veracity of 2D radiography compared to CBCT precipitated this study, in which measurements were meticulously conducted on OPGs in 2D views and on CBCT images in coronal views and curved slices. Additionally, it was observed that IANC could be accurately traced in 2D views. This study examined the reliability and accuracy of measurements procured from OPG as compared to those derived from CBCT. Furthermore, this study seeks to ascertain whether OPGs can be utilized as an alternative diagnostic modality for bone screw placement. The findings of this study revealed a statistically insignificant difference between the measurements conducted using CBCT and OPG.
Most studies have evaluated the preferred location site using CBCT, as CBCT is considered the standard method for assisting orthodontic diagnosis. In a comparative evaluation of 2D radiographs and CBCT images for mini-implant planning, Caetano et al. demonstrated that CBCT facilitates precise site selection in interradicular areas and contributes to improved placement success. 20 Conversely, Grünheid et al. reported that the radiation exposure associated with CBCT protocols commonly employed in orthodontic practice is considerably greater than that of digital 2D radiographic systems. Their findings indicated that effective dose values obtained from combined maxillary and mandibular CBCT scans, including those performed with i-CAT units, ranged from 4 to 42 times higher than the dose delivered by a conventional panoramic radiograph acquired using an Orthophos Plus DS system. 21 Additionally, given that CBCT is more expensive, its use necessitates consideration of cost-effectiveness.
OPG is extensively utilized in orthodontic diagnosis and performed in routine clinical practice. Its advantages include minimal radiation exposure, cost-effectiveness, and comprehensive visualization of the entire dentition and surrounding structures. A study by Bennemann et al. evaluated the positioning of miniscrews using OPG compared to CBCT. The findings indicated that OPG allows for a preliminary assessment of the screw position relative to adjacent anatomical structures. Despite its lower accuracy compared to CBCT, the significantly lower radiation exposure of OPG makes it a viable option, typically providing an adequate estimate for miniscrew insertion. 16 Thus, 2D radiographic imaging may represent a more feasible and cost-efficient alternative to 3D CBCT-based planning in routine bone screw placement.
However, the determination of the ideal placement site is influenced by several factors, including the applied biomechanics and local anatomical considerations, such as the course of the IANC.3, 4 The trajectory and morphology of the IANC can exhibit considerable variability across different facial types and skeletal malocclusions, necessitating careful evaluation to mitigate potential complications when placing buccal shelf bone screws. To ensure the safety and stability of the buccal shelf bone screw, variations in proximity to IANC among different sagittal and vertical patterns should be considered.3–7 The findings revealed distinct anatomical variations in proximity to the IANC among different skeletal malocclusion classes and vertical growth patterns, carrying significant clinical implications for bone screw placement. The greatest distance between CEJ and IANC, indicating the lowest risk of nerve encroachment, was observed in Class III hypodivergent individuals, reflecting reduced proximity to the IANC and thus more favorable conditions for bone screw insertion. In contrast, the shortest measured distance to the IANC was observed in Class II hyperdivergent subjects, signifying increased proximity and a comparatively higher anatomical risk. A consistent trend was noted across all skeletal malocclusion and growth patterns, with proximity to the IANC increasing progressively in the distal direction from the mesial CEJ of the first molar to the distal CEJ of the second molar. This pattern was most pronounced in hyperdivergent individuals, emphasizing their greater susceptibility to neurovascular complications during bone screw placement. The findings of this study are in concordance with those reported by Eto et al. 18 A significant increase in proximity to IANC in hyperdivergent growth pattern was found compared to hypodivergent and normodivergent growth patterns. These findings highlight the necessity of integrating both sagittal and vertical skeletal assessments in clinical planning to ensure safe and effective miniscrew insertion, particularly in high-risk groups such as Class II hyperdivergent patients.
A study conducted by Oliveira et al. reported that the trajectory of the IANC differed according to vertical growth pattern: in hypodivergent and normodivergent cases, the canal coursed adjacent to the root apices, whereas in hyperdivergent individuals it was located closer to the inferior border of the mandible, with ramifications extending towards the apical region. 22 Notably, the methodology for orienting the jaws was not clearly described, which could lead to inconsistencies in the measurements.
Evidence from the literature suggests that nearly 63% of neuropathic complications are associated with improperly performed invasive approach. Consequently, it is imperative for clinicians to possess a comprehensive understanding of the correlations between the anatomical positions of these molars and the IANC. 23 Such variations among placement sites possess significant risk factors during buccal shelf bone screw placement.8, 9, 12
Therefore, the insertion site distal to the second molar seems to be suitable for en masse distalization in hypodivergent individuals, whereas in hyperdivergent individuals, more mesial placement of bone screws is favorable in anterior space closure cases.
Despite the methodological standardization and clinically relevant findings derived from 2D radiographs, certain limitations of the present study must be acknowledged. Soft tissue parameters were not evaluated in this study, which opens the scope for further research. Additionally, variations in mandibular morphology and IANC position across different ethnic populations may limit the generalizability of the findings. Moreover, as this study was retrospective in nature, clinical outcome measures were not assessed. Prospective clinical studies would be beneficial to evaluate clinical success. Future research should consider additional factors, such as bone height for bone screw placement, to enhance the clinical relevance of the topic.
Conclusion
As there were no differences in the measurements of CBCT and OPG, OPG can be used as an alternative to CBCT for the evaluation of buccal shelf area, with an advantage for low radiation exposure and reduced cost.
Proximity to the IANC progressively increased in the same direction in the three distinct vertical facial types.
Hyperdivergent individuals exhibited a significant increase in proximity to the inferior alveolar canal compared to hypodivergent and normodivergent individuals.
The insertion site distal to the second molar seems to be suitable for en masse distalization in hypodivergent individuals, whereas in hyperdivergent individuals, more mesial placement of bone screws is favorable.
Footnotes
Authors Contribution
Dhanvi Desai: Designed the study, collected and analyzed data, Manuscript writing.
Alap Shah: Conceived research idea, Reviewing, provided critical revisions.
Bharvi Jani: Conceptualized & designed the study, Reviewing, provided revisions.
Adith Venugopal: Review for the manuscript.
Jhalak Vekaria: Contributed to manuscript drafting, Reviewed literature.
Sarvraj Singh Kohli: Review for the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was granted by the Institutional Ethical Committee No. KSDEC/23-24/Apr/023.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.