
Abstract
Introduction:
Altered airway and growth are interrelated; hence, a study was planned to develop a diagnostic protocol that may help in diagnosing difficult airway by utilizing routine radiographic assessment.
Material and Methods:
Lateral cephalograms of 60 children aged 12 to 14 years who were grouped based on the growth pattern into 3 groups with 20 cases each (Group 1—normodivergent cases; Group 2—hypodivergent cases; Group 3—hyperdivergent cases) were observed. The diagnostic protocol included 3 diagnostic methods (Handelman–Osborne area method, Maw et al method, and Holmberg et al method) routinely used by ENT surgeons for altered airway evaluation, and their diagnostic efficacy was correlated with McNamara’s airway analysis.
Results:
Highest specificity and diagnostic accuracy were found with Holmberg et al method followed by Maw et al method. Poor specificity was observed with Handelman–Osborne area method.
Conclusion:
The new diagnostic protocol which includes commonly used cephalometric methods by ENT surgeons can be helpful for orthodontists in early evaluation of altered airways, so that preventive and interceptive procedures can be carried out to normalize the altered craniofacial growth. Among the methods used in this diagnostic protocol, Holmberg et al and Maw et al methods had better sensitivity and specificity.
Keywords
Introduction
Abnormal breathing due to an obstructed airway produces skeletal, soft tissue, and dental malformations in a species. These are due to the altered functional demands on the craniofacial muscles and their enforced response. 1
Nasal obstruction is caused by hypertrophied adenoids, tonsils, nasal polyps, allergic conditions, and structural deformities of the nose. It usually predisposes an individual to mouth breathing, snoring, and obstructive sleep apnoea (OSA), which is a matter of grave concern not only to orthodontists but also to pediatricians, otolaryngologists, and speech therapists. Such conditions can be prevented and intercepted early, for which airway assessment is essential.
Ricketts has stressed on the need for airway evaluation, which should be done before any removal of protective lymphoid tissue, as such removal would increase velopharyngeal insufficiency and produce cleft palate speech in the affected children. 2
A lateral cephalogram is one of the diagnostic aids used by an orthodontist which can also provide important information related to the airway. McNamara airway analysis is the most commonly used cephalometric method of airway evaluation in orthodontics, but it has shown poor sensitivity, as per a study by Feres et al. 3 There are multiple diagnostic imaging techniques used by ear, nose, throat (ENT) surgeons and anesthesiologist for evaluating airway like acoustic reflection, fluoroscopy, magnetic resonance imaging, computed tomography, cone beam tomography (CBCT) and nasopharyngoscopy which have limitations of cost, availability and need of expensive specialized equipments. 4 It has been observed that orthodontists do not refer cases routinely to them prior to initiating orthodontic treatment. If airway evaluation is done along with the diagnostic tests performed by ENT specialists, the diagnostic accuracy of airway evaluation can be improved. These tests can be performed through utilizing the routine diagnostic aid, that is, the lateral cephalogram, which would be of great help in the prevention of and interception in cases involving an obstructed airway.
Several studies in the literature have used the lateral cephalogram for evaluating adenoids and the airway. Bergland 5 used a triangle to describe the bony nasopharynx based on three anatomical landmarks, the pterygomaxillare, harmonion, and basion, but this method has limitations. It may not fit the outline of the nasopharynx, as the adenoid tissue is situated anterior to it and the basion has less influence on the limits of the posterior pharyngeal wall.
Another method, described by Handelman and Osborne, is the trapezoid analysis, which provides a better evaluation of airway and adenoids using the lateral cephalogram as it delineates the limits of the bony nasopharynx clearly. 6
The method prescribed by Fujioka for assessment of the upper airway, commonly used by ENT specialists, uses the adenoidal-nasopharyngeal ratio. However, this method needs additional steps for calculations. 7 It also has low sensitivity and diminished observer correlation. 8
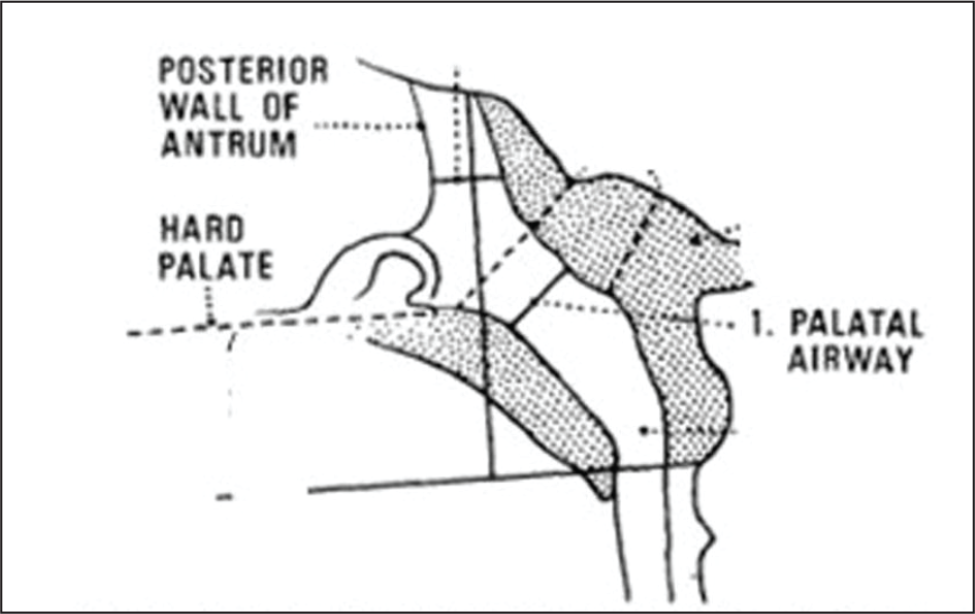
A method formulated by Maw et al has been tested for validity of the cephalometric measurements (palatal airway) through correlating them with the adenoid tissue removed during adenoidectomy. 9
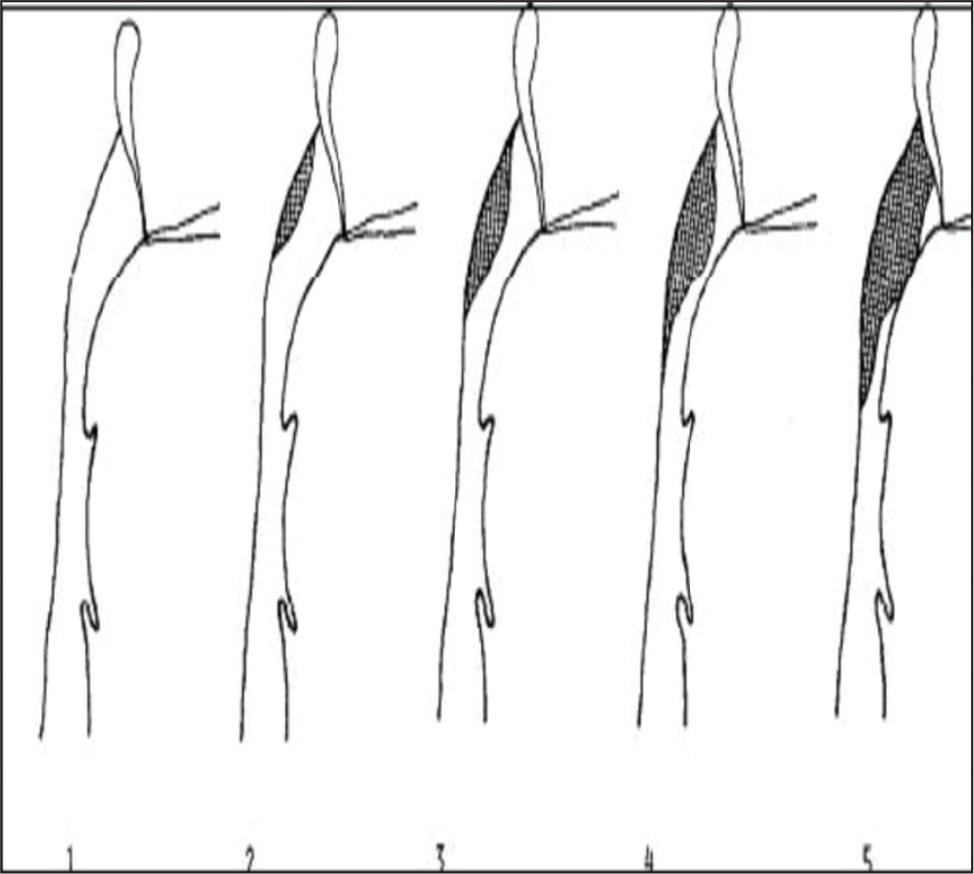
A method described by Holmberg and Linder-Aronson for evaluation of adenoid size and airway using the lateral cephalogram, consisting of five index scales, has shown good correlation with adenoid size on rhinoscopy. 10
Therefore, this study was planned to develop a diagnostic protocol that could be used by orthodontists for early evaluation of altered airways and their association with altered craniofacial growth, including the cephalometric methods commonly used by ENT surgeons (Handelman–Osborne area method, Maw et al method, and Holmberg and Linder-Aronson method), which were correlated with McNamara airway analysis.
Subjects and Methods
The study was conducted after getting approval from Institutional Ethical Committee (IEC). The pretreatment lateral cephalograms of the selected 60 children of age 12 to 14 years, in the natural head posture, keeping teeth in the maximum intercuspation, were obtained. These cases were then divided into three groups of 20 cases each, based on cephalometric parameters: group 1—normodivergent (Frankfort–mandibular plane angle [FMA] 22° to 28°, mandibular plane [MP] angle 30° to 36°, gonial angle 130° ± 7°); group 2—hypodivergent (FMA < 26°, MP angle < 32°, gonial angle < 130°); and group 3—hyperdivergent (FMA > 30°, MP angle > 36°, gonial angle > 137°). The inclusion criteria were: no history of orthodontic treatment, extractions, myofunctional therapy, maxillary expansion, and neuromuscular disorder. The exclusion criteria were: a history of missing teeth, facial asymmetry, TMJ disorders, and cleft lip and cleft palate.
Method
The diagnostic protocol for airway assessment included cephalometric methods of airway and adenoid evaluation commonly employed by ENT surgeons, such as the following:
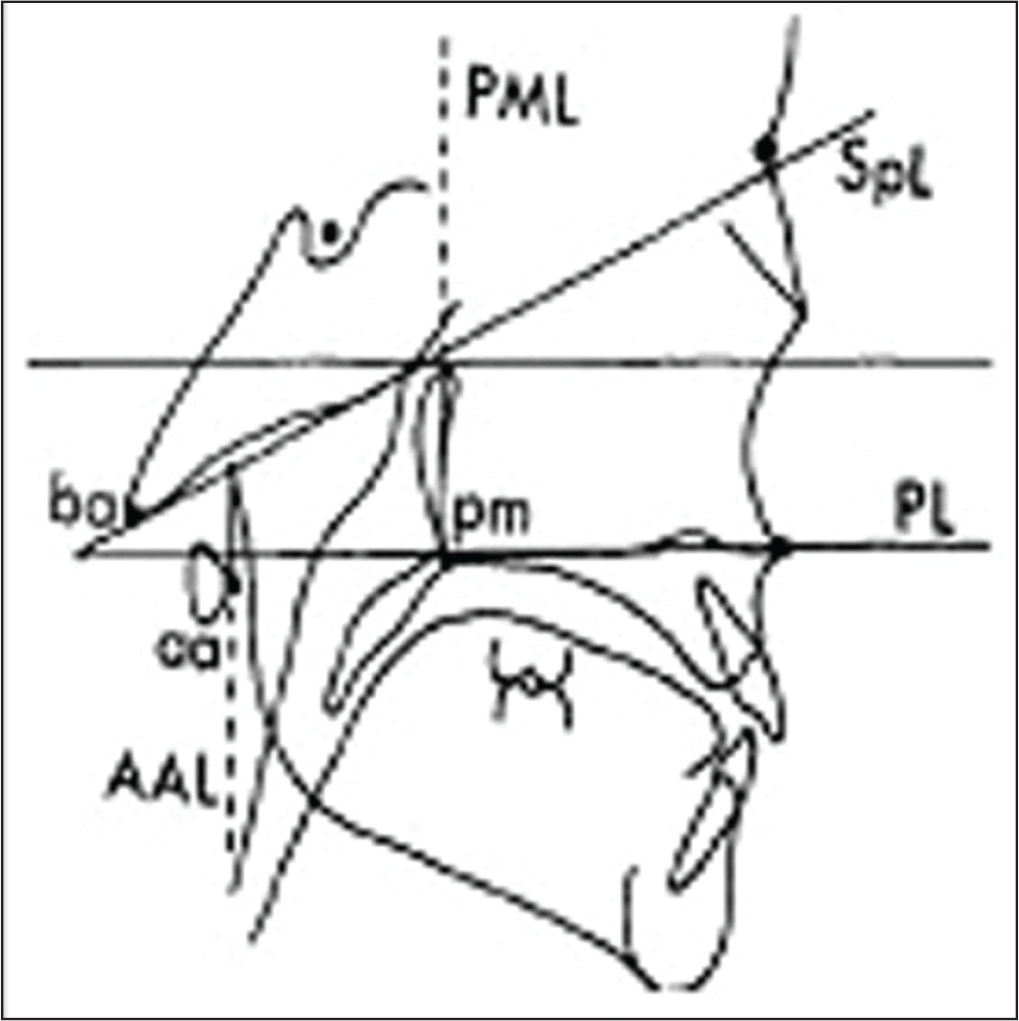
Ba: basion; SpL: sphenoid line (tangent to the lower border of sphenoid registered on Ba); PL: palatal line (anterior to the posterior nasal spine); Pm: pterygomaxillare; PML: pterygomaxillary line (perpendicular to PL registered on Pm); Aa: Anterior arch of atlas; and AAL: anterior atlas line (perpendicular to PL registered on aa).
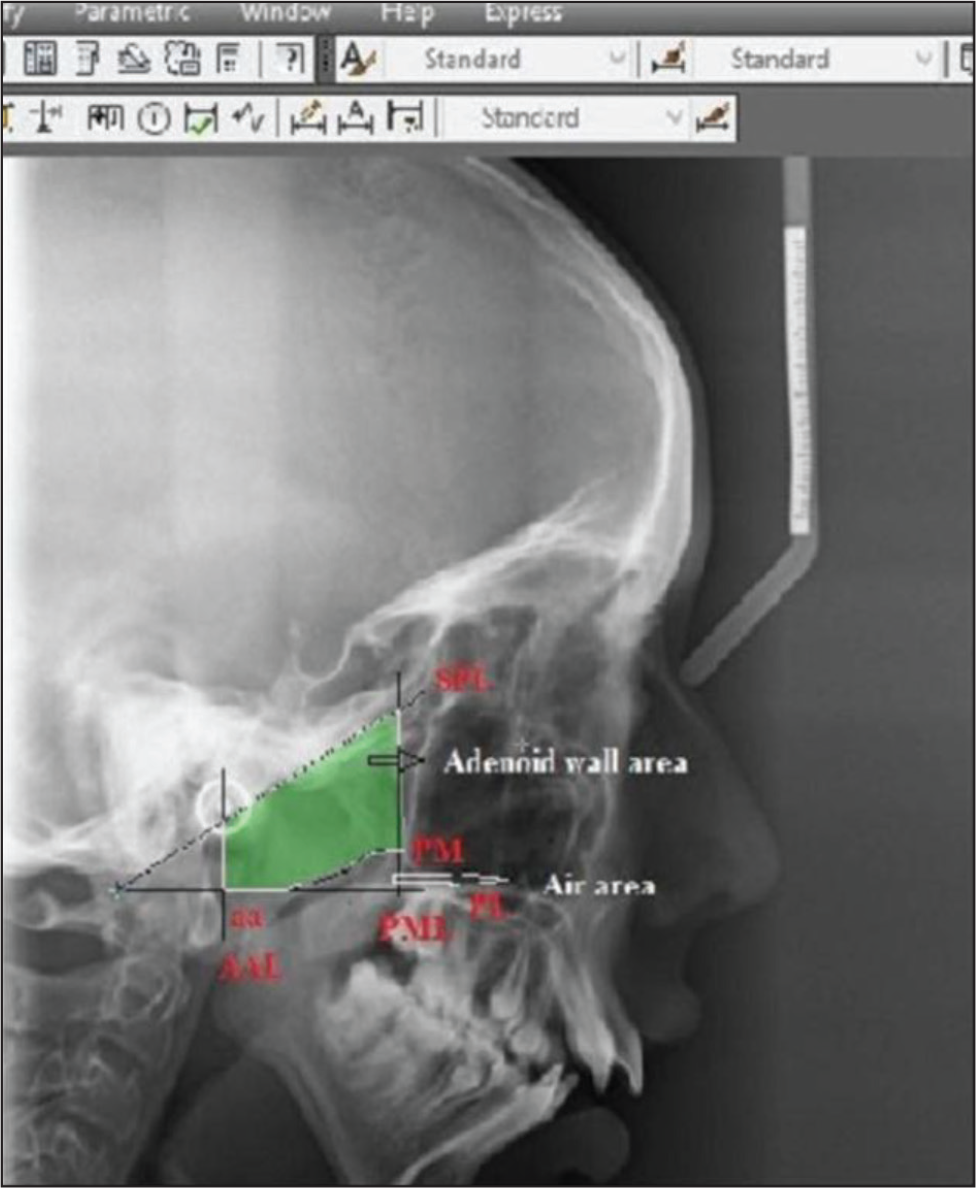
The nasopharyngeal area (Np area) is defined by four lines that form a trapezoid: the palatal line, the sphenoid line (tangent drawn to the lower border of the sphenoid registered on the basion), the anterior atlas line, and the pterygomaxillary line, which is drawn perpendicular to the palatal line registered on the pterygomaxillare (Figure 1). This trapezoid defines the Np area, which is further divided into the adenoidal-pharyngeal wall area (Ad area—that part of the Np area consisting of soft tissue, ie, adenoid or pharyngeal wall) and the nasopharyngeal airway area (air area—that part of the Np area that is airway). This is measured in millimeter square. A soft copy of the digital lateral cephalogram of a selected case in the JPG format was pasted into AutoCAD 2010 software and scaled in millimeters. Using the polyline command from the side bar menu, the required drawing was made, as shown in Figure 2. The first- and last-selected points of the image were joined, and the closed area formed represented an area. The Ad area was derived by subtracting the air area from the Np area and then compared for evaluation.
1 = No adenoids
2 = Small adenoids
3 = Moderate adenoids
4 = Large adenoids
5 = Very large adenoids
Statistical Analysis
All the findings were tabulated and subjected to statistical analysis to determine their significance using the software IBM SPSS version 17.0 (P < .05). The repeated measures ANOVA test was used for overall comparison of mean adenoid wall area, air area, palatal airway, and upper airway. The post hoc Tukey test was used for intergroup comparisons. The Kruskal Wallis test was applied for analyzing the adenoid size. Then, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy was derived for the Holmberg and Linder-Aronson method, Maw et al method, and the Handelman–Osborne area method against the McNamara method, which is widely and routinely used by orthodontists for evaluating the airway.
Results
It was observed that the specificity and diagnostic accuracy of the Holmberg and method was the best, followed by those of the Maw et al method. Specificity and diagnostic accuracy were poor in the Handelman–Osborne area method. In the present study, the highest specificity and diagnostic accuracy were found to be associated with the Holmberg and Linder-Aronson method (96.49% and 96.67%, respectively). The Maw et al method too showed good specificity (81.82%) and diagnostic accuracy (83.33%). On the other hand, the Handelman–Osborne area method had poor specificity (21.82%) and diagnostic accuracy (28.33%) (Table 1).
Sensitivity and Specificity of the Various Methods

Discussion
Adenoid hypertrophy is the most common cause of airway obstruction.
ENT surgeons need to ascertain the amount of airway obstruction before adenoidectomy for evidence-based diagnosis. Clinicians face difficulties in the history taking and examination of small children who are possible adenoidectomy candidates. A history of snoring has been correlated with the size of adenoids removed on surgery for children over 7 years of age. 12
Hibbert et al reported that the posterior rhinoscopy was an unreliable predictor of adenoid size. 13
Linder-Aronson and Henrickson found good correlation with adenoid size on rhinoscopy and on lateral cephalograms.
14
Since then, various cephalometric parameters have been used extensively by orthodontists and ENT surgeons for evaluating adenoids and upper-airway space. The other methods used commonly for evaluation of airway and adenoids include:
Handelman–Osborne area method; Maw et al method; and Holmberg and Linder-Aronson method.
Airway evaluation is also an important aspect of cephalometric diagnosis for orthodontists. However, there are very few parameters for evaluation of adenoids,one of them being commonly used is McNamara airway analysis. This analysis, when studied by Feres et al, 3 showed poor sensitivity, that is, it failed to diagnose the positive cases.
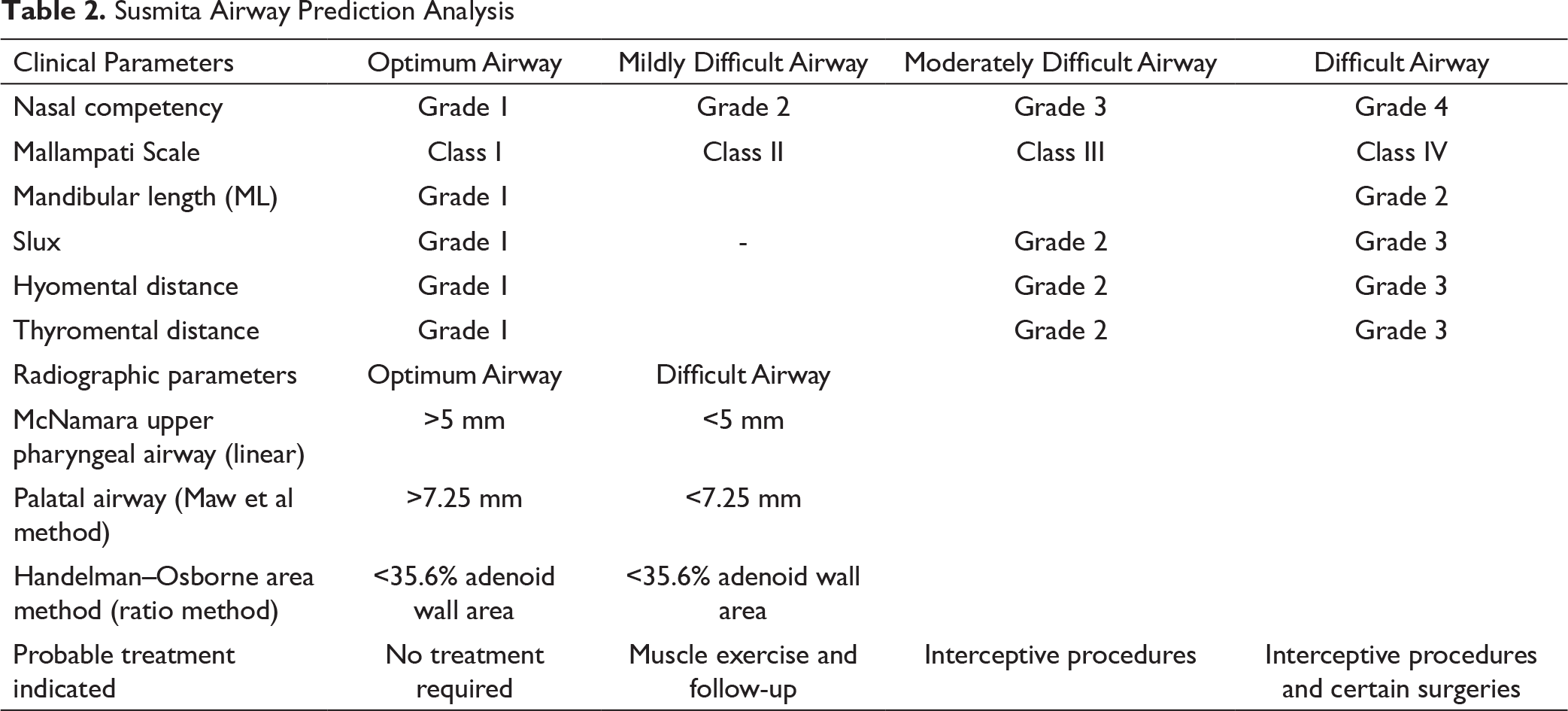
Therefore, a diagnostic protocol named ‘’Susmita Airway Analysis’’ (Table 2) was developed in the Department of Orthodontics to evaluate airway difficulties and was correlated with growth pattern and malocclusion. As class II cases are more prone to airway difficulties, this group was selected.
Some of the cephalometric methods from this protocol were used for airway and adenoid assessment in the present study for the selected cases. These included:
Handelman–Osborne area method; Maw et al method (palatal airway); Holmberg and Linder-Aronson method; and McNamara airway analysis.
Then, the sensitivity, specificity, and diagnostic accuracy of each method were calculated and compared with those of McNamara airway analysis.
In the present study, the highest sensitivity, specificity, and diagnostic accuracy were found to be associated with the Holmberg and Linder-Aronson. method (100%, 96.49%, and 96.67%, respectively) (Table 1). For deriving the sensitivity and specificity of this test, grades 1 to 3 adenoid sizes were considered to be nonobstructive, and grades 4 and 5 adenoid sizes were considered as obstructive.
Major et al also reported in their systematic review that Holmberg and Linder-Aronson’s subjective method of adenoid assessment had a fair correlation with the adenoid size evaluated using endoscopy. 15
Souki et al observed 78% (moderate) sensitivity and 91% (high) specificity using a similar method. 16 In the present study, a similar method could diagnose cases with better sensitivity (100%) and specificity (96.49%). Thus, this method could be useful for orthodontists in treating cases with airway obstruction due to adenoid hypertrophy, as preventive and interceptive procedures can be carried out.
In the present study, the Handelman–Osborne method showed good (100%) sensitivity but poor specificity (21.82%) (Table 1). The cut-off value for this parameter was set at 35.6% of the adenoid wall area for males and 39.9% for females. However, Souki et al found moderate sensitivity (75%) and good specificity (94%) using the same method. 16 Nevertheless, the limitation of the Handelman–Osborne area method was its inability to measure the transverse dimension of the nasopharynx. It is difficult and time-consuming, needing specialized equipment (planimeter) or software for calculating the airway area.
In the present study, 100% sensitivity, 81% specificity, and 83% diagnostic accuracy were observed using the linear method proposed by Maw et al (Table 1). The cut-off value was set at 7.25 mm for this parameter. Major et al, in their systematic review on the assessment of a lateral cephalometric diagnosis of adenoid hypertrophy and posterior upper airway obstruction, observed that the Major et al method had good correlation with the volume of adenoid tissue removed during adenoidectomy (r = 0). 15 Feres et al evaluated radiographic parameters designed to investigate adenoid hypertrophy and nasopharyngeal obstruction against videonasopharyngoscopy. They observed moderate correlation with the palatal airway and measured choanal obstruction on videonasopharyngoscopy clips. They found that the palatal airway parameter had 81.8% sensitivity and 70.8% specificity. 17 In the present study, the same parameter was used, and better sensitivity (100%) and specificity (81.82%) were observed. Thus, the palatal airway could be used for evaluating airway space by orthodontists for identifying cases of obstructed airway to carry out needful preventive and interceptive measures. Bitar et al conducted a study to evaluate the correlation between palatal airway, shortest adenoid distance and most convex adenoid distance on lateral cepalograms. 18 They graded adenoids as: grade 1—indicating less-than-50% airway obstruction; grade 2—indicating more-than-50% airway obstruction; and grade 3—indicating near-total airway obstruction. They found good correlation with this parameter. Present study too found a good sensitivity and specificity using same parameter (palatal airway).
Conclusion
This study concludes that the diagnostic protocol that includes cephalometric methods of airway evaluation commonly employed by ENT specialists is also useful for orthodontists for early evaluation of an altered airway. Using Susmita Airway Prediction Analysis, orthodontists can carry out preventive and interceptive measures to normalize the altered craniofacial growth for better general health and well-being. Among the methods used in the diagnostic protocol, the Holmberg and Linder-Aronson method and Maw et al method have better diagnostic accuracy.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.