
Abstract
Aim:
To determine the correlation between palatal rugae (PR) pattern and subjects with vertical, average, and horizontal growth pattern and to determine gender variation if any.
Material and Methods:
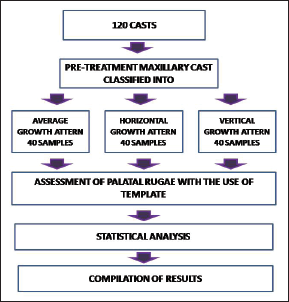
One hundred and twenty study models were divided into horizontal, vertical, and average growth patterns with 40 (20 males and 20 females) samples in each group. The pattern of PR was assessed in each group using a template.
Result:
Type B (wavy type) PR occurs more often in horizontal and average growth pattern (80% and 72.5% respectively), whereas its occurrence in vertical growth pattern subject is the least among other growth patterns, that is, 42.5% of the total subjects. Type E (curved type) PR has appeared highest in 27.5% of average growth pattern patient followed by 12.5% of vertical growth pattern subjects. The occurrence of type E PR is least in horizontal growth pattern which is just 5% of the total subjects.
Conclusion:
Curved-type PR was more prevalent in vertical and average growth patterns. Diverging PR pattern was mainly seen in vertical growth pattern. PR also shows sexual dimorphism. The association is clinically significant as it will lead to determination of facial vertical growth pattern at early age; thus, it serves as a diagnostic adjunct for different malocclusions very early in life and aids in preventive or interceptive orthodontic measures to alleviate forthcoming growth pattern.
Keywords
Introduction
A number of factors such as tooth size, teeth arrangement, arch size, arch shape, jaw size, jaw relationship, and soft tissue factors play a significant role in skeletal and dental development. 1 Growth pattern plays a significant role in growth modulation; thus, its evaluation plays a major part in orthodontic diagnosis and treatment planning during adolescence. Various techniques have been used in the past for accurate prediction of both magnitude and direction of craniofacial growth. However, prediction of abnormal growth variation is still limited due to complex interaction of genetic and environmental factors affecting growth.1-3
Palatal rugae are situated in the anterior portion of the palate on either side of the mid palatal raphe and just behind the incisive papilla. They are ridges that extend up to one-half of the distance. 4 PR are formed from the connective tissue in the palatine bone in the third month of intrauterine life. Development of PR is controlled by epithelial–mesenchymal interactions. 5
In forensic odontology, stomatognathic system plays an important role in identification. In case of missing teeth, PR are used as an alternative. Palatoscopy is identification of a person by studying their PR. 6 Sexual dimorphism is seen in PR pattern. The position, uniqueness, regional difference, and antemortem resistance provide a reliable source for identification 7 ; thus, PR can be used for sex differentiation. 8 However, PR has little use in orthodontics, which is a stable reference plane in cast superimpositions.
For proper diagnosis and treatment plan of skeletal malocclusion, it is beneficial to identify the malocclusion early during growing stage. Stability and non-influential nature of PR helped us formulate the hypothesis that different facial divergence may show a correlation with PR. The correlation of growth pattern and PR pattern is clinically significant as this association will help in determination of facial vertical growth pattern at an early age by determining the rugae pattern in the individual. This in turn may be used as a diagnostic adjunct for determination of malocclusions very early in life and help in preventive treatment as well as interceptive treatment to alleviate forthcoming growth pattern.
Material and Methods
The sample size has been estimated using GPower Software v. 3.1.9.2. Considering the effect size to be measured (f) at 30%, power of the study at 80%, and the margin of the error at 5%, the total sample size needed is 111, which is rounded off to 120. Thus, each study group will comprise of 40 samples.
The present study was conducted retrospectively after obtaining study records of 120 young adult patients who had reported to OPD of Department of Orthodontics. The study was conducted after obtaining institutional ethical clearance.
The inclusion criteria for the sample were age group—15 to 30 years, South Indian ethnicity, complete complement of permanent teeth till second molars, study models with well-defined rugae, and lateral cephalograms taken in natural head position. Exclusion criteria were history of previous extraction of teeth/orthodontic treatment, congenital/ acquired deformity of head and neck, and deleterious habits.
Ethnicity of patient was determined through family history where both the mother and father are from South Indian ethnicity. Lateral cephalograms of the patients were assessed for determining the growth pattern. Angular measurement from Sella-nasion to gonion-gnathion (16° to 35°), Frankfurt-mandibular plane angle (26° to 38°), Y-axis (53° to 66°), and Jarabak’s ratio (62% to 65%) were the parameters considered to decide upon the growth pattern.
The sample was classified into 3 groups on basis of their growth pattern.
Average growth pattern; Horizontal growth pattern; and Vertical growth pattern.
After determining the growth pattern, the patients were divided in 3 groups with 40 samples (20 males, 20 females) in each group.
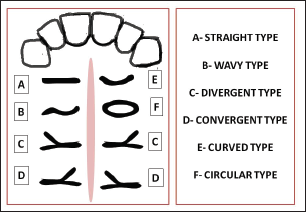
All study casts poured in orthocal were assessed by single investigator who was blinded. Primary PR (rugae length >5 mm) were marked using a 0.3-mm graphite pencil. PR was classified according to the Thomas and Kotze classification and was recorded under each group (Figure 1). 9 The study design is provided in Figure 2.
Template Used to Identify the Rugae Type.
Study Design.
Statistical Analysis
Statistical Package for Social Sciences (SPSS) for Windows Version 22.0 (Released 2013. Armonk, NY: IBM Corp.) was used to perform statistical analyses.
The level of significance was set at P < .05.
Result
As the sample was equally divided between the two genders among different growth patterns, we were able to tabulate the result of full sample as well as the result for each gender.
The results of Figure 3 showed the rugae pattern type (type A to F) occurrence among different growth patterns of the whole sample, out of which type B and E gave a statistically significant results. Type B (wavy type) PR occurs more often in horizontal and average growth pattern (80% and 72.5%, respectively), whereas its occurrence in vertical growth pattern subject is the least among other growth patterns, that is, 42.5% of the total subjects.
Prevalence of Various Palatal Rugae Patterns Between Different Growth Patterns in Total Samples.
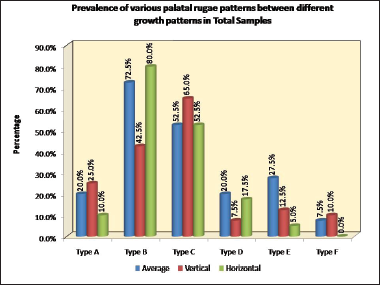
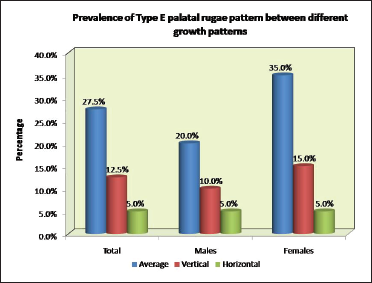
Type E (curved type) PR has appeared highest in 27.5% of average followed by 12.5% of vertical growth pattern subjects. The occurrence of type E PR is least in horizontal growth pattern which is just 5% of the total subjects.
After using z test for proportion, as shown in Figure 4, for comparison of type B PR between the 3 growth patterns, there is significance seen between average and vertical with difference of 30% and between vertical and horizontal of pattern of – 37.5%.
Prevalence of Type B Palatal Rugae Between Different Growth Patterns.
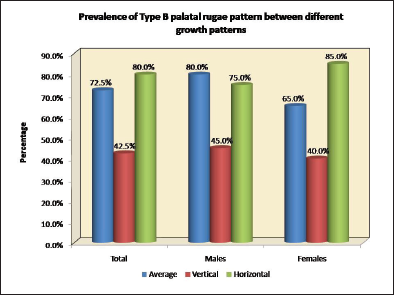
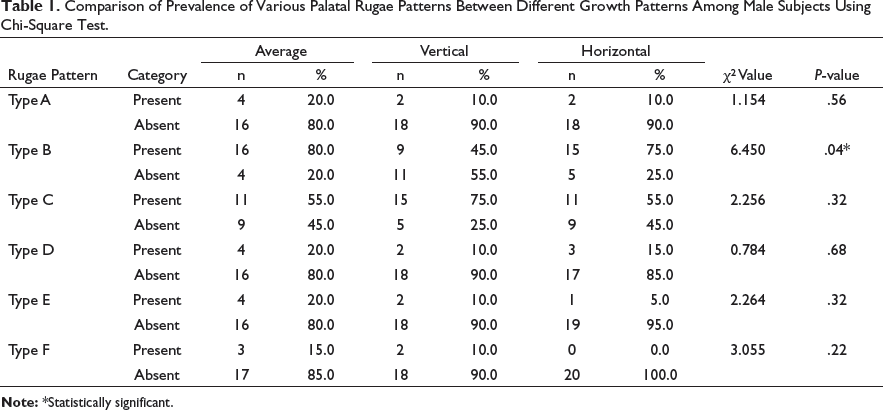
After using z test for proportion, for comparison of type E PR between the 3 growth patterns, there is significance seen between average and horizontal of pattern of – 22.5%, which is depicted in Figure 5. Comparison of prevalence of various Palatal Rugae patterns between different growth patterns among male subjects using Chi-Square Test is shown in Table 1, type B PR was more prevalent in horizontal and average growth pattern (75% and 80% respectively) whereas least prevalent in vertical growth pattern male patients which accounts to only 45% of the male sample.
Prevalence of Type E Palatal Rugae Between Different Growth Patterns.
Comparison of Prevalence of Various Palatal Rugae Patterns Between Different Growth Patterns Among Male Subjects Using Chi-Square Test.
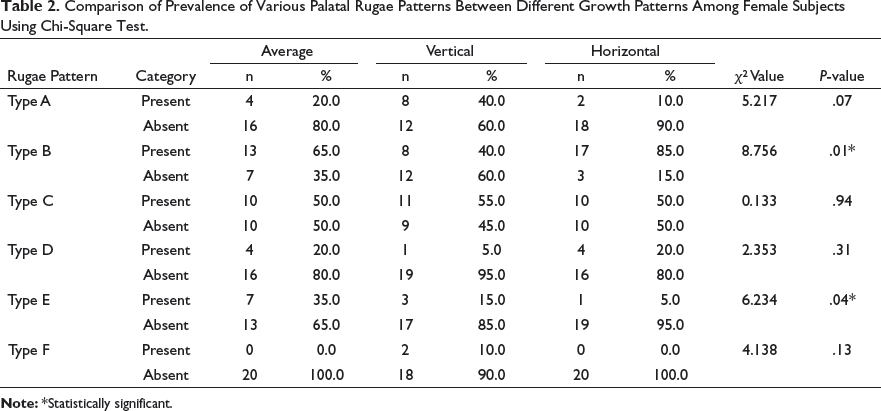
Comparison of Prevalence of Various Palatal Rugae Patterns Between Different Growth Patterns Among Female Subjects Using Chi-Square Test.
Discussion
Vertical control is considered as a significant factor during any orthodontic treatment. Downward and forward maxillary and mandibular displacement has been replaced to more vertical displacement in many patients which leads to extended treatment timing, compromised treatment objectives, and poor soft tissue changes. Most of the treatment modalities used for vertical control often depend on patient’s compliance, and it is also difficult to identify the patients who need vertical control. 10
Palatal rugae analysis may serve as an important diagnostic aid in identifying growth pattern earlier in life as they are considered unique to each individual. Their shape, direction, and unification remain stable throughout life. 11 PR is an internal structure in the head; thus, it is protected from high temperature and trauma and also resists secondary shape change. 12 PR can aid in early identification of malocclusion as it remains stable after its establishment early in intrauterine life.
In contrast to this study, a pilot study by Kapoor et al does not support stability of second and third primary rugae (medial and lateral rugae points) in individuals treated with midpalatal expansion for forensic identification. 13
The stability and non-influential nature of PR led us to formulate the hypothesis that different facial divergence may show a correlation with PR which is performed in our study. This in turn may be used as a diagnostic adjunct for determination of malocclusions very early in life and help in preventive treatment as well as interceptive treatment to alleviate forthcoming growth pattern.
Many techniques are available for analysis of PR. One of the most common methods is intraoral examination which is easy and also economical. A disadvantage in this method is inability to maintain a record for future reference. 14 To overcome this disadvantage, oral impressions and photographs can be used. Dental cast has an added advantage, that is, it can be performed anywhere in a laboratory, is easy to perform, and economical. 15 In our study, dental casts were used as it is an essential diagnostic aid and, thus, readily available. Classifications given by Hauser et al 16 and Thomas and Kotze 9 are commonly used in the field of forensic odontology. Due to the simplicity of understanding and repeatability, in our study, we have considered Thomas and Kotze classification. 9
Studies have been conducted to determine the stability of PR during growth and effect of different treatment modalities on the rugae position, which led to the conclusion that headgear treatment leads to significant changes in lateral points of PR, whereas medical points are relatively stable and a suitable anatomic reference point. 17 Thus, the primary medial rugae were assessed in this study for attaining unbiased results.
Various studies have been performed to understand the prevalence of PR type in different ethnic groups. In their study, Kapali et al 18 compared the PR pattern in Australian Aborigines and Whites and found that the rugae pattern of Australian aborigines displayed more number of primary rugae when compared to the latter. Australian Aborigines had prominently curved and wavy type of PR. 18 Similar studies by Kashima 19 and Shetty et al 20 compared Indian population with Japanese and Tibetan population which revealed significant differences in PR pattern.19, 20
In their study, Nayak et al concluded that there is a statistically significant difference in PR shape when South Indian and Western Indian population group was compared. 21 As there has been a significant difference of PR pattern within ethnic group, in the present study, South Indian population was considered. Nayak et al also showed no sexual dimorphism in his study. 21 Present study also showed statistically different results among male and female population, thus confirming the sexual dimorphism in palatal rugae pattern. In various ethnic populations, malocclusion can be investigated and correlated with specific PR pattern. Thus, PR pattern aid in intercepting different malocclusions at a very early age. 22 This article is the first one to compare PR to the growth pattern for interception of growth pattern at early age.
A study by Kapoor et al concluded that all malocclusions have similar number of primary, secondary, and fragmentary rugae except class II div 2. Forking diverging type of PR is distinct in class III malocclusion. 23 In our study, diverging PR pattern was mainly seen in vertical growth pattern but was not significant. There was a significant result with relation to wavy and curved type of PR. Wavy PR pattern was most prevalent in average and horizontal growth pattern and least prevalent in vertical growth pattern. We saw the same result when genders were separately evaluated.
Curved type of PR had a decreasing prevalence by being most prevalent in average growth subject, moderately prevalent in vertical growing subjects, and least prevalent in horizontal growth pattern subjects. Similar results were obtained in female subjects. However, when male subjects were considered, the curved type of PR results was not significant. This shows that there was a sexual dimorphism in our population.
We were not able to accomplish a definite correlation of each PR type to particular growth pattern. Further studies on large growth pattern would be necessary to come to a definite conclusion.
Conclusion
There was a correlation observed in wavy type PR with horizontal and vertical growth pattern.
Curved type PR was more prevalent in vertical and average growth pattern.
Diverging PR pattern was mainly observed in vertical growth pattern.
Palatal rugae show sexual dimorphism. Type B PR was more prevalent in average growth pattern and horizontal growth pattern whereas least prevalent in vertical growth pattern of male patients. Type B PR was more prevalent in average growth pattern and horizontal growth pattern whereas least prevalent in vertical growth pattern of female patients. Type E PR was also most prevalent in female subjects with average growth pattern followed by female with vertical growth pattern and least prevalent in female patients with horizontal growth pattern.
Clinical Significance: For proper diagnosis and treatment plan of skeletal malocclusion, it is beneficial to identify the malocclusion early during growing stage. Stability and non-influential nature of PR helped to formulate the hypothesis that different facial divergence may show a correlation with PR. The correlation of growth pattern and PR pattern is clinically significant as this association will lead to determination of facial vertical growth pattern at an early age by determining the rugae pattern in the individual. This in turn may be used as a diagnostic adjunct for determination of malocclusions very early in life and help in preventive treatment as well as interceptive treatment to alleviate forthcoming growth pattern.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.