
Abstract
Objective
This study aimed to evaluate the prevalence and patterns of impacted mandibular third molars (MTMs) and their association with distal caries in adjacent mandibular second molars (MSMs).
Methods
A total of 2000 randomly selected orthopantomograms (OPGs) were analyzed. MTM impaction patterns were classified using Winter’s and Pell-Gregory systems, and distal caries on MSMs were assessed. Statistical analyses included chi-square tests and multivariate logistic regression to evaluate associations between impaction characteristics and caries prevalence.
Results
Of the 1594 eligible OPGs, 37% exhibited MTM impactions. Among the 828 impacted MTMs identified, 19.56% were associated with carious lesions on the distal surface of adjacent MSMs. Statistical analysis revealed that mesioangular impactions significantly increased the likelihood of distal caries in MSMs. In contrast, Pell-Gregory Classes II-C and III-C were associated with reduced odds of caries. Age emerged as a strong predictor, whereas gender and other Winter’s classification categories did not significantly influence caries occurrence.
Conclusion
Impacted MTMs are associated with an increased risk of caries on the distal surface of MSMs. Impaction patterns and patient age influenced the prevalence of caries. Prophylactic removal of impacted MTMs in high-risk cases may help reduce the risk of caries development in MSMs.
Introduction
An impacted mandibular third molar (MTM) is one that has not erupted into its correct position in the dental arch within the expected developmental timeframe. Its eruption may be obstructed by adjacent teeth, bone, or soft tissue, resulting in either complete or partial impaction. 1
Several factors influence tooth impaction. 2 Genetics plays a significant role, as hereditary factors can determine tooth development and positioning. 3 A discrepancy between arch length and tooth size can lead to impaction when there is insufficient space for the teeth to erupt. 4 Late eruption also contributes, as teeth that emerge later may not have enough room. Additionally, pathological conditions such as cysts or tumors can obstruct the eruption path of a tooth. 5
Impacted MTMs, although often asymptomatic, can result in complications such as bone loss, periodontal pathologies, pericoronitis, distal caries or root resorption affecting adjacent mandibular second molars (MSMs), and the development of odontogenic tumors or cysts.2,6–10
Caries on the distal surface of the MSM are frequently associated with an impacted MTM. This association is primarily attributed to the eruption pattern of the MTM, which often leads to chronic food impaction and difficulty in maintaining adequate oral hygiene in the area between the two molars.11,12 From a clinical perspective, an impacted MTM significantly complicates root canal therapies and restorative procedures on the distal surface of the adjacent MSM. The proximity of the MTM creates challenges in accessing the affected area, further compounded by limited visibility and inadequate lighting during treatment. 13 Additionally, placing a matrix band for a Class II preparation on the MSM can be particularly challenging if the proximal box is deep, situated on an undercut, or associated with a concave root structure. 14
These clinical complexities, particularly the increased risk of distal caries and treatment challenges, often question the management of impacted MTMs. While the decision to extract a symptomatic MTM is straightforward, the prophylactic extraction of asymptomatic MTMs remains controversial due to conflicting evidence.15–17 Some studies suggest that prophylactic removal can prevent pathological changes, including distal caries and periodontal issues in adjacent MSMs.17–20 However, others argue that current evidence is insufficient to support or refute this practice definitively. 21 Recent research emphasizes the importance of early detection and risk assessment of pathologies associated with MTMs to address this uncertainty.10,19,22,23 Identifying high-risk cases, particularly those with specific impaction patterns and anatomical features, can guide clinical decisions on whether preventive extraction is warranted. Hence, a comprehensive approach that integrates risk assessment, anatomical evaluation, and clinical indicators is essential for making informed decisions regarding the necessity of prophylactic removal.
Building on these insights, previous studies have explored the relationship between caries on the distal surface of MSMs and the presence of impacted MTMs. Variability in findings has been reported across different populations, potentially influenced by differences in demographics, sample sizes, and methodologies.12,22,24–26
Although previous studies have explored the association between impacted MTMs and distal caries in various populations, no research has specifically addressed this topic in the Palestinian population. This study aimed to fill this gap by providing population-specific data and evaluating whether the impaction patterns of MTMs and their influence on distal caries risk in adjacent MSMs differ from those observed in other regions.
Methods
Sample selection
This retrospective, observational, cross-sectional study was conducted at a private dental center in Nablus, Palestine, and adhered to the STROBE guidelines for reporting observational studies. 27 Patient records and digital orthopantomograms (OPGs) from individuals who sought dental care at the center between January 2014 and March 2024 were retrieved and analyzed. All OPGs used in this study were obtained as part of routine dental care, with no additional imaging performed solely for research purposes. The study included patients aged 18 years or older with at least one impacted MTM. Exclusion criteria included prior extraction of MTMs or other mandibular posterior teeth, poor-quality radiographs, incomplete root formation of MTMs, craniofacial or dental anomalies, pathologies, syndromes, or a history of orthodontic treatment. Findings were cross-checked against the center’s database to ensure data accuracy and avoid diagnostic limitations associated with panoramic radiography. Records with discrepancies, incomplete data, or missing information were excluded to maintain methodological consistency and minimize potential biases.
The OPGs were acquired using the Carestream 8100 digital X-ray machine, and the images were processed with its software. All patient details were fully de-identified before analysis to ensure anonymity and confidentiality, and no identifiable information was used in the study. Ethical approval was obtained from the Institutional Review Board of the Arab American University (Approval Number: 2024/A/9/N), and the study was conducted in accordance with the Helsinki Declaration of 1975, as amended in 2013.
Sample size calculation
To estimate the prevalence of impacted MTMs, the required sample size was calculated to be 273 radiographs, assuming a prevalence rate of 23.05%, a 95% confidence level, and a 5% margin of error. A prior study conducted in a regional population informed both the 23.05% prevalence assumption and the finding that, on average, each patient has 1.49 impacted MTMs. This yielded an expected total of approximately 407 impacted MTMs within the sample radiographs. 11 However, the sample size was increased to 2000 OPGs to ensure adequate representation of less common Winter’s and Pell-Gregory classification subgroups and to enhance statistical power for subgroup analyses. This approach reduces the risk of Type II errors (false negatives) and improves generalizability by capturing a broader spectrum of impaction patterns and associated risks. It aligns with a previous study that similarly increased the sample size to account for subgroup variability and ensures sufficient power to detect significant associations. 11
Subgroup sample size calculations for Winter’s and Pell-Gregory classifications were informed by prior research to ensure sufficient statistical power for detecting significant differences in caries risk. 11 Using data from a previous study, the mesioangular group in Winter’s classification, which had a distal caries rate of 24.3%, was used as the reference. Distal caries rates for other subgroups were 4.5% for distoangular, 4.67% for vertical, and 11% for horizontal impactions. These proportional differences were applied as effect sizes in a power analysis, with a significance level of α = 0.05 and a power of 80% (β = 0.2). This analysis determined the required sample sizes for the current study: 43 for distoangular, 44 for vertical, and 125 for horizontal impactions. For Pell-Gregory classification, Class I-A (56.5%) was designated as the reference, with comparisons made to other classes: Class I-B (20.37%), Class I-C (4.16%), Class II-A (8.06%), Class II-B (16.99%), Class II-C (15.26%), Class III-A (0%), Class III-B (0%), and Class III-C (5.88%). A similar power analysis determined the required sample sizes as follows: 5 participants for Classes III-A and III-B, 9 for Class I-C, 12 for Class II-A, 19 for Class II-C, 22 for Class II-B, 27 for Class I-B, and 11 for Class III-C. The 2000 OPGs were randomly selected from the center’s records using computer-generated random numbers to ensure a representative and unbiased dataset. These radiographs were screened against the inclusion and exclusion criteria to identify eligible cases.
Data collection
Two experienced specialists—a certified operative dentistry specialist and a periodontist, both faculty members at the associated dental school and actively involved in daily clinical decision-making regarding the diagnosis and management of impacted MTM and associated pathologies—independently reviewed the OPGs to determine the status of MTMs and the presence of distal caries on adjacent MSMs. To ensure consistency and accuracy in data interpretation, both examiners participated in a calibration session before analysis. This included a review of the diagnostic criteria and classifications using a set of radiographs to achieve consensus. Inter-examiner reliability tests showed substantial agreement for angulation (κ = 0.8), moderate for ramus relationship (κ = 0.6), and perfect for depth of impaction (κ = 1.0). Intra-examiner reliability tests indicated excellent consistency, with both examiners showing perfect agreement for angulation and depth (κ = 1.0, p < 0.0001) and substantial agreement for the ramus relationship (κ = 0.8, p < 0.0001).
Patient gender was recorded, and age was categorized into the following groups: 18–21, 22–25, 26–29, 30–33, 34–37, 38–41, and 42–45 years. These intervals were chosen based on clinical evidence linking age to distal caries risk. 28 The narrow ranges aimed at capturing the gradual development of caries that can occur with long-term impaction of MTMs, identify high-risk groups and provide a practical framework for determining the optimal timing for interventions, such as prophylactic removal of MTMs. MTMs were classified as either absent or retained, with retained MTMs further subcategorized as impacted or non-impacted. Non-impacted MTMs were defined as fully erupted teeth that had reached the occlusal plane, while all other retained MTMs were classified as impacted. 18 Radiographs with non-impacted MTMs were further classified as bilateral (present on both sides) or unilateral (present on one side and absent on the other). Similarly, radiographs with impacted MTMs were categorized as bilateral or unilateral, with unilateral cases defined as having an impacted MTM on one side and either an absent or non-impacted MTM on the opposite side.
Impacted MTMs were analyzed using Winter’s classification for angulation and Pell and Gregory’s classification for depth of impaction relative to the occlusal plane and horizontal relationship to the ramus. These classifications are standard in the literature, ensuring meaningful clinical interpretation and methodological consistency. Radiographic analyses, including angle measurements and spatial assessments, were conducted using specialized software to ensure precision in categorizing impaction patterns. 29
Winter’s classification categorizes impacted MTMs based on the angle formed between the long axes of the MSM and the MTM. Figure 1 visually demonstrates the angulation measurement, where the long axis of the MTM was compared to the long axis of the MSM. The angle between these two lines determines the classification of the impaction into one of five categories: vertical (parallel to the MSM, within −10° to 10°), mesioangular (tilted toward the MSM, within 11° to 79°), horizontal (perpendicular to the MSM, within 80° to 100°), distoangular (angled away from the MSM, within −11° to −79°) or other (angles outside these ranges).12,30–32

Measurement of the angle between the long axes of the mandibular second molar and mandibular third molar using a digital protractor. The angle is 44.66°, which falls within the range of 11° to 79°, indicating a mesioangular impaction pattern.
Pell and Gregory’s classification assesses the depth of impaction and the horizontal relationship of the MTM to the ramus. Figure 2 demonstrates the radiographic evaluation of the impaction depth relative to the MSM’s occlusal plane. A reference line was drawn along the occlusal plane of the first and second molars to determine the position of the MTM. The highest occlusal point of the MTM was compared to this reference line and the MSM’s cementoenamel junction (CEJ) to classify the impaction depth. The classification is as follows: Class A indicates the highest point of the MTM is at or above the occlusal plane of the MSM; Class B places it between the CEJ and the occlusal plane; and Class C is below the CEJ. For the horizontal relationship of the MTM to the ramus, Figure 3 illustrates the measurement of the mesiodistal width of the MTM and compares it to the available space between the distal surface of the MSM and the external oblique ridge of the ramus. The classification is as follows: Class I indicates the available space exceeds the mesiodistal width of the MTM; Class II indicates the space is smaller than the MTM’s width; and Class III indicates no space exists between the MSM and the ramus.29,31

Radiographic evaluation of the impaction depth of the third molar. The blue line represents the highest point of the mandibular third molar, while the yellow line marks the occlusal plane of the adjacent molars. The highest point of the mandibular third molar is positioned between the cementoenamel junction and the occlusal plane of the second molar, indicating a Level B impaction pattern.
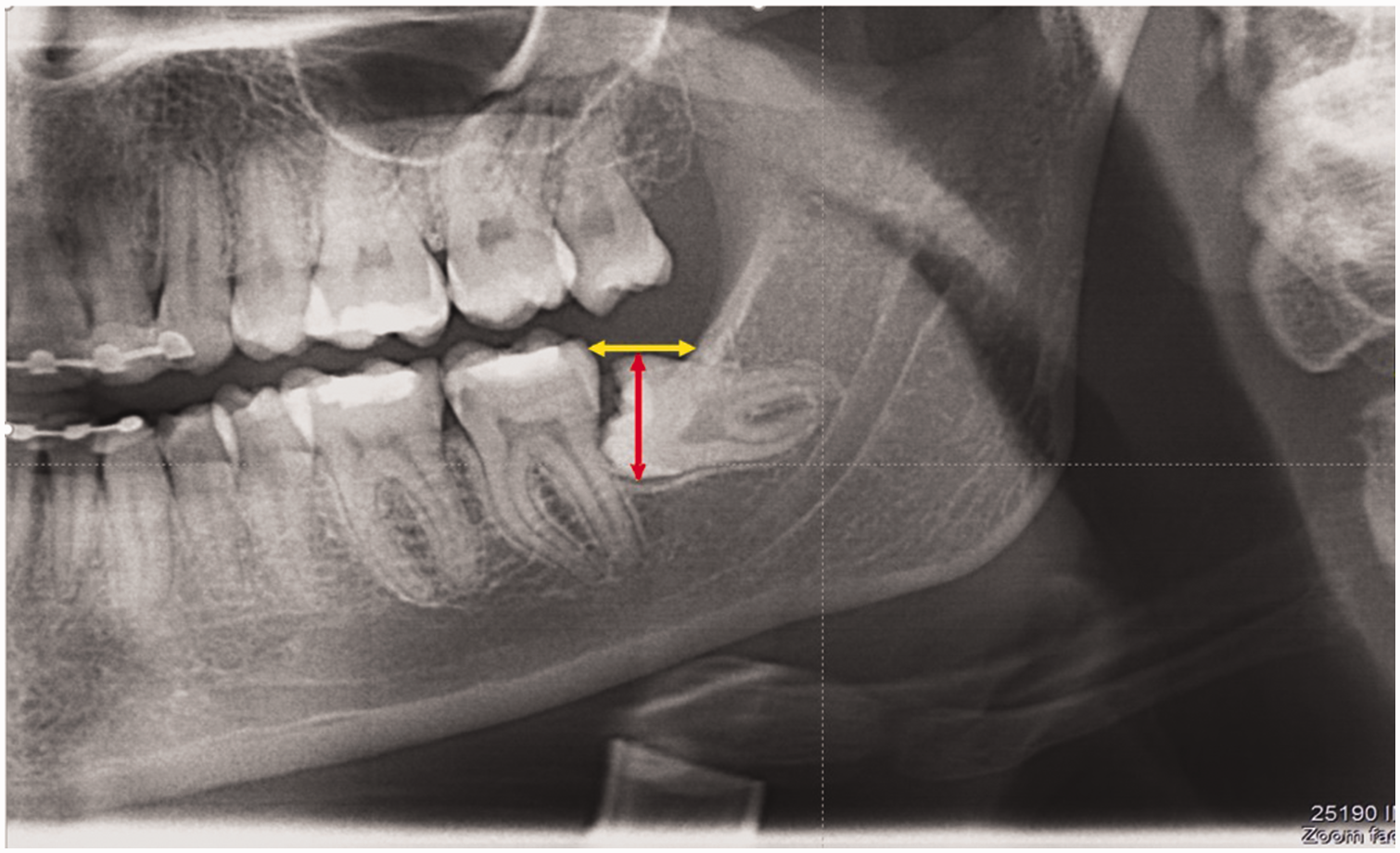
Radiographic assessment of the horizontal relationship between the third molar and the ramus. The red line indicates the mesiodistal width of the mandibular third molar, and the yellow line denotes the distance from the distal surface of the second molar to the ramus of the mandible. The mesiodistal width of the third molar is smaller than the available space between the distal surface of the second molar and the external oblique ridge of the ramus, indicating a Class II impaction pattern.
Statistical analysis
Descriptive statistics and chi-square tests were used to analyze the distribution of impaction patterns (angulations, depths, and horizontal relationship to the ramus) and examine unadjusted associations between variables such as gender, age, impaction patterns, and distal caries in adjacent MSMs. All analyses were performed using IBM SPSS Statistics V. 28 (IBM Corp., Armonk, New York, United States of America). Rows with zero observations (e.g. “Others” category in Winter’s classification) were excluded from statistical analysis to avoid distorting results.
Subgroup analyses explored differences in caries prevalence across demographic and clinical variables, including age, gender, angulation patterns, impaction depth, and ramus relationships, classified according to Winter’s and Pell-Gregory systems. Chi-square tests evaluated univariate associations, and logistic regression models assessed multivariate relationships while adjusting for potential confounders such as age, gender, Winter’s classification, and Pell-Gregory classification. Statistical significance was set at p < 0.05, with results reported as adjusted odds ratios and 95% confidence intervals (CIs) where applicable.
Results
Of 2000 radiographs screened, 406 did not meet the inclusion criteria due to poor image quality (n = 86), incomplete records (n = 67), a missing posterior tooth (n = 184), and other reasons (n = 69), leaving 1594 OPGs for analysis. Among these, 1004 radiographs had no MTM impactions; 664 had bilateral non-impacted MTMs, while 340 had unilateral non-impacted MTMs with the opposite MTM absent. Of the 1594 eligible OPGs, MTM impactions were identified in 590 individuals (37%), comprising 202 bilateral and 388 unilateral impactions. Of the unilateral cases, 203 had an absent opposite MTM, while 185 had a non-impacted MTM on the opposite side. Figure 4 visually represents the distribution of radiographs based on inclusion and exclusion criteria, categorizing MTM impactions into bilateral and unilateral cases.
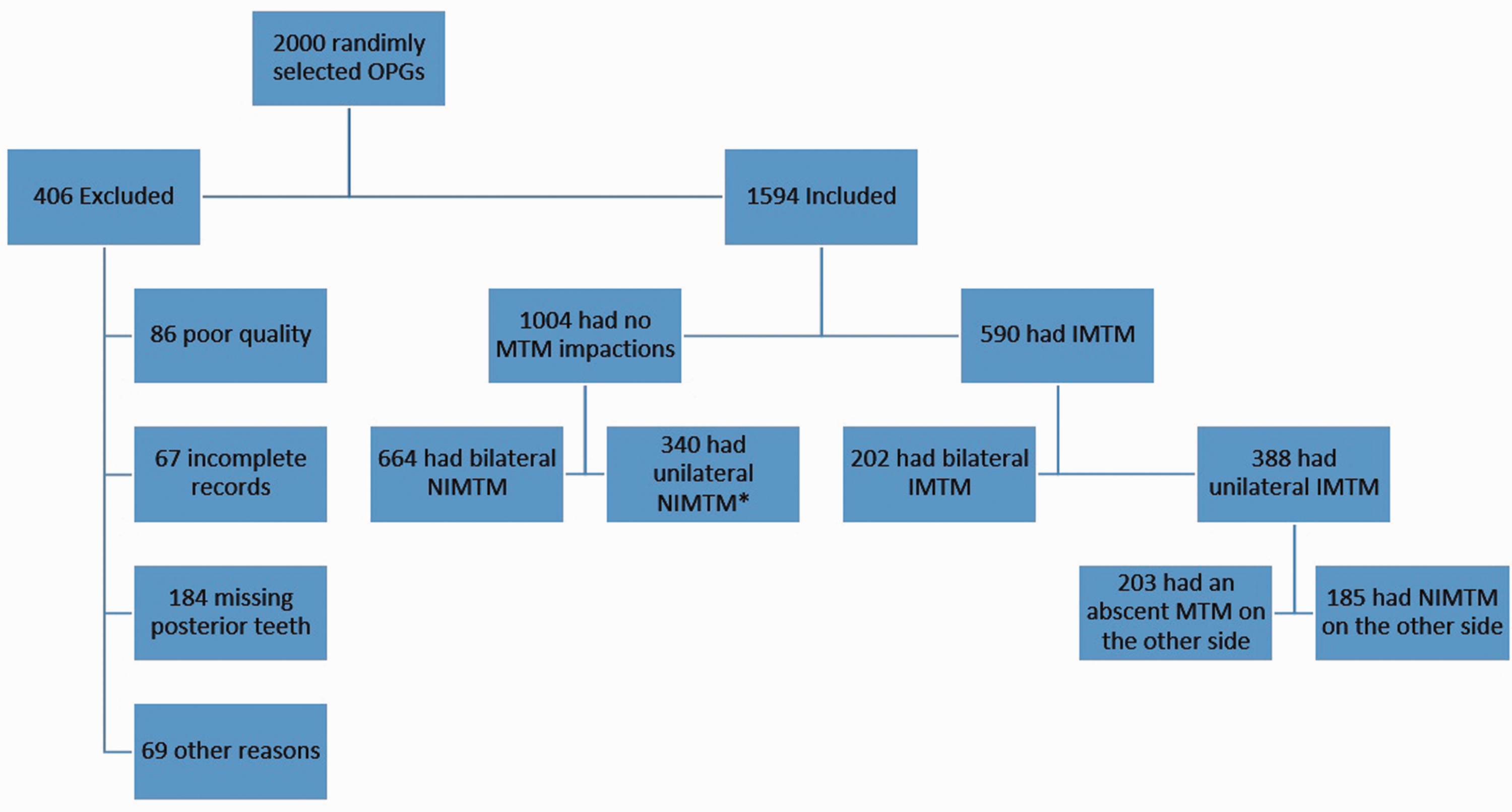
A flowchart showing the distribution of radiographs based on inclusion and exclusion criteria, categorizing MTM impactions into bilateral and unilateral cases. IMTM: impacted mandibular third molar; MTM: mandibular third molar; NIMTM: non-impacted mandibular third molar; OPG: orthopantomogram. *The mandibular third molar on the other side was absent.
In total, 828 impacted MTMs were recorded based on radiographic analysis. Of these, 57.12% (473 impacted MTMs identified in 358 OPGs—243 unilateral and 115 bilateral cases) were in females, while 42.88% (355 impacted MTMs, identified in 232 OPGs—145 unilateral and 87 bilateral cases) were in males. These findings indicate a higher prevalence of impacted MTMs in females than males, demonstrating that unilateral impactions are more common than bilateral impactions in both genders. These findings and a detailed breakdown of the data are presented in Table 1. The dataset was complete with no missing values for any of the analyzed variables, ensuring the integrity of statistical analyses.
Gender, age, and classification-based distribution of mandibular third molar impaction patterns.
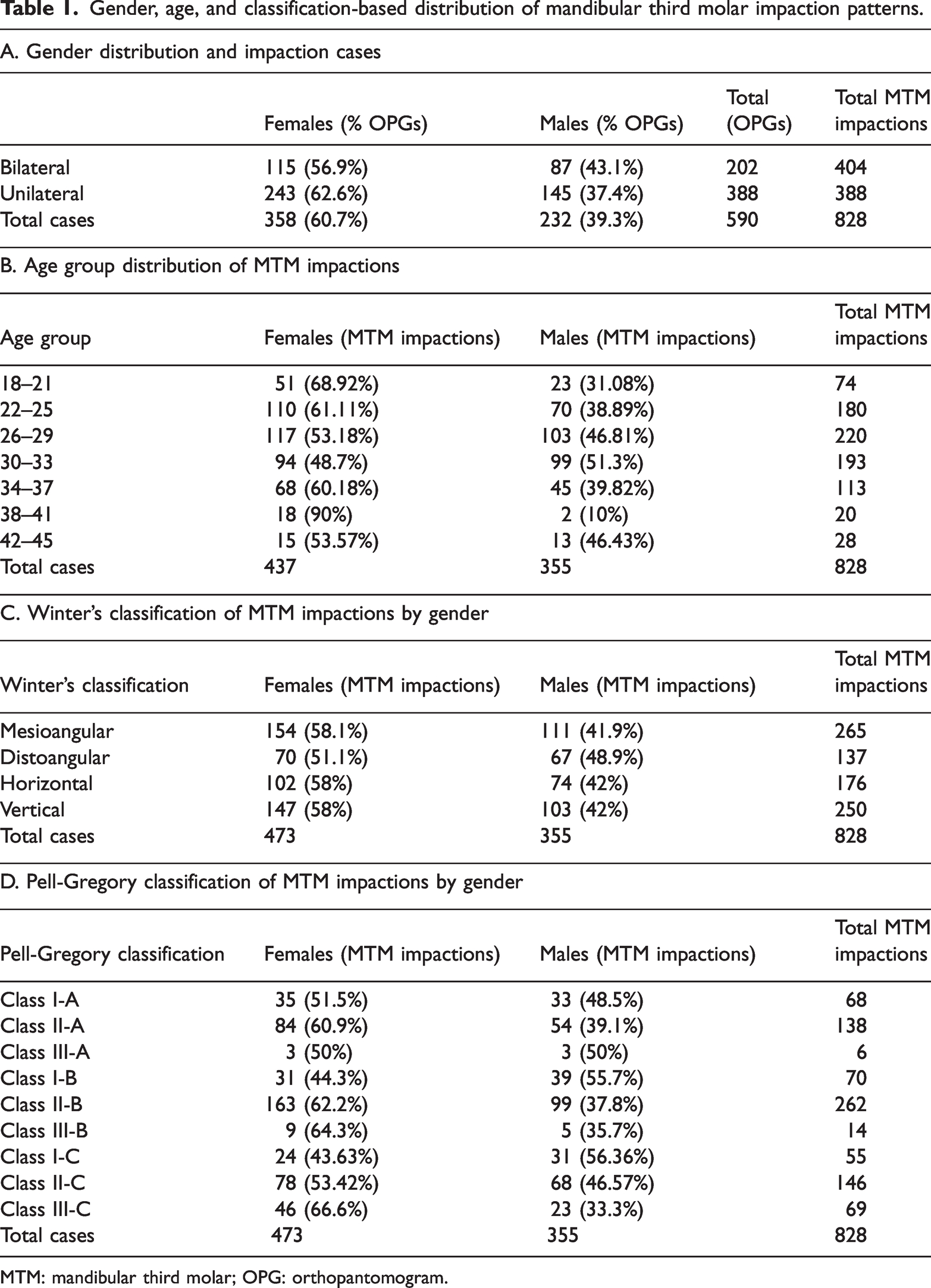
MTM: mandibular third molar; OPG: orthopantomogram.
Table 2 presents the distribution of impacted MTMs according to angulation, depth, and ramus relationship. Among the angulation patterns, mesioangular impactions were the most prevalent (32%), whereas distoangular impactions were the least frequent (16.55%). No cases were recorded in Winter’s “Others” category. The chi-square test for angulation patterns revealed significant differences in distribution (χ2 = 53.5, p < 0.001), indicating that specific angulation patterns occur more frequently than others. Regarding impaction depth, Level B was the most common (41.42%), followed by Level C (32.6%) and Level A (25.97%). The chi-square test also showed significant differences (χ2 = 29.88, p < 0.001), highlighting variations in the frequency of different depths. For the horizontal relationship of the impacted MTM to the ramus, Class II was the most frequent (65.34%), followed by Class I (23.19%) and Class III (11.47%). The chi-square test indicated significant differences in distribution (χ2 = 398.7, p < 0.001), highlighting variations in the frequency of different ramus relationship classifications of impacted MTMs.
Distribution of 828 impacted mandibular third molars by angulation, impaction depth, and ramus relationship.

MTM: mandibular third molar.
The prevalence of distal caries on MSMs adjacent to impacted MTMs was 19.56%. No significant gender-based differences were observed, with 19.66% of females and 19.43% of males affected (χ2 = 0.01, p = 0.98). A statistically significant association was found between age and caries on the distal surface of MSMs adjacent to impacted MTMs (χ2 = 62.36, p < 0.001). The prevalence of carious lesions increased progressively in younger age groups, starting at 11.66% in individuals aged 22–25 years and rising to 15.45% in those aged 26–29 years. The highest prevalence was observed in the 30–33 years age group at 35.23%, followed by a slight decline to 28.32% in individuals aged 34–37 years. The lowest prevalence was recorded in the youngest group (18–21 years) at 1.35%. The prevalence continued to decrease among older age groups, dropping to 15% in those aged 38–41 years and further declining to 10.7% in individuals aged 42–45 years.
However, the prevalence of distal caries on MSMs varied significantly based on the angulation patterns of impacted MTMs, as detailed in Table 3. Mesioangular angulation had the highest caries prevalence at 34.34%, followed by vertical (14%) and horizontal (13.07%) angulations. Distoangular angulation had the lowest prevalence at 9.49%. A chi-square test confirmed a statistically significant association between angulation patterns and the presence of distal caries on MSMs (χ2 = 55.24, p < 0.001).
Association between angulation patterns of impacted mandibular third molars and the presence of caries on the distal surface of mandibular second molars.

MTM: mandibular third molar; MSM: mandibular second molar.
A chi-square test was conducted to assess the association between the ramus-depth relationship of impacted MTMs and the presence of caries on the distal surface of adjacent MSMs. The analysis revealed a statistically significant association (χ2 ≈ 32.12, p < 0.001). Class I-C exhibited the highest prevalence of carious MSMs among the ramus-depth categories at 29.09%, followed by Class I-B at 26.87%, Class II-B at 25.57%, and Class I-A at 25%. Class II-C (14.38%), Class II-A (13.77%), and Class III-A (11.1%) had lower prevalence rates. The lowest prevalence was observed in Class III-B (7.14%) and Class III-C (2.89%). The detailed distribution of caries across ramus-depth categories is summarized in Table 4, highlighting the significant variability in caries prevalence based on the ramus-depth relationship of impacted MTMs.
Association between ramus-depth relationship of impacted mandibular third molars and the presence of caries on the distal surface of mandibular second molars.
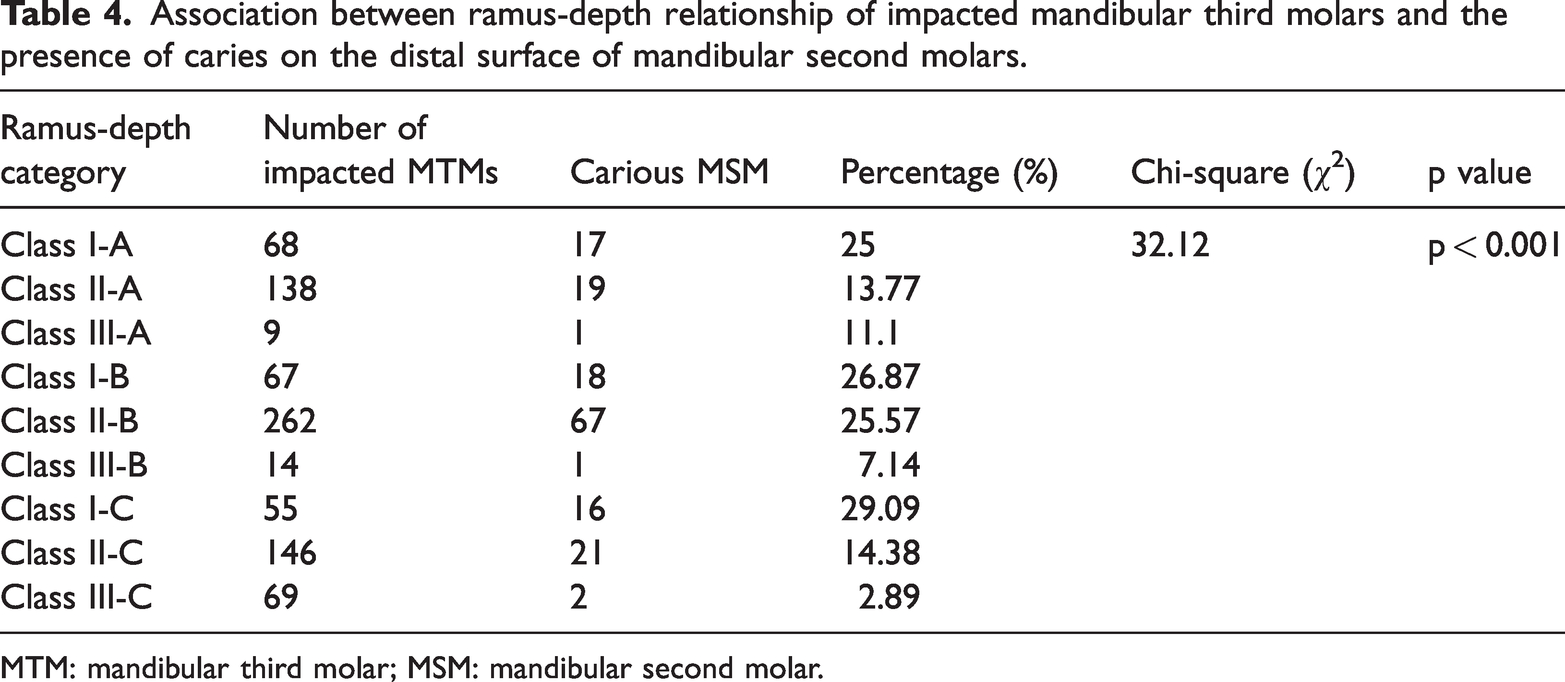
MTM: mandibular third molar; MSM: mandibular second molar.
A multivariate logistic regression analysis, summarized in Table 5, was conducted to assess the association between impacted MTM characteristics and caries on the distal surface of MSMs while adjusting for age, gender, Winter’s classification, and Pell-Gregory classification. The results indicated that mesioangular impaction of MTMs was significantly associated with higher odds of caries (β = 1.91, odds ratio [OR] = 6.76, p < 0.001). Additionally, specific Pell-Gregory classes emerged as significant predictors: Class II-C (β = −1.10, OR = 0.33, p = 0.012) and Class III-C (β = −3.26, OR = 0.04, p < 0.001) were associated with reduced odds of caries compared to the reference category (Class I-A). Age was also a significant predictor; all older age groups exhibited higher odds of caries relative to the reference group (18–21 years), with the highest odds observed in participants aged 30–33 years (β = 4.13, OR = 62.10, p < 0.001) and 34–37 years (β = 3.99, OR = 54.18, p < 0.001). In contrast, gender and Winter’s classifications for horizontal and vertical impactions were not significantly associated with caries. The logistic regression model had a pseudo R-squared value of 0.2074, indicating that it explains 20.74% of the variance in the presence of caries.
Results of multivariate logistic regression analysis assessing the association between mandibular third molar impaction characteristics and caries on the distal surface of mandibular second molars.

OR: odds ratio.
Bold indicates statistically significant results (p < 0.05).
Reference categories: Winter’s classification—Distoangular; Pell-Gregory classification—Class I-A; Gender—Female; Age—18–21 years.
Discussion
The prevalence of impacted MTM shows significant variation among populations. In this study, the prevalence was 37%, which is higher than rates reported in Hong Kong (21.1%), 9 the United Arab Emirates (23.05%), 11 Iran (23%), 33 and Saudi Arabia (27.3%). 34 However, it closely aligns with findings from Yemen (38.8%) 35 and was lower than the prevalence reported in Oman (54.3%), 36 where significantly higher rates are observed. These variations may be attributed to differences in genetic predispositions, dietary habits, access to healthcare, and racial characteristics influencing facial growth, jaw size, and tooth eruption patterns. 37 These findings highlight the importance of considering local demographic, genetic, and environmental factors when interpreting and generalizing prevalence data across populations.
This study identified 828 impacted MTMs, with a higher prevalence in females (57.12%) than in males (42.88%). This gender disparity is consistent with previous research indicating a more significant occurrence of MTM impactions in females.33,38,39 These studies suggest that factors such as differences in mandibular size, eruption patterns, or hormonal influences on dental development may contribute to this trend. However, other studies have reported no significant gender differences, indicating inconsistencies in the literature.37,40–44 Despite these discrepancies, the observed higher prevalence in females underscores the importance of incorporating gender-specific considerations in clinical evaluation and management.
The findings indicate that mesioangular impactions were the most frequent (32%), followed by vertical (30.2%), horizontal (21.25%), and distoangular (16.55%). The predominance of mesioangular impactions aligns with existing literature, consistently identifying this pattern as the most common.35,37,45 Numerous studies have similarly reported mesioangular impactions as the most prevalent, with vertical impactions ranking second.33,34,37,39,40,43 However, variations exist. Some studies have identified mesioangular and horizontal angulations as the most common,38,41 while other reports have found mesioangular to be the most frequent, followed by distoangular. 11 In contrast, Jung and Cho 46 found horizontal impactions to be the most common, with mesioangular following. Other studies have reported vertical impactions as the most prevalent, followed by mesioangular and distoangular.42,47 El-Khateeb et al. 34 also noted that most impacted MTMs had vertical angulation, followed by horizontal, mesioangular, and oblique, with distoangular being the least common. Extreme or unusual impaction angles were rare in the present study, consistent with prior research reporting minimal or no cases of such patterns.30–32 Future studies with larger sample sizes or different populations may identify cases within this category, offering further insights into rare impaction patterns.
In the current study, MTM impactions were categorized as Level B (41.42%), followed by Level C (32.6%), and then Level A (25.97%). These results align with findings of Hatem et al. 40 (44.7%), Alsaegh et al. 11 (45.5%), Eshghpour et al. 38 (63.85%), and Padhye et al. 37 (45.8%). In contrast, studies by Al-anqudi et al. 36 (58%), Zaman et al. 43 (52%), and Gupta et al. 42 (61.8%) reported Level A impactions as the most prevalent. Meanwhile, other studies identified Level C as the most common depth of MTM impaction.2,33,44 The present study also revealed that most MTMs (65.34%) were classified as Class II, aligning with findings from previous research that reported a higher prevalence of Class II impactions.11,37,38,40,42 Clinically, the depth of impaction and its relationship to the ramus are critical factors in assessing surgical difficulty and potential complications. Level B and C impactions and Class II and III impactions, often require more complex surgical techniques and pose higher risks of complications. 12
Interpreting and comparing data on impacted MTMs requires careful consideration of methodological and demographic variations. Differences in parameters such as angulation, depth, and horizontal relationship to the mandibular ramus may arise due to racial and ethnic diversity and variations in sampling methodologies. Inconsistencies in statistical analyses across studies further complicate cross-study comparisons, emphasizing the need for standardized reporting criteria. The variability in impaction patterns highlights the importance of comprehensive, individualized preoperative assessments. Such evaluations are essential for developing tailored treatment plans, providing effective patient counseling, and implementing appropriate surgical strategies for managing impacted MTMs, ultimately improving patient outcomes and reducing complications.
The study investigated the association between impacted MTMs and the presence of caries on the distal surfaces of MSMs, revealing an overall prevalence of 19.56%. This finding aligns with various studies across different populations. For instance, Özeç et al. 48 reported a 20% prevalence in a Turkish population, while Alsaegh et al. 11 observed an 18.36% prevalence among Emirati patients. Haddad et al. 12 found a lower prevalence of 12.2% in an Iranian cohort, and Tai et al. 49 reported the highest prevalence at 24.63% in a Chinese population. Chang et al. 26 identified a 17.2% prevalence in Korean patients, and Chu et al. 9 noted a 7.7% prevalence in a Hong Kong Chinese population. Although the reported prevalence rates vary across populations, the overall trend suggests that impacted MTMs are a significant risk factor for the development of caries on adjacent teeth.
The multivariate logistic regression analysis revealed that MTM impaction patterns significantly influence the risk of distal caries in adjacent MSMs. Among Winter’s classification of MTM impactions, mesioangular impactions demonstrated a statistically significant positive association with distal caries, suggesting that they are the most likely to contribute to caries development compared to other impaction angulations. In contrast, horizontal and vertical impactions did not significantly correlate with distal caries. These findings are consistent with prior studies that highlight the critical role of mesioangular impactions in distal caries development, as their angulation and proximity to the adjacent MSM create plaque-retentive areas and impede effective oral hygiene.11,12,26,28,48,50–53 The lack of significance for horizontal and vertical impactions may be attributed to their differing spatial relationships with the MSM, which reduce their potential to contribute to caries risk.
The analysis of Pell and Gregory classifications revealed that deep impactions classified as II-C and III-C were significantly less likely to contribute to distal caries on MSMs. Specifically, Class II-C and Class III-C demonstrated a statistically significant inverse association with distal caries on MSMs. These findings suggest that deeper impactions are less likely to predispose the adjacent MSM to caries, likely because their distance from the MSM reduces direct contact and plaque accumulation. These findings align with studies reporting a low prevalence of distal caries in MSMs adjacent to deeply impacted Level C and Class III MTMs.12,28,50 Conversely, classifications such as I-B, I-C, II-A, II-B, and III-B did not show statistically significant associations, indicating their influence on distal caries may be limited or inconclusive. These results underscore the importance of spatial and depth considerations when assessing caries risk associated with impacted MTMs.
Age was identified as a significant predictor of distal caries on MSMs, with progressively higher odds observed in all age groups compared to the 18–21 years reference group. The 30–33 years age group exhibited the highest odds ratio (OR = 62.10), demonstrating the strongest association with distal caries on MSMs. This likely reflects the cumulative effects of prolonged plaque retention, age-related changes in oral health, and difficulties in maintaining optimal oral hygiene over time. Although the risk of caries remained high in older age groups (38–41 and 42–45 years), it was slightly lower than the peak risk seen in the 30–33 years group. These findings, consistent with prior research, highlight the critical need for early preventive measures to address age-related increases in caries risk.25,28,48,51,52,54 Gender, however, was not found to influence the occurrence of distal caries on MSMs significantly. These findings align with previous studies that reported no significant gender differences in caries risk.25,28,54 Nevertheless, some studies have reported conflicting results, with higher caries prevalence observed in either males or females.51,52,55
Overall, the findings indicate that MTMs play a significant role in the development of distal caries on adjacent MSMs. Multiple factors influence this relationship, including impaction angulation, depth, ramus relationship, and patient age. It is consistent with prior research linking impacted MTMs to increased caries risk and periodontal complications in adjacent MSMs.10,17,49,56–58 The multivariate logistic regression model confirmed these variables as critical predictors, with a pseudo R-squared value of 0.2074, indicating that the model explains 20.74% of the variance in caries presence. While this suggests that the included predictors significantly influence caries risk, other unaccounted factors such as oral hygiene, diet, and fluoride exposure may further contribute to the outcome. These results highlight the importance of integrating these factors into comprehensive risk assessments and developing targeted preventive and treatment strategies while considering population-specific characteristics. Early identification of at-risk patients through routine dental monitoring and public education is essential to minimize complications, such as distal caries and periodontal issues. Proactive measures, including prophylactic extractions of high-risk impactions, could significantly reduce the prevalence of these complications. 59 Discrepancies in the literature, particularly regarding the role of gender, highlight the need for further research to clarify these relationships, accounting for differences in study design, demographics, and sample sizes. This evidence supports adopting a tailored, evidence-based approach to managing third molars, ensuring that interventions are optimized to improve patient outcomes.
Previous studies have utilized a variety of diagnostic modalities, including clinical examinations, 26 periapical radiographs, 60 bitewings, 61 cone-beam computed tomography (CBCT),62,63 and combinations of these methods.24,25,64 Each approach has strengths and limitations that influence diagnostic accuracy and strategy selection. This retrospective study evaluated the impaction patterns of MTMs and the presence of distal caries in MSMs using OPGs. As supported by prior research, panoramic radiography is widely recognized as a reliable tool for assessing impaction patterns and adjacent structures.11,26,28,30,32,51,53–55,57,58 While it is less accurate than bitewing radiography for diagnosing proximal caries, 65 its clinical effectiveness in the mandibular molar region has been demonstrated. 66 Moreover, OPGs are often preferred due to their accessibility and ability to examine larger sample groups without subjecting patients to additional radiation exposure. However, this method cannot evaluate demineralization and initial enamel caries alone, underscoring its diagnostic limitations. 67 Consequently, it is likely that the observed prevalence of distal caries in second molars is an underestimation of the actual value.
This study provides insights into the prevalence and patterns of impacted MTMs and their relationship with distal caries on adjacent MSMs within the Palestinian population. By utilizing widely accepted classification systems, such as Winter’s and Pell and Gregory’s, the findings can be effectively compared to studies conducted in other populations using similar methodologies. The research design was robust, involving the evaluation of a large dataset of digital OPGs, data collection by two independent researchers with high inter-examiner reliability, and applying multivariable statistical analysis. The use of multivariable analysis was a particular strength, as it helped control for confounding factors. However, despite these strengths, the exploratory nature of the findings warrants cautious interpretation due to some limitations.
One limitation is the reliance on two-dimensional radiographs, which can present diagnostic challenges. Artifacts such as overlapping enamel may obscure findings, and external root resorption could be misclassified as caries, especially in mesioangular or horizontally impacted MTMs. Additionally, the retrospective design introduces potential selection bias, as critical variables like oral hygiene practices, dietary habits, dental visit frequency, and socioeconomic status—factors that could influence caries risk—were not assessed. The absence of a control group, such as MSMs adjacent to non-impacted or absent MTMs, further limits the ability to compare caries risk between impacted and non-impacted cases. Moreover, the single-center sampling restricts the generalizability of the findings to the broader Palestinian population. Sensitivity analyses were not conducted in this study. However, the study employed a large sample size and adjusted for key confounders using multivariate analysis, enhancing the findings’ reliability. Nonetheless, the absence of sensitivity analyses limits our ability to evaluate the robustness of results under varying methodological assumptions or data-handling approaches. Future studies should incorporate sensitivity analyses to assess the stability of findings further.
Expanding the scope to incorporate variables such as oral hygiene practices, dietary habits, and dental visit frequency would provide a more comprehensive understanding of the factors influencing caries development associated with impacted MTMs. As one of the first studies to explore these associations in the Palestinian population, expanding future studies to include larger sample sizes from multiple centers across urban and rural settings would yield more definitive findings. Future studies should integrate clinical examinations and advanced imaging techniques, such as bitewing radiographs or CBCT, to overcome the limitations of relying solely on radiographs, enhance diagnostic accuracy, and validate results. Including a control group of MSMs adjacent to non-impacted or absent MTMs would also provide a valuable comparative framework to understand better the specific role of impacted MTMs in caries development.
Conclusion
In conclusion, this study found that 37% of the studied population had impacted MTMs, with prevalence and impaction patterns in the Palestinian population aligning with global trends while reflecting unique demographic characteristics. Mesioangular and vertical impactions were associated with a higher risk of distal caries on adjacent MSMs, whereas Class II-C and III-C impactions appeared to pose a lower risk. Age was a significant predictor, with the highest risk observed in individuals aged 30–33 years, whereas no notable gender differences were identified. These findings underscore the importance of early detection, regular monitoring, and prophylactic removal of high-risk impactions to prevent complex carious lesions. Patient-specific treatment plans remain essential, and further research involving diverse populations is recommended to enhance evidence-based prevention and treatment strategies for impacted MTMs.
Footnotes
Acknowledgements
None.
Author contributions
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.