
Abstract
Background:
Self-perceived orthodontic treatment need is strongly influenced by what is perceived to be the esthetic norm amongst a community, and reluctance toward treatment amongst adolescents with clinically ascertained malocclusion may often be due to readily remediable factors. Of particular interest is the prevalence of malocclusion amongst such communities as a probable indicator of the role of diet and genetics in establishing a predominant clinical phenotype that may also play a role in the construct of what is perceived as the esthetic norm amongst the community, thereby influencing the self-perceived need for treatment. Studies aimed at evaluating the association between self-perceived esthetics, and self-perceived treatment need have not been performed amongst a population with no prior exposure to orthodontic treatment
Objectives:
The purpose of this study was to evaluate the self-perceived orthodontic treatment need amongst the tribal adolescents belonging to regions with remote access to orthodontic treatment by way of a verbally assigned index and to also identify the reasons of reluctance toward treatment to better understand how to make orthodontic treatment readily accessible to such populations.
Participants, Materials, and Methods:
The agency areas of Paderu located at 18.0833°N 82.667°E and Parvathipuram located at 18°46'N 83°25'E are 2 revenue districts of Visakhapatnam and Vizianagaram, respectively, in the state of Andhra Pradesh, India, that are home to various tribal populations with remote access to orthodontic treatment. A total of 2,016 school-going tribal adolescents of the Paderu revenue division and 819 tribal adolescents of the Parvathipuram revenue division were examined to ascertain the prevalence of malocclusion. Necessary consent and permissions were obtained from the tribal authorities, the school authorities, parents, and the institutional ethical clearance committee. The screening was done utilizing natural daylight in compliance with infection prevention and control protocol. Clinical examination aimed at categorizing the observed occlusion into either ideal occlusion or one of the three classes of Angle’s class I, II, and III malocclusions. The Simplified Malocclusion Index For Layperson Evaluation (SMILE) was verbally assigned in the vernacular language while interacting with each child and the findings made note of for calculation of relevant scores related to their orthodontic awareness, self-esteem as related to self-perceived esthetics, and their self-perceived need for treatment. Reasons for reluctance to undergo treatment were noted down if expressed. An initial group of 31 adolescents categorized as presenting with clinical malocclusion were randomly picked up and assigned the SMILE index a second time to assess the reliability of the index by way of Cohen’s kappa statistic.
Results:
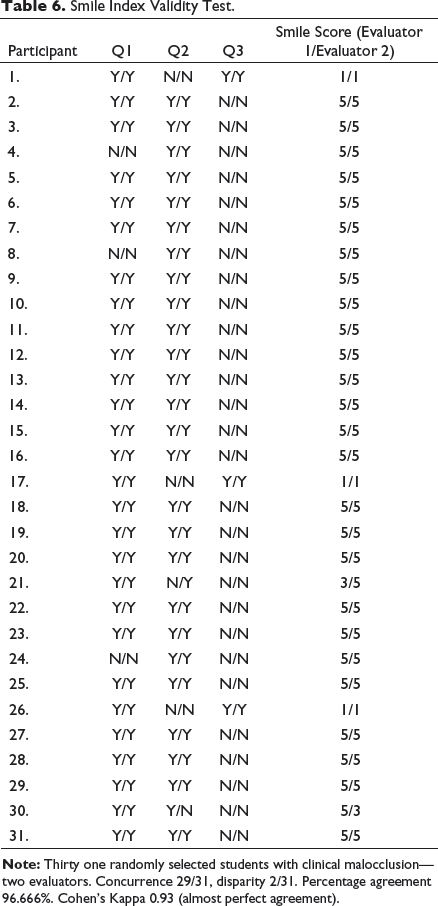
The initial test group of 31 individuals assigned the SMILE twice showed a Cohen’s kappa of 0.93 validating almost perfect intraoperator agreement. The SMILE index revealed that 80.95% of the adolescents of Paderu revenue division had orthodontic awareness and 79.51% had self-perceived esthetics but only 15.97% felt a need for orthodontic treatment. Pearson’s Chi squared statistical analysis indicated a gender bias related to the self-perceived need for orthodontic treatment (X 2 [1, N = 1,371] = 19.71, P < .001). The Index assigned to the Parvathipuram division revealed that 77.04% had orthodontic awareness and 78.38 had self-perceived esthetics but only 6.95% felt the need for orthodontic treatment. Pearson’s Chi squared statistical analysis indicated a gender bias related to the self-perceived need for orthodontic treatment (X 2 [1, N = 764] = 4.95, P = .02).
Conclusion:
The self-perceived need for orthodontic treatment is often based on the self-perceived esthetics of an individual or the self-esteem as influenced by the perceived esthetic norm of the community. Orthodontic treatment of adolescents with borderline malocclusion derangements requires careful ascertaining of the actual perceived need of the patient to enable the rendering of a justifiable orthodontic treatment with the complete trust of the young patient. This helps build community trust in regions where orthodontic treatment has not yet made in roads and may help ensure higher end of treatment satisfaction levels.
Background
The Merriam-Webster dictionary describes “normal” as “conforming to the standard or common type” characterized by that which is considered usual, typical. 1 The significance of this in determining the orthodontic treatment need of a group of individuals is the clinician’s appraisal based on certain clinical norms vs the patient’s self-appraised notion of what is considered normal, or what is referred to as the psychosomatic norm, based on the most prevalent dentofacial patterns which is the socially accepted norm.2, 3
The scheduled tribes of Southern India are thought to have originated from the Ancestral South Indians whose lineage can be traced back to both the Ancient Ancestral South Indians and the Indus Valley Civilization.4–8 The Scheduled Castes and Scheduled Tribes Orders (Amendment) Act (Central Government of India), 2002 recognizes 34 scheduled tribes in Andhra Pradesh of which 10 tribes are specific to the hilly regions or agency areas of Paderu and Parvathipuram revenue divisions. 9
The parameters indicated by the government in identifying the socially distinct and identifiable diverse endogamous tribal races often referred to as “jatis” include a culture that is identifiably distinct usually secluded on account of geographical isolation with a certain degree of backwardness or primitive traits in relation to neighboring urbanized cultures.9–11 Von Fürer-Haimendorf states that the preservation of these distinct cultures has not only been due to geographical isolation and ethnic displacement but also due to the natural Indian tolerance to cultural diversity rather than a missionary zeal to convert one and all to a single common faith.12, 13
As these tribes are strictly endogamous, with marriages occurring within the community, the processes of miscegenation and acculturation that form the basis of the genetic melting pot theory are missing and certain traits like the dentofacial clinical phenotype are well preserved along with the perception of what is considered normal.14, 15 As pointed out by researchers like Susanne, Cassidy, Mossey, Carels, Cakan, and Vieira, the genetically determined clinical phenotype is often subjected to environmental modifiers like nutrition and coarseness of diet.16–21 As early as 1841 Lefoulon put forward, amongst various etiological factors of malocclusion, the role of constitutional differences resulting from geographic or socioeconomic conditions. 22
Numerous studies on twins have tried to highlight the genetic significance of malocclusion as influenced by the environment and dietary influences in what has been referred to as “nature vs. nurture.”23–27 Researchers like Hunter, Begg, Proffit, Foster, and Corrucini have debated that malocclusion is often less prevalent in cultures where coarse diet forms a major part of the staple diet by way of attrition-related accommodation while researchers like Enlow and Solow stress on the role of various aspects of mandibular growth as an accommodative phenomenon.28–33 Rats and primates, fed with a soft diet, have an impaired musculoskeletal development of the jaws and associated crowding.34–36 Researchers have found less interproximal and occlusal wear in modern skulls as compared to medieval skulls.37–39
Shaw has suggested that the need for orthodontic treatment may be uncertain at times as based on proposed psychological or functional benefits. 40 The self-perceived deviation from a socially acceptable norm of visible dentofacial alignment has been documented as the prime cause for adolescents seeking orthodontic treatment and has also been documented as a factor negatively influencing the self-perceived oral health quality of life.41,42 Self-perceived satisfaction related to dentofacial appearance has been shown to be linked to both sex and age with young adults expressing more dissatisfaction as compared to adolescents and females being more particular about their dentofacial appearance and hence, their self-perceived need for orthodontic treatment.43-48 In a study by Philips et al., males expected orthodontic treatment to translate to better social interactions and interpersonal gains while females expressed a simple contentment over the improvement in appearance.49 Tung and Kiyak indicated that children and their parents most often express an expectation of a betterment of self-image and oral function when they opt for orthodontic treatment.50 This raises questions regarding the need of orthodontic treatment in borderline cases of malocclusion which invariably depend on the outcome of the interaction between the orthodontist and the patient’s parent or guardian.
Of additional significance is the informed consent obtained from both the adolescent and the parent or guardian in the light of research that shows that while the process of obtaining informed consent has become more organized, a true gauging of whether the patient or parent has understood all aspects of treatments is still questionable. 51 The main emphasis on a better patient understanding of the proposed treatment is in ensuring patient compliance that goes a long way in securing a positive end result. 52
Health-care systems require documentation of a need for orthodontic treatment and this need is most often evaluated by utilizing an index. Early examples of such indices include the method of occlusal assessment proposed by Massler and Frankel in the 1950s, Summer’s occlusal index, Grainger’s treatment priority index and Salzman’s handicapping malocclusion assessment record in the 1960s, Little’s irregularity index of the 1970s, the index of orthodontic treatment need proposed by Brook and Shaw in the 1980s and more recently the Oral Aesthetic Subjective Impact Scale proposed by Mandall in 2000.53–65 An interesting point to note is the eventual inclusion of patient inputs to indicate a need for treatment as these indices evolved. This almost contradicts the need for informed consent in the assumption that this would be the responsibility of the clinician on the one hand and the parent or guardian on the other.
The cross-section of tribal population chosen for the study was one in which there was unimpeded growth and development and hence, a higher prevalence of near-normal occlusion was anticipated with minor deviations from the clinical norms in those with clinically determined malocclusion. Although the population was aware of orthodontic treatment on account of dental awareness and screening camps, there was no facility for orthodontic treatment nearby making the chosen population ideal for evaluation of a genuine self-perceived desire for treatment.
Of relevance to this study was a verbally assigned simplified index, the “Simplified Malocclusion Index for Layperson Evaluation” (SMILE) proposed by the authors that was used to directly assess the self-perceived esthetics, orthodontic awareness, and self-perceived need for orthodontic treatment of the adolescent with no direct influence from either the clinician or the parent or guardian. The index was verbally assigned in a very casual manner during interaction, preferably in the native language of the adolescent, to elicit a true response with no coercion. The sample cross-section of tribal adolescents chosen comprised of 2 tribal populations with no access to orthodontic treatment, thus allowing for an unbiased opinion of self-perceived treatment needs.
Materials and Methods
The purpose of this study was to ascertain self-perceived orthodontic treatment needs of a population of adolescent tribals screened in the Paderu revenue division of Visakhapatnam district and the Parvathipuram revenue division of Vizianagaram district. This cross-sectional evaluation study was performed after obtaining consent from the parents and the institutional ethics committee (ANIDS/IEC/2019020).
Participants
A total of 2,016 school-going tribal adolescents of the Paderu revenue division and 819 tribal adolescents of the Parvathipuram revenue division, aged 13 to 19 years, who presented with normal growth and development, without any form of nutritional deficiency, stunted growth, or craniofacial anomalies, were screened for prevalence of malocclusion and verbally assigned the SMILE index. Children excluded were those presenting with missing teeth, rampant caries, or any form of mutilated malocclusion. Orthodontic diagnostic screening was performed in natural daylight with fresh disposable examination gloves and presterilized diagnostic instruments for every child to comply with infection prevention and control guidelines. The prevalence of orthodontic malocclusion was evaluated based on Angle’s classification and the findings were tabulated along with additional findings (Tables 1 and 2, Figures 1 and 2). While the examination was being performed, the children were asked questions related to the SMILE index in their vernacular (Telugu) to make them feel at ease.
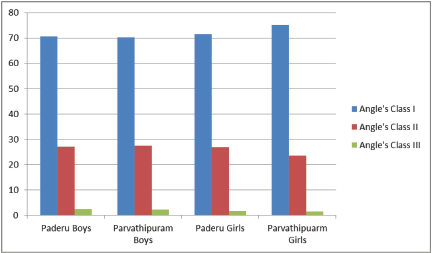
Gender-Based Prevalence of Malocclusion in Both Regions.
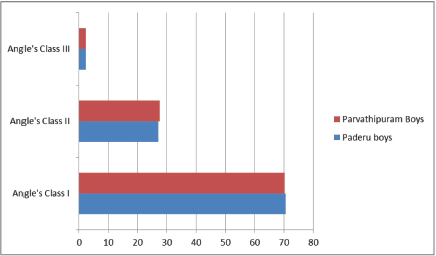
Prevalence of Malocclusion Amongst the Boys in Both Regions.
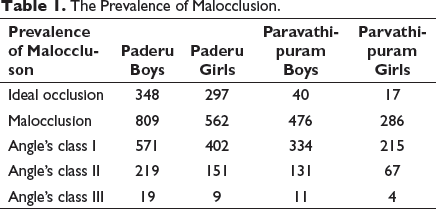
The Prevalence of Malocclusion.
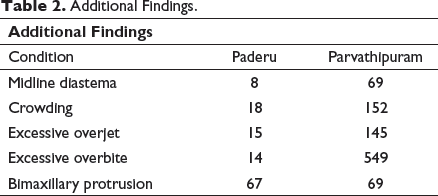
Additional Findings.
SMILE Index Data.

SMILE Index
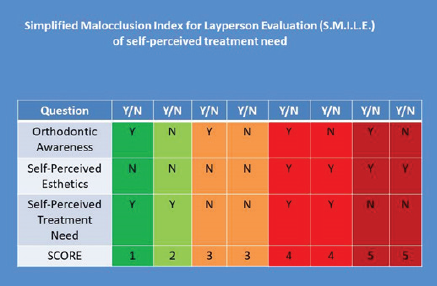
The index was designed to be verbally assigned with 3 very simple questions to be posed to the adolescent while interacting and examining the child. The questions, asked in the native language of the child, covered aspects of orthodontic awareness, self-perceived esthetics, and self-perceived need for orthodontic treatment. The scores were assigned in a Yes/No manner and cross-compared with the options grid later. The options grid comprises of all the 8 possible responses that the 3 questions can elicit (Table 4).
The Various Possible Responses That the Three Questions Can Elicit With Scores That Are to Be Assigned.
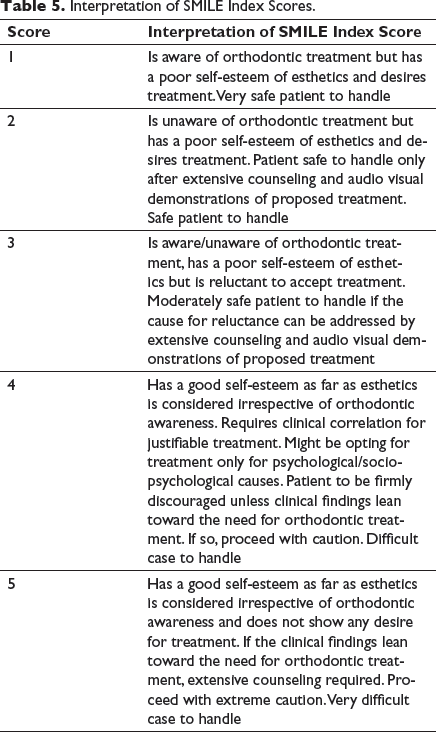
Interpretation of SMILE Index Scores.
The SMILE index was first subjected to a validation process by randomly selecting 31 adolescents with clinically documented malocclusion from the first group and subjecting them to the verbally assigned questions by a second operator (Table 6). This process resulted in a Cohen’s kappa of 0.93 validating almost perfect intraoperator agreement. The SMILE index was assigned to all remaining adolescents as well and the findings of the SMILE index and clinical examination were tabulated in Microsoft Excel 2010. These findings were then analyzed for percentage distribution (Figure 3). The causes for reluctance were also tabulated and analyzed for percentage distribution (Figure 4).
Prevalence of Malocclusion Amongst the Girls in Both Regions.
A Comparison of Other Findings.
Smile Index Validity Test.
Results
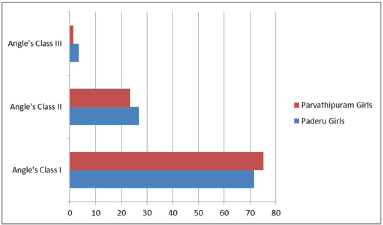
The predominant malocclusion in both regions was Angle’s class I with bimaxillary protrusion with no variation based on geographical location or gender. Of the adolescents screened at Paderu, 32% had normal occlusions. Of the 68% with malocclusion, 71% had Angle’s class I malocclusions, 27% had Angle’s class II malocclusions, and 2% had Angle’s class III malocclusions. The Chi Square statistical analysis for the Paderu revenue division indicated no gender bias related to the prevalence of malocclusion (X 2 [2, N = 2,016] = 5.5, P = .13).
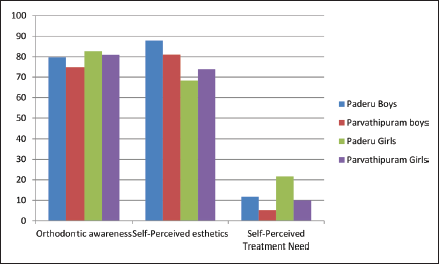
The verbally assigned SMILE revealed that 78.24% of the boys and 81.85% of the girls with malocclusion of Paderu revenue division had orthodontic awareness, 80.96% of the boys and 68.14% of the girls had self-perceived esthetics but only 12.11% of the boys and 20.99% of the girls felt a need for orthodontic treatment. The Chi square statistical analysis of the data obtained from the SMILE index indicated a gender bias (X 2 [1, N = 1,371] = 19.71, P < .001).
Of the adolescents screened at Parvathipuram, 7% had ideal occlusion and 93% (762) had malocclusion categorized as 72% with Angle’s class I, 26% with Angle’s class II, and 2% with Angle’s class III. The Chi Square statistical analysis for the Parvathipuram revenue division indicated no gender bias related to the prevalence of malocclusion (X 2 [2, N = 762] = 2.5, P = .28).
The index assigned to the adolescents with malocclusion at Parvathipuram division revealed that 73.52% of the boys and 79.72% of the girls had orthodontic awareness, 81.09% of the boys and 72.72% of the girls had self-perceived esthetics but only 5.25% of the boys and 9.79% of the girls felt the need for orthodontic treatment. The Chi square statistical analysis of the data obtained from the SMILE index indicated a gender bias (X 2 [1, N = 764] = 4.95, P = .025). The gender-based distribution of SMILE Index responses of both regions are depicted in Figure 5.
Discussion
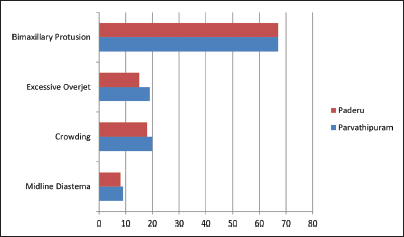
The tribal populations of Andhra Pradesh largely rely on food that is cultivated and meat from livestock or animals that are hunted66-68. As this diet is predominantly coarse, one might expect such a diet coupled with unimpeded musculoskeletal growth in the absence of detrimental habits as a basis for the clinically ascertained distinct phenotype seen in the tribal adolescents of both revenue divisions with a predominantly normal or Angle’s class I type malocclusion accompanied with bimaxillary protusion.69–73
Regular dental camps and general screening at the public health centers in both tribal regions along with the awareness created in the schools has helped establish a good level of awareness of what dentistry can offer as remedial and preventive care including orthodontic treatment. The perception of dentofacial esthetics in closed communities is largely influenced by the prevailing majority and this psychosocial influence on perceiving what is normal has been referred to as the psychosomatic norm by Abdel Kader and may often play a vital role in case selection or post-treatment patient satisfaction. 2 The results of the SMILE index highlight a good level of orthodontic awareness but a relatively low level of a self-perceived need for treatment which is most probably influenced by what is perceived to be normal amongst the community. Bleidorn et al., have indicated a slightly lower self-esteem amongst adolescent girls and this may in fact be related to a heightened awareness of esthetic parameters amongst the girls as compared to the boys. 74 Numerous studies have attempted to evaluate the perception of esthetics by adolescents including a cultural basis and also by laypersons as compared with a clinician trained to notice certain parameters.75–79 Delcides Ferreria Paula et al., in their study highlighted the role of the display of anterior teeth as an esthetic parameter of self-esteem. 79 Geld et al., have stressed on the importance of self-perception in relation to smile esthetics as a basis to smile attractiveness. 80 The self-perceived need for orthodontic treatment is often based on a complex interplay of the initial motivational factors along with the negative and positive influences of influencing factors that could include direct experiences or information gathered from peers undergoing orthodontic treatment. For example, as most individuals screened had bimaxillary protrusion, it wouldn’t be considered unsightly or abnormal by the community. Diastemas were rare but were considered by most tribal adolescents as a sign of good luck and prosperity. Adolescence is usually the period of mental maturation with the strengthening of certain set patterns of likes, dislikes, and beliefs based on cultural norms and such patterns may vary based on gender and age.74, 76, 79, 80
Of extreme importance, especially in dealing with a community where orthodontic treatment is yet to make in roads, is to be able to very clearly elicit patient preferences related to treatment to avoid treatments sought just to satisfy psychological or sociopsychological needs rather than true somatic needs. 81 Extensive studies have been performed to assess the self-perceived oral health status and self-perceived esthetics as related to the prevalence of malocclusion but these studies rely on the clinical interpretation of the investigator with no simple way of eliciting a young adolescent’s response, thus not truly eliciting informed consent from the adolescent with the main involvement of only the clinician and a parent or guardian.50, 82–92
The World Health Organization indicates the need for any index to be simple, reliable, reproducible, and accurate enough to cater to the screening of large groups of individuals. 93
The verbally assigned SMILE index proposed by the authors allows the child to feel at ease and allows for spontaneous and truthful answers to be elicited without the coercion or pressure a young adolescent would feel if asked to fill up a printed questionnaire. The SMILE index has a grid of 8 possible combinations of responses, 4 of which are indicative of a self-perceived need for treatment. Of significance are only 2 results (Table 3), both in which the child feels he or she does not have an esthetic smile and therefore desires orthodontic treatment. The only difference is in whether the child possesses an awareness of orthodontic treatment or not thus making the task a bit more difficult if the child has no prior idea as to what orthodontic treatment entails. The purpose of the proposed index is in being able to elicit a truthful need for treatment as perceived by a young adolescent who is not afflicted by any form of handicapping malocclusion but who might desire orthodontic correction from an esthetic standpoint.
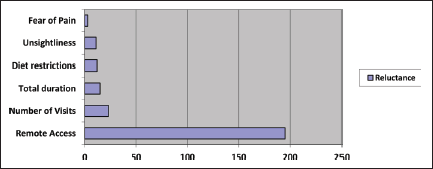
The limitation of the index might stem from reluctance as an overpowering factor. In spite of a perceived need for treatment, there are numerous factors that might influence a reluctance to pursue orthodontic treatment (Figure 6). General factors like easy access to orthodontic treatment and the general community acceptance of orthodontic treatment as a modality to improve the esthetic alignment of teeth may in fact play a far more important role than some of the personally perceived problems cited in literature like fear of pain or discomfort on account of the treatment.94–96 Tribal populations in India usually inhabit locations that are remote from urbanized locations and this negatively impacts the access to certain facilities commonly accessible amongst urbanized populations like orthodontic treatment and also influences the acceptance of the same. This study highlights the reasons specified by the tribal adolescents behind reluctance to pursue orthodontic treatment amongst 2 tribal populations in Andhra Pradesh as a guideline for implementation of health-care schemes in such remote access areas.
Gender-Based Distribution of SMILE Index Responses.
Weightage of the Reasons for Reluctance to Undergo Orthodontic Treatment.
Conclusion
Perceptions of esthetics are largely based on cultural norms and these may influence the perceived success or failure of orthodontic treatment rendered for esthetic corrections. The perception of esthetics and the outcome of proposed orthodontic treatment may differ from the viewpoint of the patient, the parent, and the dentist. It is therefore of paramount importance to elicit responses from the young patient in addition to requests for treatment that may be posed by the parent or guardian with subsequent inputs given by the orthodontist as to the feasibility of requested corrections and proposed treatment outcome. A simplified index is proposed as an easy to use, verbally assigned index that elicits an honest response related to the self-perceived need for orthodontic treatment in the light of orthodontic awareness and self-perceived esthetics allowing the clinician to make a balanced judgment especially in remote areas where orthodontic treatment is yet to be made readily accessible to one and all. This is of paramount importance especially when dealing with the correction of what may be referred to as borderline cases wherein there is no handicapping occlusion and the outcome is aimed more at improving esthetics and masticatory efficiency. It is in such situations that documentation of the clinician’s opinion alongside the expressed self-perceptions of the adolescent along with inputs of a parent or guardian go a long way in establishing the trust that orthodontics requires in a community.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.