
Abstract
Background
An analysis of the factors influencing the decision-making process in accepting orthodontic treatment can be of profound importance in establishing trust and ensuring an overall positive outcome. This is all the more significant when dealing with a patient who has not had any prior interaction with an orthodontist. The Simplified Malocclusion Index for Layperson Evaluation (SMILE Index) allows an unbiased cross-evaluation between the perceived need for treatment and the factors of orthodontic awareness and self-perceived esthetics.
Objectives
Tribal adolescents belonging to 2 regions with no prior access to orthodontic treatment were chosen for the study. Most adolescents of this region were assumed to have orthodontic awareness by way of information from their schools and dental camps. During the orthodontic screening process, a verbally assigned questionnaire base index was used to elicit their willingness to undergo treatment and to understand influencing factors.
Methods
A total of 2,835 tribal adolescents between the ages of 13 and 19 years belonging to the Revenue divisions of Paderu (Visakhapatnam) and Parvathipuram (Vizianagaram) were screened in this study. Chosen candidates presented with normal growth and development, and had no nutritional deficiencies or metabolic disorders. Consent and permissions were obtained from the regional tribal authorities, institutional ethical clearance committee, the school authorities, and the parents or guardians of the adolescents. The orthodontic screening was performed under natural daylight with strict adherence to infection prevention protocol. Observed occlusions were categorized into either an ideal occlusion or Angle’s Class I, II, and III malocclusions. During the screening, the SMILE index was assigned in the vernacular Telugu. A percentage distribution analysis was made of the responses of those presenting with malocclusion.
Results
An analysis of the SMILE index results of the adolescents of Paderu Revenue division revealed higher SMILE index scores in categories III and V with a percentage distribution of 24.46% for males and 26.86% for females in SMILE Index Score Category III and 63.40% for the males and 52.13% for the females in Category V. Similarly, the results of Parvathipuram division had a higher score distribution in the categories of III and V with a percentage distribution of 16.07% for males and 15.84% for females in category III and 78.67% for males and 74.25% for females in category V.
Conclusion
Orthodontic treatment with proper counseling providing clarity of facts facilitates an easier decision-making process and enables both the patient and the orthodontist to understand one another and the treatment process better for a much more predictable overall treatment outcome.
Introduction
Hicks and Kluemper 1 have indicated that decision-making may be the result of systematic analysis of a situation which may include certain preferences related to the understanding termed as a cognitive bias or it may be entirely based on a heuristic process. The American Academy of Pediatric Dentistry stresses on issues centered around the informed consent which is particularly important when dealing with an adolescent. 2 Ackerman and Profit 3 have stressed that to avoid decision-making that might be ambiguous and without a foundation of clarity especially when an adolescent is deciding upon orthodontic treatment, it is of paramount importance to make the decision-making process a shared decision-making process with equal inputs from the patient and the clinician. As there is the possibility of overshadowing of opinion of the adolescent by family members or the accompanying guardian, it is also important to elicit an unbiased and candid opinion from the patient.4, 5 Researchers have indicated that female adolescents seem to be more aware of disturbances in dentofacial appearance and most adolescents look for orthodontic treatment seeking an improvement in confidence levels and overall psychosocial well-being and quality of life.6–10
Researchers have also indicated that there is a lot of well-intentioned parental influence or bias in the decision-making process that may not allow the adolescent to express their candid opinions which might help the orthodontist understand how to counsel them better.11–13 The physician plays an important role in ensuring a degree of decision autonomy in view of the paternal influence. 14 Abdel Kader 15 has pointed the significance of the influence of the community on the child or parent’s decision-making by way of what has been referred to as the psychosomatic norm. Literature has documented discrepancies between the subjective evaluation of the patient related to perceived esthetic or functional insufficiency versus the clinical judgement of the orthodontists in proposing a need for the treatment.16–19
Most orthodontic treatment need indices focus on clinically ascertained aspects and not on the perceived treatment need of the patient and thereby do not directly focus on the psychosocial well-being of the patient.20–32 The purpose of this study is to highlight the possibility of eliciting a candid response related to the decision-making process from the adolescent himself or herself using an index that elicits data by way of verbally assigned questions during the screening process, without the influence parental decision choices. 33
Materials and Methods
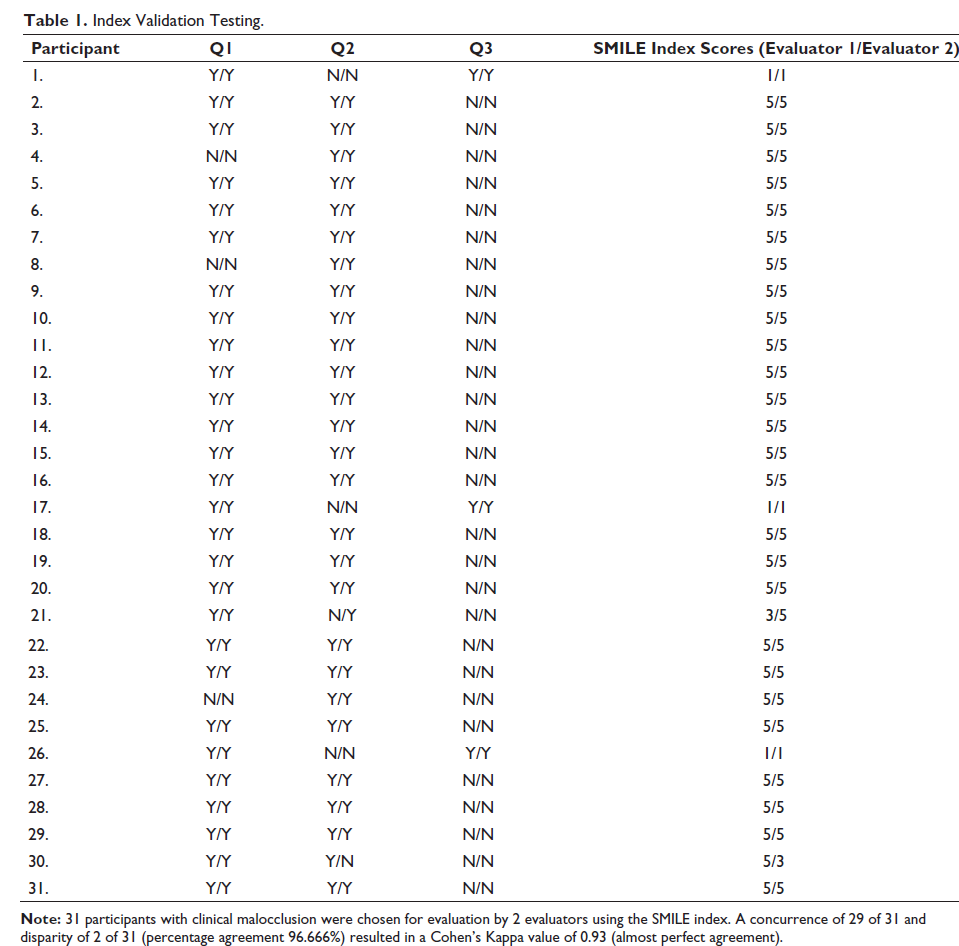
The study was designed as a prospective study. A total of 2,835 tribal adolescents of the Parvathipuram and Paderu revenue division aged 13 to 19 years presenting with normal growth and development, no form of nutritional deficiency, stunted growth, or craniofacial anomalies were screened and assigned the Simplified Malocclusion Index for Layperson Evaluation (SMILE) index (Table 1) in their vernacular verbally. Children presenting with missing teeth, rampant caries, or mutilated malocclusion were excluded. Required consents were obtained from parents, the school authorities, the tribal authorities, and the institutional ethical clearance committee (ANIDS/IEC/2019020). The clinical screening process was performed in natural daylight observing standard infection and cross-contamination prevention and control protocols. The observed occlusions were categorized into ideal occlusion or malocclusion based on Angle’s classification. The SMILE-Index was put forth in the vernacular language Telugu during the interaction with each adolescent to elicit an unbiased YES/NO response regarding esthetics self-esteem related to their dentition, awareness regarding orthodontic treatment, and their own self-perceived need for orthodontic treatment. Responses were recorded as per the SMILE Index scoring system and these findings were tabulated and analyzed for percentage distribution. Thirty-one randomly selected students with clinical malocclusion were evaluated by 2 evaluators and subjected to a Cohen’s Kappa analysis for validation of the SMILE Index.
Index Validation Testing.
Results
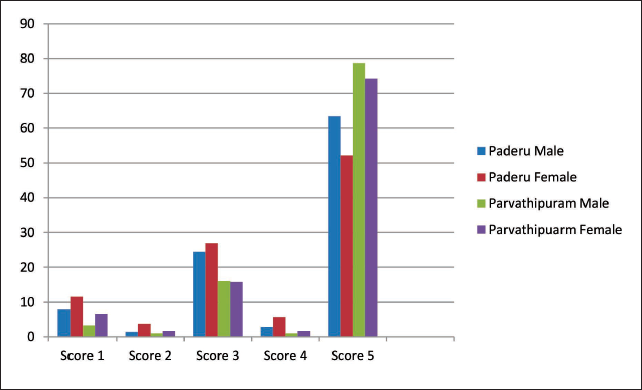
The SMILE Index data was tabulated and a percentage distribution evaluation was performed for adolescents presenting with clinically ascertained malocclusion in the 2 regions analyzed (Figure 1). The Cohen’s Kappa analysis showed a concurrence of 29 of the 31 chosen with a disparity of 2 of 31 with a result of 0.93 indicating almost perfect agreement (Table 2).
The Percentage Distribution of SMILE Index Scores Between the Two Tribal Communities.
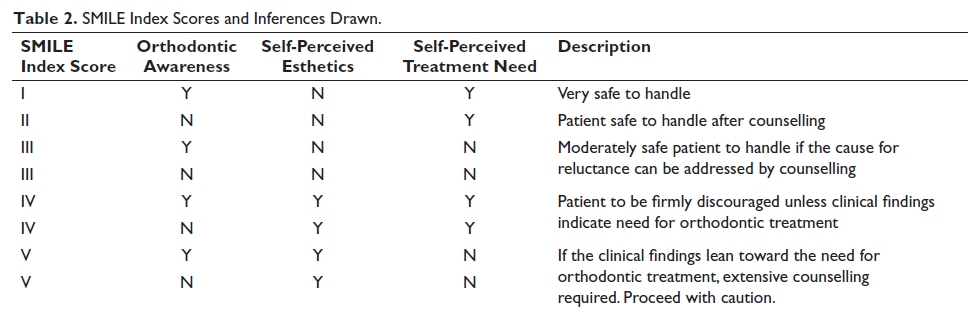
SMILE Index Scores and Inferences Drawn.
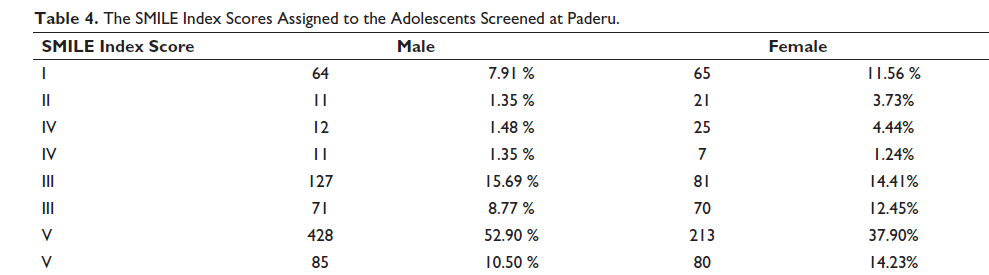
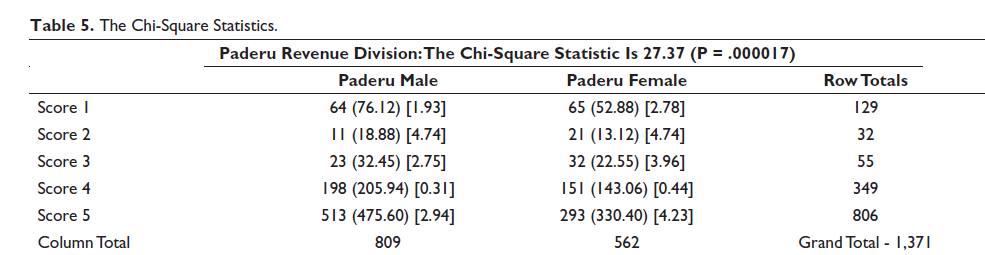
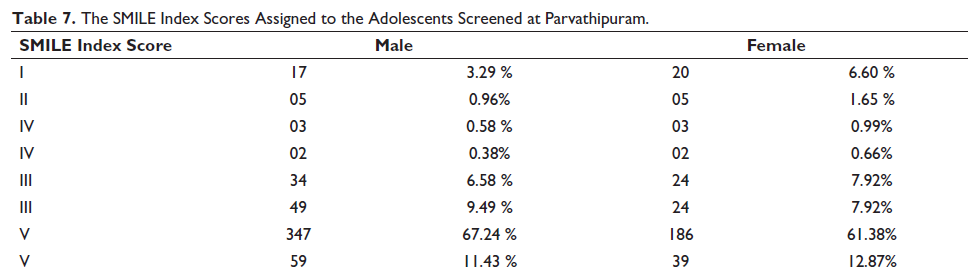
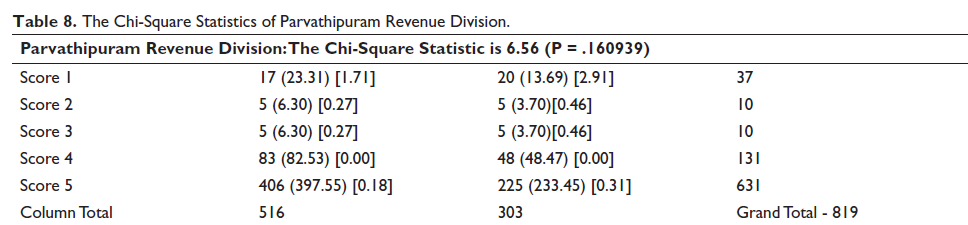
The analysis of the data of the Paderu Revenue division (Tables 3 and 4) revealed higher SMILE index scores in categories III (24.46% males and 26.86% females) and V (63.40% males and 52.13% females). A chi-square analysis (Table 5) revealed that the gender bias was of statistical significance with a value of 27.37 (P value = .000017). Similarly, the results of Parvathipuram division (Tables 6 and 7) had a higher SMILE Index score distribution in the categories of I (16.07% males and 15.84% females) and V (78.67 males and 74.25% females). These results indicated an overall higher reluctance toward treatment as expressed by the adolescents. Although there seemed to be a gender bias, a chi-square analysis (Table 8) revealed a lack of statistical significance with a value of 6.56 (P = .160).
Adolescents From the Revenue Division of Paderu Identified With Malocclusion.

The SMILE Index Scores Assigned to the Adolescents Screened at Paderu.
The Chi-Square Statistics.
Adolescents From the Revenue Division of Parvathipuram Identified With Malocclusion.

The SMILE Index Scores Assigned to the Adolescents Screened at Parvathipuram.
The Chi-Square Statistics of Parvathipuram Revenue Division.
Discussion
As Chen and Das 14 have pointed out, most orthodontic patients are adolescents and minors, there is limited scope for autonomous decision-making with more emphasis on the paternal decision-making or influencing process. Ann McNary 34 has summarized the current trend in obtaining informed consent highlighting cases in which a minor may be allowed to give consent for himself or herself. Based on this, it is of importance to also elicit the child’s unbiased opinion with regard to self-perceived treatment need as this will help decide the dynamics of the subsequent clinician-patient-parent interaction. Malocclusion has been documented as a major influencer in self-perceived esthetics as documented by Badran et al.35–37 Numerous reasons may influence this decision-making process as they directly or indirectly affect the perceived need for treatment and willingness for the same. Esthetics is by far and large the most powerful motivating factor just as pain or economic considerations became the discouraging factors.38–46
The SMILE index helps distinguish between the subjective need and normative need emphasizing on the influences of orthodontic awareness and self-perceived esthetics. The index is designed to convert patient-based responses to a series of scores based on the level of orthodontic awareness, self-perceived esthetics as a decision influencer, and finally the self-perceived need for treatment which may be positively or negatively influenced by a multitude of factors. To avoid operator bias, the responses to these 3 queries posed during the clinical examination result in a score specific to the 3 responses as shown in Table 1. The index scores of 3 and 5 indicate an overall final reluctance toward treatment and scores 1, 2, and 4 indicate a final willingness and perceived need for treatment. The only variables were those of orthodontic awareness and self-perceived esthetics. The scores for 1, 2, and 4 presented with a gender bias probably indicating that the female adolescents were more discerning about their appearance as compared to their male counterparts as has been documented in the literature. While orthodontic awareness could be a factor worth considering, it was not considered to be statistically significant as the regions had no history of prior orthodontic treatment and hence the awareness was not the one influenced by direct interaction with a peer. Of more importance was the self-perceived esthetics. On one hand, there were respondents who felt a need for treatment on account of esthetic insufficiency and such candidates were probably the most appropriate for orthodontic treatment as is commonly commented upon in literature.47, 48 On the other hand were the respondents who indicated an interest in treatment in spite of a high esthetic self-esteem. The final responses chosen for analysis comprised both of candidates with poor esthetic self-esteem in what could be perceived as a genuine need for treatment and also candidates with high enough esthetic self-esteem for whom treatment could probably be considered only necessary if the clinical judgment indicated a normative need for orthodontic correction based on a minor degree of malocclusion that could be corrected yielding improvement upon the existing scenario.
Summary and Conclusion
This study aims to highlight the successful use of a verbally assigned index to obtain a candid unbiased opinion from adolescents related to their decision of self-perceived need for orthodontic treatment. The index prevents operator bias by way of a scoring system that also helps highlight if there is a genuine need or orthodontic correction. Similarly, the index helps lay an emphasis on situations where a child may be reluctant to undergo treatment in spite of the psychosocial consequences of malocclusion and can be counseled accordingly based on the normative need.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was given by the Institutional Ethical Committee of our institution (ANIDS/IEC/2019020).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
This is a questionnaire-based study on tribal population. So no patient consent is required.