
Abstract
Background and Objectives:
The use of mini-implants has become more popular, and there has been a heightened focus on factors that contribute to their success. The purpose of the study is to compare the effects of various surface treatment methods of mini-implants on their bone cutting capacity, insertion torque required, and fracture resistance when compared with the untreated machined mini-implants.
Materials and Methods:
The study included 4 groups. Each group consisted of 10 orthodontic mini-implants (OMIs). The first experimental group contains titanium oxide coated mini-implants, the second group contains grit-blasted implants with aluminum oxide, the third group consists of mini-implants coated with hydroxyapatite crystals, and the control group is formed by untreated machined mini-implants. Each group is evaluated for cutting efficiency, maximum insertion torque, and fracture resistance using a customized torque testing gauge.
Results:
The results showed that surface treating OMIs with hydroxyapatite particles increases the surface roughness, thereby enhancing their stability without decreasing the bone cutting ability compared with OMIs without surface treatment.
Conclusion:
Roughened surface of OMIs with hydroxyapatite particles exhibited maximum fracture resistance without decreased corresponding bone cutting efficiency.
Introduction
As stated by Newton’s third law, every action has an equal and opposite reaction; likewise, reciprocal forces of the same magnitude but opposite in direction are generated on teeth during orthodontic treatment when subjected to forces and moments. This is especially pertinent where the action is the favorable tooth movement and reaction is unwanted tooth movement. To avoid these unwanted tooth movements, the reciprocal forces must be redirected, which can be achieved by reinforcing an orthodontic anchorage. 1
Miniscrews give orthodontists superior control over tooth movement in all 3 dimensions and enable them to provide the best treatment result as well. However, a few unsuccessful cases have also been reported. Fracture of the OMI, early loosening, inflammation, and root damage are considered as the cause of failure. Among these, loosening in the early treatment stage is considered to be clinically important. 2
Surface treatments of OMIs induce osteointegration and improve stability with a low risk of fractures. The available surface treatment methods for dental implants include acid etching, grit blasting, anodization, coating with calcium phosphate, and titanium plasma spraying, which are noted to have better osseointegration than the machined surfaces, which are nonsurface-treated. 3
The studies on nonsurface-treated titanium alloy dental implants are extensive; however, biomechanical properties of the surface-treated titanium alloy OMIs are yet to be explored. Furthermore, the pattern of insertion of the self-drilling OMIs might be altered because of the change in the bone cutting capacity of the surface-treated OMIs. This needs additional evaluation to determine the clinical significance.
Materials and Methods
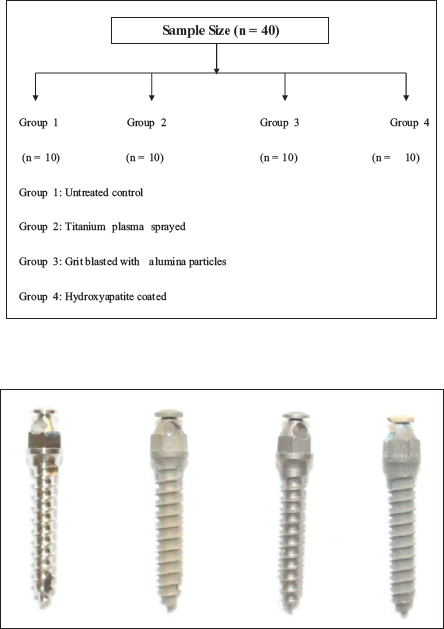
Forty OMIs of size 1.4 mm × 8 mm were used for this study. The study includes 4 groups, of which one is the control group and 3 are experimental groups. Each group consists of 10 OMIs. One experimental group contains titanium oxide coated mini-implants, second group contains grit-blasted implants with the aluminum oxide, the third group consists of the mini-implants coated with hydroxyapatite crystals, and the control group is formed by the untreated machined mini-implants (Figure 1).
1.4 mm × 8 mm Dentos Inc. Orthodontics Microimplants, Drill-Free Type with a Tapered Design.
The bone tissue used in the study was obtained from the pig, as the osseous characteristics are similar to that of the human bone. 4 The pig bone was obtained from the butcher’s shop, and the overlying soft tissues were thoroughly cleaned and stored in physiological saline while transporting. 5 The cortical bone thickness of each of the block was measured using a digital vernier caliper on both ends, which was found to be approximately 2 mm.
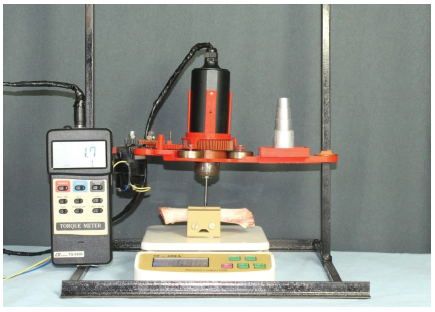
For torque testing, a digital torque meter was attached to a custom fabricated setup to hold the bone block and allow the implant to be placed over the bone surface perpendicularly (Figure 2). The implant driver shaft was attached to the torque meter. 1 kg initial load was applied by the rotational axis of the torque tester to place micro-implants. This load was calibrated by a load cell to check the initial load applied before starting the procedure.
Custom Fabricated Setup to Hold the Bone Block and Allow the Implant to be Placed Perpendicular to the Bone Surface.
Each mini-implant was placed into the cortical bone perpendicularly into blocks that are located in the central portion of the pig bone. Tests on insertion of the mini-implant were carried out without performing any preliminary drilling, using the mini-implant driver shaft coupled to the switch, fitted to a hand piece with reduced speed.
During the insertion, the torque meter rotated at a constant speed of one rotation per minute (RPM) as per the guidelines of American Society for Testing and Materials (ASTM) F543-02 for the precise monitoring of the changes in torque. The maximum insertion torque (MIT) was noted up to the cortical bone penetration.
Contrastive to the self-tapping OMIs, the self-drilling OMIs can penetrate the bone during the insertion process utilizing their cutting edges. Total insertion time to place the OMI determines its bone cutting ability. The bone was sectioned into blocks of approximately 6 cm length and embedded into acrylic blocks for shape standardization and to stabilize the bone in the universal testing machine (Figure 3).
Bone Embedded in Acrylic to Stabilize in the Universal Testing Machine (to Check Fracture Resistance).

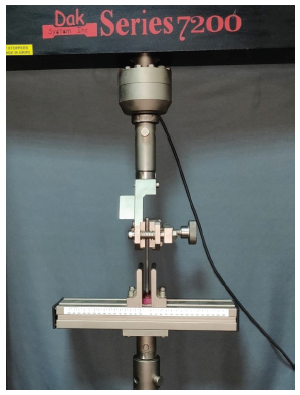
Universal testing machine “Dak System Inc (Model no: T-72502)” was used to test specimens and fixed parallel to the ground and perpendicular to the applied force. The testing machine was connected to model software in the compression test mode with a 50 KN load cell at a speed of 5 mm/min. A chisel-shaped active tip was used to determine the force applied on the mini-implant (Figure 4).
Universal Testing Machine “Dak System Inc (Model no: T-72502).”
All the values thus obtained were subjected to statistical analysis, and the following results were drawn.
Results
The data were tabulated and analyzed using the SPSS (Statistical Product and Service Solutions) Version 23. Chicago: Illinois (USA). Descriptive statistics, one-way analysis of variance (ANOVA), and post hoc Tukey test were carried out.
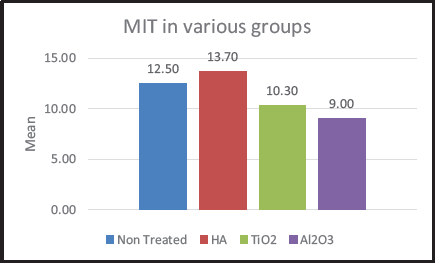
Aluminum oxide-coated particles showed the least insertion torque followed by titanium dioxide-treated OMIs, while nontreated machined implants showed a mean insertion torque of 12.5 Ncm. Insertion torque was the highest in hydroxyapatite-coated implants (Figure 5).
Overall Intergroup Comparison of Maximum Insertion Torque (MIT) (One Way ANOVA).
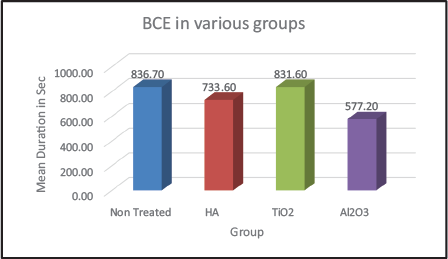
Aluminum oxide-coated particles showed the maximum bone cutting efficiency (BCE), followed by hydroxyapatite-coated implants. While titanium dioxide-treated mini-implants showed a BCE of 831.6, followed by nontreated machined implants (Figure 6).
Overall Comparison of Bone Cutting Efficiency (BCE).
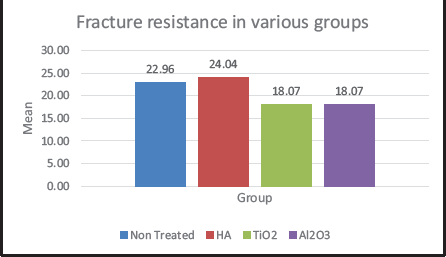
Hydroxyapatite-coated implants showed maximum resistance to fracture, while titanium oxide and aluminum oxide-treated implants showed decreased fracture resistance compared to the nontreated machined orthodontic mini-implants (Figure 7).
Fracture Resistance in Various Groups.
Discussion
Cortical anchorage system, in recent years, has become a cardinal segment of orthodontic treatment. Temporary anchorage devices comprise a category of adjunctive devices that have the potential for “absolute anchorage,” also known as a skeletal anchorage, that has come into existence following Branemark’s discovery during a study done to inspect the blood flow in the rabbit bone using a titanium implant chamber. 6 Bone integration with the implant was noted such that they could not be separated when the titanium chambers were removed. Hence, he coined the term “osseointegration.”
Reduced reliance on patient compliance, preventing unwanted tooth movements with opening horizons to movements in teeth which were unattainable previously have expanded possibilities for various treatments modalities using mini-implants.7, 8
Mini-implants depend on the mechanical retention along with the implant and the thread–bone interface. The primary stability is considered as a prime mover in the success of the mini-implant retention.9, 10 Immediate loading of the implant is possible because of the mechanical interlock with the bone, eliminating the waiting period needed for osteointegration. Once the implant is stabilized in bone, the polished implant surface prevents fusion of bone to the implant. 11
Early loosening of the implant, soft-tissue impingement, and irritation aphthous ulcers are commonly reported complications along with tooth sensitivity, infection-causing swelling and pain around the implant site (peri-implantitis), fracture during placement or removal, and root damage. Of these, early loosening is crucial in the early stages of treatment. 12
Although titanium and its alloys are ideal biomaterials, adequate results are not always guaranteed by their use. OMIs are sometimes unpredictable because of incomplete osseointegration, thus increasing the risk of losing the applied medical device. Therefore, additional investigations have to be done to improve host cell-mini-implant interaction to enhance the osseointegration process. 13
Accordingly, different modifications to OMI designs were carried out to improve their stability. For space reduction between bone and implant, a conical shape was given. 14 In an attempt to enhance stability with improved osseointegration with the added benefit of a reduced fracture potential, self-tapping OMIs with surface treatments are proven to be better.
Surface roughness determines the fixation biomechanically and osteointegration of titanium implants. Based on the level of features, surface roughness is classified into macro, micro, and nano-sized topologies. The available surface treatments for the dental implants include grit blasting, titanium plasma spraying, anodization, coating calcium phosphate, and acid etching. These procedures give added advantage of osseointegration over nonsurface-treated machined surfaces. 3
The implants chosen for this study were Ti6Al4V, 1.4 × 8 mm, and tapered design drill-free type of implants. Removal torque value is directly proportional to the square of implant diameter, so for better stability under rotational moments, microimplants of 1.4 mm diameter were used.
The microimplant length of 8 mm was used because it is usually sufficient to achieve adequate primary stability. The implant driver shaft provided by the manufacturer was attached to the custom-fabricated jig to insert implant perpendicular to the bone surface.
In this study, the MIT and BCE were evaluated using pig ribs. Pig ribs were chosen for this study because of their similarities to human skeleton and previous employment as models for experiments in skeletal research. The lamellar structure and remodeling rate of pig osseous tissue are strikingly similar to that of human osseous tissue.
Survival of the OMIs predominantly depends on sufficient primary stability, which means that suitable and enough torque is needed during insertion. If the moments exceed fracture resistance of the mini-implant, it may result in its fracture, and maximum torque load capacity should be noted for clinical significance. 9
MIT in this study was evaluated by insertion torque measurement. The rotational force required during miniscrew implant insertion into bone is known as insertion torque and is reported in most literature as Newton cm. 15
In the current study, MIT (ie, the primary stability) values among all the 4 groups in the ascending order were as follows. Mini-implants coated with hydroxyapatite crystals exhibited MIT (ie, 13.70 ± 0.82 Ncm), followed by the control group, which was formed by untreated machined mini-implants (12.50 ± 0.7 1 Ncm). Whereas titanium oxide-coated mini-implants showed MIT of (10.30 ± 0.82 Ncm), and the least primary stability was recorded in the group of grit-blasted mini-implants with aluminum particles (9.00 ± 0.94 Ncm).
In the self-drilling method, bone cutting capacity is an important factor because it is required for the insertion. The cutting region may be altered by surface treatment, thereby affecting bone cutting ability and increasing retention. The time elapsed till complete insertion (6 mm) of the cutting blades was used by Jang et al 16 in their study to compare bone cutting efficacy. They concluded that it took a longer time with acid etching. Acid etching results in the formation of microscale porous structures on cutting blade surfaces which attribute to the difference noted. Similar results were found in the present study with surface-treated OMIs.
To determine the BCE in the present study, the total insertion time to place a mini-implant into the artificial bone was measured. To simplify it, less the time (in seconds) taken for the implant to penetrate into the bone, more was its BCE. According to the time recorded, the following results were obtained.
Maximum BCE was exhibited by the grit blasted mini-implants with aluminum oxide particles (577.20 ± 21.61 s) followed by hydroxyapatite-coated particles (733.60 ± 20.01 s), and then titanium oxide coated particles (831 ± 21.18 s) followed by nontreated machined implants (836.70 ± 18.84 s).
Another parameter evaluated in this study was fracture resistance. Fracture of mini-implants results if torque values are high during insertion or removal. 17 Decreased implant diameter and increased cortical bone thickness exhibit increased risk of fracture of mini-implants.
The maximum fracture resistance was measured by subjecting the mini-implants to a compression test in the universal testing machine. The fracture torque values in this study ranged from 18.07 Ncm to 24.04 Ncm.
Maximum fracture resistance was shown by the group of mini-implants coated with hydroxyapatite particles, ie, (24.04 Ncm), which showed sufficient primary stability. Stability of miniscrew implants is directly proportional to their stability; the more stable a miniscrew implant, the greater load resistance it possesses and could be subjected to early loading or function.
The fracture resistance in the noncoated machined mini-implants was found to be 22.96 Ncm which was slightly decreased when compared to the fracture resistance value provided by the manufacturer, ie, 25 Ncm. The least fracture resistance was found in the group of implants surface treated with titanium oxide particles and aluminum oxide particles, ie, 18.07 Ncm.
Electropolished titanium implants with Hydroxyapatite (HA) nanoparticle deposits improved bone-to-implant contact (BIC) and removal torque, attributed to HA nanoparticles. 18 Experimental groups with hydroxyapatite coating displayed the best stability without any reduction in bone cutting capacity.
When a mini-implant hits a root during placement, its fracture vulnerability increases because of an exponential increase in insertion torque. 19 Because interradicular sites are common mini-implant placement sites, the risk of damage to Periodontal Ligament (PDL) and roots during removal is quite common. The knowledge of the maximum torque capacity of the mini-implant during insertion is vital to scale back the possible risks related to this clinical procedure.
Understanding and evading the maximum torque capacity of the mini-implant during insertion is crucial in bringing down the risks related to the mini-implant fracture and decreasing the apprehension felt by the patient and orthodontist. 15 In animal experiments, comparing surface-treated mini-implants and machined mini-implants, a higher mean removal torque value and new bone formation around the surface were noted with Sandblasted and Acid-etched (SLA) implants.
The orthodontist can count on the benefit of rotational stability of the surface-treated mini-implant, as long as the removal is not difficult. The degree of osseointegration is very important. 20 Partial osseointegration represents a definite advantage in orthodontic applications because rotational stability supports lever arm mechanics, but the implant remains easy to remove.
Primary stability depends not only on the torque of insertion but also on the quality of bone. Osteointegration of implants and primary stability depend on the insertion torque; nevertheless, above 35 Ncm of insertion torque, there seems to be no correlation between insertion torque and implant failure. 20
Biomechanical stability of OMIs and histological changes in bony tissues around OMIs with diverse force application conditions require additional studies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.