
Abstract
Orthodontic treatment has become a common practice in recent times. With today’s patients turning toward high-profile needs, it is apparent that they receive orthodontic treatment with the same consideration given to the esthetic needs of these patients. With these, an orthodontist usually turns to contemporary orthodontics and recent advancements to achieve this result, such as mini-implants. However, the correct placement of these mini-implants is vital to the result. The correct position not only aids in the treatment but also helps in the compliance of the patient. Such a procedure is ST-ENT for the placement of mini-implants.
Introduction
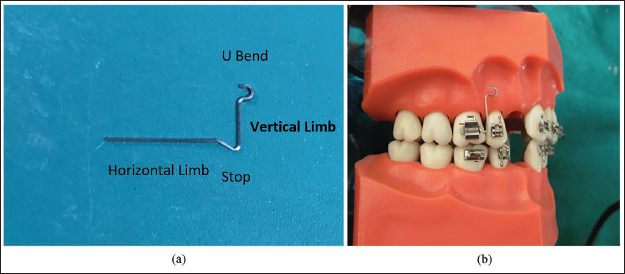
Implants are auxiliaries and aid in the treatment during orthodontic therapy. They are reinforcements in anchorage control. They gain retention by the interlocking of their threads into the bone, providing retention and stability to the implant. So, the precise positioning of a mini-implant is of prime importance for its stability. 1 Proximity to the root surface, placement in the alveolar mucosa, and unsuitable angulations impute to its failure. The disposition of a mini-screw in close proximity to the root surface often results in inadequate bone remodeling around the screw, and the transmission of occlusal forces through the teeth to the screw leads to implant failure. 2 Even though periodontal structures have restorative traits subsequent to trauma by temporary anchorage devices (TADS), 3 it is of utmost importance to select the insertion sites using clinical and radiographic evaluation of their anatomical details. The proximity of the roots can be avoided by angulating the mini-implant to the long axis of the tooth. This facilitates the placement of the tip of the mini-implant toward the apex of the root. This reduces root proximity as well as increases the contact between the mini-implant and the cortical bone, with increased stability of the mini-implant. Hence, a stent was designed to aid in optimum mini-implant placement (Figures 3a and b). A stent is a surgical guide that aids in the proper placement of the mini-implant in the three dimensions of space, namely, sagittal, vertical, and transverse.
Steps in Fabrication
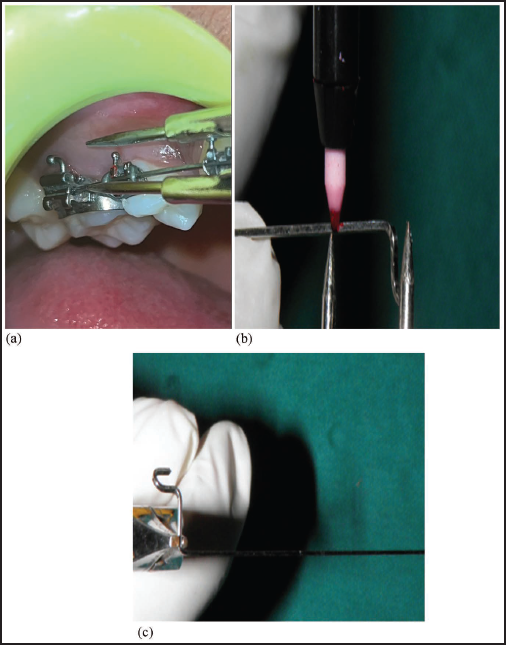
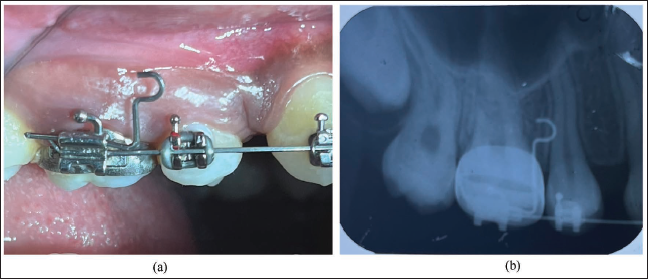
A 0.017 × 0.025″ stainless steel wire of 5 cm was taken, and a small U-bend was made at the end of the wire (Figure 1). A vertical distance was measured from the site of insertion to the level of the auxiliary tube (Figures 2a and b); with the vertical dimension, a horizontal bend was made in accordance with the measurements (Figure 2c). Horizontal distance was measured mesial to the molar tube to the insertion site of the mini-implant (Figures 3a, 3b and 4a), and excess wire was cut. An intraoral periapical radiograph (IOPA) was taken to determine the height of the stent (Figure 4b). After a positive confirmation, the implant was inserted into the designated site (Figures 5a & 5b).
A U-bend was Made at One End of the Wire.
(a) A Vertical Length was Measured from the Site of Insertion of the Mini-implant to the Auxiliary Slot. (b) The Measurement was then Transferred and Marked with a Marker. (c) A 90 Bend is Given for the Insertion of the Wire into the Auxiliary Slot.
(a) Stent with its Parts. (b) Stent as in Model Representation.
(a) Clinically, the Stent was Placed, and the Site was Determined. (b) An Intraoral Periapical Radiograph (IOPA) was Taken for Confirmation of the Placement Site.
(a) An Implant was then Placed. (b) Placement was Confirmed with a Radiograph.

Advantages of STE-NT
It is an easy procedure to fabricate, making it cost-effective.
With placement in the auxiliary slot and the removal of STE-NT being facile, the main slot can still be used by the main archwire without hindrances.
Being versatile, its design can be used in all four quadrants for the placement of mini-implants in the areas of the maxilla and mandible.
With the distance of the vertical height fixed, it not only allows placement of the implant at the correct occlusion gingival height, in the midst of the root mesiodistally, and at an appropriate angulation to the long axis of the tooth, but also the same wire can be used in each of the quadrants to achieve uniformity in the arches for equal force on the archwire.
Conclusion
Anchorage has always been a crucial factor in orthodontics. The use of mini-implants has exceptionally risen in the last few years due to their superiority in clinical efficiency with respect to anchorage control. The precise placement aids in the control of the direction of the force vectors, which enables different tooth movements without compromising the anchorage. The reprobatory concern about mini-implants is their orientation. It is of vital importance to place the implant in a location that does not harm abutting roots or other vital tissues. The wire guide is not only simple in design, easy to fabricate, and inexpensive but can also be used with a variety of mini-screws.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical permission was not applicable for this article, as this is a short communication drafted from various research articles and not from patients directly.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Consent was not needed/not applicable, as this is a short communication compiled from various research articles and guidelines and not from patients directly.