Abstract
Background:
Cleft lip and palate are the most common congenital craniofacial defects, which need early intervention with a multidisciplinary approach including surgeons, orthodontists, speech therapists, pedodontists, etc. Craniofacial growth is affected the most, leading to marked skeletal discrepancies. Constricted maxillary arch is one of the reasons for faulty occlusal inclined planes which results in abnormal loading of condyles, thus leading to temporomandibular disorders (TMDs) in cleft. Condylar head inclination helps to evaluate the position of condyle in the glenoid fossa. Thus, changing the position of condylar head in the glenoid fossa at an early age prevents further worsening of TMD condition. The purpose of this study was to evaluate condylar inclination in individuals with cleft lip and palate and compare it with non-cleft individuals.
Method:
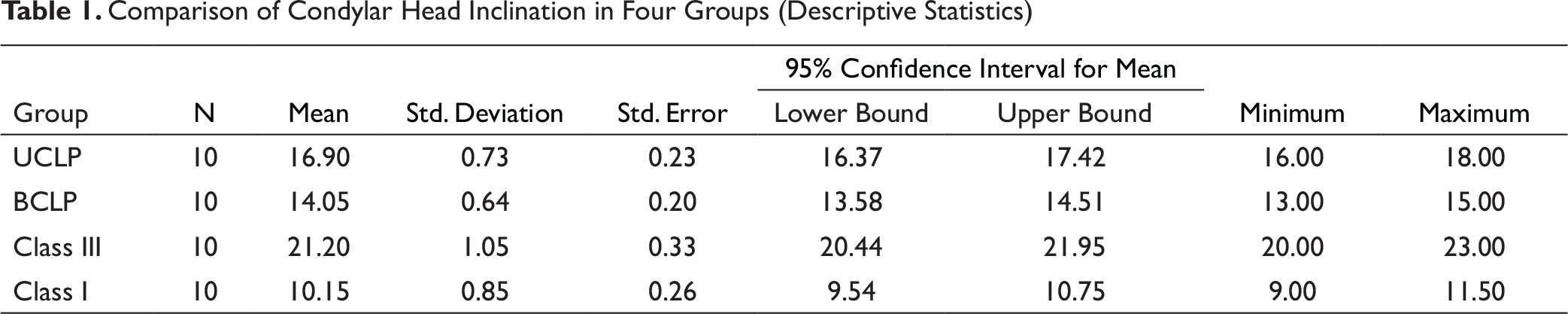
The study comprised of 40 subjects aged between 9 and 12 years, divided into 4 groups (10 in each)—unilateral cleft lip and palate (UCLP), bilateral cleft lip and palate (BCLP), and class III and class I malocclusion. Scanned three-dimensional digital volume tomography (3D-DVT) images were taken, and condylar head inclination was evaluated and compared.
Result:
Significant findings were obtained when group 1 was compared to group 2, group 3, and group 4 (P-value = .001). Also, when group 2 was compared to group 3 and group 4, the values were statistically significant with P-value = .001.
Conclusion:
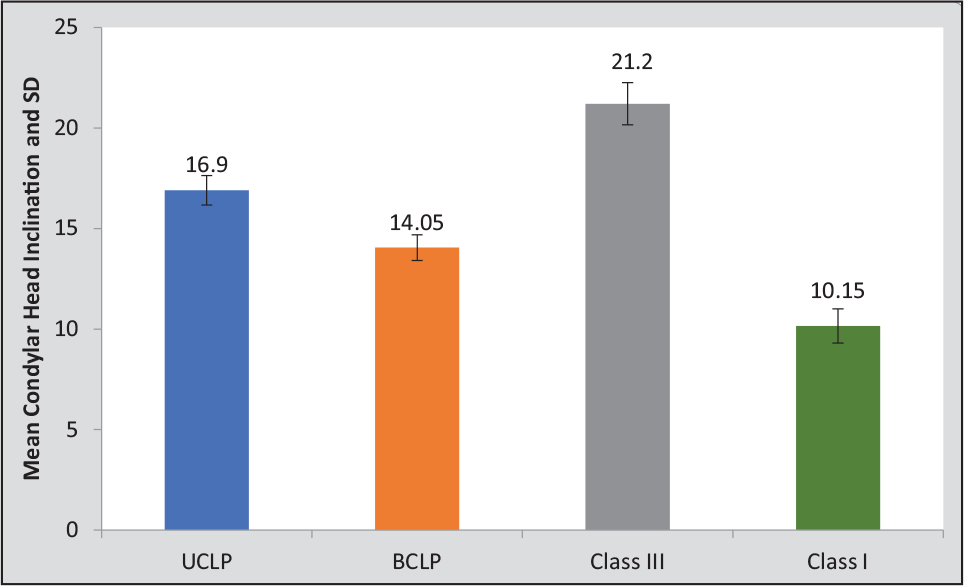
Condylar head inclination was found to be most anteriorly angulated in the class III group compared to all the other groups. Unilateral cleft lip and palate had more anteriorly angulated condyle than bilateral cleft lip and palate.
Introduction
Knowledge regarding the correlation between skeletal and dental components of a particular malocclusion is important in dentofacial orthopedics. This may influence the approach to the treatment. As rightly said by Moss “form follows function,” it is considered that the functional forces affect the morphology of the temporomandibular joint (TMJ). Also, several factors such as age, sex, facial growth pattern, pathological or functional alterations, changes in the muscular activity, and changes in the dental occlusion affect the morphology of TMJ. Due to these changes, as a result of adaptation, there is remodeling and reconfiguration of the TMJ surfaces. 1
To sustain a good occlusion and stomatognathic system, evaluation of mandibular condyle and other structures of TMJ is important. Condylar cartilage resembles the epiphyseal cartilage of the long bones, and thus, mandibular condyle is considered as the chief site for growth of the mandible. 2 Morphology of condyle is known to vary in different malocclusions. 3 Inclination of the condylar head and facial morphology are also corelated. Posterior inclination of the condyle is seen in classic long face syndrome, and anterior inclination of the condyle is associated with anti-clockwise rotation of the mandible. 1
In cleft lip and palate, the growth of craniofacial complex is observed to be affected, leading to marked skeletal discrepancies. Individuals with cleft have constricted maxillary arches, due to which there may be faulty occlusal inclined planes, leading to faulty loading of condyle in TMJ. 4 This is one of the reasons why mandibular growth is altered or deviated. Individuals with cleft usually have varying degrees of class III malocclusion, which is due to the faulty loading of the TMJ and the adaptive changes that occur at the condylar region. 5 Also, the abnormal position of the condyle leads to temporomandibular disorder (TMD) conditions in these individuals. 6 Evaluation of condylar head inclination helps us to know the position of the condyle in the glenoid fossa. Thus, changing the position of the condyle in the glenoid fossa at an early age prevents further worsening of the TMD condition.
Cleft management requires a multidisciplinary and timely approach to prevent skeletal abnormalities. Proper knowledge regarding the altered growth and development is important to prevent skeletal discrepancies by early intervention of the defect. There are limited studies in the literature which focus on the inclination of the condyle in cleft and its effects on the mandibular growth and development in cleft lip and palate cases. The purpose of this study was to evaluate condylar inclination in individuals with cleft lip and palate and compare it with non-cleft individuals.
Materials and Methods
This study was conducted in the Department of Orthodontics and Dentofacial Orthopaedics, Sharad Pawar Dental College and Hospital. Data were collected from the previous research conducted in the department, which were used for evaluation of condylar morphology. The sample size calculation was conducted using G* Power ver.3.1.9.2. to obtain the statistical difference between the groups with 95% confidence (alpha 80%), the estimated samples required per group was 8(~10).
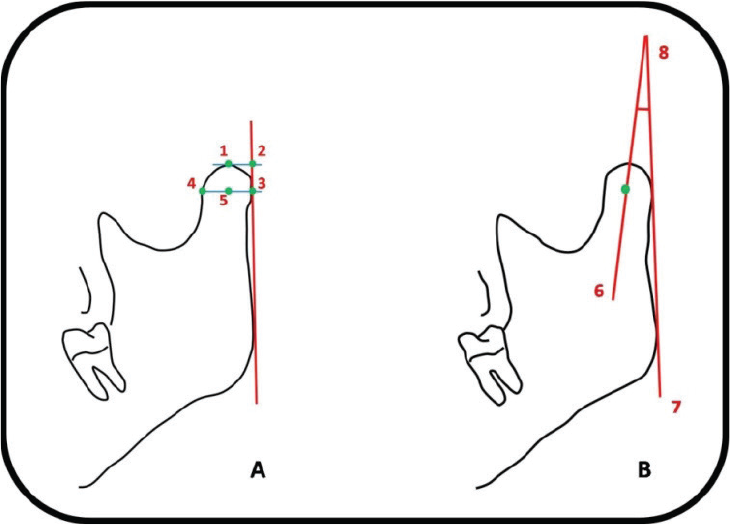
Condylar head inclination. (A) Landmarks and reference planes. (B) Measurements used in this study. 1, Most superior point of condylar head; 2, point intersecting perpendicular projection of point 1 and ramus tangent; 3, outermost point of condylar head; 4, point intersecting perpendicular projection of point 3 and inner condylar outline; 5, midpoint between points 3 and 4; 6, line connecting points 1 and 5 (condylar axis); 7, ramus tangent; and 8, angle between condylar axis and ramus tangent (condylar head angle).
The sample thereby consisted of 40 cases. Individuals between 9 and 12 years were selected and divided into 4 groups with 10 samples in each group.
Group 1: 10 unilateral cleft lip/palate cases Group 2: 10 bilateral cleft lip/palate cases Group 3:10 class III cases Group 4:10 class I cases
The inclusion criteria were as follows:
Samples examined were in the range of 9 to 12 years. Cleft lip, unilateral cleft lip and palate, bilateral cleft lip and palate, and cleft palate only patients who have been previously operated were included.
The exclusion criterion was
Non-syndromic cleft lip and palate patients.
Three-dimensional digital volume tomography (3D-DVT) scanned images which were taken using Phillips Allura Xper FD20 3D RA and digital subtraction angiography unit (Netherlands) with exposure parameters of 80 kvp, 10 Mpa, and 4 to 5 seconds, field of view 12″ 270° rotation, and radiation dose of 1.8 mSv were analyzed.
For each group, condylar head inclination with respect to glenoid fossa was evaluated and compared in (Figures 1 and 2).
Results
Statistical analysis was conducted using descriptive and inferential statistics using one-way ANOVA and multiple comparison (Tukey test) and software used in the analysis was SPSS 24.0 version, and P < .05 was considered as level of confidence.
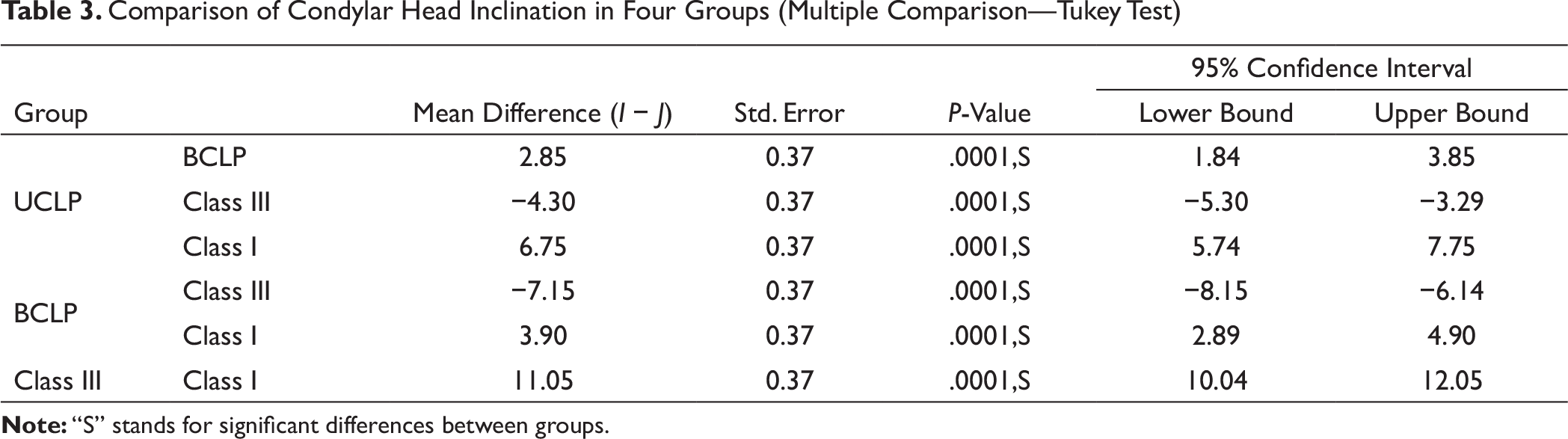
With respect to the condylar head inclination, one-way ANOVA test revealed statistically significant values (P-value = .001*) between the groups and within the groups. Significant findings were obtained when group 1 was compared to group 2, group 3, and group 4 (P-value = .001). Also, when group 2 was compared to group 3 and group 4, the values were statistically significant (P-value = .001) (Tables 1 to 3).
Comparison of Condylar Head Inclination in Four Groups
Discussion
In previous literature, it has been stated that the shape of condyle varies in different skeletal malocclusions. 8 The relation between condyle and fossa might also differ. This correlation between condyle and mandible can be explained by Lavergne and Petrovic’s 7 servosystem theory, which states that “the controlling factors of mandibular growth are the occlusal parameters of maxillary arches due to adaptive changes in the retrodiscal bilaminar zone of condyle.”
Being the most common congenital craniofacial defect, cleft needs early intervention with multidisciplinary approach including surgeons, orthodontists, speech therapists, pedodontists, etc. Faulty loading of condyle in TMJ might result in class III condition in individuals with unilateral cleft. 4 This is because of the constricted maxillary arch which sets the mandible free for sagittal growth, thus affecting the condyles further. Whereas, in individuals with bilateral cleft, the downward placement of premaxilla prevents the growth of mandible even if the maxilla is constricted. The condyle position in glenoid fossa is different in both the cases, resulting in different condylar head inclination in these cases. Therefore, knowledge regarding size, shape, position, angulation, and inclination of the condyle is mandatory in cleft so as to intercept at an early age by altering the position of condyle in the glenoid fossa, thus preventing further worsening of the condition. There are limited studies available on condyle position, inclination, morphology and affected growth in patients with cleft lip and palate. Evaluation of condylar head inclination helps us to know the fault in the position of the condyle, which might lead to temporomandibular dysfunction. 7 Altering the position of the condyle through either orthopedic or functional appliance can prevent further worsening of the TMD condition. Thus, this study was conducted to evaluate condylar head inclination in cleft lip and palate so that the position of the condyle in the glenoid fossa can be determined.
Condylar head inclination was found to be most anteriorly angulated in class III group than all the other groups. Katsavrias and Halazonetis 8 also found similar results stating that class III group has a more elongated and anteriorly angulated condyle in the glenoid fossa. Individuals with unilateral cleft cases have a tendency towards class III condition. In this study, it was observed that UCLP had more anteriorly angulated condyle than BCLP, stating that UCLP had more tendency towards class III condition. Similar findings were observed by Gupta et al, 9 stating that maximum cases of UCLP had a tendency towards class III and class II condition, while BCLP had more tendency towards class II malocclusion. The condyle was found to be more anteriorly angulated in BCLP cases compared to class I condition.
Conclusion
Comparison of Condylar Head Inclination in Four Groups (Descriptive Statistics)
Comparison of Condylar Head Inclination in Four Groups (One-Way ANOVA)

Comparison of Condylar Head Inclination in Four Groups (Multiple Comparison—Tukey Test)