
Abstract
Background
Cleft lip and palate (CLP) is the second most common of visible congenital anomalies. Considering the extent of strain this condition has on the child as well as the parents, it requires a multidisciplinary, protocol-based management approach. Efforts are also on to make this condition notifiable. The rationale of this study is to determine the level of management of CLP in tertiary care centers of Chennai. The objectives are to determine if registers are maintained and linked to a central registry, if multidisciplinary, protocol-based teams manage this condition, and who constitutes such teams along with their level of contribution.
Materials and Methods
Twelve tertiary health care centers providing CLP treatment were identified, including seven public sector hospitals and five private hospitals. Two were dental institutions, and 10 were medical institutions. A structured questionnaire was given to collect information pertaining to the type of register maintained, the information included in the register, whether the registers are linked to a central registry, the constituents of the team, and the type of protocol followed.
Results and Conclusion
Handwritten registers are maintained by the centers, and they are not linked to a central registry. Ten specialists are involved in the multidisciplinary teams. Plastic surgeons, maxillofacial surgeons, and orthodontists contribute the most. Otolaryngologists and geneticists contribute the least. A standard reference protocol is not being followed by the teams.
Introduction
Cleft lip and palate (CLP) is one of the most common congenital anomalies of the craniofacial region, 1 with an incidence of 1 in 700 live births worldwide and 2 in 1,000 births in the Asian subcontinent. 2 Efforts are underway to make this a notifiable disease considering its impact on the child, caregivers, and society as a whole. 3 As part of that exercise, the Indian Council of Medical Research (ICMR) and the Centre for Dental Education and Research, All India Institute of Medical Sciences (AIIMS), New Delhi submitted a task force report in 2016. The report concluded that there is a lack of a central registry for CLP patients. It also highlights observations made by Gopalakrishna and Agarwal 4 about a wide variation in CLP management in India and a lack of an interdisciplinary approach. Studies on CLP conducted in Tamil Nadu assessed the incidence and presentation of CLP.5–8
This descriptive study was undertaken to record the status of CLP management in the tertiary health care centers of Chennai, focusing on whether there is a central registry or database of CLP patients, the specialists involved in CLP management, the existence or otherwise of multidisciplinary teams with working protocols. Presently, no such data are available from the southern part of India.
Materials and Methods
The objectives of this study are
To ascertain the presence or absence of a central registry of CLP patients in the state of Tamil Nadu, India. To identify Government and Private tertiary health care centers in Chennai that manage CLP patients. To get an overview of the total number of CLP cases handled annually in major tertiary care centers of Chennai. To identify specialties that contribute to the management of CLP patients. To describe the role and degree of contribution of the specialties identified. To ascertain if these specialties form multidisciplinary teams with protocols.
The study design is descriptive, and based on a structured questionnaire survey. The questionnaire consisted of 12 questions [Annexure I (Supplementary Material)]. Cronbach’s alpha value of the questionnaire is 8.5 indicating an acceptable reliability. A panel of subject experts verified the content validity of the questionnaire.
The sampling frame included tertiary care medical and dental hospitals, which are described as centers that provide a level of care obtained from all the specialties in medicine and dentistry. The sample consisted of tertiary centers with a record/registry of CLP cases that included information about specialists providing active cleft care.
All Government and Private tertiary health care centers in Chennai were approached with an initial interview with Chief Medical Officer (Government) or Hospital Director (Private) regarding CLP exposure in their centers, centers with medical records of treated cases of CLP were considered as cleft care service providers.
On the basis of the above criteria the tertiary care centers were classified as those managing CLP patients and those that do not. Following the identification of Government and Private tertiary health care centers managing CLP patients, the structured questionnaire was given to the specialists involved and the nodal officers of the centers.
The pertinent information covered by the questionnaire includes
How is the record/database on CLP patients visiting the center maintained? Is such record/database part of a central registry? What are the specialties involved in the management of CLP patients in the center? What is the contribution of individual specialties? If multiple specialties are involved in CLP management in a center, do they work independently or as a team? If a center has a multidisciplinary team managing CLP patients, does the team follow a protocol similar to those recommended by bodies such as the American Cleft Palate-Craniofacial Association? Do centers having multidisciplinary teams to manage CLP patients coordinate with other centers having similar teams?
The questionnaire was self-administered. Filled questionnaires were collected and data were entered in an Excel sheet. The information was verified and validated by the Chief Medical Officer in Governments centers and the Medical Superintendent in Private hospitals. Suitable descriptive statistical analysis was done on the collected data.
Results
Twelve tertiary health care centers were identified as centers managing CLP patients. The centers are Apollo Children’s Hospital Government Royapettah Hospital Government Peripheral Hospital, Tondiarpet See Balaji Dental College and Hospital Institute of Child Health Government Peripheral Hospital, Anna Nagar Tamil Nadu Government Dental College and Hospital Sri Ramachandra Institute of Higher Education and Research Kilpauk Medical College and Hospital Rainbow Children’s Hospital Fortis Maar Hospital, Adyar Stanley Medical College and Hospital
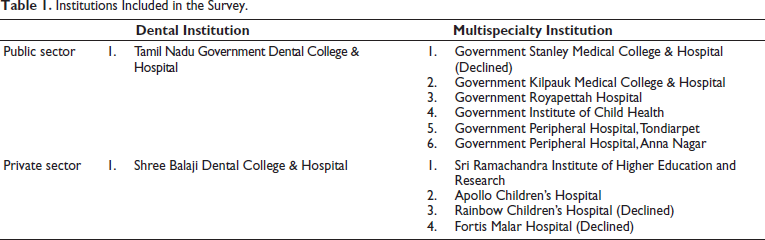
Amongst these 12 centers, 7 are public sector hospitals, and 5 are private hospitals. Two institutions are dental schools (Tamil Nadu Government Dental College & Hospital and Shree Balaji Dental College & Hospital). The remaining 10 institutions are medical schools or multispecialty hospitals (Table 1). Three centers (Rainbow Children’s Hospital, Fortis Malar Hospital, and Stanley Medical College & Hospital) refused to provide data, citing hospital policy. The remaining nine centers responded to the questionnaire with informed consent. Five centers (Apollo Children’s Hospital, Sree Balaji Dental College and Hospital, Institute of Child Health, Tamil Nadu Government Dental College and Hospital, and Sri Ramachandra Institute of Higher Education and Research) directly managed the cleft anomalies and the remaining four centers (Government Royapettah Hospital, Government Peripheral Hospital Tondiarpet, Government Peripheral Hospital Anna Nagar, and Kilpauk Medical College and Hospital) referred the cases to other centers.
Institutions Included in the Survey.
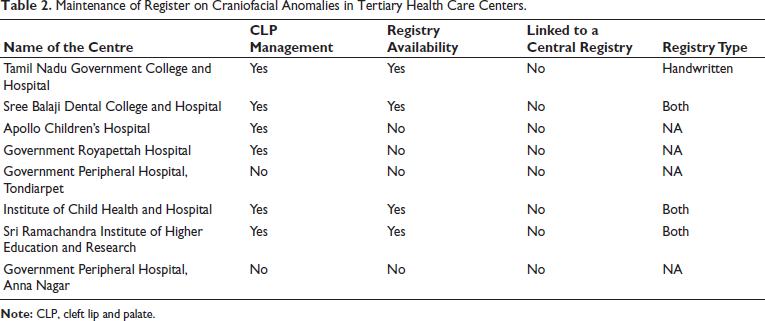
Among the centers that treat CLP cases, four centers: Sree Balaji Dental College and Hospital, Institute of Child Health, Tamil Nadu Government Dental College and Hospital, and Sri Ramachandra Institute of Higher Education and Research, maintain a register of cases with craniofacial anomalies. The registers are handwritten in all centers with some centers maintaining both handwritten and computerized registers (Table 2). The information in the registers maintained in all centers includes Name, OP No, Age/Sex, Diagnosis, and Follow-up period. None of the centers have their registers linked to a central registry. The annual case count of CLP in the centers ranges from five in Government Peripheral Hospital Anna Nagar to 600 in Sree Balaji Dental College and Hospital (Table 3). Sree Balaji Dental College and Hospital is undertaking cleft surgeries, which are funded by Smile Train, an international organization.
Maintenance of Register on Craniofacial Anomalies in Tertiary Health Care Centers.
Annual Case Count of Cleft Lip/Palate Cases in the Tertiary Care Centers.

A multidisciplinary protocol management is followed in three tertiary centers: Sree Balaji Dental College and Hospital, Tamil Nadu Government Dental College and Hospital, and Sri Ramachandra Institute of Higher Education and Research (Table 4). In these centers, the common denominators in the multidisciplinary teams are plastic surgeons, maxillofacial surgeons, orthodontists, pediatric surgeons, and speech therapists.
Multidisciplinary Team Management.
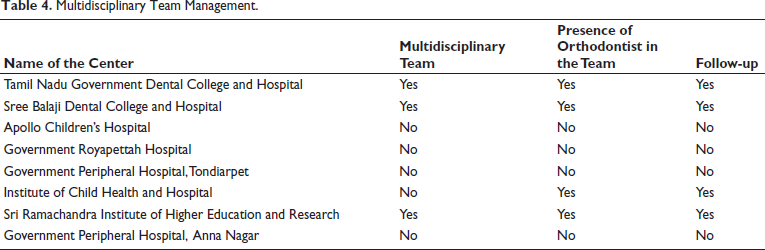
Plastic surgeons, maxillofacial surgeons, and orthodontists contribute the most in the majority of the teams. All the teams are currently not following a structured referral or treatment protocol.
Discussion
The Health Ministry of the United Kingdom constituted a clinical standard advising group that investigated the standards of treatment of CLP patients. 9 Such a standard of treatment care is still not available in India. There has been an ongoing effort to make CLP a notifiable disease. A central registry is a requirement for that. There is a lack of protocol-backed multidisciplinary team management. ICMR’s task force project highlighted these aspects in its report. 2 The role of an orthodontist in the multidisciplinary team is considerably high in our study results. While the ICMR task force found that 28% of cases sought orthodontic treatment after cleft surgery, our results show that 40% of cases seek orthodontic treatment post-primary repair. Speech therapy is another area where the trend shows change. Only 30% of cases had speech therapy as part of the overall management, compared to 77% of cases in the ICMR task force report. Orthodontists, along with plastic surgeons and maxillofacial surgeons, contribute considerably to the management of CLP. However, the study did not include an inquiry into the timing and type of orthodontic interventions. Genetic counseling 10 seems to be an important area that is being neglected. This could be owing to a lack of awareness and the socio-economic background (middle to lower socio-economic status) of the majority of patients reporting this anomaly.
The relevance of this study is being additive to the ICMR task force report in highlighting the need for a central registry of CLP in India, making it a notifiable entity and formulating a standardized protocol for nationwide management of CLP patients.
Conclusion
The salient conclusion of this study is that data on CLP patients is sparse, not systemized, and not linked to a central registry. Registers of CLP cases have demographic data but do not specify the pattern and distribution of the defect. The maximum yearly CLP case count is attributed to two private sector tertiary centers. This could be because of their collaboration with “Smile Train,” an international children’s charity that funds CLP surgeries. Plastic surgeons, maxillofacial surgeons, orthodontists, pediatric surgeons, and speech therapists are contributors in most of the teams. Plastic surgeons, maxillofacial surgeons, and orthodontists contribute the most. Otolaryngologists and geneticists contribute the least in the teams. Multidisciplinary teams, when present, are in want of proper protocol-based coordination.
The above conclusions align with the conclusions of the ICMR task force report and point toward an urgent need to create a central registry for craniofacial anomalies, particularly CLP. A protocol-backed multidisciplinary team management for CLP management is the recommendation of this study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the Institutional Review Board (Ref 1/IERB/2022).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Consent was obtained to use patient records, maintaining confidentiality.