
Abstract
Aim:
To evaluate the effect of primer and its curing techniques on shear bond strength of orthodontic metal brackets and cleaning procedures during debonding of orthodontic adhesive when used with metal brackets.
Materials and Methods:
A total of 100 freshly extracted human maxillary premolar teeth were cleaned to remove blood and tissue debris and stored in distilled water solution until the time of bonding procedures. The samples were divided into 4 groups in which the teeth were then mounted on self-cured, color-coded acrylic blocks such that the roots were completely embedded into the acrylic block up to cement-enamel junction, and the buccal surface of the crown is perpendicular to the base of the block. In group I, brackets were bonded in a conventional manner with the primer cured before placement of the filled adhesive material. In group II, primer was not pre-cured. In group III, primer was not at all applied. All these 3 groups were bonded with Transbond XT (3M Unitek). Group IV was bonded with no primer adhesive, Heliosit (Ivoclar). After bonding, all the samples were tested for shear bond strength with Instron testing machine in shear or peel mode at a crosshead speed of 1 mm/min. The debonded surfaces were examined for Adhesive Remnant Index (ARI) scores under stereomicroscope at 10x magnification. The obtained values were statistically analyzed. An analysis of variance (ANOVA) test was applied to determine whether significant differences in debonded values existed among the groups. The chi-square test was used to determine significant differences in ARI scores among the different groups.
Results:
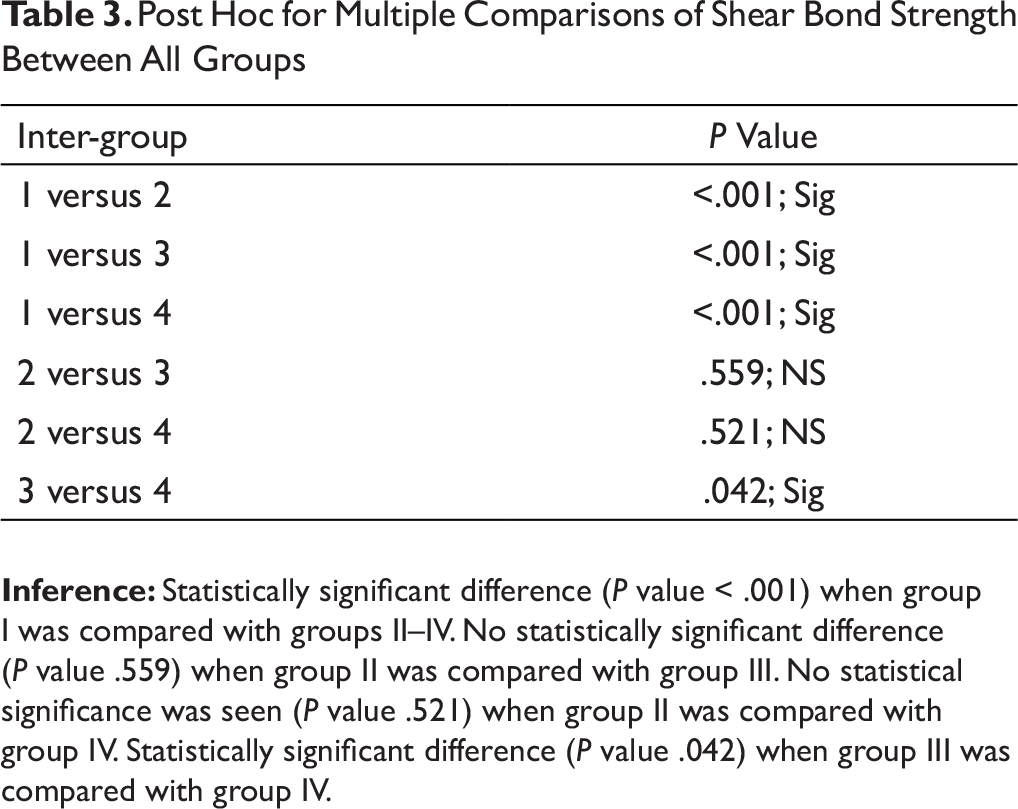
Statistically significant difference (P value < .001) was observed when group I was compared with groups II–IV. No statistically significant difference (P value = .559) was observed when group II was compared with group III. No statistical significance was seen (P value = .521) when group II was compared with group IV. Statistically significant difference (P value = .042) when group III was compared with group IV. Post hoc test was performed for multiple comparisons of ARI scores between all groups. Chi-square test revealed that the differences in percentage distribution of ARI scores between various groups were statistically significant (P value < .001).
Conclusion:
There was a significant difference in the shear bond strength of brackets bonded with Transbond XT and other groups in our study. Even though the average bond strength value of Transbond XT without primer was lower than that of Transbond XT bonded with conventional procedure, it had a low ARI score and eliminated the use of primer. The bond strength values were also considerably greater than the ideal bond strength values required for orthodontic bonding. Hence, the use of Transbond XT without primer made the bonding, debonding and cleaning procedure easy and less time consuming. It also reduced the risk of contact dermatosis in orthodontic personnel and type IV delayed hypersensitivity in patients as the primer was eliminated.
Manuscript
Bonding of orthodontic brackets generally involves etching the enamel surface, application of an unfilled or lightly filled liquid resin onto the etched surface, followed by a filled resin on the bracket base to form the final bond between the bracket and the tooth before self-curing or light curing of the adhesive. Although the manufacturer’s instructions do not mention the need of precuring the liquid resin, some clinicians cure the unfilled resin in a separate step, while others cure both the filled and the unfilled resin together. 1
Limited literature is available regarding the efficacy of light-cured unfilled liquid resin before placement of the filled bracket adhesive. It is an established concept that enamel adhesion is secured by mechanical interlocking between the etched enamel prisms and the polymerized resin tags. An intermediate unfilled low-viscosity liquid resin is, therefore, essential for thorough wetting of the enamel surface, in order to maximize the bond strength.
When curing an orthodontic adhesive, light is not applied directly to the composite material but is rather reflected below the base of the bracket. This mostly creates an area of uncured composite resin adhesive below the bracket, which results in a decreased bond strength. Curing the unfilled resin separately increases the amount of total light delivered to the resin system and, therefore, can have a positive effect on the bond strength.
In order to speed up the process of orthodontic bonding, no primer adhesives have been used. Studies showed similar or slightly lower shear bond strength values when compared with conventional adhesive systems 2 while using this method.
Surface etching using phosphoric acid is known to produce dissolution of the outermost enamel layer and thus provides a mechanical interlock for bonded orthodontic brackets. However, the debonding and subsequent clean-up procedure at the end of treatment may be time consuming. Care must be taken not to induce iatrogenic effects, including cracks, scratches, and removal of pieces of enamel while debonding. Several in vitro bond strength tests denote that bond failure with metal brackets is likely to take place at the adhesive resin–bracket mesh interface. 3 This implies that the mechanical interlocking which occurs when the adhesive penetrates into etched enamel to a depth of 50 μm may be stronger than necessary. So a weaker attachment between the enamel and adhesive would allow an easier and less time-consuming cleanup, without high failure rates.
A series of Norwegian studies showed that orthodontic personnel had the highest incidence of dermatosis on their hands among all sorts of dental personnel.4, 5
If orthodontic bonding could be accomplished clinically without the use of liquid resin, it may be possible to lower the risk of occupational exposure to liquid resin and its unpolymerized components.
Hence, this study was conceptualized to determine the effect of precuring, not precuring, and the absence of primer or use of no primer orthodontic adhesive (Heliosit) during bonding of stainless steel brackets.
Aim
The aim of this article is to evaluate the effect of primer and its curing techniques on shear bond strengths and cleaning procedures during debonding of orthodontic adhesive when used with metal brackets.
Materials and Methods
Sample Preparation
A total of 100 freshly extracted human maxillary premolar teeth were collected and cleaned to remove blood and tissue debris, and stored in distilled water until the start of bonding procedures. The teeth were then randomly distributed into four equal groups (groups I–IV; n = 25 per group), and on the day of bonding, the teeth were mounted on self-cured, color-coded acrylic blocks such that the roots were completely embedded into the acrylic up to the cement–enamel junction, and the buccal surface of crown was perpendicular to the base of the block. The color coding was representative of the respective groups (Table 1) The buccal surfaces of all the samples were then prepared for bonding by pumice polishing with rubber cups, followed by acid etching using 37% phosphoric acid for 30 sec. Stainless steel brackets (Victory SeriesTM MBT, 0.022 slot) were used for all the samples in the study, and the bonding procedure was carried out on the same day for all the groups.
Group Characteristics (Table 1)
In group I, brackets were bonded in a traditional manner with primer applied to etched enamel surface and cured before placement of filled adhesive material. In group II, the primer was not precured before placement of adhesive, and in group III, no primer was applied. All the 3 groups were bonded with Transbond XT (3M Unitek). group IV was bonded with a “no primer adhesive,” Heliosit (Ivoclar).
In all cases, brackets were bonded on the teeth with a firm pressure, and excess adhesive was removed from around brackets. All the procedures were performed by a single operator, in order to avoid inter-operator variability.
Test of Bond Strength
After bonding, all the samples were stored in artificial saliva for 24 h before being subjected to shear bond strength testing in accordance with International Organization for Standardization (ISO) guidelines on testing of adhesion to tooth surface (ISO 11405-2015). The shear bond strength was tested using an Instron machine (Model 8801) in shear or peel mode at a crosshead speed of 1mm/min. The debonded surfaces were examined under stereomicroscope at a magnification of 10×, and ARI scores were given based on the system proposed by Artun and Bergland. 2
Statistical Analyses
The obtained bond strength values were presented as mean values ± standard deviation (SD). Analysis of variance (ANOVA) test was used to determine any significant differences in the mean bond strength values among the groups. For comparison of individual ARI scores across the groups, the chi-square test was employed. In both the instances, results were considered statistically significant at P < .05.
Results
Bond Strength (Table 2 and Figure 1)
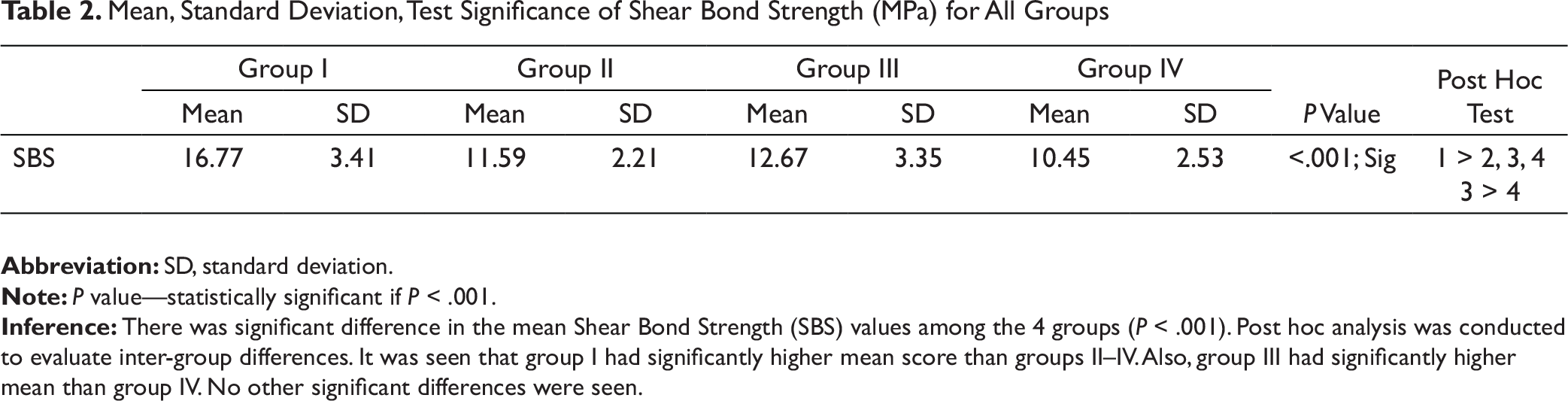
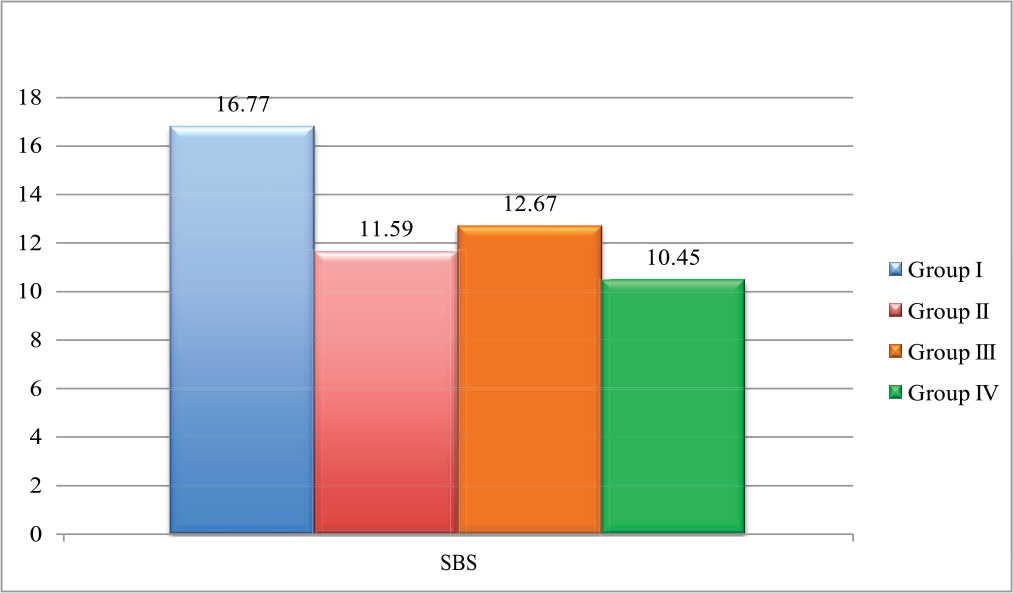
The highest mean bond strength calculated was for group I (16.77 MPa), while it was lowest for group IV (10.45 MPa). Data from Table 3 suggested that there was a statistically significant difference when group I was compared to group II (P < .001), III (P < .001) and IV (P < .001), and when group III was compared to group IV (P = .042). No statistically significant differences were observed when comparing group II to group III (P = .559), and to group IV (P = .521).
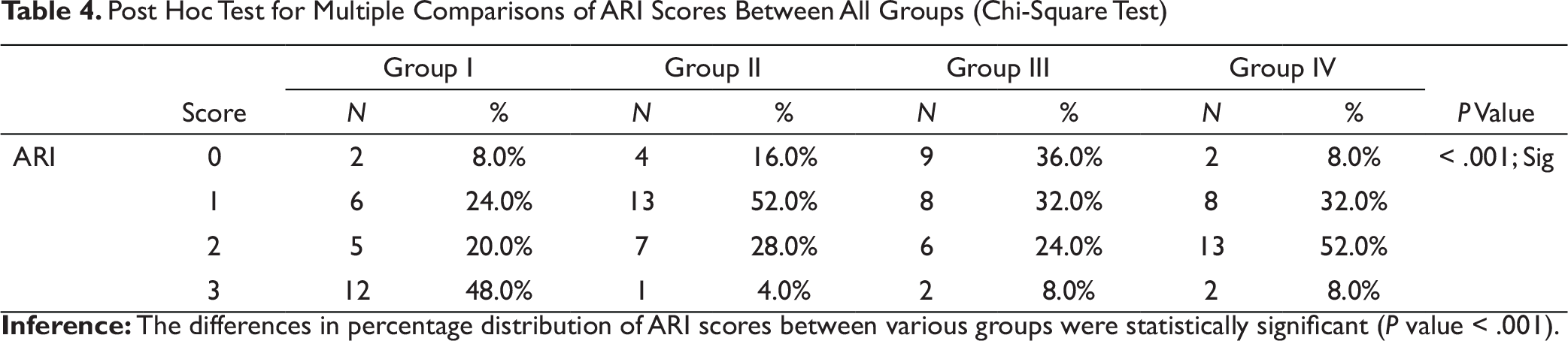
Adhesive Remnant Index Scores (Table 4 and Figure 2)
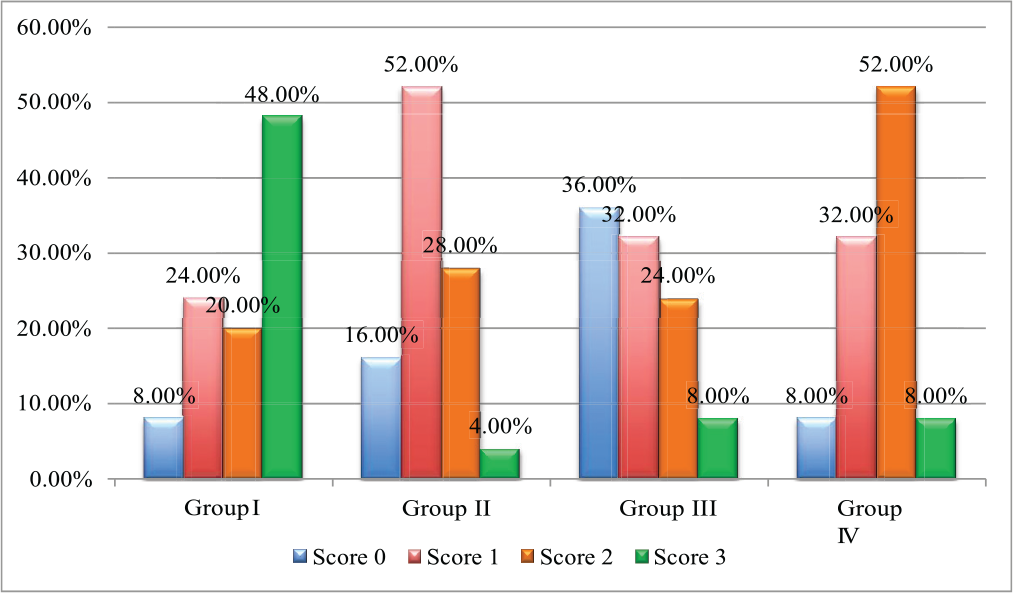
The frequency distribution of ARI scores calculated within each group showed that group I had a greater distribution of score 3 (48%), group II had greater distribution of score 1 (52%), group III had greater distribution of score 0 (36%), and score 2 was more frequently observed in group IV (52%) (see Figure 2).
The post hoc test for multiple comparisons (chi-square test) (see Table 4) showed that the differences in percentage distribution of ARI scores between various groups were statistically significant (P < .001).
Discussion
The study was undertaken in order to evaluate the effect of primer on the shear bond strengths of metal brackets and comparing the ARI scores by precuring the primer, not precuring the primer, and not applying the primer at all on the tooth surface before the application of orthodontic adhesive and thereby to improve the bonding and debonding procedure by minimizing or eliminating the iatrogenic effects of orthodontic bonding and debonding.
Any orthodontic bonding accomplished with adequate retention along with the following features will have superior clinical advantages
2
:
Easier and quicker debonding with little damage to the enamel surface. Minimal effect on the outer, fluoride-containing enamel surface. No resin tags left behind in the enamel surface.
The conventional bonding system used to place orthodontic brackets has proven to be reliable over time, but the procedures have changed very little from the introduction by Buonocore and Newman in the 1950s and 1960s. The systems create an etched surface on the enamel, which, when washed and dried, creates a high-energy surface that is readily wetted by the resin. A liquid resin wets the etched surface, creating resin tags that provide mechanical retention, which helps in achieving good bond strength. 1
Group Characteristics

Mean, Standard Deviation, Test Significance of Shear Bond Strength (MPa) for All Groups
The Mean of Shear Bond Strength of Groups I–IV
Post Hoc for Multiple Comparisons of Shear Bond Strength Between All Groups
It was also anticipated that the time spent for the cleanup of tooth after debonding the brackets will be shortened because the composite residue left on the teeth will be minimal since no resin tags are formed when primer is not applied. But this has to be achieved without jeopardizing the ability to maintain clinically useful bond strength and without causing any deleterious effects on the tooth structure. 2
The Transbond XT system has become the gold standard for bonding brackets and buttons in orthodontic practice, thanks to its ideal consistency, light curing capability, and superior adhesion. Because of the difficulty in comparing the properties of the materials and the brackets between different studies, most researchers used Transbond XT as a control group. 6
The Frequency Distribution of ARI Scores of Groups I–IV
The quest to overcome shortcomings of conventional filled composites has led to the development of flowable composites. They merit great attention due to good clinical characteristics. Heliosit (Ivoclar Vivadent), a primerless orthodontic bonding composite has been scarcely studied. Unique properties of a primerless system include increased strength, non-stickiness, adequate working time, and short curing time. One step of applying primer to the etched enamel surface as well as to the underside of the bracket is eliminated, giving the orthodontist extra clinical working time and rebonding costs. 7
In this study, Transbond XT with different types of bonding techniques (groups I,–III) is compared to no prime adhesive Heliosit (group IV) to evaluate shear bond strength and ARI scores.
Post Hoc Test for Multiple Comparisons of ARI Scores Between All Groups (Chi-Square Test)
The bond strength values (11.59 MPa) of group II were less when compared to group I, probably because the primer was not cured due to insufficient exposure to light. Bradburn and Pender 9 proposed similar results. This group showed ARI score of 1, which suggests that the bond failure has occurred within the composite, leaving adhesive on both tooth surface and bracket base as well, but more on the bracket base. This is probably because the primer has not cured completely due to insufficient exposure to light. This might be the reason for reduced bond strength values. This would allow easier cleaning, but the disadvantages of using primer like delayed Type-IV hypersensitivity and occupational dermatosis on the hands of dental personnel still remain.
The bond strength values (12.67 MPa) of group III was less than group I but greater than group II. The difference in bond strength between groups II and III was not statistically significant. This is in accordance with previous study by Tang et al 5 and Oesterle et al. 11 This group showed an ARI score of 0, which suggests that the bond failure has occurred at the tooth surface–composite interface, leaving no adhesive on the tooth surface. This reduced ARI score might be due to the absence of resin tag formation. 14 Although resin tags were not formed when the primer was not applied, intimate contact of the filled resin with the enamel was adequate to produce sufficient bond strength.
The bond strength values (10.45 MPa) achieved using Heliosit were the lowest among all the groups, but still more than the minimum bond strength value proposed by Reynolds. 15
This group showed an ARI score of 2, which suggests that the bond failure has occurred within the composite leaving adhesive on both tooth surface and bracket base as well, but more on the tooth surface. This is probably due to formation of resin tags because of the low viscosity of the material. This is supported by studies conducted by Scribante et al. 8 Even the bond strength values were lower than the achieved when Transbond XT adhesive was cured without primer application.
The bond strength values achieved without precuring the primer and without primer application were significantly greater (11.59 MPa and 12.67 MPa, respectively) than the minimum bond strength value of 6–8 MPa for orthodontic brackets proposed by Reynolds. 15
Recent randomized controlled trial by Nandhra et al 14 studied the clinical bond failure of metallic brackets bonded with and without primer. In our study, measuring the bond strength values and ARI scores provided a more comprehensive insight on the significance of primer during orthodontic bonding. The bond strength values, although lower than that of conventional bonding procedure, are still more than ideal bond strength values required. This study also suggests an advantage of using Transbond XT without primer, in that this makes the bonding, debonding, and cleaning procedure easy and less time consuming.
Other factors which should have been considered in this study are the effect of consistency of the resin and procedural bias of the clinician on the shear bond strength values of the adhesive.
According to Andrea Scribante, brackets with 80-gauge mesh base has presented higher shear bond strength with Transbond XT conventional adhesive system (with priming) and with Heliosit no-primer adhesive, thus indicating that with these devices, adhesion is not influenced by the filler content but by resin type. 8
Although precautions are taken, there might be some procedural errors like variation in application of pressure while pressing the bracket to the tooth surface. Application of controlled bonding pressure through a bracket holder that has a pressure gauge could be another way to gain a homogenous adhesive thickness between the bracket and enamel.
Further studies can be done considering the aforementioned aspects.
Further research by doing a scanning electron microscopy (SEM) study of the debonded tooth surface to check for the enamel cracks and resin tag formation in the various groups can be conducted to evaluate the results better.
Conclusion
The results of our study indicate that the use of Transbond XT without primer produced clinically acceptable bond strength values and thus are easier and faster to clean up during the debonding procedure.
Clinical Relevance
Orthodontic bonding can be carried out without primer application, which subsequently minimizes the risk of contact dermatosis in orthodontists and type IV delayed hypersensitivity in patients. The time consumed for bonding can also be considerably reduced, owing to the elimination of a step in the procedure.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.