
Abstract
The purpose of this review is to clarify the terminology, possible cells of origin, and expected behavior of the most common synovial tumors in dogs. The synovial lining consists of 2 cell types, type A and type B. Type A synoviocytes are histiocytes of bone marrow origin that are immunoreactive with antibodies against typical markers of histiocyte origin, such as CD18, Iba-1, and CD204. Certain breeds and dogs with previous injury to a joint, especially cranial cruciate ligament rupture, are predisposed to synovial histiocytic sarcoma. Type B synoviocytes are mesenchymal cells that produce synovial fluid. There are no specific markers of type B synoviocytes, but based on their gross and microscopic appearance, synovial myxosarcomas (previously considered synovial myxomas) are presumed to be of type B synoviocyte origin. These can infiltrate into surrounding tissues, but are slow-growing and rarely metastasize, and then only to regional lymph nodes. Synovial histiocytic sarcomas and myxosarcomas can cause lysis in multiple bones surrounding the joint, but they have different prognoses and require histopathology and sometimes immunohistochemistry to diagnose them. Synovial sarcoma and synovial cell sarcoma are terms used in the human medical literature for a tumor that is not of synovial origin; these terms should not be used in veterinary medicine.
Keywords
In humans and other animals, sarcomas of synovial origin have been plagued by confusing terminology. The purpose of this review is to clarify the terminology, possible cells of origin, and expected behavior of the most common synovial tumors in dogs. The histology of normal synovium is similarly confusing, with some histology textbooks having no mention of synoviocytes at all 32 and some naming the cells synoviocytes but not mentioning that they comprise multiple cell types. 35 Most textbooks describe 2 synovial cell types,42,44 but some publications describe a third intermediate type, based on ultrastructural characteristics, especially in fetal synovium.4,13,43 The existence of an intermediate cell type has been refuted by transmission electron microscopy of serial sections of synovium. 15 The two most widely accepted types of synoviocytes are type A (phagocytic) and type B (which produce synovial fluid). 44 These two cell types are indistinguishable by routine staining and together form a thin (1-2 cells-thick) layer that lines the inside of joints, bursae, and tendon sheaths. 44 By electron microscopy, type A synoviocytes have a Golgi apparatus, vacuoles, vesicles, microvilli, and microplicae.3,4,15 By immunohistochemistry, type A cells express CD18, a marker of bone-marrow derived cells that is often used to identify histiocytes (dendritic cells and macrophages) in formal-fixed, paraffin-embedded tissues.8,24 They also express Iba-1, a histiocyte marker. 28 By electron microscopy, type B synoviocytes have more rough endoplasmic reticulum.3,4 Type B synoviocytes are often called “fibroblasts,” but they do not produce collagen. They are mesenchymal cells that produce synovial fluid, which has been described as “a highly specialized fluid form of synovial extracellular matrix.” 44 Although heat shock protein 25 and cadherin 11 have been used as markers of type B synoviocytes,2,13,40,43 these also immunolabel many other mesenchymal cell types. 7
Intra-articular tumors in animals can arise from synoviocytes or any of the supporting tissues within the joint. The most common intra-articular tumor in dogs is histiocytic sarcoma, which is reported to arise from interstitial dendritic cells in the underlying synovial tissues. 24 However, much of the data supporting that cell of origin is unpublished 23 and large studies of synovial histiocytic sarcomas have not been performed. This author hypothesizes that some synovial histiocytic sarcomas arise from type A synoviocytes, but data supporting this hypothesis are lacking. The second most common intra-articular tumor is synovial myxosarcoma, which was previously referred to as synovial myxoma. 7 Synovial myxosarcoma presumably arises from type B synoviocytes, although there are no specific markers for type B synoviocytes to confirm this. These two tumors can both cause bony lysis, making them difficult to distinguish radiographically. Because they have different behaviors, histopathology and sometimes immunohistochemistry are essential for making the diagnosis and thereby determining the prognosis.
Synovial Histiocytic Sarcoma
Cell of Origin
There are 2 types of histiocytes from which intra-articular histiocytic sarcoma could arise: type A synoviocytes within the synovial membrane and perivascular histiocytes (interstitial dendritic cells) in the underlying (synovial sublining layer) tissue. Both of these types of cells are immunoreactive with CD18 and Iba-1 antibodies, but only Langerhans cells and less commonly macrophages express E-cadherin. 24 In intraepidermal Langerhans dendritic cells, E-cadherin binds to the E-cadherin expressed by keratinocytes. For comparison, other tumors known to arise from Langerhans cells are pulmonary Langerhans cell histiocytosis in cats, cutaneous Langerhans cell histiocytosis in dogs, and benign cutaneous histiocytomas in dogs. 24 Benign cutaneous histiocytomas arise from intraepidermal or dermal Langerhans dendritic cells and express E-cadherin, in both a membranous and intracytoplasmic pattern.27,31 Histiocytomas do not express E-cadherin uniformly, and some do not express it at all. 24 Most histiocytic sarcomas in nonsynovial locations arise from interstitial dendritic cells, and therefore do not express E-cadherin. 24 In the normal canine synovial lining (2 of 2 dogs examined), there are cells that react with antibodies to E-cadherin (likely type A synoviocytes; Fig. 1a) and cells that do not (likely type B synoviocytes). The E-cadherin positive cells are along the surface of the synovial membrane, which is where type A synoviocytes are located in electron microscopy studies. 15 Although no studies have been performed, some (2 out of 2 in the author’s personal experience) synovial histiocytic sarcomas are immunoreactive for E-cadherin (Fig. 1b), suggesting that they could arise from type A synoviocytes, rather than the interstitial dendritic cells in the surrounding tissues. The labeling in the normal synoviocytes and synovial histiocytic sarcomas is cytoplasmic, rather than membranous as expected, but histiocytomas, which are of Langerhans cell origin, can have either membranous or cytoplasmic labeling for E-cadherin.27,31 Although E-cadherin is not a lineage-specific marker, positive cells within the synovium are unlikely to be anything other than type A synoviocytes (whether they be Langerhans cells or macrophages). Unfortunately, many of the markers that are needed to distinguish subsets of histiocytes require frozen tissues, 25 which are rarely available for retrospective studies. A larger number of synovial histiocytic sarcomas need to be tested for CD1a, E-cadherin, and CD204 expression to determine the cell(s) of origin, and whether the cell of origin affects prognosis.
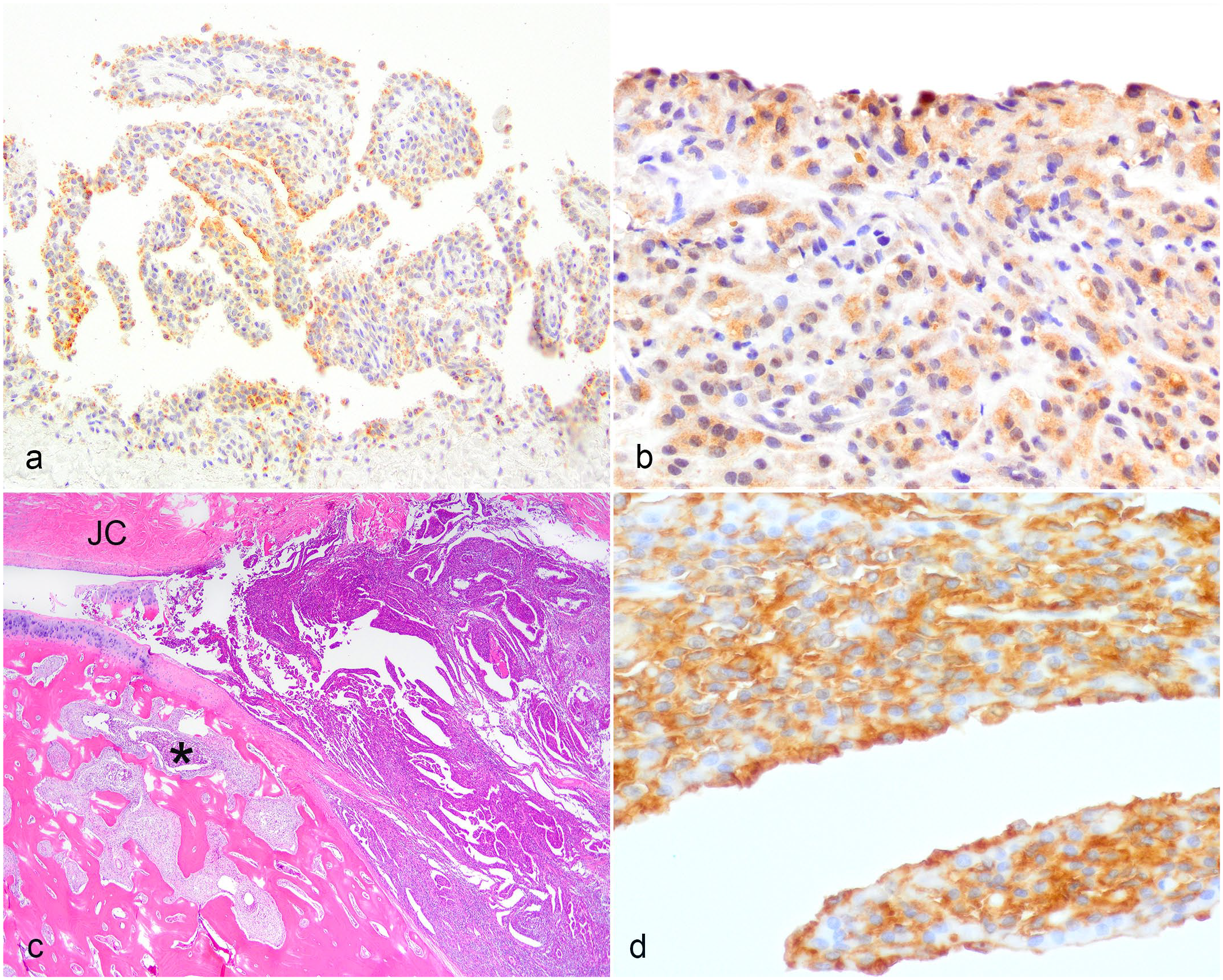
Normal synovium and synovial histiocytic sarcoma, dog. (a) . Normal synovium. The superficial layer of synoviocytes (type A, presumptive) has coarsely granular cytoplasmic E-cadherin immunoreactivity. E-cadherin Immunohistochemistry (IHC). (b) . Synovial histiocytic sarcoma. There is finely granular cytoplasmic E-cadherin immunoreactivity in the cells on the synovial surface and the neoplasm below. E-cadherin IHC. (C) . Synovial histiocytic sarcoma. The neoplasm is within the joint capsule (JC) of an interphalangeal joint and invades into the bone (asterisk). Hematoxylin and eosin. (d) . Synovial histiocytic sarcoma. Higher magnification of neoplasm in (c). The neoplastic cells on the surface and deeper have CD18 immunoreactivity. CD18 IHC.
Some authors refer to synovial histiocytic sarcomas as “periarticular,”17,20,41 but in this author’s opinion, they should be termed articular or synovial histiocytic sarcomas because they arise within the joint, often spreading to surrounding soft tissues, and sometimes bones. Although some are detectable as soft tissue masses before they cause bony lysis, 41 this does not rule out their origin within the joint. Some are grossly and microscopically only inside the fibrous joint capsule 6 and continuous with the synovial lining (Fig. 1c); both the histiocytic sarcoma and the synovial lining contain CD18-positive cells (Fig. 1d). Others are below the synovial lining. 23
Histiocytic sarcomas are more likely to occur in joints with previous injury, including cranial cruciate ligament rupture (with or without repair), patellar luxation, elbow dysplasia, trauma, infectious arthritis, and autoimmune polyarthritis. 21 Presumably, the resulting joint inflammation stimulates chronic activation and, in some dogs, eventual malignant transformation of resident dendritic cells. 6 As all of these predisposing conditions result in synovial inflammation, rather than inflammation of the tissues outside the joint capsule, the resulting neoplasm would be expected to be intra-articular, not periarticular. Not all synovial histiocytic sarcomas are preceded by injury.
Signalment
Histiocytic sarcomas have striking breed predispositions. Bernese mountain dogs are most predisposed with a lifetime risk of 25%, 1 but retrievers (flat-coated and golden), Rottweilers, miniature Schnauzers, and Pembroke Welsh corgis are all more likely to develop histiocytic sarcoma than other breeds.17,25,30 Only the large breeds are predisposed to the synovial form. 16 Rottweilers are especially likely to have prior joint disease. 21 By comparing Bernese mountain dogs and flat-coated retrievers with histiocytic sarcoma, Hedan et al 12 found multiple DNA aberrations in affected dogs that are tumor-specific (shared between breeds), as well as some breed-specific aberrations. DNA aberrations found only in flat-coated retrievers could explain why they are more likely to develop the synovial form of histiocytic sarcoma. 12 Some of the DNA aberrations were in genes associated with apoptosis and tumor suppression, but no single gene has been identified that predisposes to histiocytic sarcoma. 12
Studies limited to Bernese mountain dogs have found that those with prior joint disease are 2.5 times 33 to 5.4 times 41 as likely to develop histiocytic sarcoma than those without. Interestingly, Bernese mountain dogs treated with prescription anti-inflammatory medications for longer than 6 months are less likely to develop histiocytic sarcoma, 33 providing more evidence that the synovial inflammation is contributing to the malignant transformation.
Diagnosis
Because prior injury to the joint, such as cranial cruciate rupture, predisposes to this tumor,17,21 affected dogs often have a preexisting lameness that can delay detection of the neoplasm clinically. Radiographically, there can be bony lysis caused by the neoplastic cells replacing bone, as well as bony proliferations, some of which may be related to the pre-existing degenerative joint disease (Fig. 2a). 36 Grossly, synovial histiocytic sarcomas consist of pink-tan coalescing nodules that line and fill the inside of affected joints (Fig. 2b). 6 The neoplastic nodules also invade and replace bones, surround the joint (Fig. 2a), and infiltrate into the muscle and other soft tissues. 6
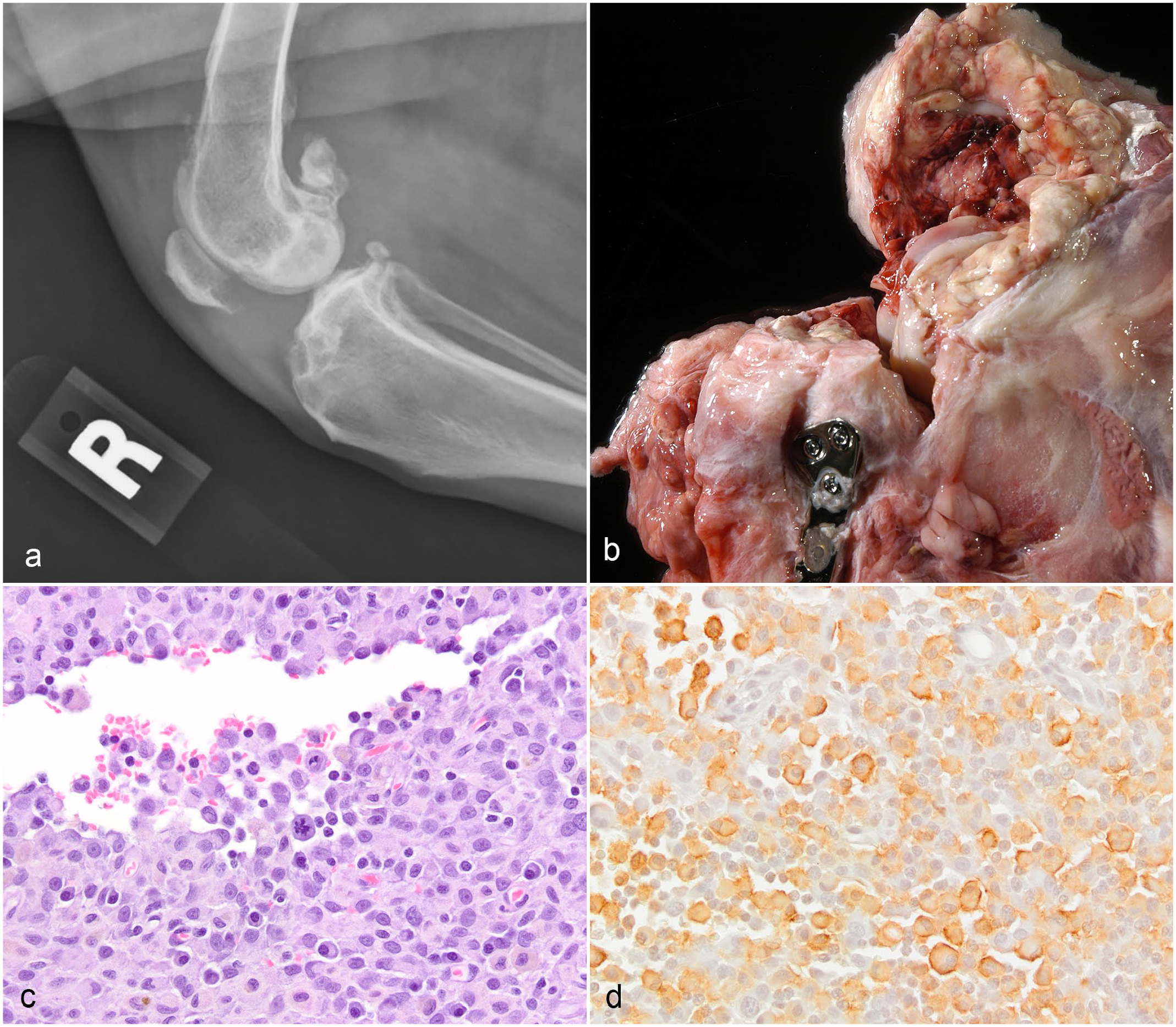
Synovial histiocytic sarcoma, dog. (a) . Radiograph of the stifle showing bony lysis in the distal femur, proximal tibia, and patella. (b) . Pale tan-pink nodules line and fill the stifle joint. Prior to development of this tumor, this dog had a ruptured cranial cruciate ligament and tibial plateau–leveling osteotomy. (c) . Most of the cells in this field are malignant histiocytes, with a background of inflammatory cells (mostly lymphocytes and plasma cells). Hematoxylin and eosin. (d) . Same neoplasm as in (c) . The neoplastic histiocytes (larger cells) have membranous IBA1 immunoreactivity. IBA1 immunohistochemistry.
The microscopic appearance of synovial histiocytic sarcomas is similar to histiocytic sarcomas in other sites. The cells are round to polygonal to spindle shaped, with eosinophilic cytoplasm. The cell margins are variably distinct, and there can be cytoplasmic vacuoles. 8 Nuclei range from irregularly oval with minimal anisokaryosis to markedly pleomorphic. Many histiocytic sarcomas have multifocal to diffuse infiltrates of inflammatory cells, which can include lymphocytes, neutrophils, and eosinophils (Fig. 2c). Immunohistochemistry for CD18, Iba-1, or CD204 can be used to confirm the histiocytic origin of the neoplastic cells. Although CD18 is a panleukocyte marker, neoplastic cells with typical histiocytic morphology (abundant cytoplasm) that are CD18-positive can be identified as histiocytic. The CD18 labeling may be cytoplasmic or membranous. Iba-1 is expressed in all histiocytic cells (including both dendritic antigen presenting cells and macrophages) and in microglial cells. CD204 is a scavenger receptor and another useful marker to confirm histiocytic origin; it is expressed by some, but not all, macrophages and interstitial dendritic cells, but not by Langerhans dendritic cells. 23 Not all of the neoplastic cells within a histiocytic sarcoma will label with these markers (Fig. 2d), but finding features of malignancy within the cells that do label confirms that the neoplasm is histiocytic. The pathogenesis of this uneven immunolabeling pattern is not known, but the presence of an intra-articular neoplasm (space-occupying and with features of malignancy) helps differentiate histiocytic sarcoma from a nonneoplastic infiltration of antigen presenting cells.
Prognosis
Dogs with histiocytic sarcomas that arise within joints have a better prognosis than those with histiocytic sarcomas that arise elsewhere (overall median survival time of 391 days for synovial and 128 days for nonsynovial histiocytic sarcomas). 16 No other prognostic factors (such as mitotic count or immunohistochemical labeling pattern) have been reported.
Synovial Myxosarcoma
Cell of Origin
Type B synoviocytes are mesenchymal cells that produce synovial fluid. 44 Synovial myxosarcomas are mesenchymal tumors that arise within joints and contain abundant viscous fluid grossly; microscopically, they comprise sparsely cellular nodules with abundant pale basophilic extracellular matrix. 7 Therefore, it is logical to hypothesize that these tumors arise from type B synoviocytes. The neoplastic cells have minimal atypia and only rare mitotic figures. The original reports of this tumor used the term “synovial myxoma”7,29 because they are slow-growing and were not previously known to metastasize. However, they do rarely metastasize to regional lymph nodes (Brian Murphy, personal communication and author’s personal observation), and they invade into bone and along fascial planes, sometimes to the amputation margin, 9 so a more appropriate term would be “synovial myxosarcoma.” Because the synovial myxomatous tumors that have metastasized have been histologically similar to those that have not metastasized, with no more mitotic figures or other histologic features of malignancy, in this author’s opinion, all of them should be diagnosed as myxosarcoma.
Signalment
Breed predispositions are not as pronounced for synovial myxosarcomas as for synovial histiocytic sarcomas. A multi-institutional review of 39 cases included 11 Doberman pinschers, 10 Labrador retrievers, 4 Basset hounds, 3 Rottweilers, 2 Shetland sheepdogs, 6 mixbreed dogs, and 1 each of miniature poodle, labradoodle, and beagle. 7 However, the 9 cases diagnosed at the University of Tennessee since that publication include no Doberman pinschers, 2 Labrador retrievers, 2 mixbreed dogs, and 1 each of Basset hound, Shetland sheepdog, Norwegian elkhound, border collie, and golden retriever. The average age at the time of diagnosis is 8.5 years (range = 2–14 years). 7 Combining cases from the 2010 publication 7 and the 9 cases since, the stifle is the most commonly affected joint (40%) followed by the tarsus (23%), digit (21%), elbow (6%), carpus (6%), hip (2%), and vertebrae (2%).
Diagnosis
Radiographically, synovial myxosarcomas are difficult to distinguish from synovial histiocytic sarcomas because both can cause bony lysis (Fig. 3a).6,9 Grossly, synovial myxosarcomas can contain pockets of clear viscous fluid resembling synovial fluid (Fig. 3b) and the affected joint often contains excessive similar fluid. 7 Cytologically, this fluid resembles synovial fluid: sparsely cellular with a pink matrix. 8
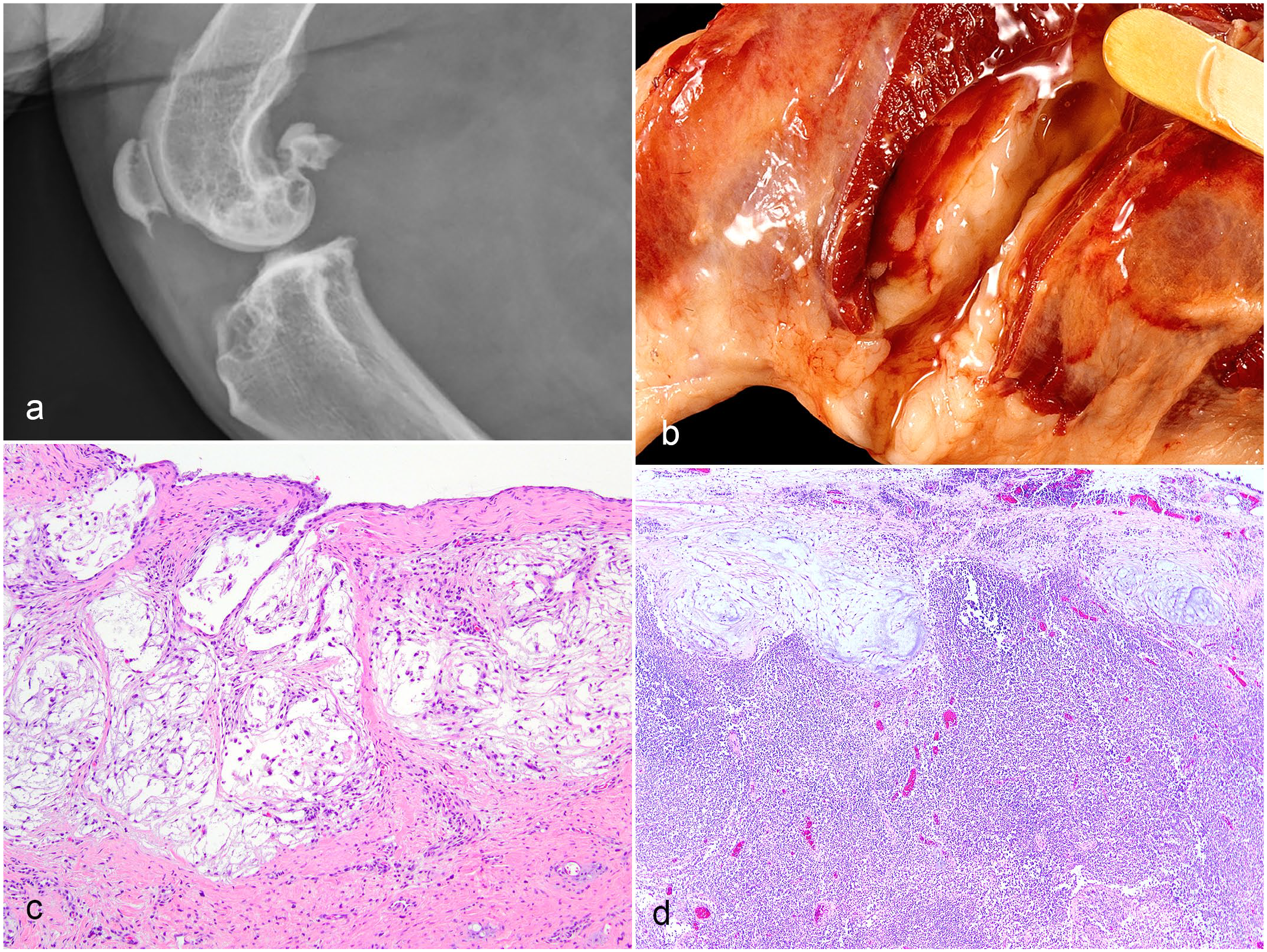
Synovial myxosarcoma, dog. (a) . Radiograph of the stifle joint showing bony lysis in the distal femur, proximal tibia, and patella. (b) . Periarticular pockets of clear viscous fluid surround the affected stifle. (c) . The tumor consists of sparsely cellular nodules of stellate mesenchymal cells suspended in a pale basophilic to clear myxomatous matrix. Hematoxylin and eosin (HE). (d) . Metastatic nodules at the periphery (subcapsular sinus) of a lymph node.
Histologically, synovial myxosarcomas have a distinctive nodular pattern, with each nodule consisting of sparse stellate mesenchymal cells suspended in an abundant clear to pale basophilic extracellular matrix (Fig. 3c). 7 The neoplastic cells have small hyperchromatic nuclei with no features of malignancy. Some areas of the tumor will be more cellular with less matrix. The microscopic appearance of this tumor is characteristic and diagnostic. Although immunohistochemistry has been attempted to identify the cell of origin as type B synoviocytes, no marker has been shown to be specific for this cell type.7,15 Immunohistochemistry is not required or helpful in diagnosing this tumor.
Prognosis
Synovial myxosarcomas are slow-growing tumors, and the clinical signs of lameness and joint swelling can mimic degenerative joint disease. The average duration of clinical signs before diagnosis is 6 months, with a range of 1 week to 3 years. 7 Amputation is often required for complete excision, but survival times are long (average 2.5 years), even with incomplete excision. 7 The myxomatous nodules of neoplastic cells infiltrate along fascial planes and can invade into bone causing lysis. 7 Rarely, metastasis to regional lymph nodes occurs (Brian Murphy, personal communication and author’s personal experience). In the 9 cases seen by Dr Murphy and this author, the metastatic nodules resemble the primary tumor and are often at the periphery of lymph nodes (Fig. 3d), suggesting they arrive through afferent lymphatic vessels. Although most sarcomas metastasize through blood vessels, rather than lymphatic vessels,10,11 in dogs, subcutaneous myxosarcomas are more likely to metastasize to lymph nodes than other sarcoma types. 14 Although these tumors are locally infiltrative and can metastasize, they still have a relatively good prognosis, in that none of the reported cases resulted in the death or euthanasia of the patient. 7 Metastases beyond regional lymph nodes have not been reported.
“Synovial Cell Sarcoma”
The diagnosis of synovial cell sarcoma should not be used in veterinary medicine. In human medicine, this term (or the more current “synovial sarcoma”) denotes a tumor that can arise anywhere in the body and is not of synoviocyte origin.18,23,34,37,39 The misnomer arose from the resemblance of the neoplastic cells to embryonic synovium. Based on the cytokeratin expression of this misnamed nonsynovial neoplasm, cytokeratin expression has been inaccurately recommended to identify synovial cell sarcomas in animals. 6 Based on this recommendation, cytokeratin expression has been mistakenly used as a marker of synovial origin for both intra-articular19,26 and extra-articular20,38 tumors in animals. As cytokeratin is a marker for a tumor in humans, which is known to be of nonsynoviocyte origin, it should not be used in veterinary medicine to diagnose synovial neoplasms. One suggestion has been to use the term “cytokeratin-positive joint-associated sarcoma,” 22 but cytokeratin-positive sarcomas can occur anywhere in the body,5,11 and a recent study comparing 25 subcutaneous and 7 periarticular sarcomas showed that the expression of cytokeratin by sarcomas does not differ by location or affect prognosis. 9 Therefore, there is no need to test sarcomas, synovial or otherwise, for cytokeratin expression.
Other Sarcomas That Can Occur Within Joints
Other mesenchymal cells within joints can give rise to sarcomas. A few examples include fibroblasts (fibrosarcoma), adipocytes (liposarcoma), and chondrocytes (chondrosarcoma). 6 The diagnosis, treatment, and prognosis of these tumors should be the same as their extra-articular counterparts.
Footnotes
Acknowledgements
The author thanks Dr Silke Hecht for providing the radiographs, Dr A. James Cooley for providing Fig. 3b, and Dr Danielle Reel for providing the slide for ![]() .
.
Author Contributions
LEC wrote the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.