
Abstract
This report describes the clinical and pathologic characteristics of cystic and myxomatous lesions of synovial joints in 16 cats. The average age was 13.4 years. The elbow was most commonly affected (12/16), and all lesions were unilateral. Degenerative joint disease was a frequent concurrent but bilateral condition. The lesions consisted of fluid-filled cysts lined by synoviocytes (3 cases), solid foci of stellate cells in a myxomatous matrix (2 cases), or a combination of the two (11 cases). In some cases there were areas of transition between the cystic and myxomatous lesions. Mitoses and other features of malignancy were rare to nonexistent. In the 13 cats with follow-up information, the lesion gradually increased in size over a period of years. None of the cats died or were euthanized because of this lesion. We propose that some cats with degenerative joint disease develop synovial cysts, which have the potential to transform to a synovial myxoma.
Degenerative joint disease (DJD) is a gradual breakdown of articular cartilage with periarticular bony proliferation most often related to joint laxity. Radiographically detectable DJD is common in cats and increases with age. 6,10 The hip and elbow joints are commonly reported to be affected, but these joints are often included on thoracic and abdominal radiographs, so their overrepresentation may be a sampling bias. 10 Feline DJD is often bilateral, especially in the elbow joints. 4 Synovial cysts are herniations of synovial membrane associated with DJD. 14,16 Their formation is presumed to be the result of increased intraarticular pressure. 5 Despite the prevalence of DJD, synovial cysts are rare. In one detailed study of DJD in the elbows of 22 cats, no synovial cysts were reported. 4
Canine synovial myxomas mostly occur in the stifle and digits of large breed, middle-aged dogs. 2 They have a characteristic microscopic appearance consisting of round nodules of stellate cells within a myxomatous matrix. The neoplastic nodules can invade into bone, muscle, and along fascial planes between muscles. 2 Rarely, they metastasize to regional lymph nodes (Brian Murphy, personal communication). The purpose of this study was to provide similar diagnostic and prognostic information about feline synovial myxomas.
The anatomic pathology databases at the University of Tennessee College of Veterinary Medicine and Athens Veterinary Diagnostic Laboratory were searched from January 1, 2002, until December 30, 2018, for feline species combined with the words synovium, synovial, or joint, and words containing “myxo-”. All reports identified in the search were reviewed, and cases indicating cysts or a myxomatous tumor near a joint were evaluated. The histopathology slides from potential cases were reviewed by 2 pathologists (PMK and LEC) to confirm cases of synovial cysts or myxoma. Two additional cases were submitted to one of the authors (LEC) for second opinion consultation. All cases included routinely processed biopsy submissions and hematoxylin and eosin–stained slides. Immunohistochemistry was performed manually on 13 synovial cyst and/or myxoma cases for vimentin (Agilent, Santa Clara, CA), CD18 (Ca16.3c10, Peter Moore, University of California-Davis), and IBA-1 (Wako-Chem) on formalin-fixed, paraffin-embedded 5-µm sections. Antigen retrieval was performed for CD18 using proteinase K (Agilent, Santa Clara, CA) at room temperature for 5 minutes, and for vimentin and IBA-1 using heat (95 °C for 20 minutes). A horseradish peroxidase–labeled polymer system (Envision+, Agilent, Santa Clara, CA), with diaminobenzidine as chromogen, and hematoxylin counterstain were applied to all slides.
Most cats were presented for a slowly progressive unilateral enlargement of the elbow joint, with or without lameness. In lame cats, the lameness was attributed to DJD, as it was unrelated to the severity of the soft tissue enlargement. The duration of clinical signs was rarely recorded but ranged from 9 months to 2 years prior to presentation. The swelling was described as multilobular, cystic, fluctuant, or firm, and slowly enlarged to eventually extend down the antebrachium and proximally along the humerus over a period of years. Radiographs were performed in 5 cases and showed bilateral DJD with osteophytes, but no bone lysis. Radiographically, the masses were of soft-tissue consistency. Six cats were not radiographed, but had similar DJD findings on physical examination, such as stiffness, joint capsule thickening, and periarticular bony enlargement.
The site, age, treatment, survival time, and cause of death are listed in Table 1 for the 16 cats in this study. Two cats were euthanized for renal failure, and the lesions were diagnosed at necropsy, although they had been noted clinically. The survival time was available for 12 cats and ranged from 6 months to 5 years; the average was 2.3 years; 5 cats were still alive at the time of writing. No deaths were attributed to the cystic or myxomatous synovial lesions, but 2 cats were euthanized for severe DJD. Eight cats were spayed females, 7 were neutered males, and in 1 case the sex was not provided. Ten cats were domestic shorthair, and there was 1 each of the Angora, European shorthair, Maine coon, Persian, and Siamese breeds.
Site, Microscopic Findings, Age, Treatment, Survival and Outcome of 16 Cats with Synovial Cystic and Myxomatous Lesions.
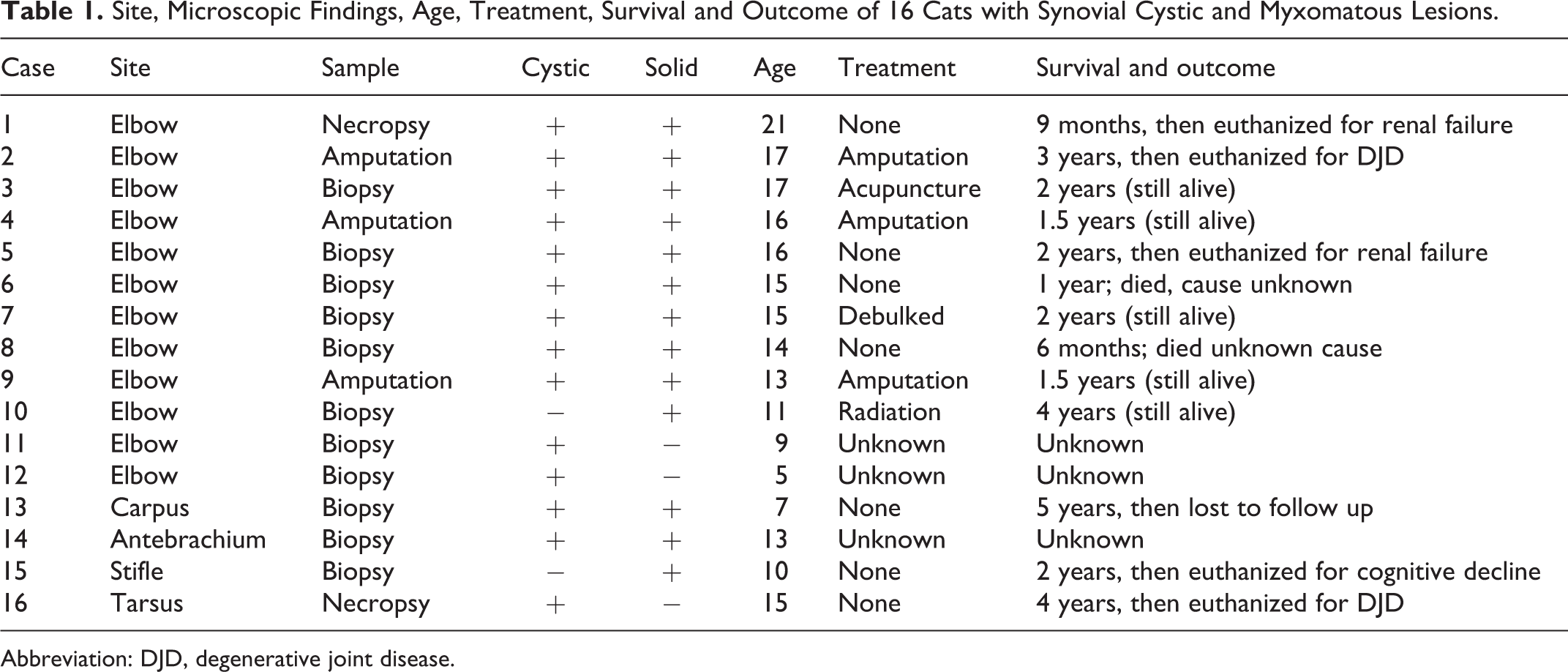
Abbreviation: DJD, degenerative joint disease.
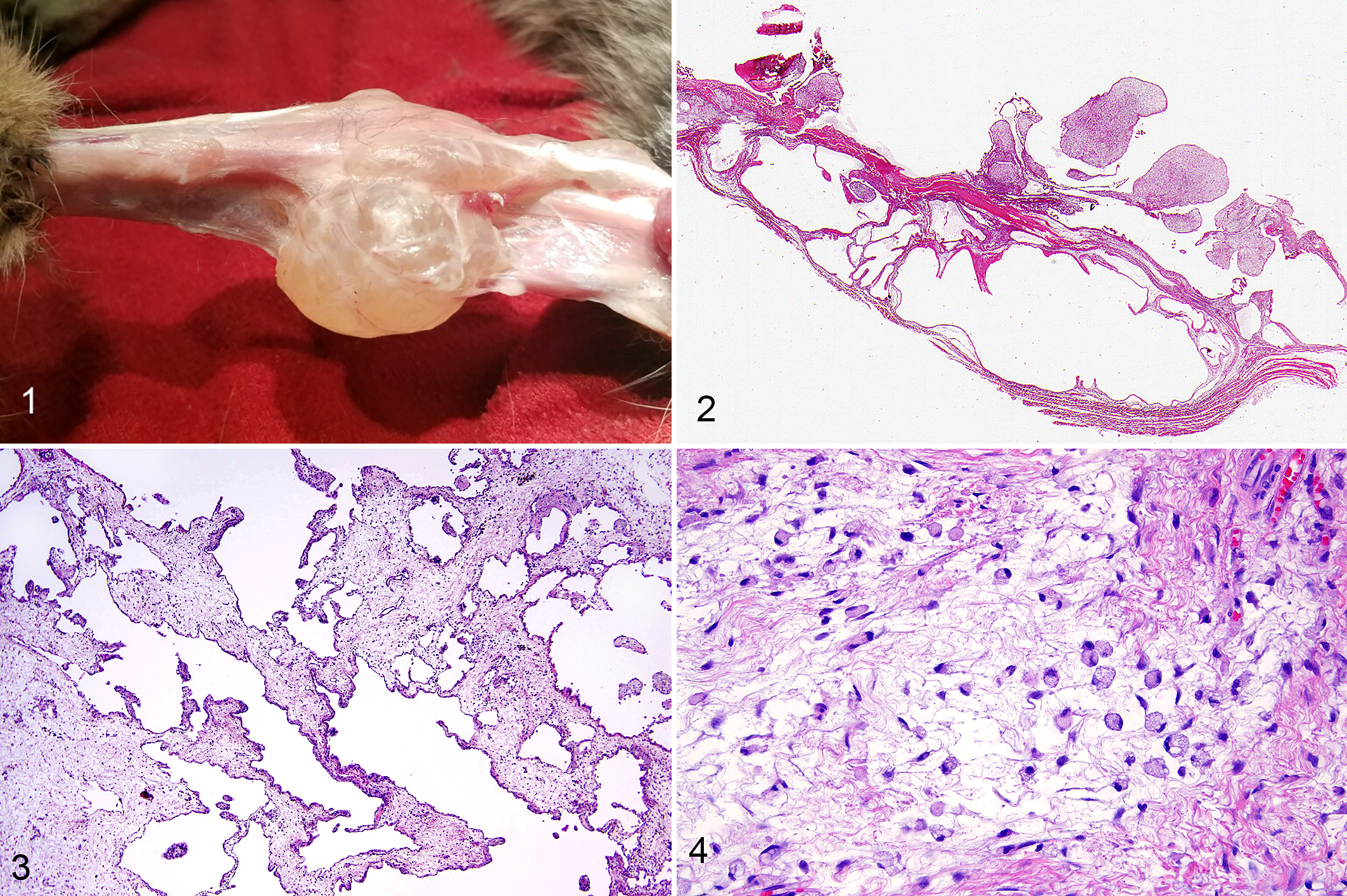
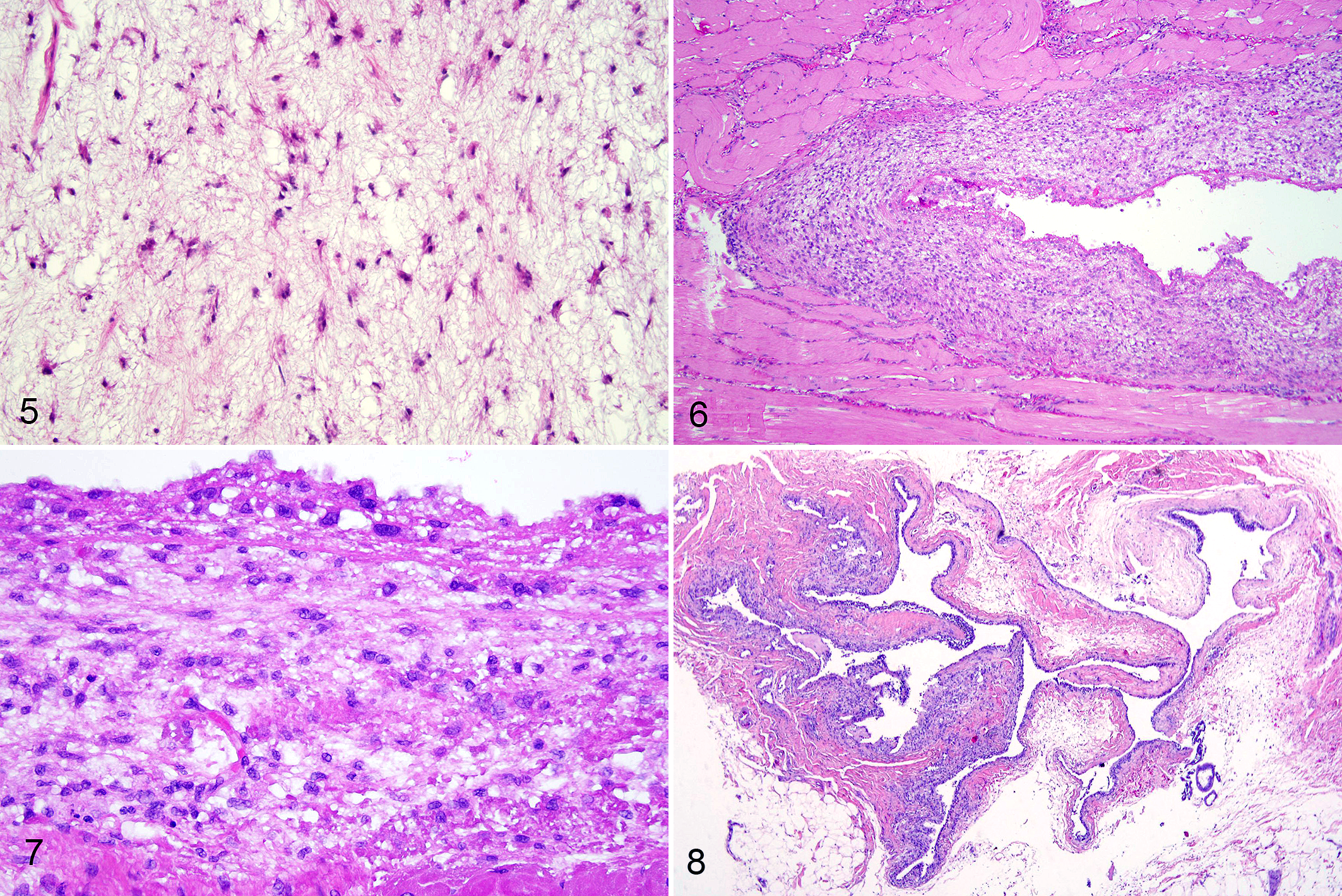
Grossly, the masses consisted of cystic or soft nodules (Fig. 1). Fluid aspirated from the lesions was clear and viscous, resembling synovial fluid. Cytology of the fluid was of low cellularity with only scattered macrophages. Microscopically, the masses consisted of cysts lined by a layer of cells resembling synovium (3 cats), nodular to irregular populations of stellate cells within a myxomatous matrix (2 cats), or a combination of both (11 cats; Figs. 2, 3). There were also foamy macrophages within the myxomatous matrix, presumably in response to the excess extracellular matrix (Fig. 4). Of the 5 whole-limb samples (3 amputations and 2 necropsies), 4 contained both patterns. The stellate cells as well as those lining the cysts had small hyperchromatic nuclei with minimal anisokaryosis, rare to zero mitoses, and no features of malignancy (Fig. 5). In some areas there were findings suggestive of transformation from a cyst to a more solid mass in which the cyst lining became thicker with more layers of synoviocyte-like cells (Figs. 6, 7). Of the 4 cats with joints other than the elbow affected, one had only solid myxomatous nodules (case 15, stifle) and one had only cysts (case 16, tarsus; Fig. 8). Thirteen cases had tissue available for immunohistochemistry. All 13 were uniformly positive for vimentin and had scattered cells positive for IBA-1 and CD18. The morphology of the IBA-1 and CD18 positive cells resembled foamy macrophages.
Synovial cysts and myxomas, cat.
Synovial cysts and myxomas, cat.
The membrane that lines synovial joints is composed of 2 cell types. Type A synoviocytes are phagocytic cells of macrophage or histiocyte origin. Macrophage markers such as CD18 12 and IBA-1 8 can be used to identify type A synoviocytes. Type B synoviocytes are mesenchymal cells that produce synovial fluid. There are no specific markers for type B synoviocytes or for tumors that may arise from them. 11 However, the amount of viscous fluid and the myxomatous nature of the synovial myxomas in dogs and cats suggest that these tumors are of type B synoviocyte origin.
Compared with synovial myxomas in dogs, which are most common in the stifle, this similar lesion in cats is more common in the elbow. The elbow is a joint with very little intraarticular space, which may explain why cystic herniations of synovium and the myxomatous tumor nodules in cats are more commonly surrounding the joint rather than within it. Microscopically, the synovial myxomas in dogs consist of round nodules, while the feline lesion contains more fluid-filled cysts lined by synoviocyte-like cells and solid myxomatous areas that are more irregularly shaped. The reason for the difference in shape of the solid areas between cats and dogs is unknown. The tumor in both dogs and cats is locally infiltrative and slow-growing. None of the cats in this study had any evidence of metastasis, and no deaths were attributed to the tumors. This is similar to the behavior in dogs; however, metastasis to local lymph nodes has been seen in rare cases of canine synovial myxoma (Brian Murphy, personal communication). Since metastasis is the hallmark of malignancy, the myxomatous synovial tumor in dogs is more appropriately termed synovial myxosarcoma. All canine synovial myxomatous tumors should be considered a low-grade malignancy (synovial myxosarcoma), since they are locally invasive but rarely metastasize. Synovial sarcoma is a misnomer for a human tumor that can be biphasic and cytokeratin-positive but is definitively identified by a chromosomal translocation. In humans, it occurs outside of joints and in distant sites, such as pleura, kidney, and mediastinum. Although the cell of origin of this human tumor is unknown, it is not of synoviocyte origin. No tumor of synoviocyte origin has been identified in humans. 3
Of the 12 cats that had evaluation of their joints (radiographically or by orthopedic exam), 11 had bilateral DJD. The synovial cysts and myxomas were all unilateral. The relationship between DJD and the development of these lesions is unknown. One possibility is that increased intraarticular pressure in affected joints results in herniation of synovium, which forms extraarticular synovial cysts. The type B synoviocytes within these cysts could then undergo neoplastic transformation into myxoma. In humans, juxta-articular myxomas are associated with DJD and are theorized to arise from synovial cysts. 1 This would explain why some cats had only cysts and others had both cysts and solid myxoma nodules. Another explanation for the absence of both cystic and solid areas in some cats is sampling error. Thin-walled cysts and myxomatous tumors are both difficult to biopsy and this may result in samples that are not representative of the entire lesion. Of the 5 whole-limb samples (3 amputations and 2 necropsies), 4 contained both patterns, suggesting that biopsy samples containing only one pattern may not represent the entire lesion. The one case diagnosed at necropsy that consisted of only cysts was in the tarsal joint.
Synovial cysts without a neoplastic component have been reported in 10 elderly cats, 8 of which affected the elbow joint. 7,9,13 –16 The lesions were identified as cystic by ultrasound, 7,9,16 arthrogram, 9,14 computed tomography, 9 and/or histopathology. 7,13 –15 Arthrogram showed communication of the cysts with elbow joint. 9 The microscopic findings are similar to the cystic components of the cats in this study. In all but one case, 13 the cysts occurred in joints with DJD, but the DJD was bilateral in all cases examined. 7,9,14 –16 Surgical excision did not improve the lameness and 8/10 surgically excised lesions recurred. 7,9,13 –16 These lesions typically began or were most severe on the medial side of the elbow. 9,13,14,16 Interestingly, a review of DJD in the elbow of 22 cats found the medial side of the joint was more severely affected than the lateral side. 4 In retrospect, some of the previously reported synovial cysts may have been a combination of cysts and synovial myxoma. Only one case was treated by amputation (digit), and the published histopathologic image included solid areas as well as cystic areas. 7 Clinically, the consistency of the cysts was described as a combination of fluctuant and firm, 16 and in the arthrograms, some of the “cysts” did not fill with contrast material. 9
In summary, cystic and myxomatous lesions occur unilaterally in the elbow of older cats with preexisting, usually bilateral DJD. The cysts and solid proliferations (myxomas) often occur concurrently and may represent a continuum from DJD with synovial herniation and periarticular cysts to myxoma. The lesions slowly increase in size but otherwise have a good prognosis.
Footnotes
Editor’s Note
Dr Craig, an Associate Editor with the journal, was not involved in the editorial review or decision to publish this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.