
Abstract
Hepatic lipidosis is commonly diagnosed in pet bearded dragons (Pogona vitticeps). However, there are no studies detailing the histological features of hepatic lipid changes in this species. This study describes the microscopic features of lipid change and details an associated scoring system. Histologic hepatic sections were retrospectively evaluated from 252 bearded dragons submitted for necropsy. Pathologic assessment was used to develop a grading scheme with 2 qualitative, 1 quantitative, and 6 semi-quantitative microscopic parameters, which were refined based on variability. The final grading system developed for diffuse and panlobular lipid accumulation included 2 semi-quantitative and 1 quantitative categories: percentage of hepatocellular vacuolation, fibrosis, and hepatocellular swelling, respectively. Hepatocellular swelling was indirectly quantified by counting the number of nuclei per unit area. There was a strong positive correlation (P < .001) between the percentage of hepatocellular vacuolation and lipid content, a strong negative correlation (P < .001) between nuclear count and lipid content, and a moderate correlation (P < .001) between fibrosis and lipid content. Each category was given a numerical value ranging from 0 to 4, with the sum of each representing the final grade. Cutoff values stratified microscopic changes into mild (final grade 1–4), moderate (5–7), and severe (≥8). There was strong interrater agreement for assessment of vacuolization, fibrosis, and severity classification and moderate for hepatocellular swelling. This study documents the features of hepatic lipid changes in bearded dragons. Although a cutoff to differentiate pathologic from nonpathologic lipid accumulation could not be estimated, the proposed grading scheme can be used to inform future studies.
Hepatic lipidosis, also known as fatty liver disease or steatosis, is a condition affecting several reptilian species. This disease is particularly common in bearded dragons (Pogona vitticeps), one of the most popular pet reptiles worldwide. 30 The basis of this condition involves excess lipid accumulation, mainly triacylglycerols, within hepatocytes, resulting in impaired cellular function, ultimately leading to dyslipidemia, liver failure, and death.3,8,10,11,32
Livers with hepatic lipidosis may grossly appear tan to yellow with rounded margins, have a friable and greasy consistency, and float when placed in formalin.3,7 Routine processing of these tissues for development of hematoxylin and eosin (H&E) slides uses lipid solvents, which wash out lipids leaving optically empty vacuolations. 35 These empty vacuoles, with sharp cytoplasmic rims, are the basis for the microscopic assessment of hepatic lipid content. 35 In reptiles, microvesicular or macrovesicular lipid can cause hepatocellular enlargement and large vacuoles can displace hepatocellular nuclei.8,26 However, macrovesicular lipidosis alone, as described in humans, 24 is not reported in reptiles. 8 It should be noted that all hepatic vacuoles visualized on microscopic examination are not necessarily lipid as some may contain water, glycogen, and other nonlipid material. 7 Some visual features, such as the presence of vacuolar pigment or poorly defined vacuolar margins (as with glycogen), can help distinguish the nature of the vacuoles. Special stains, such as periodic acid-Schiff (PAS) before and after diastase treatment, can be used to confirm glycogen accumulation. 13 Additional lesions that are reported to be associated with hepatic lipidosis include inflammation and fibrosis; however, progression to cirrhosis is uncommon in reptiles.3,10,15,33 Hepatic fibrosis has been reported in reptilian species secondary to chronic injury, infection, and neoplasia, but its correlation with hepatic lipidosis has not been investigated.9,12,16,18
While histopathology of the liver remains the gold standard for diagnosis of this disease, 33 no consensus has been reached regarding the amount of hepatic fat constituting a diagnosis of lipidosis. Current recommendations in reptiles warrant a microscopic diagnosis of hepatic lipidosis when the cytoplasm is vacuolated with lipid in more than 20% of the parenchyma; however, this threshold is not based on primary clinical or physiological assessments.8,25 It has been proposed from subjective observation that hepatic lipidosis should be considered moderate when at least 80% of the parenchyma is affected and marked when 100% of the parenchyma is affected.8,25 In addition, guidelines on interpretation of physiological hepatic lipid content in regard to species, season, and sex are poorly defined. 21 In bearded dragons, a certain degree of hepatic vacuolation may be physiologic, and it is unclear what amount is considered pathologic.8,31 A few reports suggest that the liver of lizards should only carry approximately 5% of the total body lipids.1,4
Due to the high frequency of hepatic lipidosis in captive bearded dragons, and the limited number of validated diagnostic modalities, the goal of this study was to describe the histological features of hepatic lipid accumulation in this species and to develop a microscopic grading system to assess the severity of associated changes. Although this study was not devised to establish a cutoff to differentiate hepatic lipidosis as opposed to normal lipid accumulation, the proposed grading system can be used to ground future studies aimed at understanding the pathogenesis of this disease, test novel treatment options, and ultimately develop a standardized diagnosis of hepatic lipidosis.
Materials and Methods
Case Retrieval
Necropsy cases of bearded dragons (P. vitticeps) submitted between 1998 and 2018 at the Animal Health Laboratory (AHL, University of Guelph, ON, CA) and the Zoo/Exotic Pathology Service (Sacramento, CA, USA) were retrieved. Biopsy cases were excluded. Inclusion criteria required that each case had a diagnosis of hepatic lipidosis on the final pathology report and availability of histology slides with hepatic sections for review. In addition, all necropsy cases with available slides for review, and without a diagnosis of hepatic lipidosis, were collected from the AHL to be used as negative controls for development of the grading scheme. The diagnosis of hepatic lipidosis relied on each case’s pathologist and was not harmonized for this study due to its retrospective nature and lack of a broadly adopted diagnostic definition of hepatic lipidosis. However, the initial diagnosis was not used to inform the grading scheme. Cases with systemic and/or other primary hepatic pathologies were not excluded, as hepatic lipidosis is often concurrent with other diseases.
A total of 197 cases diagnosed with hepatic lipidosis and 55 cases without hepatic lipidosis (total, 252; 113 females, 70 males, 14 unknown) met the inclusion criteria and were used to optimize the grading system.
Scoring Scheme Development
Initially, H&E hepatic sections from 50 of the 252 cases were evaluated by 2 members of the research team (L.S. and T.B.) in a nonblinded approach at a multiheaded microscope to develop a scoring scheme. Cases were selected to represent a wide array of severity associated with lipid accumulation, as assessed by the original case pathologist. This initial screening was carried out to identify morphological characteristics that showed variation between mild and more severe lesions, and would therefore prove useful for developing a grading system.
The initial parameters for the development of the grading scheme included 2 qualitative, 1 quantitative, and 6 semi-quantitative categories as detailed below:
1. Subgross distribution of lipid vacuolation (qualitative). For cases with a score other than 0 in the assessment of lipid vacuolation (see parameter 3 below), lipid distribution was characterized as focal, multifocal, or diffuse, based on the available hepatic sections.
2. Lobular distribution of lipid vacuolation (qualitative). For cases with a score other than 0 in the assessment of lipid vacuolation (see parameter 3 below), the lobular distribution of lipid was characterized as centrilobular, mid-zonal, peri-portal, panlobular, or random.
3. Percentage of hepatocellular vacuolation (semi-quantitative). This change was scored 0–4 based on the percentage of the cytoplasm that is filled with lipid in the hepatocytes (0 was 0%–5%, 1 was >5%–25%, 2 was >25%–50%, 3 was >50%–75%, 4 was >75%), as estimated using 400× magnification (field of view [FOV] is described below).
4. Hepatocellular swelling (quantitative). This parameter was included to assess the degree of hepatocellular swelling associated with cytoplasmic lipid accumulation. This parameter was included to contextualize other assessments of lipid accumulation on a per cell basis and link it with hepatic cytopathology. As cellular size was difficult to objectively identify, due to poorly defined hepatocellular boundaries in more severe cases, cytoplasmic swelling was assessed by counting the number of hepatocellular nuclei per area unit. It was hypothesized that more severe degrees of cytoplasmic swelling would be associated with fewer nuclei on section.
To implement this, the average number of nuclei in 10 high-power fields was counted using a 40× objective (400× magnification) on a microscope (Leitz Laborlux K) equipped with an INFINITY2 camera (Lumenera 1.4 megapixel Infinity 2-1) and Infinity analyze software (Lumenera v 6.5.6). Mid-zonal areas were chosen for evaluation while avoiding portal and centrilobular spaces. Those nuclei that were within sinusoids (eg, endothelial cells, red blood cells), associated with pigmented cells (melanomacrophages), or cut by the FOV were not counted.
Counting was done manually using screen-projected images for each field (multipoint tool in ImageJ version 1.53a). The microscope was calibrated with a stage ruler (AmScope MRo95), and the resulting FOV of the camera and microscope was determined using a stage micrometer to be approximately 0.02 mm2. The final output for this parameter was the average number of nuclei in ten 0.02-mm2 FOVs or 0.2-mm2 FOVs. For microscopes with a 2.37-mm2 FOV (most common), the number of nuclei defining the severity categories should be divided by 11.85 to approximate a 0.2-mm2 FOV. Cutoffs for the average number of nuclei were established as follows: 0 (no hepatocellular swelling), average ≥ 30 nuclei; 2 (moderate), average = 29–16 nuclei; and 4 (severe), average ≤15 nuclei. Hepatocellular swelling was scored in increments of 2 units to increase the weight of this category in the overall grade, as it appeared to be the most obvious marker of cellular damage caused by lipid accumulation, and it is known to have significant impact on cell function and health in other species.19,24
5. Fibrosis (semi-quantitative). This change was scored 0–4 based on the amount of fibrosis in the histologic section of the liver: 0 was <10%, 1 was >10%–25%, 2 was >25%–50%, 3 was >50%–75%, and 4 was >75%, with no further modifier for lobular distribution. Focal areas of fibrosis associated with granulomatous inflammation, areas of necrosis or hemorrhage, or neoplastic lesions were not included. Similarly, fibrosis associated with clear evidence of cholangitis was not included.
6. Inflammation associated with lipid (semi-quantitative). This change was scored 0–3 based on granulomatous inflammation directly associated with extracellular release of lipid, as seen in relation to lipogranulomas or inflammation surrounding cholesterol clefts (0 was 0%–5% of the histologic section of liver affected by inflammation, 1 was >5%–25%, 2 was >25%–50%, 3 was >50%). This type of inflammation was differentiated from extramedullary hematopoiesis and/or granulopoiesis due to the lack of precursor cells and clear association with fat. Heterophilic granulomas were not included in this category, as these have a likely bacterial origin. 7
7. Inflammatory cells associated with fibrosis and portal tracts (semi-quantitative). This change was scored 0–4 based on the presence of mononuclear cells associated with fibrosis (described above) in the histologic section of the liver: 0 was <5% of the fibrosis affected by inflammation, 1 was 5%–10%, 2 was >10%–25%, 3 was >25%–50%, and 4 was >50%. Heterophilic granulomas were not included in this category.
8. Presence of melanomacrophages (semi-quantitative). In reptiles, hyperplasia of melanomacrophagic centers is observed as a nonspecific response to a multitude of diseases. 7 Therefore, this category was included and was scored 0–4 based on the average percentage of melanomacrophages occupying the histologic section evaluated (based on histologic section of the liver: 0 was <15%, 1 was 15%–25%, 2 was >25%–50%, 3 was >50%–75%, 4 was >75%).
9. Presence of necrosis/apoptosis [coagulative or single cell] (semi-quantitative). This change was scored 0–4 based on the amount of hepatocyte necrosis or apoptosis, which was not secondary to other apparent causes (based on histologic section of the liver: 0 was 0%, 1 was 1%–5%, 2 was >5%–25%, 3 was >25%–50%, 4 was >50%).
Refinement of the Initial Grading Scheme
Following a 3-month washout period and blinding to the pathology reports, all cases (n = 252) were manually randomized by covering the label and mixing them, and graded using all 9 parameters by 1 investigator (T.B.) within 1 week to avoid diagnostic drift. 14 Initial assessment of the 9 histological features showed that only 2 semi-quantitative parameters (percentage of hepatocellular vacuolation and fibrosis) and 1 quantitative parameter (hepatocellular swelling) could be retained in the grading scheme, due to low discriminating power of the other parameters between case severities (see “Results” section).
Correlation Analysis
Correlation between the amount of lipid and these 3 parameters was further evaluated on a subset of 34 cases, which were randomly selected using a random number generator, and blocked for each severity classification of no lipid, mild, moderate, and severe (as assessed by the grading system mentioned above). The lipid content was assessed by image analysis from 3 areas of hepatic sections captured at 400×, making sure to avoid areas of fibrosis and centrilobular veins, and using the same microscope and imaging system described above. Using ImageJ 29 software version 1.53a, the background was subtracted and white balanced, and then images were converted to grayscale, prior to binarizing with the same threshold for all images. Subsequently, the percentage of white area was measured to determine the percentage of lipid in hepatocytes (Fig. 1). For each case, the percentage of lipid was averaged from the 3 pictures.
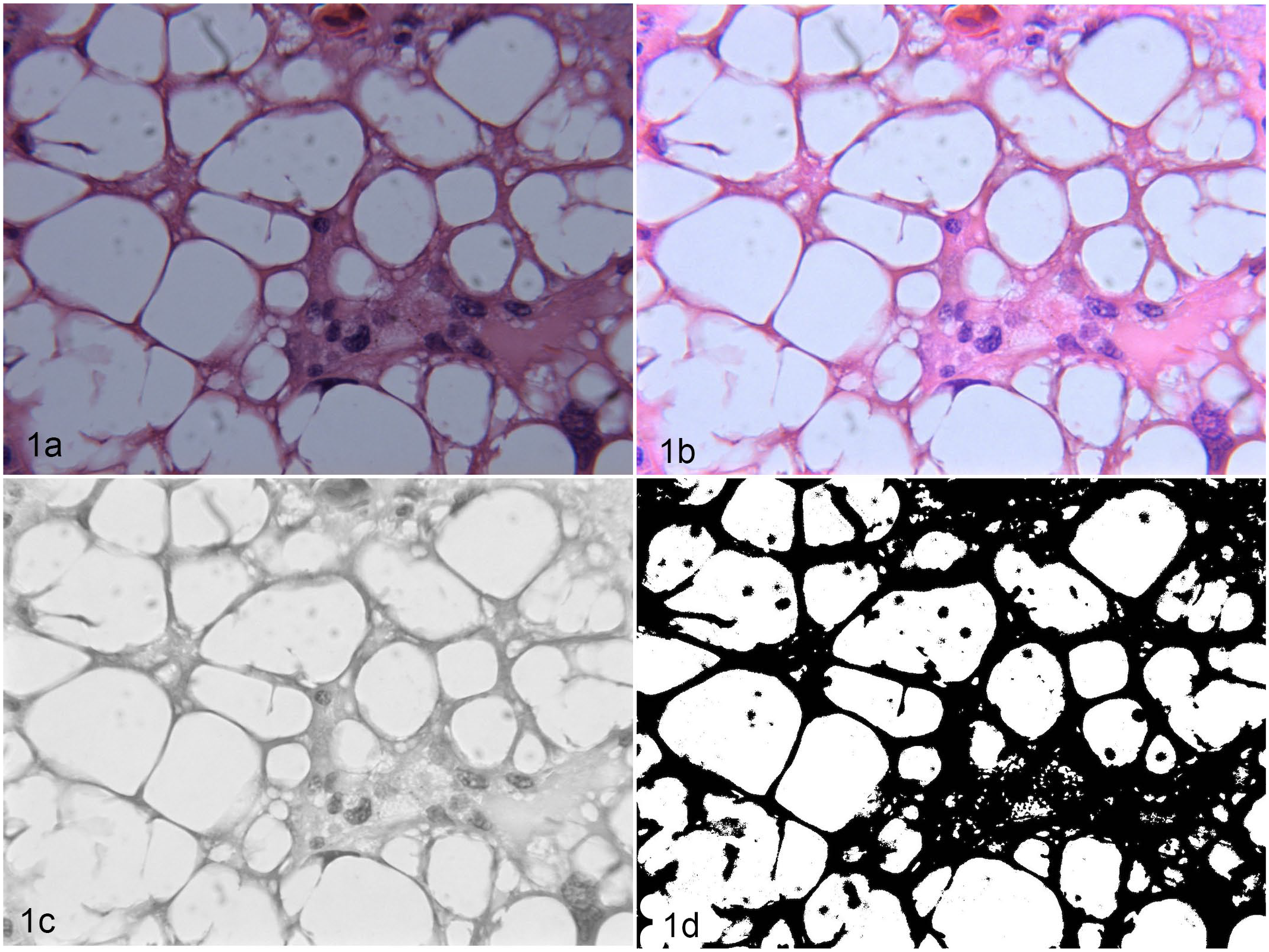
Liver, bearded dragon (Pogona vitticeps). Lipid vacuoles and cellular swelling. Hematoxylin and eosin. The figures show the process of digital image analysis for lipid percentage in the hepatocytes. Using ImageJ software, the background was subtracted and white balanced (b) from the original image (a) and then images were converted to grayscale (c), prior to binarizing with the same threshold for all images (d). The percentage area covered by white was measured as an estimation of the lipid content in liver sections.
A Spearman’s correlation coefficient was used to determine the relationship between the quantitative percentage of lipid, as assessed by ImageJ, and the grading categories of percentage of hepatocellular vacuolation, hepatocellular swelling, fibrosis, as well as the final grade and severity classification.
Cutoff Development for Severity Classification
For each case, the final grade was calculated as the sum of the 3 final parameters (2 semi-quantitative [percentage of hepatocellular vacuolation and fibrosis] and 1 quantitative [hepatocellular swelling]) and ranged from 0 to 12. Following grading, cutoffs for severity classification were subjectively created by dividing the continuum of lesions into equal increments (no lipid, 0; mild, 1–4; moderate, 5–7; severe, 8–12). This was done in an attempt to provide a clinically relevant reporting system.
Evaluation of Interobserver Agreement
The same subset of 34 cases described above was re-graded within 3 days by a second investigator (L.S.) after an 8-month washout period and blinding. To standardize the area of nuclei counts, the FOV from the digital images was converted to 0.02 mm2 for comparison between observers. 23 Interobserver correlation was subsequently calculated using Cohen’s kappa statistics with quadratic weights for the 3 categories, final grade, and severity classification. A kappa value of 0.80–0.90 was considered to have a strong level of agreement, a value of 0.60–0.79 to have a moderate level of agreement, and a value of less than 0.40 to have a weak level of agreement. 22
Results
Scoring Scheme Development
Evaluation of the qualitative parameters, subgross distribution of lipid vacuolation, and lobular distribution of lipid vacuolation indicated that most histologic sections, 246/252 (97.6%), had a panlobular and diffuse vacuolation except for 1 (0.4%) of 252 cases that had centrilobular distribution and 5 (2%) of 252 cases that had multifocal distribution. Due to the low variability within the cohort, these qualitative parameters were removed from the grading system and were considered unnecessary to enable the grading scheme.
In evaluation of the percentage of hepatocellular vacuolation, 239 (94.8%) of 252 cases had some degree of lipid accumulation. Cases with less than 5% of cytoplasm occupied by lipid vacuoles in hepatocytes were not considered to have accumulation and were given a grade 0, 33 (13.1%) of 252 cases. Cases with >5%–25% of cytoplasm occupied by lipid vacuoles in hepatocytes, grade 1, were 26 (10.3%) of 252. Cases with >25%–50% of cytoplasm occupied by lipid vacuoles in hepatocytes, grade 2, were 24 (9.5%) of 252. Cases with >50%–75% of cytoplasm occupied by lipid vacuoles in hepatocytes, grade 3, were 67 (26.6%) of 252. Finally, cases displaying lipid vacuoles taking up >75% of the cytoplasm (grade 4) were the most common (102/252, 40.5%). Lipid vacuolation showed a continuum, ranging from single or few large vacuoles, to multiple, medium to small vacuoles expanding the cytoplasm, even in the same section. Therefore, the size of vacuole was not considered to be a significant feature to include in the grading scheme. Representative pictures of the percentage of hepatocellular vacuolation, for all degrees of severity, are presented in Figs. 2–5.
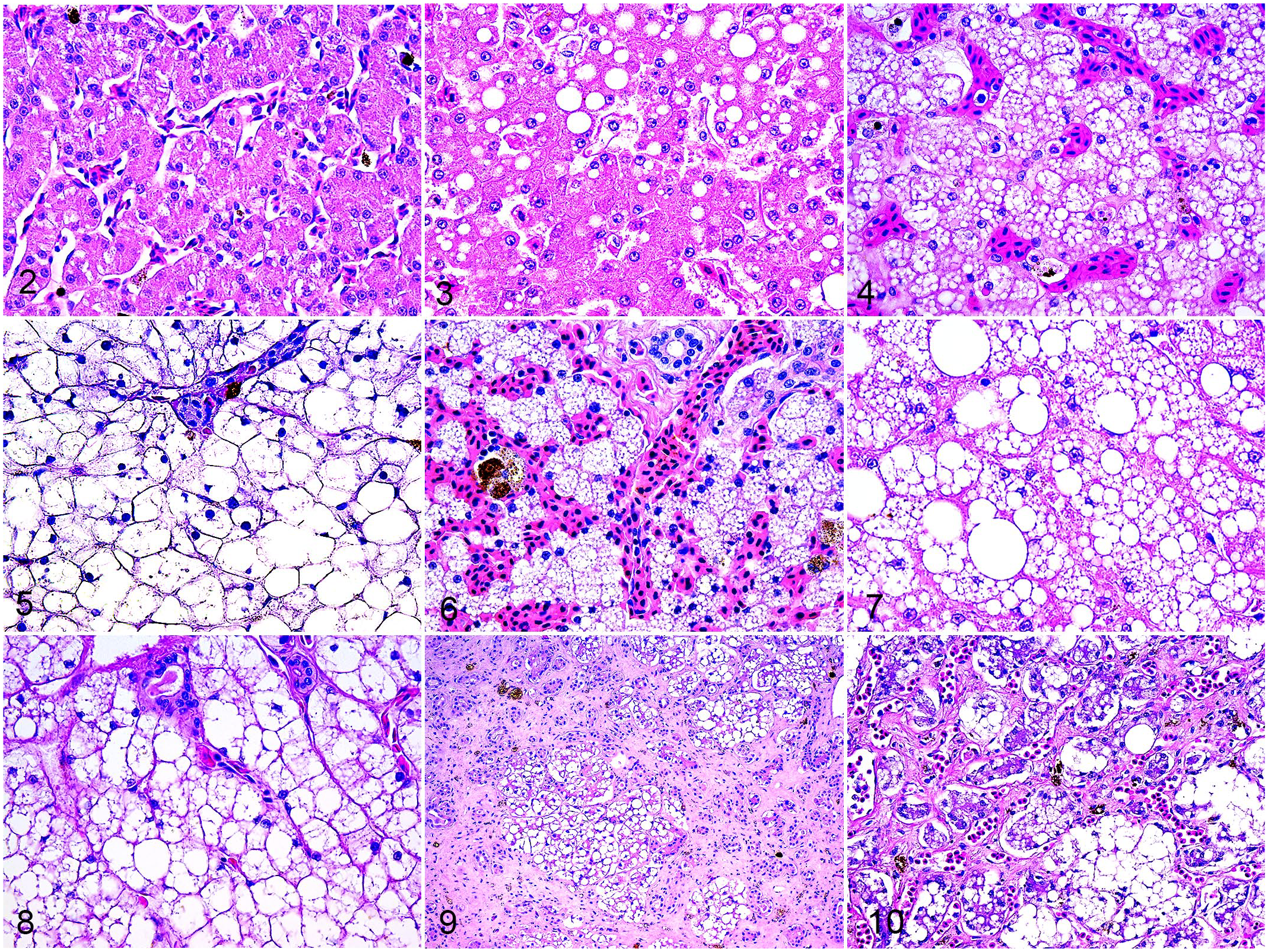
Bearded dragons (Pogona vitticeps), hematoxylin and eosin. Microscopic images representative of the morphological categories used to grade the content of hepatic lipid.
In evaluation of hepatocellular swelling, 154 (61%) of 252 cases had some degree of hepatocellular swelling, with 72 (28.6%) of 252 cases having mild to moderate swelling, grade 2, and 82 (32.5%) of 252 cases having severe swelling. This was only observed in sections that scored grade 3 or higher for the percentage of hepatocellular vacuolation (Supplemental Table S1). The remaining 98 (38.9%) of 252 cases were not considered to have hepatocellular swelling. With increased amounts of lipid, hepatocytes showed moderate to severe swelling, resulting in compression of sinusoids, apparent loss of cellular boundaries, and alteration of the regular arrangement of hepatic cords. As the hepatocytes became swollen, the nuclei became less visible on the plane of section, likely due to displacement or compression by lipid. Representative pictures are presented in Figs. 6–8.
Seventy-five cases (75/252, 30%) presented with hepatic fibrosis, with most cases being sections that scored grade 3 or higher for the percentage of hepatocellular vacuolation (Supplemental Table S1). One hundred seventy-seven (177/252, 70.2%) cases did not have fibrosis, 44 (17.5%) of 252 cases had 10%–25% fibrosis, 19 (7.5%) of 252 cases had >25%–50% fibrosis, 6 (2.4%) of 252 cases had >50%–75% fibrosis, and 6 (2.4%) of 252 cases had >75% fibrosis. Fibrosis was mainly portal, and in the most severe cases it dissected through the entire lobule with wide bridging bands of collagen or increased collagen deposition in the perisinusoidal space (capillarization). Fibrosis was often accompanied by biliary duct hyperplasia (Figs. 9, 10). Fibrosis was not associated with severe inflammation or necrosis. Regenerative nodules were not observed in association with even the most severe instances of fibrosis.
Overall, inflammation associated with lipid was rare and was only identified in 4 (1.6%) of 252 cases. These 4 cases had >5%–25% (grade 1) inflammation associated with extracellular release of lipid. This inflammation had too little variability between grades of hepatocellular vacuolation to be included in the scoring system (Supplemental Table S1). Inflammation associated with lipid was predominantly granulomatous, with occasional lipogranulomas.
Inflammation associated with fibrosis and portal tracts was also rare and only identified in 4x (1.6%) of 252 cases. These 4 cases had >10 to 25% (grade 2) inflammation associated with fibrosis, which was characterized by accumulation of mononuclear cells within strands of fibrous tissue. Both inflammation categories were removed from the grading system due to their low frequency and mild severity.
Melanomacrophages occupied <15% of the histologic section in most cases (186/252, 73.8%) and were scored as 0. Forty-eight (48/252, 19%) cases had melanomacrophages occupying 15%–25% of the histologic section (grade 1), 17 (6.7%) of 252 cases occupying >25%–50% of the histologic section (grade 2), and 1 (0.4%) of 252 cases occupying >50%–75% of the histologic section (grade 3). No cases had melanomacrophages occupying >75% of the histologic section. The melanomacrophages were present as scattered clusters of cells within sinusoids and portal spaces. There was no clear variation in the amount of melanomacrophages, in relation to the amount of lipid, as the majority of cases with increased melanomacrophages (62/66 93.9%) were grade 1 (15%–25% of the histologic section), with grades ranging from 0 to 4 for percentage of hepatocellular vacuolation (Supplemental Table S1); therefore, this category was removed from the final grade.
Single cell necrosis/apoptosis was not a common feature of the evaluated cases (5/252, 2.0%). Of the 5 cases with single cell necrosis/apoptosis, 4 cases (4/252, 1.6%) were considered to have 1%–5% necrosis and 1 case (1/252, 0.4%) was considered to have >5%–25% necrosis. When present, the necrosis was not associated with hepatocyte lipid changes as the small amounts of necrosis noted did not increase with progressive vacuolization and hepatocellular swelling (Supplemental Table S1). Therefore, this category was removed from the final grade.
Based on the assessment of the initial histologic parameters, only the following were carried forward in the final grading scheme for diffuse and panlobular lipid changes: percentage of hepatocellular vacuolation, hepatocellular swelling, and fibrosis (Table 1).
Histological grading system and severity classification for changes associated with diffuse and panlobular hepatic lipid accumulation in bearded dragons (Pogona vitticeps).
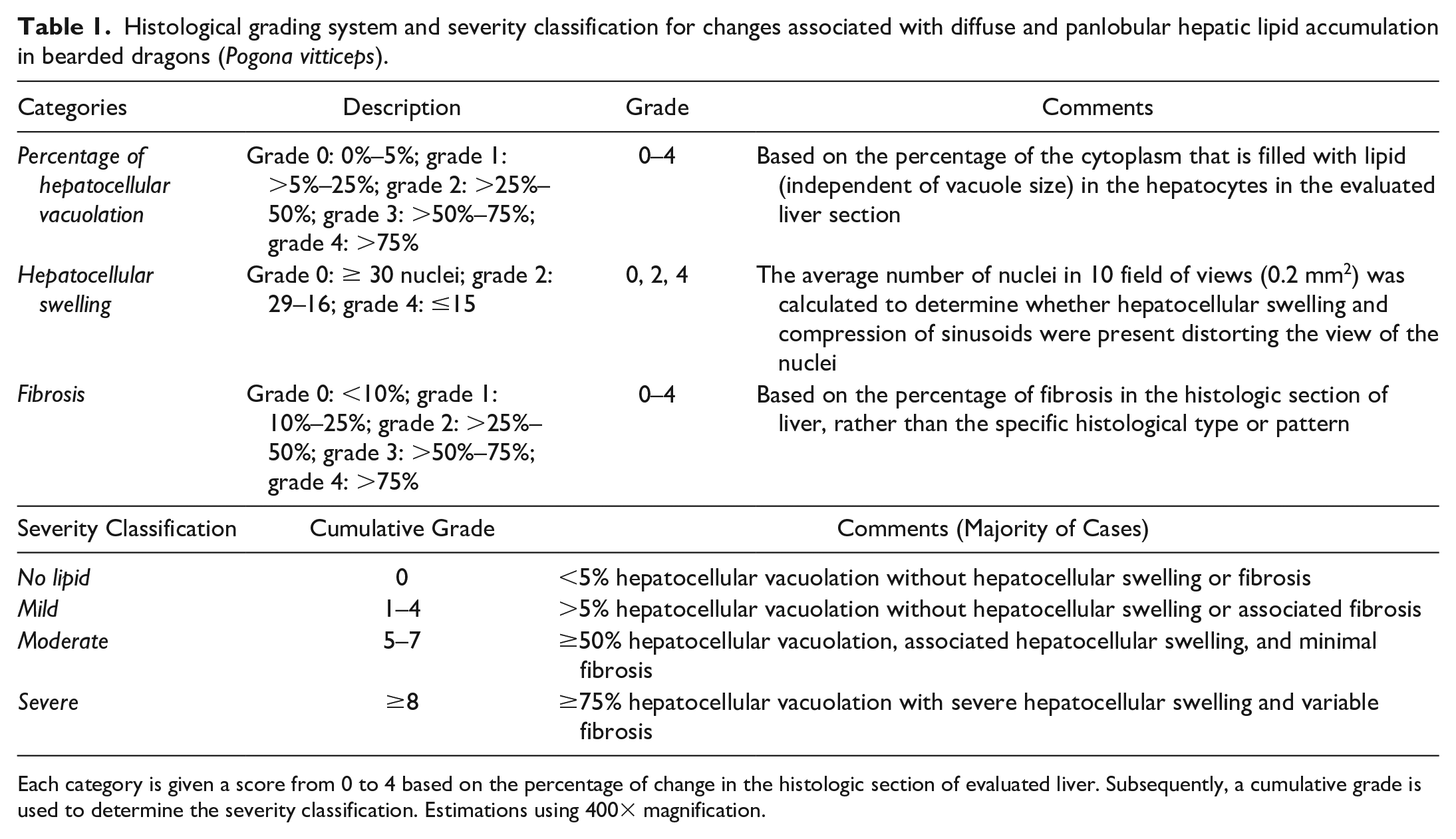
Each category is given a score from 0 to 4 based on the percentage of change in the histologic section of evaluated liver. Subsequently, a cumulative grade is used to determine the severity classification. Estimations using 400× magnification.
Correlation Analysis
Digital analysis, conducted to assess the amount of lipid content in hepatic sections, was completed in a subset of 34 cases. A Spearman’s correlation analysis determined that in comparison with the results of image analysis, there was a strong positive correlation (rho = 0.878, P < .001) between the percentage of hepatocellular vacuolation and percentage of lipid, a strong negative correlation (rho = −0.894, P < .001) between hepatocellular swelling and percentage of lipid (indicating that as lipid increased, the number of visible nuclei decreased per area unit), and a moderate correlation (rho = 0.55, P < .001) between fibrosis and percentage of lipid. Finally, a strong correlation (rho = 0.88, P < .001) was seen between the amount of lipid and the final grade as well as severity class (rho = 0.84, P < .001) (Fig. 11).
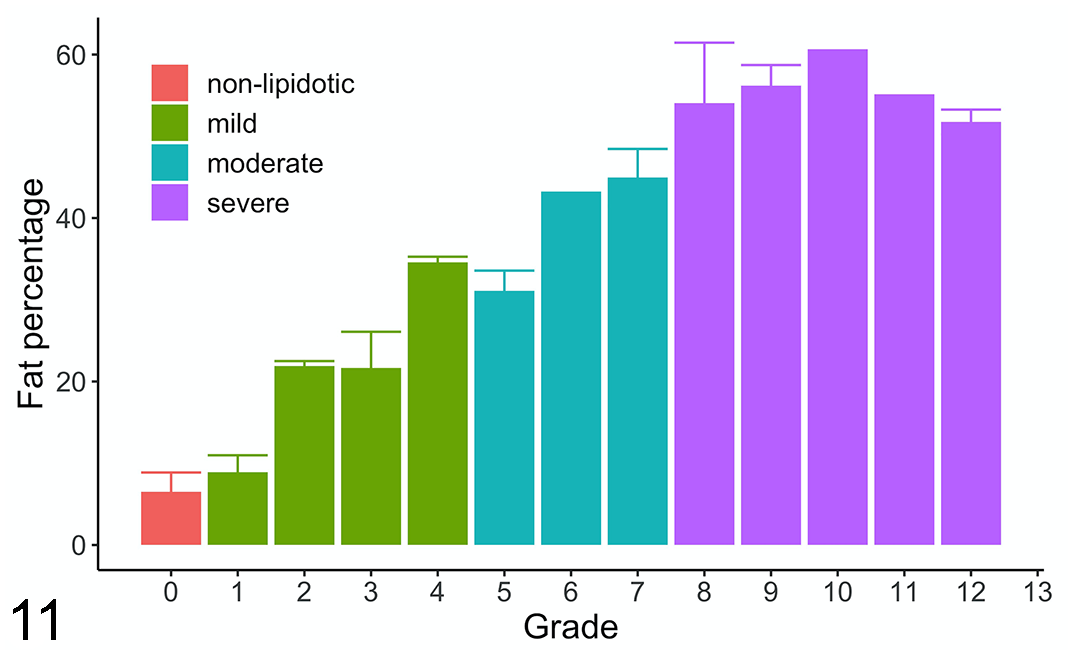
Bar graph of mean ± SEM of percentage lipid area in hepatocytes over hepatic lipid grades and classification in bearded dragon liver sections from digital analysis in a subset of cases (n = 34). An increasing slope of lipid percentage is demonstrated as the grade increases and plateaus in the severe group. There is a strong Spearman’s correlation (rho = 0.88, P < .001) between the percentage of lipid area and grades. Each bar represents the average lipid percent for the cases evaluated in that grade. Colors of the bars represent the different categories of no lipid (red), mild (green), moderate (teal), and severe (purple). The single lines represent error bars (SEM).
Cutoff Development for Severity Classification
Cutoffs for mild, moderate, and severe histologic changes (ie, severity classification) were based on equal incremental increase of the final grades. Figure 12 shows the distribution of the score of each of the 3 histologic parameters, based on severity classification. Overall, as the severity classification increased, there was progressive increase in vacuolization, hepatocellular swelling, and fibrosis.
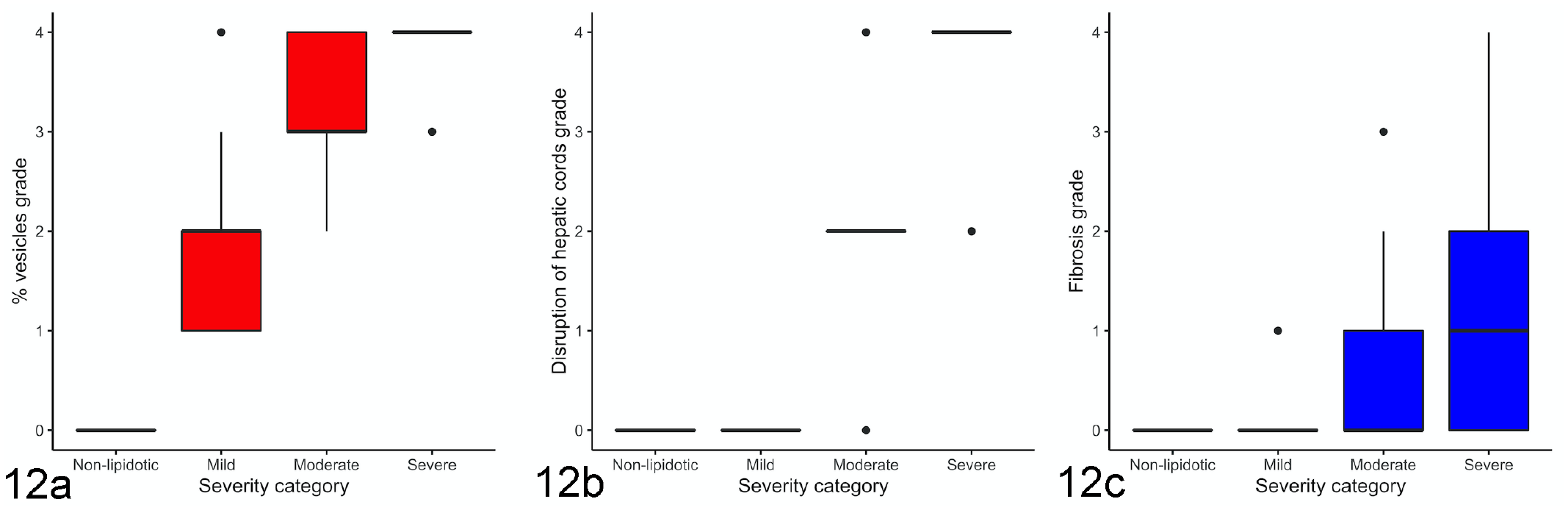
Box plots showing the distribution of the scores of the histologic parameters percentage of hepatocellular vacuolation (a), hepatocellular swelling (b), and fibrosis (c) based on the grade and classification system of hepatic lipid in bearded dragons (Pogona vitticeps). Overall, as the classification tier increases, there is a progressive increase in vacuolization, hepatocellular swelling, and fibrosis.
No lipid, mild, moderate, and severe classifications were based on final grades of 0, 1–4, 5–7, and ≥8, respectively. Sixty-three (63/252, 25%) cases were classified as mild. In the majority of mild cases (55/63, 87.3%), lipid vacuoles occupied >5%–75% of the hepatocyte cytoplasm. Fewer cases, including 3 (4.8%) of 63 cases, had >75% lipid vacuoles in hepatocytes. Five (7.9%) of 62 cases had mild fibrosis in the sections, but without hepatocellular swelling. No other lesions were observed. This class represented cases with the presence of lipid in the hepatocyte, but without hepatocellular swelling.
Seventy-three (73/252, 29%) cases were classified as moderate. Almost all of the moderate cases (72/73, 98.6%) had lipid vacuoles in at least 50% of the hepatocytes’ cytoplasm, and only 1 (1.4%) of 73 had less than 50% cytoplasmic lipid. Moderate hepatocellular swelling was present in all but 6 (8.2%) of 73 cases and fibrosis, when present, occupied up to 25% of the section, with 3 (4.1%) of 73 cases affected by >25% fibrosis in the section. The moderate class included cases with lipid accumulation that resulted in hepatocellular swelling.
Eighty-three (83/252, 32.9%) cases were classified as severe. The majority of cases (57/83, 68.7%) in the severe category included cases in which lipid vacuoles occupied >75% of the hepatocellular cytoplasm, had severe hepatocellular swelling, and variable amounts of fibrosis (0%–50% of the section). Severe fibrosis was only seen in this group. Ten (12%) of 83 cases had a lower percentage (>25%–50%) of lipid vacuoles in the hepatocytes, 5 (6%) of 83 cases had only moderate hepatocellular swelling, and 11 (13.2%) of 83 cases had moderate fibrosis. Overall, the severe class had a greater degree of hepatocellular swelling and fibrosis. A grade of 8 was chosen as the lower boundary of the severe class, as the maximum scores for vacuolization and swelling would result in a grade of 8, indicating this would be the most severe change of hepatocytes without fibrosis.
Digital image analysis was used to further describe the amount of lipid present in a quantitative manner in the proposed grading scheme. Digital analysis for these cases (Fig. 3) demonstrated an increasing slope of lipid percentage as the grade increased, which plateaued in the severe group. Sections with no obvious vacuoles, given a final grade of 0, had an average of 6% of lipid present. Sections classified as mild had an average of 9% to 34% of lipid present. Sections classified as moderate had an average of 31% to 45% of lipid present. Finally, sections classified as severe had an average of 52% to 61% of lipid present. Cases given a final grade of 8 and above had at least 50% lipid present in the slide.
Evaluation of Interobserver Agreement
Analysis of interrater agreement on features of the histologic categories showed strong agreement for the grading categories of percentage of vacuoles in hepatocytes (kappa value of 0.92, P < .001) and fibrosis (kappa value of 0.89, P < .001) with weighted kappa values. There was moderate agreement for hepatocellular swelling (kappa value of 0.73, P < .001). The interrater agreement on the final grade was moderate (kappa value of 0.66, P < .001), while the interrater agreement for severity classification was strong (kappa value of 0.88, P < .001).
Discussion
Hepatic biopsies and histopathology remain gold standard for the diagnosis of hepatic lipidosis in veterinary medicine.8,28,33,37 Although the most common features of hepatic lipidosis are descriptively reported in pathology reports, there is no concise grading system for this disease in reptiles in general, and bearded dragons in particular.
Of the removed categories, reported features such as melanomacrophages could increase due to other inflammatory or metabolic conditions, and the increase did not correlate with the severity of hepatic lipid changes. Grading and classification of hepatic lipid changes in bearded dragons based on criteria in other animals should be avoided as the characteristics and prevalence of the lesions are different. For example, as lipid vacuoles affect the parenchyma diffusely in bearded dragons, almost all cases would be considered to have significant lipidosis if human guidelines were applied, which evaluate the percentage of parenchyma affected to determine severity. 24
To reduce sampling error in humans, a 2-core biopsy of at least 15 mm in length with at least 15 portal tracts collected with 2 to 3 cm, 16-gauge needles and reviewed by a single pathologist is recommended. 36 Biopsy cases were excluded from evaluation during the development of our grading system due to variation in sample size, reduced number of portal tracts, possibility of sampling error, and to avoid grading nondiffuse processes. However, as the majority of sections contained panlobular and diffuse vacuolization of the hepatocytes, this grading system can be implemented for nontargeted hepatic biopsies. Ideally, additional diagnostics such as imaging or endoscopic evaluation of the liver are pursued prior to biopsy collection to confirm a diffuse process.
The percentage of vacuoles measured in the hepatocytes through the grading system were subjective measures of presumed lipid (white) to cytoplasm (pink) ratio. In a few cases, borders of the vacuoles appeared less crisp and were suspected to be glycogen vacuoles, but PAS stain was not available to confirm. These cases were not excluded and could have added error to the grading.
A strong negative correlation between the percentage of lipid through image analysis and hepatocellular swelling indicated that as lipid accumulated in the hepatocyte, the cells progressively expanded and the visibility of the nuclei decreased. This process has previously been described in reptiles with hepatic lipidosis. 8 To the authors’ knowledge, there are no published guidelines on hepatocyte diameter for bearded dragons. The bearded dragon hepatocyte likely has some capacity to swell due to the physiology of its storage, use, and lipogenesis of lipids. 27 It is also possible that lipid accumulation within a hepatocyte may be physiologically appropriate to the point of cellular swelling, which would be considered pathologic. Cell ballooning, which involves hepatocyte enlargement, is a key difference between steatosis and steatohepatitis in humans. 24 Assessment of wild bearded dragon liver samples during various physiological states would be helpful to determine the acceptable amount of hepatic lipid. Attempts were made by the authors to acquire liver histology slides from wild P vitticeps through the Australian Society for Veterinary Pathology, but samples for this species were not available.
Fibrosis is irreversible and is considered to occur secondary to disease processes, so it is often included in the staging of diseases. It was included in the grading of hepatic lipid changes in bearded dragons as currently there is no distinction between grade and stage of disease, and all reports of reversibility are anecdotal.3,6,8,17,24,33,34 Due to the retrospective nature of this study, a direct correlation between lipid accumulation and fibrosis cannot be made.
Due to lack of clinical data (eg, survival, clinical disease) to stratify our cases, the tiers for no lipid, mild, moderate, and severe hepatic lipid changes were based on equal increments of the final grade to capture increasing amounts of cellular damage in each category. The mild classification generally indicated the presence of lipid in the hepatocyte without structural damage, such as cellular swelling, suggesting this level of hepatic lipid change may be normal for this species or likely was not causing clinical disease. Therefore, the 5 cases of mild fibrosis in this group were likely not related to lipid accumulation. However, no other causes of hepatocellular fibrosis were observed in these cases. The moderate group contained a significant amount of lipid vacuoles in all sections and some degree of hepatocellular swelling with minimal to no fibrosis, possibly indicating reversible damage. Finally, the severe category encompassed cases with significant morphological damage to the hepatocytes and fibrosis. This category included what was suspected to be the consequences of lipid accumulation, mainly fibrosis.
It is expected that the different severity classifications are associated with different likelihoods or severity of clinical signs. However, it would be difficult to correlate clinical signs with histopathologic severity as the majority of chronic cases present with nonspecific clinical signs. 20 In addition, analytes indicating hepatocellular leakage are generally within normal limits because breakdown of hepatocytes does not seem to be a feature of this disease process in bearded dragons. 3 However, triglyceride levels, though nonspecific, have been reported to increase with hepatic lipidosis.8,10,21
Digital image analysis estimated the amount of lipid present in representative histopathologic sections of liver by objectively quantifying the percent area of vacuolation. This approach was strongly correlated with the subjective grading category of percentage of hepatocellular vacuolation as well as the hepatocellular swelling category, suggesting that this part of the grading system was highly reliable. On image analysis, sections with more than 50% lipid were most likely to be in the severe class, regardless of the other grading parameters. Due to the small sample size of image analysis, further evaluation is required. The plateauing of the percentage of lipid in the severe class as the grades increased likely represented the hepatocytes reaching their maximum swelling. Digital analysis did not account for fibrosis; therefore, the percentage of lipid plateaus as the grades continue to increase from fibrosis. There was a moderate correlation between the lipid percentage and fibrosis, indicating that as the amount of lipid increased, the liver was more likely to sustain damage leading to secondary fibrosis. Confounding factors that may have precluded a strong correlation of lipid percentage and hepatic fibrosis include cases with evidence of both hepatic lipid changes and chronic injury, infection, and neoplasia.9,12,16,18 Overall, the final grade and severity class had a strong correlation with the percentage of lipid on image analysis, indicating that diagnostic tests aimed at quantifying hepatic lipid (such as computed tomography) could be relatively accurate to estimate the lesion severity, excluding fibrosis. A limitation of image analysis was that an additional step was required for the software to exclude the sinusoids and portal spaces which, if measured, could decrease the value artificially.
While determining the repeatability of this grading system, hepatocellular swelling was found to have a moderate interobserver agreement, while the percentage of hepatocellular vacuolation and fibrosis was found to have strong agreement, in part validating the grading system. A large interobserver variability in the evaluation of hepatocyte ballooning has also been identified in grading of nonalcoholic fatty liver disease in humans.17,38 It is likely that the variability may be increased in this study, due to comparison between an experienced pathologist and clinical veterinarian. This variation has been demonstrated between pathologists with varying levels of training in liver pathology. 2 Further studies assessing interobserver variability between pathologists, with a larger sample size, and in a prospective cohort will be required, as there was moderate agreement in the final grade. However, there was strong agreement in severity classification of the disease, indicating this grading system may still be clinically relevant.
Clinical validation could not be completed due to the retrospective nature of this study. As archival materials were used, the animals’ life histories, clinical health, and antemortem diagnostic testing were unknown. In addition, samples were collected from 2 different laboratories over several years with possible differences in sample acquisition and handling, so there could be differences between groups due to unmeasured variables. 5 Finally, due to limited access to case information, it was not possible to determine whether cases were from the same household or pet store, which could have resulted in clustering of data and bias. 5
The grading system proposed in this study was derived to provide a concise and repeatable methodology, which reports the most characteristic features of hepatic lipid changes in bearded dragons. The cumulative grade and severity classification reported can be useful for monitoring of progression or improvement. Based on the lesions associated with hepatic lipid accumulation, a pathogenesis primarily involving direct lipid accumulation resulting in cellular swelling and injury, resulting in impaired hepatocyte function and secondary fibrosis, can be considered. Additional studies are needed to further validate and refine this grading system.
Supplemental Material
sj-pdf-1-vet-10.1177_03009858221128921 – Supplemental material for Morphological features of hepatic lipid changes in bearded dragons (Pogona vitticeps), and a proposed grading system
Supplemental material, sj-pdf-1-vet-10.1177_03009858221128921 for Morphological features of hepatic lipid changes in bearded dragons (Pogona vitticeps), and a proposed grading system by Trinita Barboza, Hugues Beaufrère, Drury Reavill and Leonardo Susta in Veterinary Pathology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.