
Abstract
Tumor grading is a method to quantify the putative clinical aggressiveness of a neoplasm based on specific histological features. A good grading system should be simple, easy to use, reproducible, and accurately segregate tumors into those with low versus high risk. The aim of this review is to summarize the histological and, when available, cytological grading systems applied in veterinary pathology, providing information regarding their prognostic impact, reproducibility, usefulness, and shortcomings. Most of the grading schemes used in veterinary medicine are developed for common tumor entities. Grading systems exist for soft tissue sarcoma, osteosarcoma, multilobular tumor of bone, mast cell tumor, lymphoma, mammary carcinoma, pulmonary carcinoma, urothelial carcinoma, renal cell carcinoma, prostatic carcinoma, and central nervous system tumors. The prognostic relevance of many grading schemes has been demonstrated, but for some tumor types the usefulness of grading remains controversial. Furthermore, validation studies are available only for a minority of the grading systems. Contrasting data on the prognostic power of some grading systems, lack of detailed instructions in the materials and methods in some studies, and lack of data on reproducibility and validation studies are discussed for the relevant grading systems. Awareness of the limitations of grading is necessary for pathologists and oncologists to use these systems appropriately and to drive initiatives for their improvement.
Keywords
Tumor grading refers to the microscopic assessment and quantification of parameters that correlate with the putative clinical aggressiveness of a neoplasm based on the tumor’s histomorphology. Histological grading should not be confused with staging, which refers to the extension of the disease based on tumor size and degree of local invasion, lymph node involvement, and presence of distant metastases. Staging performed by the clinician and grading performed by the pathologist provide different but interrelated information that affect oncological patient management. 25
Tumor grading assessment varies according to tumor type, and in some instances, more than one grading system is available for some tumors. Two-, 3-, or 4-tier grading systems are used. Most grading systems applied to canine and feline neoplasms are derived from the human counterparts, and with few exceptions are based on the assessment of cellular differentiation (evaluating architectural features and cell morphology) and proliferative activity. Ideally, a good grading system should be simple, easy to use, reproducible (good intra- and interobserver agreement), and able to accurately segregate categories of tumors with different biological behavior. 25,29
The aim of this review is to summarize grading systems available in veterinary pathology, provide information about their prognostic impact and reproducibility, indicate which systems have been validated by subsequent studies, and discuss the critical issues and shortcomings. Tumors for which prognostic parameters but not a grading system are currently available, such as melanoma, have not been included in this review. In order to avoid confusion and for consistency the term mitotic count (MC) will refer to the absolute number of mitoses counted in a specified number of fields or in a specified area, the term mitotic index (MI) will refer to the number of cells undergoing mitosis divided by the number of cells not undergoing mitosis, 73 and the term mitotic activity will be used as a generic term. Only a few of the grading systems described define the standard area of view for the assessment of the mitotic activity, 76,92,106 while the majority refers to high-power field (HPF), which is an inconsistent unit of measure. 73 The reader should be aware that comparison between HPF and mm2 is not possible unless the area of the HPF is defined.
Canine Soft Tissue Sarcomas
The grading system of canine soft tissue sarcoma (STS) is based on the so-called French grading system that is widely applied for human sarcomas. 27,60,128 In human medicine, soft tissues are defined as the extraskeletal connective tissues of the dermis, subcutis and fascia, striated and smooth muscle, vessels, serosal and synovial linings, and nerve sheaths. 45 STSs are therefore defined as malignant tumors that resemble, arise in or have their origin from soft tissues, and the grading system is applied to malignant tumors only. 45
In veterinary medicine the term canine STS is used inconsistently to indicate spindle cell tumors of subcutis, usually including fibrosarcoma, nerve sheath tumors, perivascular wall tumors, and undifferentiated pleomorphic sarcoma (previously known as malignant fibrous histiocytoma). 10,27,60,69 Entities such as liposarcoma and soft tissue leiomyosarcoma are inconsistently excluded from this group, thus leading to heterogeneous data in the literature. 10,27,69 These inconsistencies, the lack of specific diagnoses in some studies, 69,137 and the inclusion of benign entities in others 10,19,60 may have led to the application of the grading system also to benign canine spindle cell tumors in the daily diagnostic routine, thus creating a significant difference from the approach used in human pathology.
The French grading system was first applied by Kuntz and coauthors to canine STS with a change in the score assigned to tumor necrosis. 60 This change has subsequently been abandoned, and the original table of the French system is now consistently used. 27 Since the change in the necrosis score was associated with an adaptation of the cutoffs of total score to assign the grade, it did not affect the final result and the 2 grading schemes (French grading system and Kuntz-adapted version) represent the same system. Attention should be paid to use the appropriate cutoffs depending on the score used for necrosis. In the dog, the STS grading scheme does not apply to histiocytic sarcomas (being a leukocytic neoplasm) and is not validated in canine hemangiosarcoma or in other animal species. 27
The system divides STSs into 3 grades based on a total score obtained by the sum of individual scores estimating histologic differentiation, MC in 10 contiguous HPFs in the region with the greatest cellularity, and percentage of necrosis (Table 1). 22,27,60,128 The grade of canine STS was associated with overall survival in univariate analysis in 2 retrospective studies including 350 and 75 cases, respectively. 10,60 The grade was associated with local recurrence in 2 papers, 10,69 while consistent studies on the impact of grade on the risk of metastasis are lacking.
Grading System of Canine Soft Tissue Sarcoma. 27
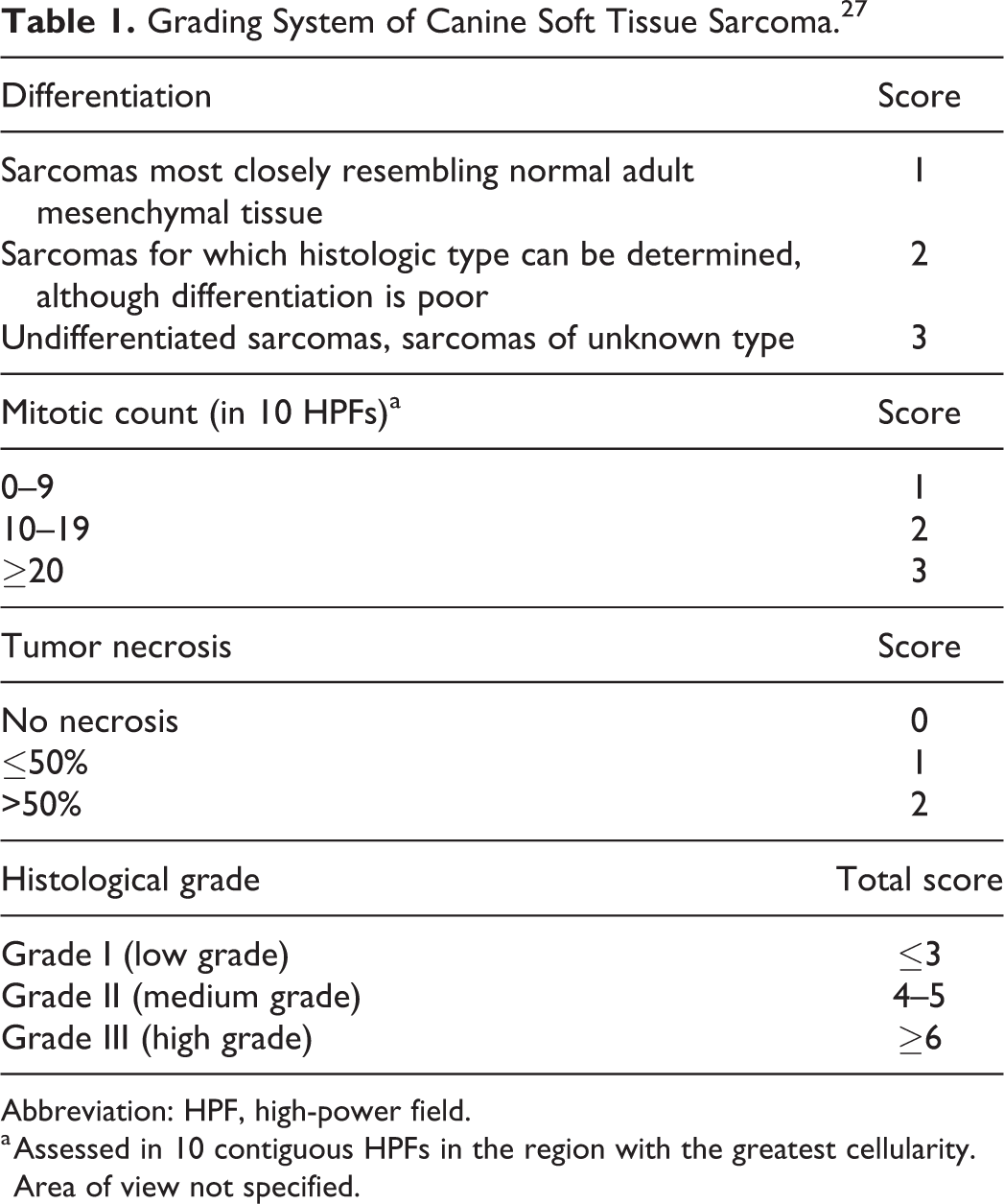
Abbreviation: HPF, high-power field.
a Assessed in 10 contiguous HPFs in the region with the greatest cellularity. Area of view not specified.
Regarding local recurrence, one study analyzed the recurrence-free time in 85 cases, which included a small proportion of high-grade STSs (4 cases). This study identified a correlation between grade and local recurrence. 69 This correlation was conditional to histological margins being less than 1 mm or infiltrated with neoplastic cells, whereas for those cases with a tumor-free margin greater than 1 mm, tumor grade was not associated with recurrence. 69 A second study of 350 cases (22 of which were high grade) also identified a correlation between grade and local recurrence, but the histological status of surgical margins was not available. 10 A third study, on 56 canine perivascular wall tumors (4 of which were high grade), failed to identify a correlation between grade and recurrence; in this study, recurrence was associated with other parameters including the status of surgical margins. 2 Prediction of local recurrence based solely on grade is therefore discouraged, and the histological status of margins should be considered the main prognostic factor for local recurrence. 2,27,60,69
For canine non-angiomatous visceral sarcomas, a significant association of grade with survival time was found in a series of 31 cases (5 grade I, 11 grade II, and 15 grade III) mainly located in the spleen and gastrointestinal tract. 62 Grade was also associated with metastatic rate, which was 20% for grade I, 27% for grade II, and 60% or grade III tumors. 62 Nevertheless, since these results are based on a small number of cases, for which the grade was determined reviewing pathology reports rather than slides, 62 it seems premature, in our opinion, to apply this grading system to visceral sarcomas until further studies confirming its prognostic impact will be available.
For canine oral fibrosarcoma, tumor grade should be weighed with caution because in this site up to 50% of low-grade tumors have an aggressive behavior characterized by rapid growth and progression, with short time to recurrence that is independent of grade (so-called histologically low-grade, biologically high-grade fibrosarcoma). 20,42,43
Critical issues regarding grading of canine STS are related to its reproducibility, having a high intraobserver but only moderate interobserver agreement. 137 The most subjective criterion is the differentiation parameter as it is defined, which may lead to disagreement among pathologists or to a bias in the evaluation of this parameter for some specific entities (eg, perivascular wall tumors do not closely resemble a normal adult tissue, 3,86 but some have a distinct histomorphology allowing for identification of the histogenesis and may not warrant a higher differentiation score). For the same reason, in human medicine, a predetermined differentiation score is assigned to a specific STS. 22 Furthermore, STS grading of presurgical biopsies has demonstrated low accuracy, often being discordant with the grade of the subsequently excised mass in 41% of the cases. 93 These discrepancies are mainly represented by underestimation of the grade on the presurgical sample. The discrepancies are independent of biopsy technique 93 and interpreted to reflect sampling of nonrepresentative tumor areas.
It has to be considered that the prognostic value of grading canine STS has been assessed by studies that are mostly retrospective and include a mixture of different tumor types, and the proportions often vary among studies or are not specified. Furthermore, imprecise diagnostic criteria may have led to the inclusion of benign tumors (eg, schwannomas or benign nerve sheath tumors) in such studies. Therefore, papers on canine STS are often difficult to compare, and the validity of the results should be weighted based on study design, number of cases, and outcome assessment.
Evaluation of STS grade has been attempted without success on cytological specimens. In one cytomorphological study of mesenchymal cell proliferations, the nuclear parameters of sarcoma cells did not differ between histological grade, MI, or necrosis score. 70 Furthermore, in cytological specimens, the nuclei from reactive proliferations were overall larger and displayed greater anisocytosis and pleomorphism than in STSs. 70
All considered, grading of canine STS is a useful prognostic tool especially in conjunction with status of resected margins, although prognostic studies with better defined criteria would be beneficial to improve its role in daily diagnostic activity.
Canine Splenic Hemangiosarcoma
As canine hemangiosarcoma generally carries a poor prognosis, it is generally not graded since most tumors fall into the highest category. Nevertheless, a grading system was applied in 2 studies on 46 and 30 cases of canine splenic hemangiosarcoma. 80,85 This grading system incorporates tumor differentiation, nuclear pleomorphism, tumor necrosis, and mitoses in 10 HPFs (Table 2). 80,85 In another study of dogs that were treated with doxorubicin, some elements of the histologic grading scheme (higher MC, increased nuclear pleomorphism, and tumor differentiation) were suggested as potential prognostic indicators. 85 However, in 1 of the 2 studies, the association of this grading scheme with survival was demonstrated on univariate but not on multivariate analysis. 80 Thus, lacking evidence of prognostic significance, this grading system has not been widely applied.
Grading System of Canine Splenic Hemangiosarcoma. 85
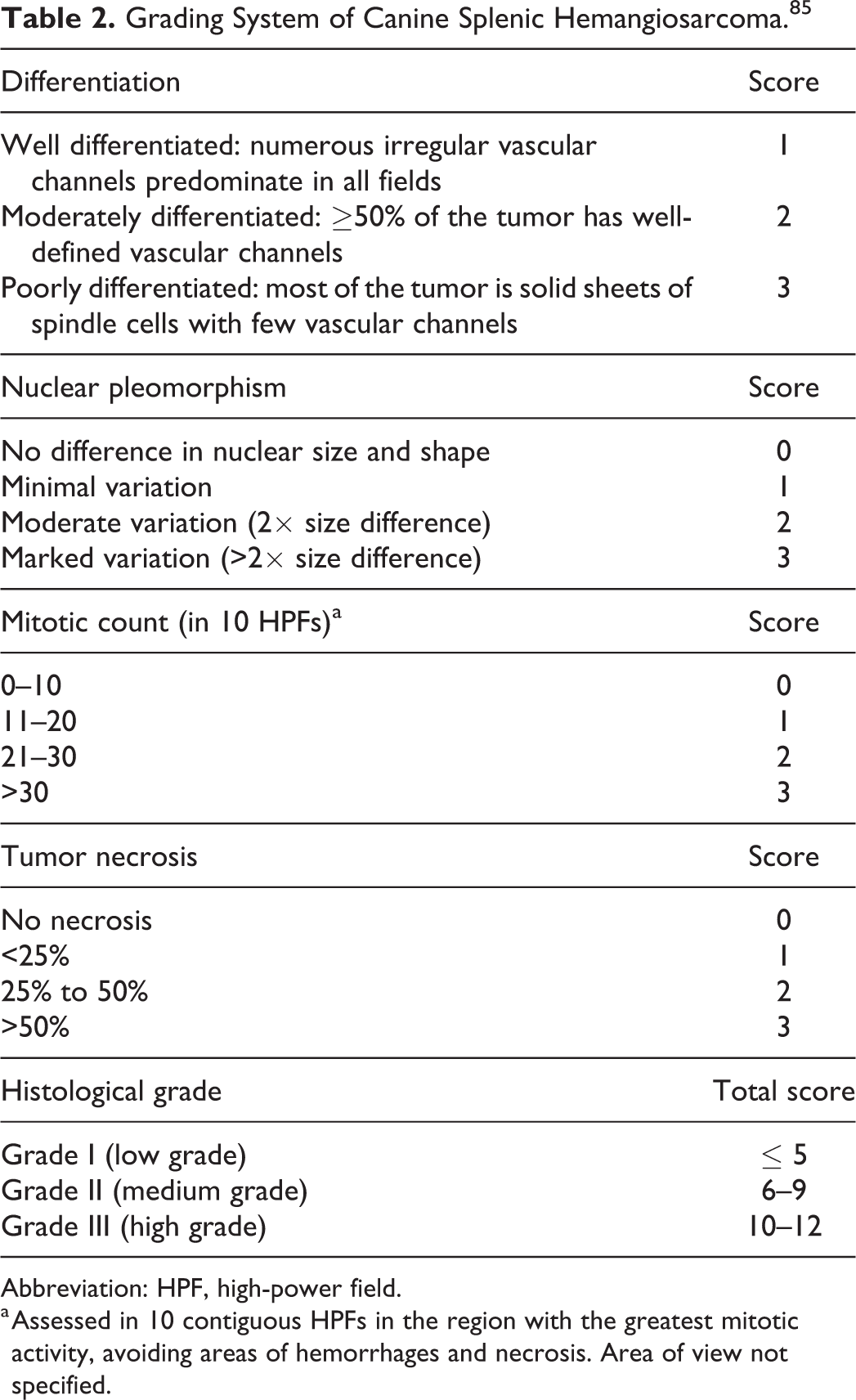
Abbreviation: HPF, high-power field.
a Assessed in 10 contiguous HPFs in the region with the greatest mitotic activity, avoiding areas of hemorrhages and necrosis. Area of view not specified.
Feline Injection Site Sarcoma
Feline injection site sarcoma (FISS) is the most frequent soft tissue sarcoma described in cats, 50 and a specific grading system for FISS has not been developed. The canine STS grading system is often used to predict FISS behavior based on a single study demonstrating an association with distant metastasis. 105 Nevertheless, subsequent studies failed to replicate this result or to demonstrate a prognostic impact. 44,94,101 A recent paper proposed a variation of the STS grading system for feline STS, maintaining the parameters of mitotic count and necrosis, and replacing the parameter of differentiation with the amount of inflammation. 32 Unfortunately, it is not clear how many cases included in the study were FISS and how many were STS not related to injection. 32 The lack of information on the proportion of these 2 groups, and lack of information on the status of surgical margins in the majority of cases, makes it difficult to assess the real prognostic impact of this scheme. 32 Thus, until larger prospective studies are performed, the application of grading in FISS is discouraged.
Canine Osteosarcoma
Two distinct grading systems are reported for osteosarcoma in dogs. One system divides osteosarcoma into 3 grades based on a total score obtained by summing individual scores evaluating degree of nuclear pleomorphism, MC in 10 random HPFs, and percentage of necrosis (Table 3). This system was initially developed for mandibular osteosarcoma and was associated with 1-year survival rate. 122 Subsequently, the same system was applied to 140 cases of appendicular and axial osteosarcoma (Loukopoulos system) and found to be significantly associated with development of distant metastases. 64 Finally, it was applied to a series of canine osteosarcomas arising from flat and irregular bones and carried no prognostic value. 59
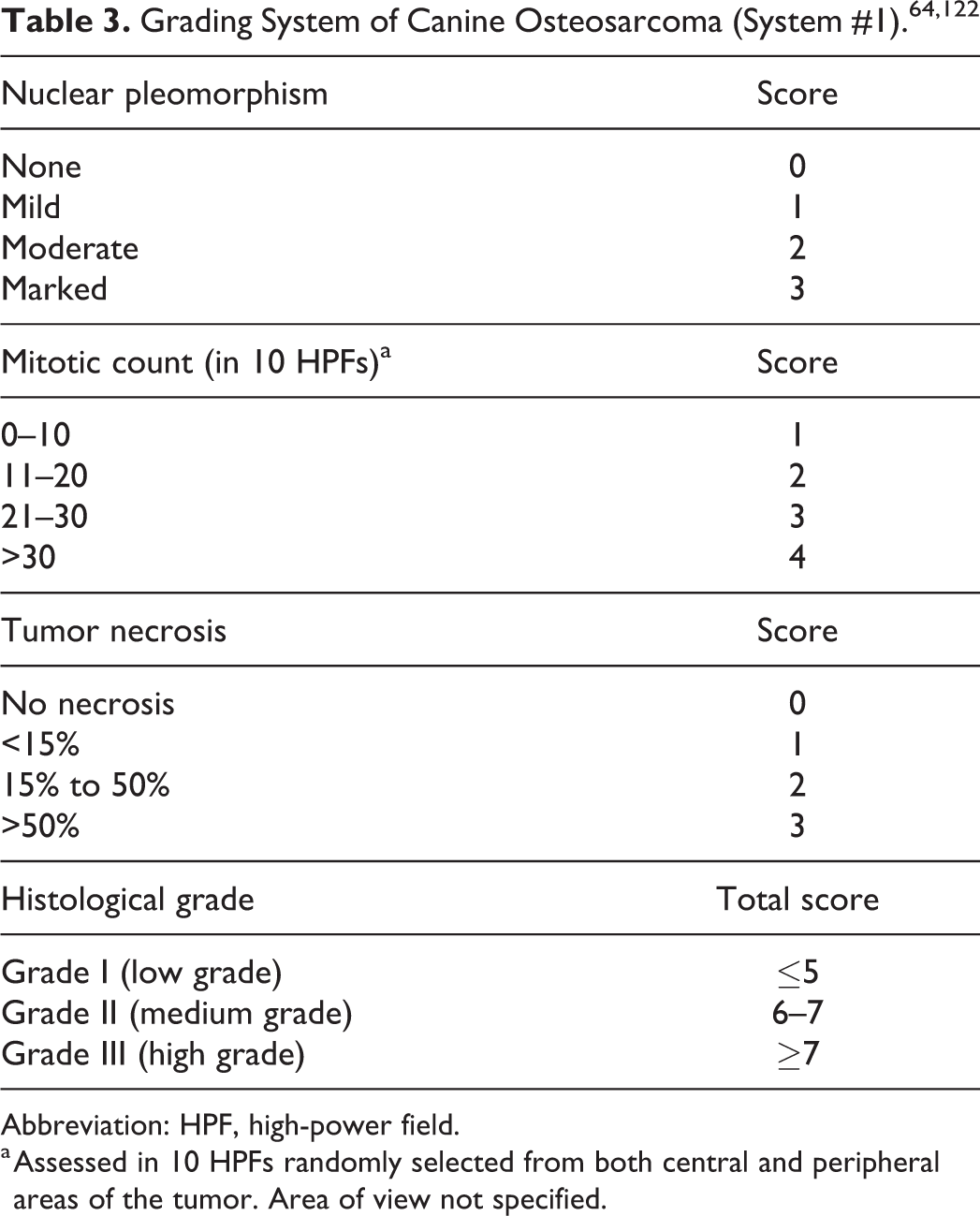
Abbreviation: HPF, high-power field.
a Assessed in 10 HPFs randomly selected from both central and peripheral areas of the tumor. Area of view not specified.
A second grading system (Kirpensteijn system) was proposed and applied to appendicular and axial osteosarcoma. It is a 3-tier system defining grade by a predetermined histologic score that assesses nuclear pleomorphism, MC in 3 random HPFs, amount of tumor matrix, cellularity, and percentage of necrosis (Table 4). All the cases with lymphovascular invasion or lymph node metastases were classified as grade III independently from any of the other parameters. 55 In the original study, performed on 166 appendicular osteosarcomas, the grade was significantly associated with disease-free interval and survival time. 55 Unfortunately, since the grade is assessed by a predetermined classification scheme and not by cumulative score, it can be difficult to assign a grade in cases with conflicting histologic features (ie, in a single case, different histologic features are associated with different grades). 55 This issue was addressed more recently, in a study comparing the performances of both grading systems on 85 appendicular osteosarcomas and in which the interpathologist agreement was low in the Kirpensteijn system and fair in the Loukopoulos system. 112 Despite the standardization of the area evaluated for the MC in the comparison study, lack of specific guidelines for the choice of the random HPF may be one of the factors contributing to the low agreement. Furthermore, neither one of the grading systems was associated with prognosis. 112
Grading System of Canine Osteosarcoma (System #2). 55

Abbreviation: HPF, high-power field.
a Assessed in 3 random HPFs. Area of view not specified.
The discrepancies regarding the prognostic significance of these grading systems might reflect differences in number of cases included in each study, site of the tumors (axial, appendicular, or both), and variable chemotherapy protocols applied, thus generating potential bias. 55,59,64,112 The suboptimal interpathologist agreement and the contradictory prognostic impact reported for both grading systems 55,64,112 warrant caution in their application and interpretation. Furthermore, studies aimed to better define the criteria and procedures used to assess the value of grading systems for osteosarcoma are needed in order to clarify differences between the competing grading systems.
Feline Osteosarcoma
An adapted version of the Kirpensteijn grading system was developed for feline osteosarcoma and tested on a case series of 62 appendicular, axial, and extraskeletal tumors (Table 5). The histological grade score was associated with survival time, disease-free interval, and recurrence-free interval. 31 In this grading system, the final grade was calculated by adding the individual score of each histological variable. Nevertheless, cutoffs for categorization and the number of cases classified as low, intermediate, and high grade were not provided, making the use of this system unfeasible. 31
Grading System of Feline Osteosarcoma. 31

Abbreviation: HPF, high-power field.
a Assessed in 3 random HPFs. Area of view not specified.
Canine Multilobular Tumor of Bone
A 3-tier grading system for multilobular tumor of bone in dogs includes assessment of the following criteria: borders of the tumors, size of the lobules, architectural organization, MC in 10 HPFs, cellular pleomorphism, and presence of necrosis (Table 6). 121 The prognostic impact of this grading system was assessed in a single study of 39 dogs (13 grade I, 17 grade II, and 9 grade III), and higher grade was associated with decreased time to local recurrence (>1332, 782, and 288 days for grades I, II, and III, respectively), time to metastasis (>820, 405, and 321 days for grades I, II, and III, respectively), and survival time (>897, 520, and 405 days for grades I, II, and III, respectively). 28
Grading System of Canine Multilobular Tumor of Bone. 121
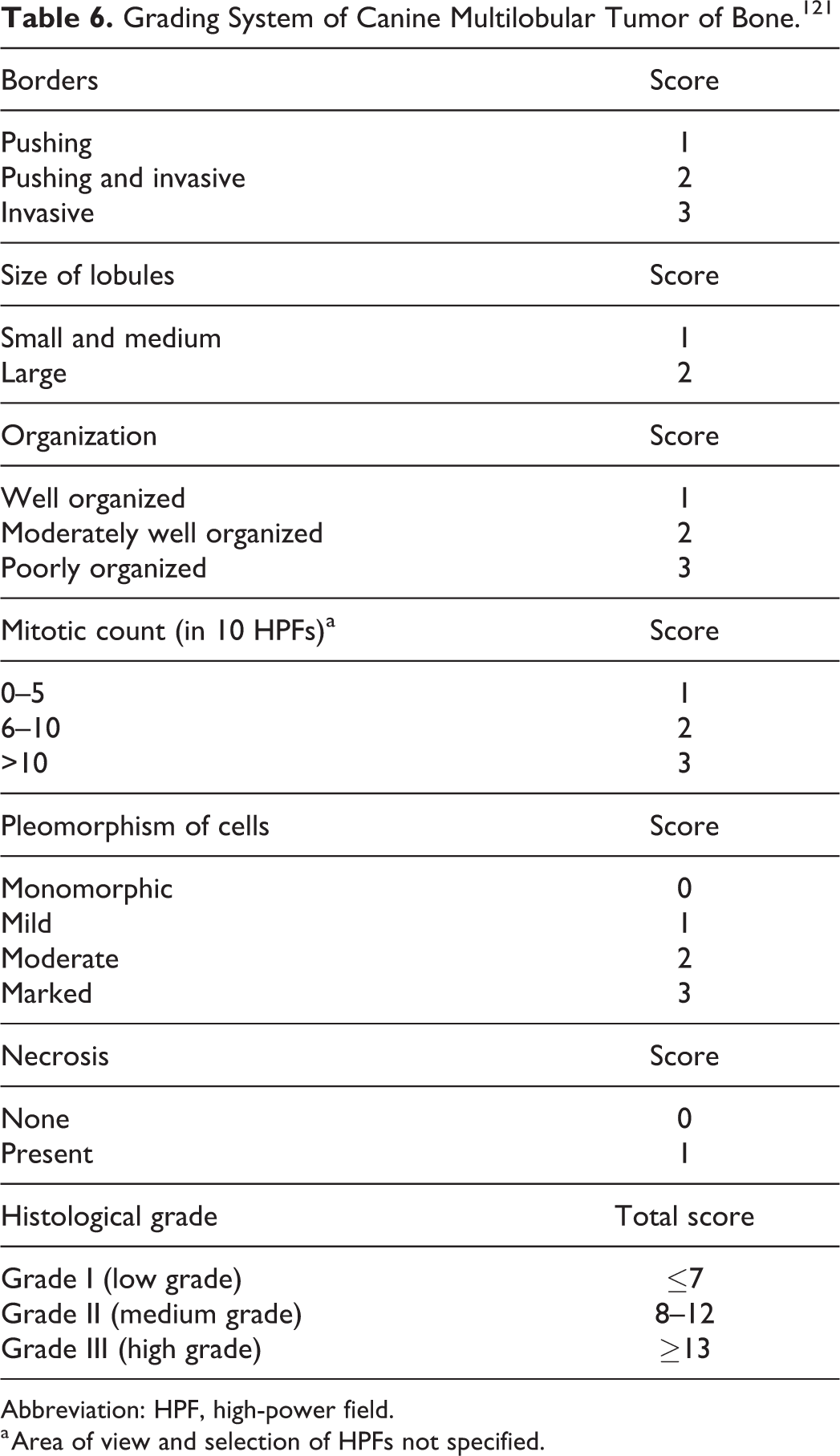
Abbreviation: HPF, high-power field.
a Area of view and selection of HPFs not specified.
Unfortunately, some of the criteria used to calculate the grade (borders, size of lobules, organization, cellular pleomorphism, and area selected for the MC) are not well specified and may be subjective. Studies assessing the reproducibility of this grading system are lacking. Further studies on larger caseloads would be beneficial to better understand the prognostic impact and reproducibility of this grading.
Canine Mast Cell Tumors
Mast cell tumors (MCTs) are common neoplasms in dogs, 8,47 the majority developing in the skin with possible secondary involvement of the subcutis. 127 Canine cutaneous MCTs have variable potential for local recurrence and metastasis, 53,120,124 and accurate prediction of the clinical outcome is critical. 8,53 Histological grade is the most widely used parameter for prognosticating and directing adjuvant treatment in dogs with cutaneous MCTs. 51,57,115
This section will focus on the different histological and cytological grading systems available in veterinary literature, methods for their application, and their shortcomings. For more specific guidelines and information on their prognostic impact, refer to the consensus paper on this topic in this issue. 6 Histological grading of canine MCTs has been developed and validated for cutaneous MCTs and it is not to be applied in primarily subcutaneous, mucosal, or visceral MCTs. 36,127 In addition, most studies assessing the grade of canine cutaneous MCTs included primary tumors removed surgically as primary therapeutic intervention, 57,89,115,120 and the prognostic relevance of grading in recurrent MCTs remains unknown. Grading on small pretreatment incisional biopsies is considered appealing, but has led to underestimation of the histological grade in a minority of cases. 115
The first grading system for canine cutaneous and subcutaneous MCTs was published in 1973 by Bostock, 9 followed in 1984 by Patnaik and colleagues, 89 which is still widely used. The Patnaik system (Table 7) is a 3-tier scheme based on assessment of tumoral architecture (tissue extension, cellularity, stromal reaction, edema, and necrosis) and cellular morphology (cell shape, cytoplasmic granularity, nuclear characteristics, and mitotic activity). 89 Despite its longevity and wide application, the Patnaik system has been associated with interobserver variability: while there is usually good agreement in diagnosing grade III MCTs, there is moderate disagreement in the diagnosis of grade I and II MCTs, 57,83,134 putatively ascribed to the subjective assessment of tissue extension: superficial dermis/interfollicular spaces (grade I) versus lower dermis/subcutis/muscle (grade II). 57,83,134 Another issue contributing to the interobserver variability may be similar to the Kirpensteijn canine osteosarcoma grading system; that is, some tumors do not quite fit into any of the 3 classifications because of differences in one or more criteria. The majority of Patnaik grade I MCTs are associated with an excellent prognosis and are usually cured by complete surgical excision. 53,81,107 Reports of metastasis of grade I MCTs exist, but they are rare, 4,97,120 and in view of the possible subjectivity in differentiating grade I and grade II MCTs, studies incorporating interpathologist agreement on grade I tumors would further clarify their prognostic significance. Patnaik grade III MCTs have been documented to be more aggressive than grade I MCTs with higher rates of local recurrence, metastasis, and tumor-related death and often requiring adjunctive therapy. 8,53,120 On the contrary, the biological behavior of Patnaik grade II MCTs is more difficult to predict and unfortunately the majority of canine cutaneous MCTs seem to fall in this category. 57 For grade II MCTs there is considerable variation among studies with regard to the rates of local recurrence, metastasis, and tumor-related death. 81,107,111,136 Although the interobserver variability likely has some impact on the disparate clinical outcomes reported in the literature for grade II MCTs, it is also clear that this category encompasses a heterogeneous group of MCTs with different biological behaviours. 53
Three-Tier Grading System of Canine Cutaneous Mast Cell Tumor. 89
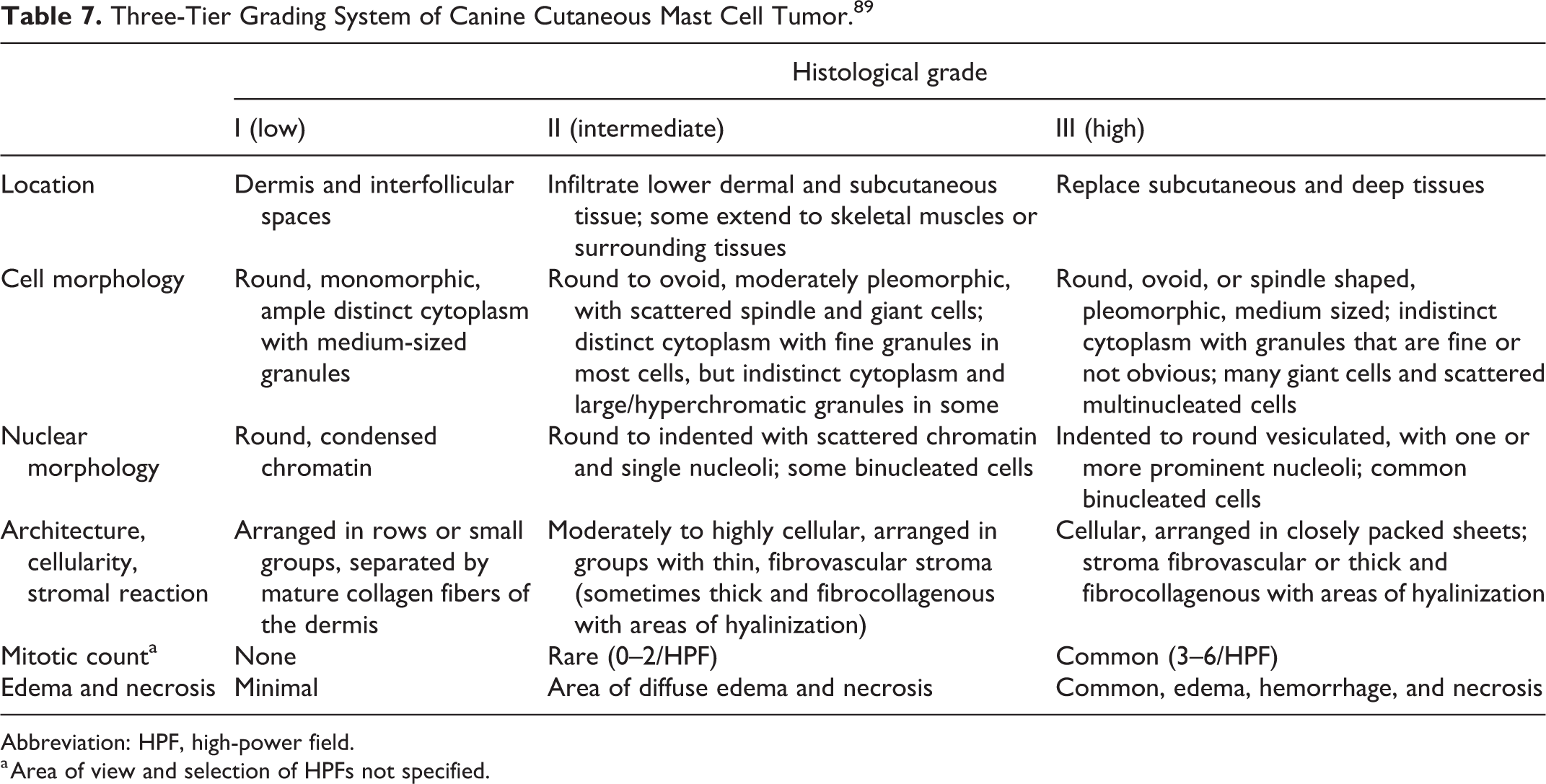
Abbreviation: HPF, high-power field.
a Area of view and selection of HPFs not specified.
In an attempt to address the limitations posed by the Patnaik system, in 2011 Kiupel and colleagues 57 proposed a 2-tier grading scheme (Table 8) to classify canine cutaneous MCTs as either low grade or high grade based only on cellular morphology (MC, karyomegaly, multinucleated cells, and bizarre nuclei). Comparing the cellular morphologic criteria included in the Kiupel system and Patnaik system, there are similarities (size and shape of the nuclei and mitotic activity), but also some differences (the Patnaik system considers the morphology of the cytoplasmic granules and the presence/absence of binucleated cells, which are not included in the Kiupel system). For the features included in both systems, the 2-tiered grading provides a more standardized approach (eg, for cells with at least 3 nuclei a specific cutoff that separates low- and high-grade MCTs is given). According to the Kiupel grading system, the majority of canine cutaneous MCTs are included in the low-grade category, even if the proportion of low-grade MCT is variable (59.6% to 89.5%). 34,53,57,91,104,107,120,124,134
Two-Tier Grading System of Canine Cutaneous Mast Cell Tumor. 57
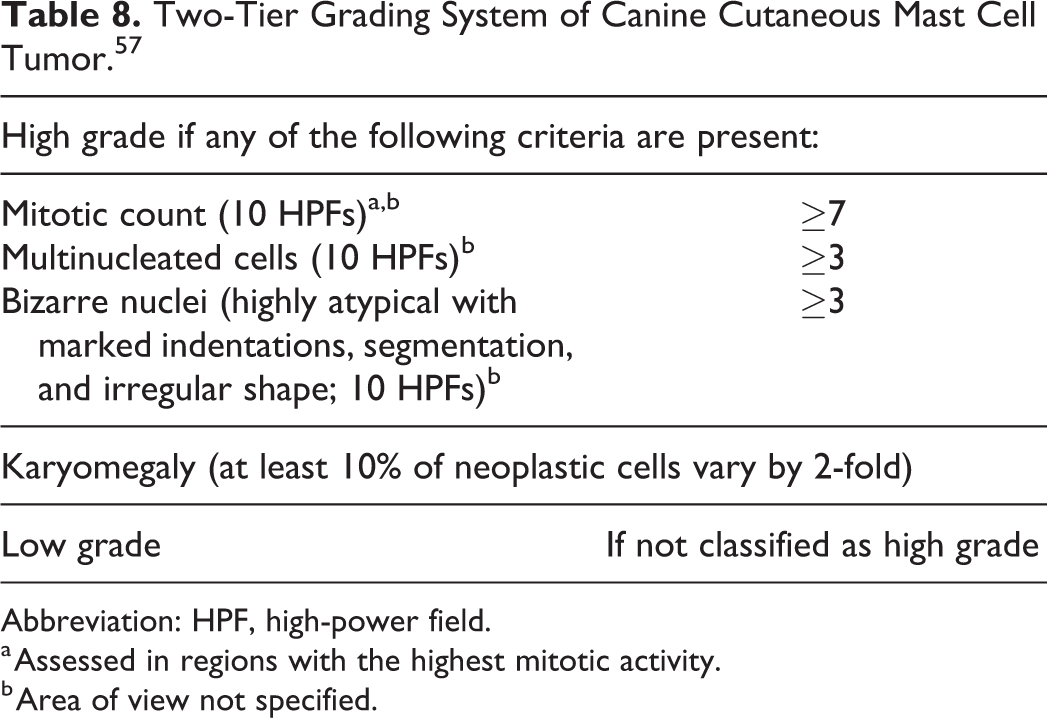
Abbreviation: HPF, high-power field.
a Assessed in regions with the highest mitotic activity.
b Area of view not specified.
Various studies have tested the performance of the Kiupel grading system alone and in relation to the Patnaik system. The Kiupel grade is an independent prognostic factor in dogs with cutaneous MCTs, 34,57,107 with low-grade MCTs having a lower rate of recurrence, metastasis, and tumor-related death than high-grade MCTs. 34,57,107,134 By removing the architectural tumor features from the grading and providing more details on how to judge the cellular morphological features, the Kiupel system improves the concordance among pathologists. 57,124 When applying the Kiupel and Patnaik systems to the same cohort of MCTs, grade I tumors are always assigned to the low-grade category and grade III tumors to the high-grade category, and consistently among the studies, most Patnaik grade II MCTs are classified as Kiupel low-grade and a smaller subset as high grade, the latter demonstrating a worse long-term prognosis. 7,34,57,107,134
Nevertheless, one study has suggested that among the Kiupel high-grade MCTs there is a difference between Patnaik grade II and grade III MCTs, with the former having longer survival times, 107 and because the Patnaik system is the one oncologists and clinicians are more familiar with, it has not been completely abandoned. For this reason, both systems are frequently used in routine diagnostic and clinical practice and are included in the most recent publications on the epidemiology, prognosis, and treatment of canine cutaneous MCTs. 66,91,104
Relevantly, studies on MCT grading system should avoid mixing cutaneous MCTs and primarily subcutaneous MCTs. Subcutaneous MCTs are less common than their cutaneous counterparts with less information in the literature regarding their histologic diagnosis and biologic behavior, although some authors have suggested a favorable clinical outcome when arising in the subcutaneous tissue. 127 Nevertheless, robust distinction between cutaneous and subcutaneous MCTs in terms of behavior is still lacking and urgently needed. However, a specific grading system for subcutaneous MCTs has not been validated yet. 127 Finally, it should be remembered that apart from the grade there are other prognostic indicators in dogs with cutaneous MCTs such as the clinical stage, and when available, these should be taken into consideration to better predict the MCT behavior. 8,79
Given the widespread use of cytology for diagnosing MCTs, grading of MCTs on cytological specimens in order to provide prognostic information prior to surgery has also been attempted. 12,51,110 The main limitation of cytological grading is the inability to differentiate between cutaneous and subcutaneous MCT. Indeed, current grading schemes apply only to cutaneous tumors; 12,51,110 thus, this is a clinically significant limitation. The development of a common grading system for cutaneous and subcutaneous MCT would be useful to overcome this limitation.
Three cytological grading schemes for MCTs have been proposed in the last 10 years. Of these, only one study correlated the performance of the proposed cytological grading system to survival time of patients. 12 The Camus system 12 is the only cytological grading scheme that added granularity (as assessed on slides stained with a modified Wright’s stain) and presence of binucleated cells. The other 2 studies only investigated the performance of the Kiupel grading system when applied to cytology, with or without changes to the cutoff values used on histopathology. 51,110
The Camus cytologic grade 12 was obtained by evaluating 100 intact cells in a single smear (modified Wright’s stained). Tumors were classified as high grade if cells were poorly granulated or two of the following were found: presence of mitoses, anisokaryosis (defined as a variation of the nuclear size greater than 50%), binucleation/multinucleation, and nuclear pleomorphism (Table 9). This grading was found to be predictive for survival time and correlated well with the Kiupel grading system (specificity of 94.8% and sensitivity of 88.2%). A weakness of this system is the overestimation of high-grade cases potentially leading to a more aggressive course of treatment. The total intraobserver agreement was 75.5% (73.6% and 81.8% for low- and high-grade MCTs, respectively), while interslide variability and interlaboratory agreement was not investigated. 12
Cytological Grading Systema of Canine Cutaneous Mast Cell Tumor. 12
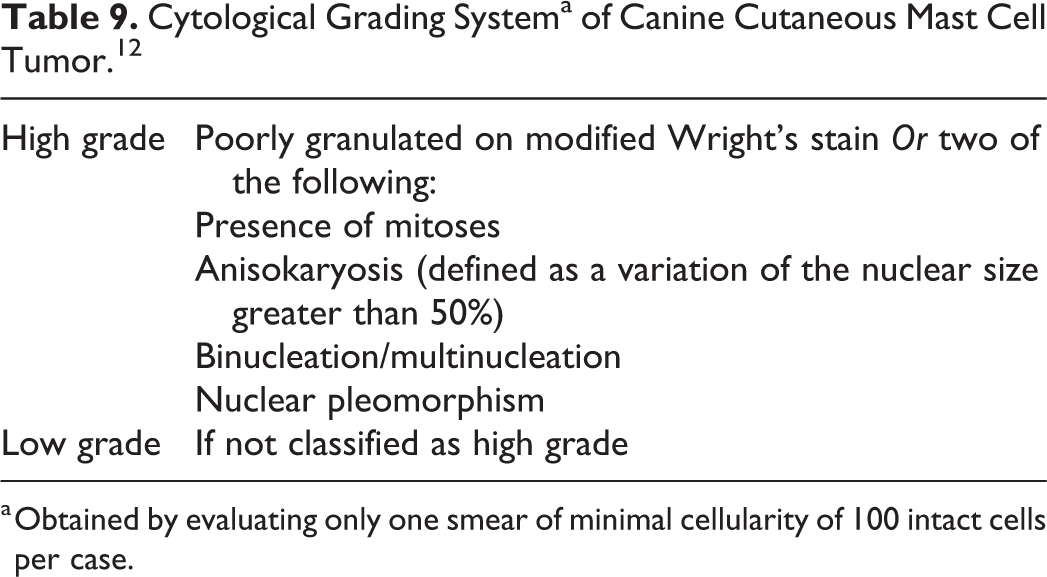
a Obtained by evaluating only one smear of minimal cellularity of 100 intact cells per case.
Scarpa and coauthors 110 proposed a cytologic grading system assessed on approximately 1000 intact cells, stained with May Grünwald-Giemsa. The areas with the most cellular monolayer or greater pleomorphism are selected for the grading. By applying the same technique and cutoff values used in the Kiupel grading, this cytologic grading showed a specificity of 97%, sensitivity of 85%, and accuracy of 94% in predicting the Kiupel histological grading. The sensitivity was increased to 92% by changing the cutoff value for mitoses to equal or greater than 1. The higher cell numbers required to use this scheme may be a limitation. 110
Similarly, Hergt and coauthors 51 used the Kiupel grading system as gold standard with overall accuracy of 94.3%, and the specificity and sensitivity were 86.8% and 97.1%, respectively, in predicting the Kiupel histological grading. By changing the cutoff values for each parameter to 1 in 10 HPF, the performance of the cytologic grading did not improve significantly. 51 Neither Scarpa nor Hergt provided information on interobserver agreement. 51,110 In a morphometric study, the mean nuclear area correlated with survival, and based on this parameter the Patnaik grade II MCTs could be subdivided into 2 groups with different behavior. This study did not evaluate interobserver variability. 123 Grading of MCTs on cytology seems therefore promising, despite the often-cited limitation that the site of tumor development cannot be identified. However, the lack of information regarding interobserver agreement 51,110 and the risk of overestimation of the grade 12 suggest further validation before their wider application. All considered, application of the 2 histologic grading systems, especially in conjunction, provides useful information to predict the behavior of canine cutaneous MCTs.
Feline Mast Cell Tumors
A 2-tier histologic grading system has been proposed for feline cutaneous MCTs. 106 Cases with multiple tumor nodules can also be assessed by this grading system if all the nodules are surgically removed. MCT is classified as high grade when MC is higher than 5 and when at least 2 of the following 3 findings are present: tumor diameter >1.5 cm, nuclear pleomorphism (irregular nuclear shape), and nucleolar prominence/chromatin clusters. Tumors that do not meet the above-mentioned criteria are classified as low grade (Table 10). For MC, areas of high mitotic activity on a slide should be selected for evaluation. MC is assessed in a 2.37 mm2 area. 73,106 Nuclear shape variation such as angular, markedly indented, or multilobulated nuclei are included under nuclear pleomorphism. If the majority of tumor cells have round to oval nuclei, nuclear pleomorphism is considered absent. Nucleolar prominence/chromatin clusters are considered present if more than 50% of tumor cells exhibit nuclei with more than one large nucleolus or coarsely stippled chromatin. The tumor diameter needs to be provided in the submission form by the clinician. 106
Grading System of Feline Cutaneous Mast Cell Tumor. 106
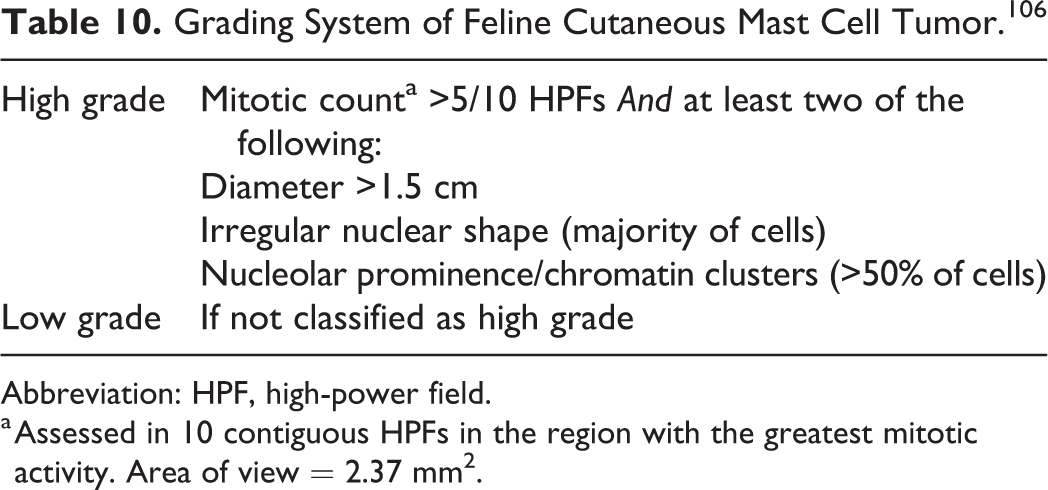
Abbreviation: HPF, high-power field.
a Assessed in 10 contiguous HPFs in the region with the greatest mitotic activity. Area of view = 2.37 mm2.
In this study, enrolling 63 cats with cutaneous mast cell tumors, the median overall survival was significantly reduced in high-grade cases compared to low-grade cases. 106 This system should be further validated in a different population of cats including a larger number of atypical MCTs.
Lymphoma
The grading of lymphoma in small animals is by definition based on histological tumor features assessed in sections of lymph nodes (fully excised or examined via Tru-cut biopsies). Except for few tumor types such as follicular lymphomas, mitotic activity is the cornerstone of histological grading. 15,100,129,130,132,133,135
Oncologists rely on diagnosis, phenotype, and grade of lymphoma to guide therapeutic decisions and prognostic judgments in small animals. Different types of lymphoma are recognized to differ in their biological behavior. 38,40,100,130,132,133 This has greatly advanced the clinical management of the disease, but at the same time it has also led to confusion and lack of distinction between the classification (giving a name to the specific lymphoma type) and the histological grading. Specifically, the term “grade” is commonly and incorrectly applied to indicate the expected clinical course of the untreated disease (eg, high-grade B-cell lymphoma), but it is pivotal to point out that this use of the term grade is inappropriate (from now on referred as “clinical grade”) and different from the true histological grade that is based on the assessment of specific histologic features.
A further consequence of this misunderstanding is that, because the cytologic evaluation of lymph node aspirates allows for the diagnosis of many lymphoma types, 15 cytopathologic reports often include in their diagnosis this “clinical grading” concept, which has an unknown relationship to the histological grade. As an example, the most common type of lymphoma in the dog, diffuse large B cell lymphoma (DLBCL), is often cytologically recognizable and has been associated with an aggressive clinical course (improperly referred as high grade). Thus, cytological diagnosis of DLBCL is often extended conceptually to provide a cytological grade to the lesion. This extension, while practically useful, further adds to the confusion between classification and grade.
In order to avoid this misunderstanding and to put an end to the confusion added by the misuse of terminology, it is advisable that oncologists, clinical pathologists, and anatomical pathologists come to an agreement to reach a clear distinction and to clearly separate clinical behavior, classification of the type of lymphoma and histological grade. Thus, it is highly recommended to use the terms indolent, intermediate, and aggressive behavior to stratify lymphomas by their predicted clinical course (when untreated) and to stratify histological grade into low-, medium- and high-grade categories. It is also advisable to avoid the term “grade” in cytological reports. Therefore, in this section, the main focus will be the histological grading of lymphoma according to mitotic activity. 15,100,129,130,132,133,135
Various studies, mainly for lymphomas in dogs, have analyzed the prognostic significance of the MC alone or in conjunction with other proliferation parameters, such as Ki67 labeling index. 5,23,30,38,40,41,56,77,90,95,98,99,126,131 Unfortunately, MC has often been evaluated with different magnifications and in a different number of fields, without indicating the area of view, thus leading to a lack of standardization and consistency (Supplemental Table S1) and hampering comparisons among studies. Also, the association of mitotic activity and tumor behavior has often been evaluated by grouping different types of lymphomas. 30,38,95,131,133 This lack of uniformity in the methods has likely contributed to the variable results reported in the literature on the prognostic significance of the MC and the histologic grading of lymphomas.
The most commonly used grading scheme for lymphomas in veterinary medicine is the WHO grading scheme, 129 which has been applied to 2 separate large cohorts of dogs with nodal lymphoma. 131,132 The World Health Organization (WHO) grading scheme defines grade based on the MC in one 400× field (Table 11). Despite the fact that the exact method of counting mitoses was not clearly specified in the Material and Methods section of these publications, the mitoses were counted in 10 fields at 400× and the average was determined (personal observations by 2 authors involved in 1 of these 2 works: W. Vernau and P. Roccabianca).
Grading System of Canine Lymphoma. 132
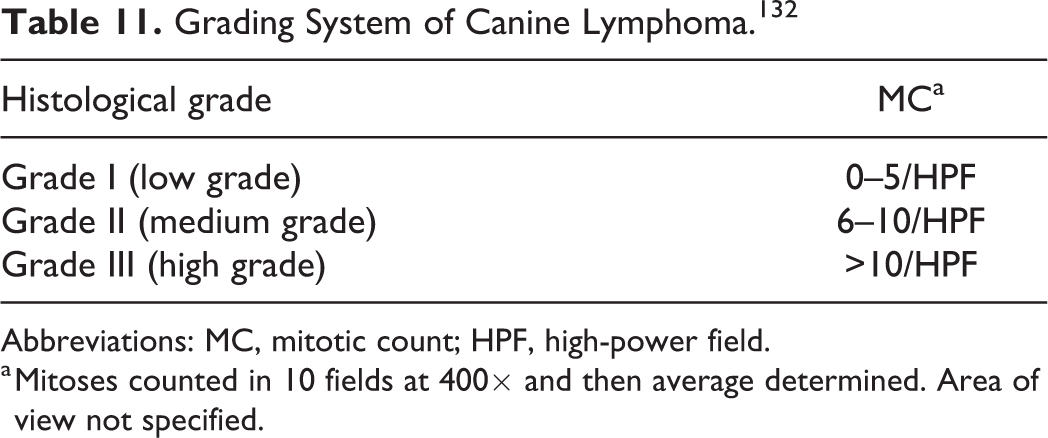
Abbreviations: MC, mitotic count; HPF, high-power field.
a Mitoses counted in 10 fields at 400× and then average determined. Area of view not specified.
In the same 2 studies the lymphomas have also been classified on the basis of other features such as immunophenotype, maturity of cells, growth pattern (nodular vs diffuse), and nuclear size determined as small (<1.5 the size of a red blood cell), intermediate (1.5–2 the size of a red blood cell), or large (>2 the size of a red blood cell). However, it is important to stress that these additional microscopic features were not used in any way to determine the grade.
In one of these 2 studies the MC correlated with the diagnosis of clinically indolent and aggressive tumors, but when divided in the 3 cutoffs used for grading, it did not correlate with overall survival. Nevertheless, when the cutoff was set into 2 categories, less than 20 mitotic figures (353 cases) and more than 21 mitoses (26 cases) per 400× field, good agreement with overall survival was obtained. However, analysis of survival was performed retrospectively on groups of heterogeneous lymphoma types and not for every single lymphoma type (because of low numerosity of certain tumors) introducing a bias on survival curves. 131
More specific information on the prognostic significance of MC and grade is available for a subset of lymphomas called nodular lymphomas (marginal zone, mantle zone, follicular, and T-zone lymphomas). These types of lymphoma have been identified according to cell size and specific growth patterns, and they were found to be associated with a low grade (because of the low MC), an indolent clinical course, and a prolonged survival. 38,39,100,113,132,133,138 Nevertheless, in 2 different studies, MC stratification did not impact survival times for nodular lymphomas, 38,133 thus suggesting that the WHO grading system does not add significant information to predict the clinical course of these entities. In 1 of the 2 reports, however, statistical analysis was performed by grouping marginal and T-zone lymphomas, again introducing a bias in the statistical evaluation. 38
A separate histological grading system has been proposed for follicular lymphomas; 129 that is, counting the number of centroblasts in 10 neoplastic follicles and then stating the average per single 400× field (Table 12). In humans, follicular lymphomas are frequent and this grading system has demonstrated clinical relevance. 71 However, follicular lymphomas are rare in dogs and cats, 38,39,131 –133 and information on the utility of this histological grading is lacking. 100,129,130,132,133
Grading System of Canine Follicular Lymphoma. 133
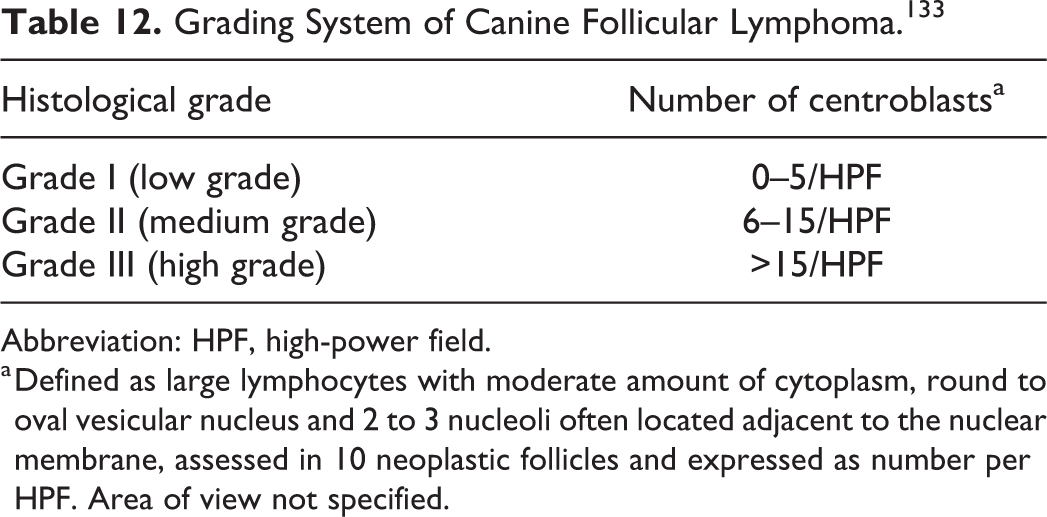
Abbreviation: HPF, high-power field.
a Defined as large lymphocytes with moderate amount of cytoplasm, round to oval vesicular nucleus and 2 to 3 nucleoli often located adjacent to the nuclear membrane, assessed in 10 neoplastic follicles and expressed as number per HPF. Area of view not specified.
Specific guidelines for histological grading of animal lymphomas that are located in anatomic sites other than the lymph nodes (eg, alimentary tract, respiratory tract, skin) have not been established yet and there is no current evidence that grading lymphomas in these locations has prognostic relevance. However, at least in the alimentary tract there is some evidence that feline and canine small cell lymphomas with low MC tend to have a better prognosis 23,90 than large cell lymphomas with high MC. 5
In the few cytopathological studies that stratified the mitotic activity (total number of mitoses identified in 5 fields at 500×: 0 to 1; 2 to 4; ≥5) of canine lymphomas, no correlation with the clinical outcome was identified. 39,40 The concern regarding cytology will always be whether the mitotic count in the sample is representative of the overall tumor mitotic activity.
In conclusion, the specific role of histological grade for prognostication of lymphomas in animals remains unclear until more studies with a standardized methodology and follow-up data on large numbers of each lymphoma type become available.
Canine Splenic Fibrohistiocytic Nodules
Histological grading of canine splenic fibrohistiocytic nodules was traditionally based on the percentage of lymphoid cells relative to fibrous and histiocytic cells estimated subjectively at 5× magnification. 119 Nevertheless, fibrohistiocytic nodules have been reclassified as they represent a heterogeneous group of diseases comprising nodular hyperplasia, lymphomas, stromal sarcomas, and histiocytic sarcomas with the latter having the worst prognosis. 78 Thus, it is highly recommended to discontinue the term “fibrohistiocytic nodule” for splenic lesions and to reevaluate prognostic parameters, including grading, according to the specific diseases previously encompassed by that term.
Canine Mammary Carcinomas
Canine mammary tumors are among the most frequent neoplasms in female dogs, half of which have malignant histologic features, but come with a broad range of clinical outcomes. 13,46 The principles of the human Nottingham Histological Grade (NHG) for breast cancer have been applied to canine mammary carcinomas (CMCs) removed surgically as the primary therapeutic intervention. 13,21,37,54,82,92,102,103,109 The NHG is based on the assessment of tubule formation, nuclear pleomorphism, and MC. Each parameter is scored from 1 to 3 and the cumulative score determines the grade. 37 The NHG system is designed for epithelial neoplasms and is not applicable to nonepithelial tumors such as mammary sarcomas. 92 However, mammary sarcomas are not common in dogs; 1 hence, the NHG system can be used in most instances.
The diversity of cellular populations involved in CMCs, which often includes luminal epithelium and myoepithelium, and the great heterogeneity of their histological patterns, led Peña and coauthors to provide guidelines on how to grade CMCs with myoepithelial component using a 3-tier grading system derived from the NHG (Table 13). 92 Since its publication, the Peña system has been widely adopted in the veterinary literature with numerous publications. 13,16,82,102,109,118 Further detail on its application in specific histotypes are available in Volume 2 (Mammary Tumors) of the series Surgical Pathology of Domestic Animals of the CL Davis Foundation. 140
Grading System of Canine Mammary Carcinomas. 92
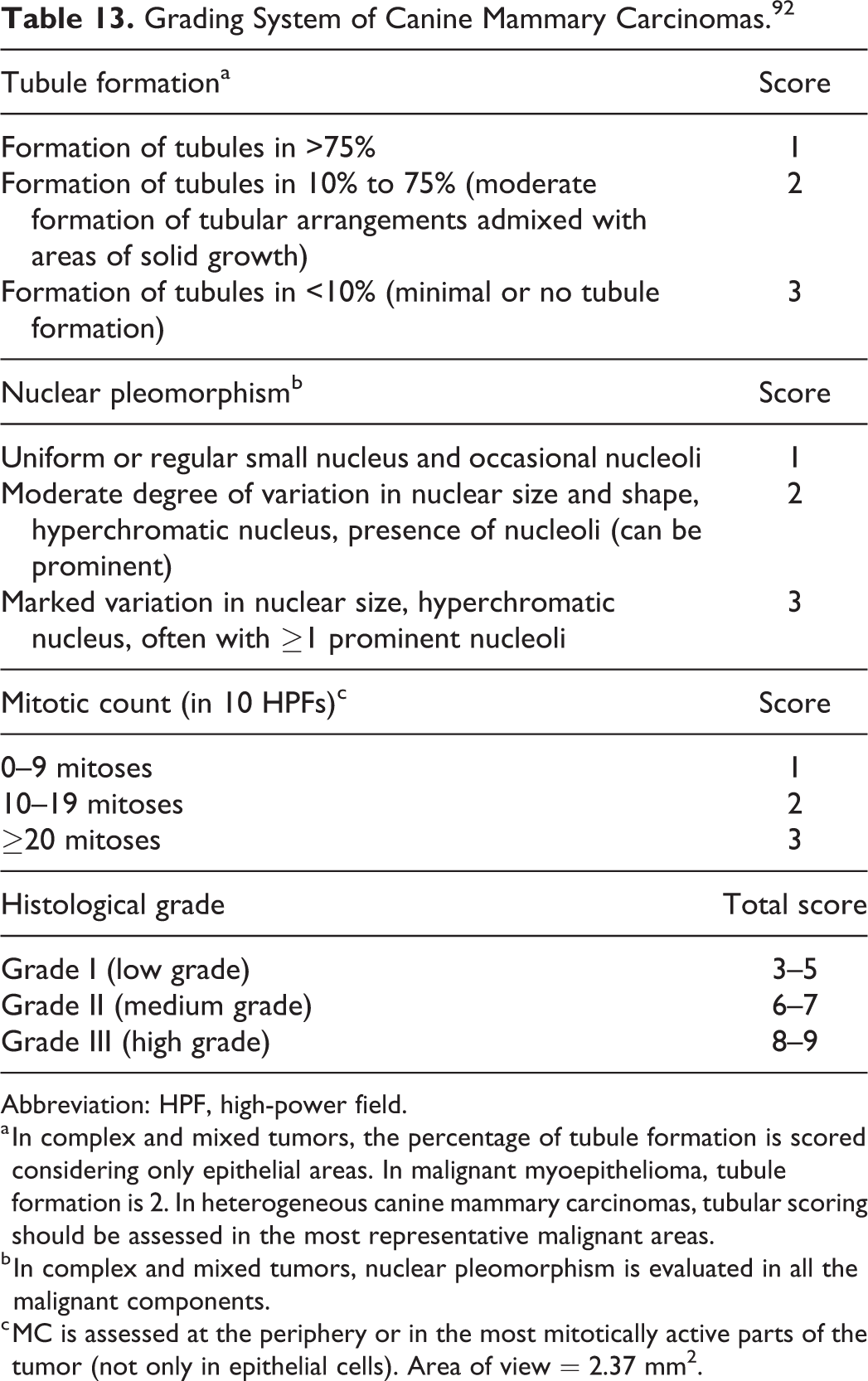
Abbreviation: HPF, high-power field.
a In complex and mixed tumors, the percentage of tubule formation is scored considering only epithelial areas. In malignant myoepithelioma, tubule formation is 2. In heterogeneous canine mammary carcinomas, tubular scoring should be assessed in the most representative malignant areas.
b In complex and mixed tumors, nuclear pleomorphism is evaluated in all the malignant components.
c MC is assessed at the periphery or in the most mitotically active parts of the tumor (not only in epithelial cells). Area of view = 2.37 mm2.
Currently, there is no agreement regarding the incidence of the Peña grading categories in CMCs. This is likely caused by intrinsic differences in the study populations investigated. 13,82,92,102,109,118 Different criteria to distinguish adenomas from carcinomas may also impact the incidence of grade I CMCs in the literature, since different criteria may lead to classification of adenomas as low-grade carcinoma. 13,82,102 The ability of the Peña system to predict the clinical outcome in dogs with mammary carcinoma has been demonstrated in retrospective 82,109 and prospective studies, 13,16,92,102 with some authors identifying the histological grade as an independent predictor of patients’ survival. 16,82,92 Consistently among the studies, grade I and grade III tumors show the longest and shortest survivals, respectively. 13,82,92,109 This is likely because grade I tumors have a lower tendency to metastasize to distant organs and recur compared to grade III tumors (metastatic rate: 19% for grade I vs 87% for grade III; recurrence rate: 12% for grade I vs 32% for grade III). 92,102,118 Most studies have failed to demonstrate a significant difference in survival between grade I and grade II CMCs, opening the debate as to whether the Peña system should be converted into a 2-tier grading scheme. 102,109 However, there is some evidence that grade II tumors have the ability to spread to regional lymph nodes and this represents an intermediate risk between grade I and grade III forms. 103 Moreover, one study showed that the 3-tier system works better than a 2-tier system for the prognosis of CMCs (low and high grades were determined by the final score of the Peña system). 109 Further investigations on the clinical significance of the grade II category are needed.
Taking into account the increasing use of the Peña system, it should be noted that there is no available information on the interobserver agreement in its application, as recently done for histological grading schemes of other canine neoplasm. 57,134,137 Finally, it is important to stress that the histological grade is only one of the recognized prognostic factors in dogs with CMCs. Other factors include tumor size, clinical stage, histological subtype, and histological evidence of infiltrative tumor growth and lymphovascular invasion. 49,92,103,109 Grade III CMCs more commonly undergo lymphatic invasion than grade II and grade I CMCs. 103
There are no studies directly comparing cytological features of CMCs with histological grading, but a few studies evaluated the utility of morphometric analysis in increasing the diagnostic sensitivity of cytology in determining the malignancy of a lesion. 33 In the last 15 years, an attempt to better define cytological criteria of malignancy in cytological samples of canine mammary lesions has been made. 33,96,116 A single study evaluated cellular morphometry on cytological samples for correlation with histological grade and clinical outcome and applied the Robinson’s cytological grading system for invasive ductal carcinoma in women. 33 The cytomorphologic criteria were scored 1 to 3 and included pleomorphism, hypercellularity, anisokaryosis, increased nuclear to cytoplasmic ratio, prominent or multiple nucleoli, nuclear molding, chromatin clearing and clumping, abnormal multinucleated cells, and mitotic activity. 33 The authors found a higher risk of metastasis and shorter survival for dogs with Robinson grade II or III tumors. Concerning is the relatively high rate of false negatives, which might lead to undertreatment if cytology were to be used in the initial planning. 33 Unfortunately, the case selection was based on cytology and only CMCs showing evident cytological criteria of malignancy were included, potentially leading to the exclusion of histological grade I CMCs. This might have introduced a bias, since the performance of the Robinson’s cytological grading system might not have been studied across the full spectrum of CMCs. 33 Further studies are needed to clarify the utility and reliability of cytological grading of CMCs in the routine diagnostic setting.
Summarizing, the Peña grading system is a useful tool in the prognostication of CMCs, especially when considered together with other prognostic variables.
Feline Mammary Carcinomas
Feline mammary tumors are less common and more uniform in terms of histomorphology and biological behavior compared to those of dogs. Most feline mammary tumors (80% to 90%) are carcinomas (FMC) and have a moderate to high propensity for lymphatic spread. 46 However, survival times vary remarkably and there is a small subset of FMCs that are considerably less aggressive. Therefore, accurate prognostication has important clinical implications. 76,139,141
The NHG developed for human breast cancer has been applied to FMCs for more than 2 decades similarly to those of dogs. 11,18,37,74,103,114,125 The principles of the NHG system work well in cats: as most FMCs are composed solely of epithelial cells, no adaptations to assess the myoepithelial component are considered necessary. 11,18,74,103,114,125 Over the years only small differences in the evaluation of the MC and nuclear pleomorphism have been proposed and most studies agree in classifying the majority of malignant FMCs as grade II or III carcinomas. 11,18,74,103,114,125 The value of the NHG method to predict survival in cats with mammary carcinomas has been demonstrated in various retrospective and prospective studies and in one multivariate analysis in which the most favorable and worst outcomes have been shown for grade I tumors and grade III tumors (0% and 90% to 100% 1-year tumor-related death rate, respectively). 11,18,74,103,114,125 The prognostic significance of the grade II category is less certain since, as in dogs, some studies have found a similar survival in grade I and II FMCs and others in grades II and III. 18,24,76,114 Data on recurrence rates and metastatic rates for the different grades of FMCs are currently lacking.
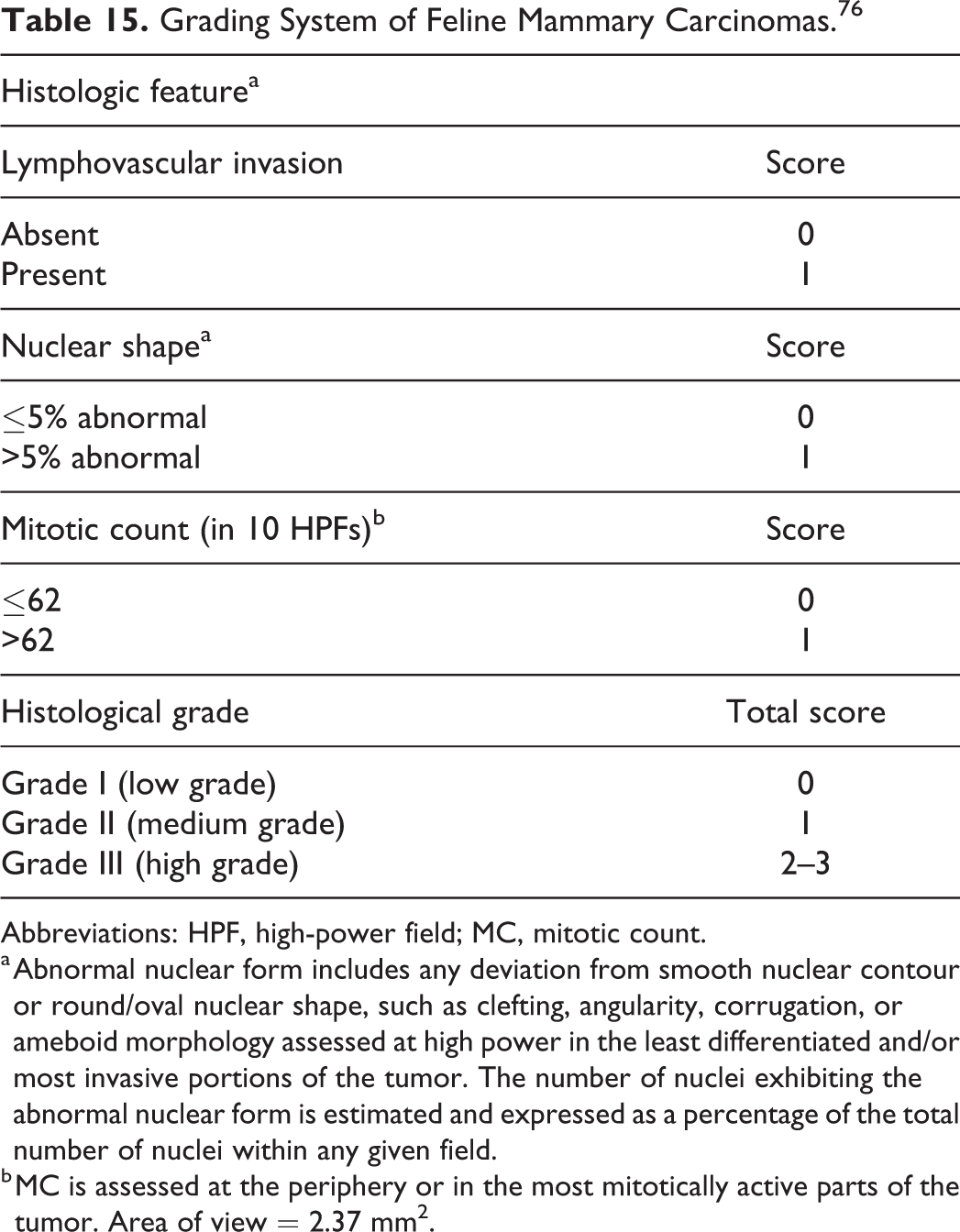
Recently, modification to the MC cutoffs of the NHG scheme has been proposed to better fit with the wide range and high numbers of mitoses in FMCs (Table 14), leading to a better performance in predicting their behavior. 24,76 In addition, in 2015, a new 3-tier grading scheme for FMCs was developed (Mills system), based on histological criteria found to be independent prognostic factors: lymphovascular invasion, MC, and nuclear shape (Table 15). With the Mills system, statistically significant differences have been found between all grades in terms of median overall survival (31, 14, and 8 months for grades I, II, and III, respectively). 76 This system should be further validated in other studies along with the effect of the size of the area evaluated on the assessment of lymphovascular invasion. Currently, there is no consensus on which grading scheme should be used for FMCs. Given that the NHG method has been successfully used for many years, it is the opinion of the authors that this method should not be abandoned and may be used together with the Mills system. The interobserver variability associated with these 2 grading schemes should be explored.
Grading System of Feline Mammary Carcinomas According to the Nottingham Human Grading System. 37
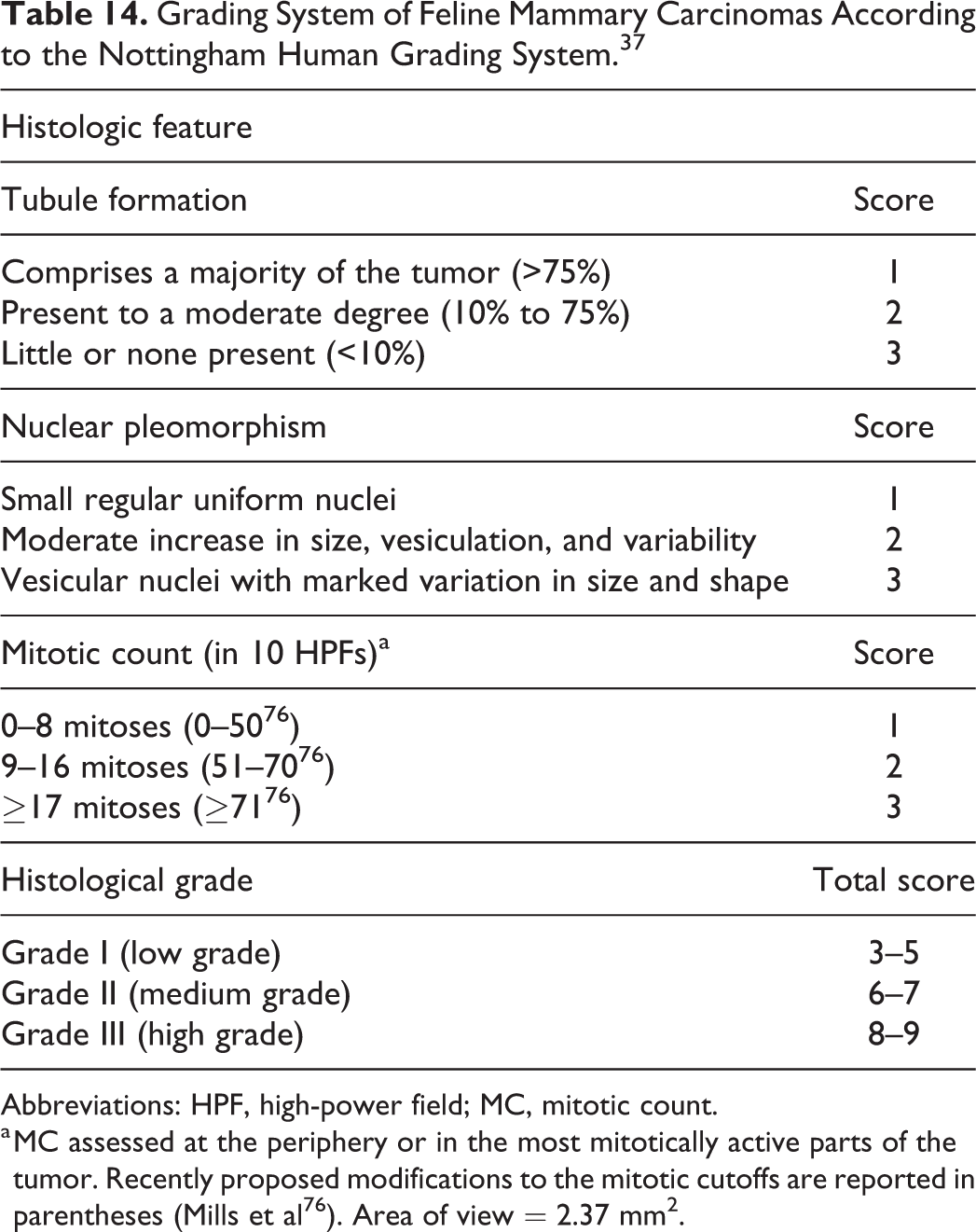
Abbreviations: HPF, high-power field; MC, mitotic count.
a MC assessed at the periphery or in the most mitotically active parts of the tumor. Recently proposed modifications to the mitotic cutoffs are reported in parentheses (Mills et al 76 ). Area of view = 2.37 mm2.
Grading System of Feline Mammary Carcinomas. 76
Abbreviations: HPF, high-power field; MC, mitotic count.
a Abnormal nuclear form includes any deviation from smooth nuclear contour or round/oval nuclear shape, such as clefting, angularity, corrugation, or ameboid morphology assessed at high power in the least differentiated and/or most invasive portions of the tumor. The number of nuclei exhibiting the abnormal nuclear form is estimated and expressed as a percentage of the total number of nuclei within any given field.
b MC is assessed at the periphery or in the most mitotically active parts of the tumor. Area of view = 2.37 mm2.
Canine Pulmonary Carcinoma
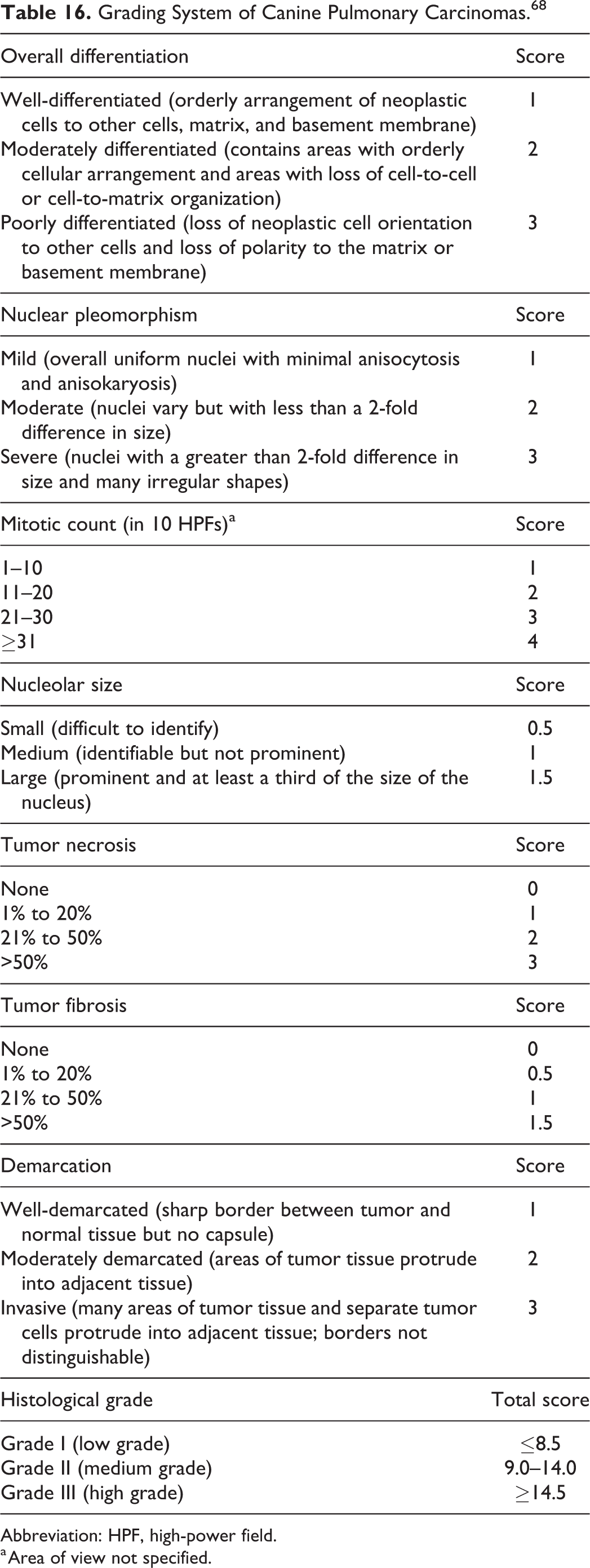
Grading of canine pulmonary carcinomas employs a scoring system including overall differentiation, nuclear pleomorphism, MC, nucleolar size, tumor necrosis, tumor fibrosis, and demarcation. The total histological score is divided into 3 grades (Table 16). 61,68 In a study on 67 canine pulmonary carcinomas, dogs with grade I tumors had significantly longer median survival time and disease-free interval than those with grade II or grade III tumors. 68 Further studies should be performed to confirm the prognostic significance of this grading.
Grading System of Canine Pulmonary Carcinomas. 68
Abbreviation: HPF, high-power field.
a Area of view not specified.
Feline Pulmonary Carcinoma
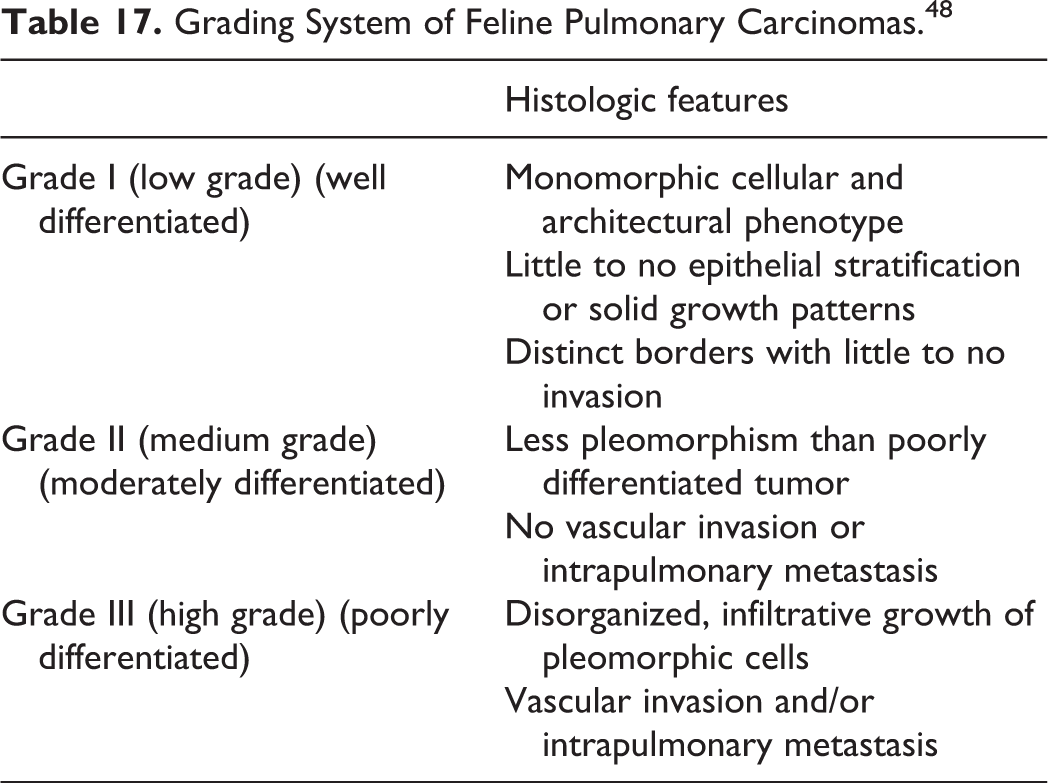
Feline pulmonary carcinomas are classified into 3 grades according to their degree of differentiation (Table 17). 48 In one study, cats with grade II tumors had a significantly longer median survival time compared to those with grade III tumors. 48 In a more recent study, cats with grade I tumors had a significantly longer median survival time compared to cats with grade II and grade III tumors. 67 The median survival time of grade II tumors was considerably different between the 2 studies (698 48 and 3 days 67 ), which may be attributed to subjective interpretation of the grading criteria and to the small sample size, including 12 and 5 grade II tumors, respectively. Another difference between the 2 studies was completeness of resection of the tumor, which was accomplished in all cases in the initial study, whereas the more recent study did not report the completeness of resection and included several patients with advanced disease. 48,67 Last, a third study on 28 cats applied the same grading system and found a significantly longer survival time in grades I and II tumors (730 days) compared to grade III (105 days). 84 Overall, the 3 papers agreed in indicating a progressive reduction of survival time with increased grade. Nevertheless, because of discrepancies in median survival times for the different categories and the small sample size of the studies, the prognostic value of this grading system should be taken with caution until larger studies are performed.
Grading System of Feline Pulmonary Carcinomas. 48
Canine Urothelial Carcinoma
Urothelial carcinoma (transitional cell carcinoma) of the urinary bladder and urethra is most common in the dog. 117 The grading scheme, especially for the dog, has been based largely on the WHO histological criteria for human urothelial carcinomas. However, since the range of urothelial proliferative lesions is greater in humans than in domestic animals, it is unclear how useful the human grading system is in domestic animals. 72 As such, newly proposed grading criteria for urothelial tumors in domestic animals simplifies the histological classification scheme by assigning 2 tumor types: urothelial papilloma and urothelial carcinoma; the latter is divided into low- and high-grade variants. High-grade urothelial carcinomas are defined by features of malignancy including atypia, cellular and nuclear pleomorphism, mitotic activity, deeper invasion, and lymphovascular invasion. 72 Specific cutoffs for the MC are not available, and studies assessing its prognostic relevance are lacking. Thus, prospective studies determining the relationship between low- and high-grade features and patient outcome represent the next logical step before the application of this grading in a diagnostic setting.
Canine Renal Cell Carcinoma
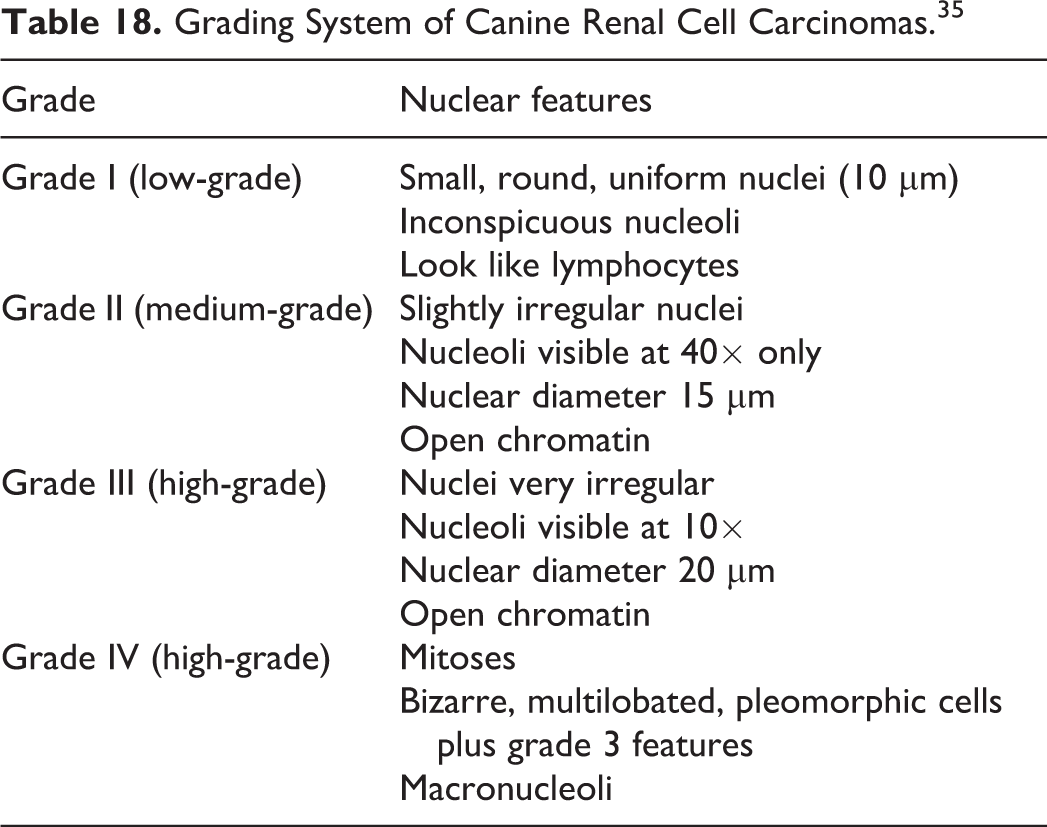
The Fuhrman grading system for renal cell carcinoma is based solely on nuclear and nucleolar morphology (Table 18). 17,35 It has been applied to the dog in 2 studies, including 64 and 70 cases. These studies obtained contradictory results of its prognostic value, perhaps because the studies included cases undergoing adjuvant therapies with different protocols. 17,35 Both studies reported an association of MC with survival, but MC was nevertheless not a part of the grading system. 17,35 MC was assessed in 10 consecutive HPFs in the areas of highest mitotic activity, equating the 2.37 mm2 standard area, and were categorized into 3 groups: <10, 10 to 30, >30. 17 Cases with a MC higher than 30 had a lower survival time (120 days) compared to cases with MC <10 or 10 to 30 (545 and 532 days, respectively). 17 A variation of the Fuhrman grading system has been proposed in human medicine, but it has never been validated in veterinary medicine. 26 Until studies on cases treated with homogeneous protocols are performed, the assessment of MC seems to be the more reliable prognostic parameter for renal cell carcinoma in the dog.
Grading System of Canine Renal Cell Carcinomas. 35
Canine Prostatic Carcinoma
A modified Gleason grading system of human prostatic carcinoma has been proposed for canine prostatic carcinoma. 88 Tissue samples collected during necropsy, prostatectomy, and biopsy were examined. Architectural patterns observed on hematoxylin-eosin-stained sections at low magnification are scored from 1 to 5 (Table 19). Scores of the two most prevalently observed histological patterns are added to obtain a total Gleason score. If a histological pattern with higher score than the primary and secondary scores are observed, the higher score is assigned as the secondary score. For example, if score 4 is the most prevalent pattern and a minor component of score 5 is observed, regardless of the second most prevalent pattern (1, 2, or 3), the total Gleason score is 9 (4 + 5). If the tumor tissue is composed of only one histological pattern, the score is doubled to obtain the total Gleason score. Various histologic growth patterns in canine prostatic carcinoma can be evaluated using this scoring system (ie, solid, cribriform, and papillary).
Grading System of Canine Prostatic Carcinomas According to the Adaptation of the Gleason Score.a,88
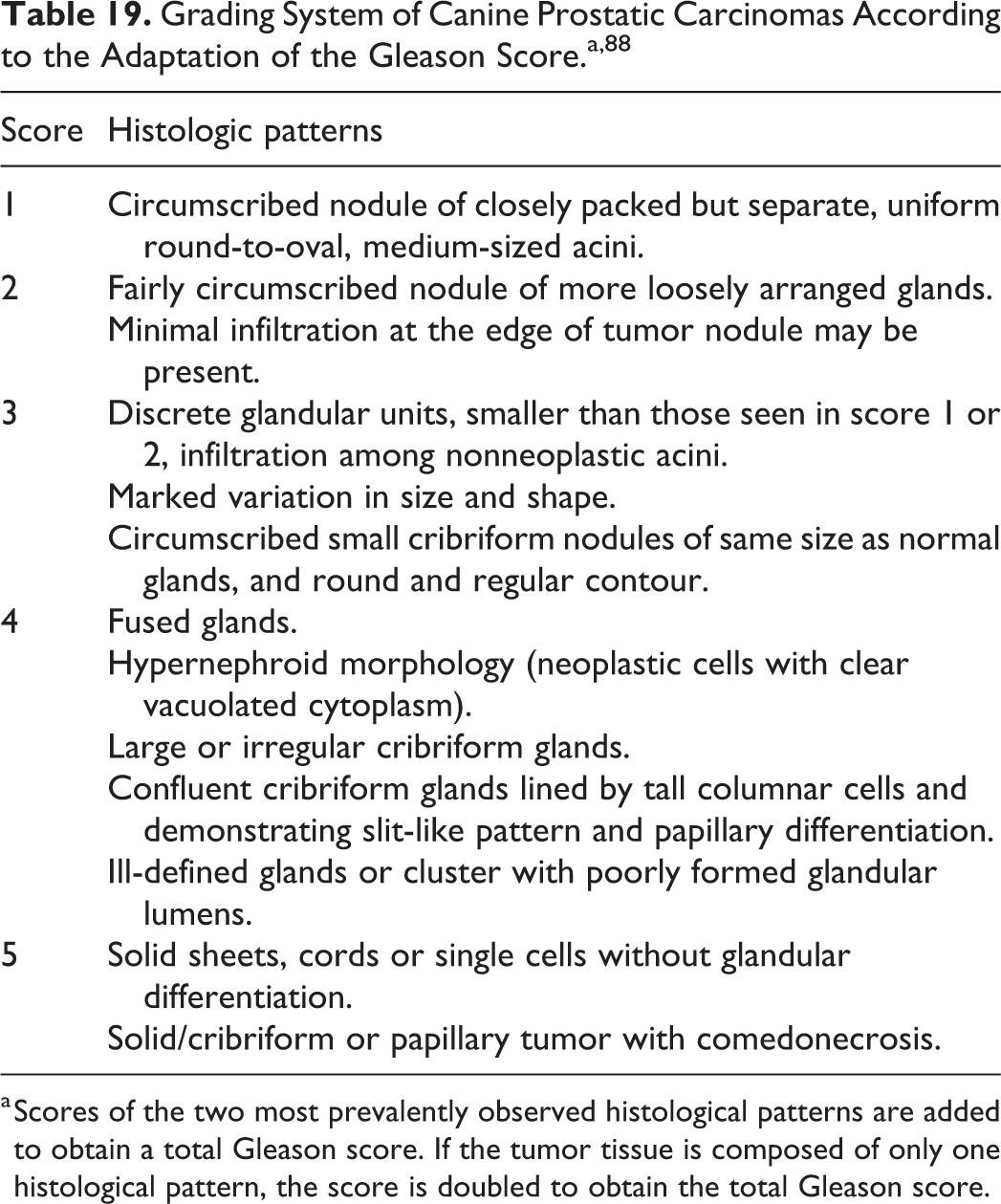
a Scores of the two most prevalently observed histological patterns are added to obtain a total Gleason score. If the tumor tissue is composed of only one histological pattern, the score is doubled to obtain the total Gleason score.
In humans, higher Gleason scores are associated with more aggressive behavior of the tumor and worse prognosis. In animals, there is no information about the correlation between this histological grade and prognosis. In humans, it is not recommended to grade urothelial carcinoma of the prostate. In dogs, urothelial carcinoma and mixed urothelial and adenocarcinoma of the prostate are common, and differentiating them from true prostate adenocarcinoma is often difficult. 87 Thus, inclusion criteria (ie, which tumor type should be graded) are necessary in order to use the grading system in routine veterinary practice.
Canine Cortisol-Secreting Adrenocortical Tumors
A scoring system, named the Utrecht score, was recently developed in a retrospective study of 50 canine cortisol-secreting adrenocortical tumors. 108 This system includes Ki67 labeling index, necrosis, and vacuolation of the cytoplasm. Ki67 labeling index was assessed as percentage of Ki67-positive neoplastic cells on the total of counted cells, counting a minimum of 1000 cells in areas of highest mitotic activity. 108 The Utrecht score is obtained by adding the Ki67 labeling index, plus 3 points when necrosis is present, and 4 points when at least 33% of neoplastic cells have a clear or vacuolated cytoplasm. 108 Stratifying the cases in 3 groups based on specific cutoffs (<6; 6–10; >10), the Utrecht score is associated with overall survival (>60, 51.5, and 14.4 months, respectively). 108
Canine Gliomas
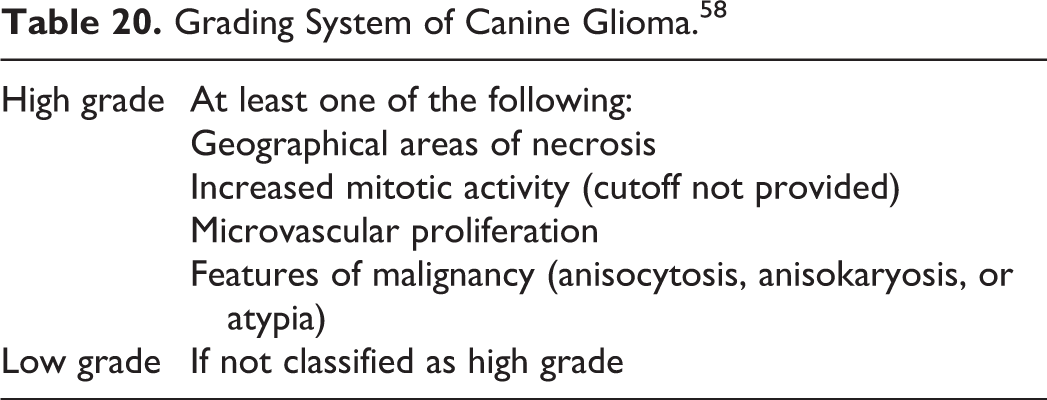
In humans, the diagnosis and prognosis of meningioma and glioma are closely tied to tumor grade, often augmented by molecular data. A grading scheme was proposed for canine glioma that simplified and codified the histological characteristics (Table 20). 58 This canine glioma grading scheme allows for 3 distinct diagnoses—astrocytoma, oligodendroglioma, and undefined glioma—that are defined based on the predominant cell pattern or, in the case of undefined glioma, an undefined cell pattern or a similar distribution of oligodendroglial and astrocytic morphology. These are further divided into low- and high-grade tumors. High-grade gliomas in the dog are diagnosed by the presence of at least one of the following: geographical areas of necrosis with or without pseudopalisading, increased mitotic activity, microvascular proliferation, or features of malignancy (anisocytosis, anisokaryosis, or atypia). 58 Importantly, the degree of invasion does not determine if a tumor is low or high grade. The lack of a cutoff for the assessment of mitotic activity may limit the use of this grading system. This grading scheme was determined using predominately necropsy samples 58 so there is no information about the correlation between histological grade and prognosis. Therefore, application to biopsies that can be studied prospectively is of utmost importance in determining if the grade is correlated with outcome.
Grading System of Canine Glioma. 58
Canine Meningiomas
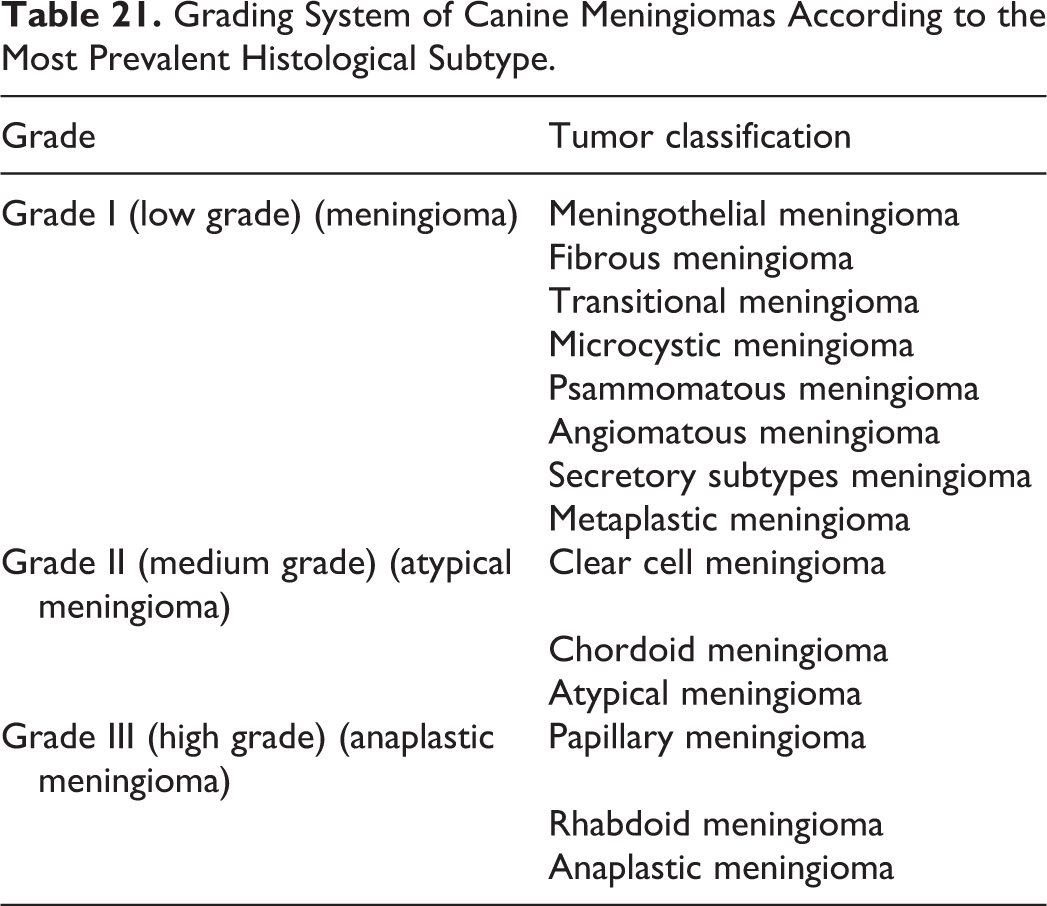
Canine meningiomas exhibit various histological patterns that are similar to human meningiomas. 75 Application of the WHO grading of human meningiomas has been proposed for grading canine meningiomas. 14,52 In the WHO grading system, tumors are graded according to their predominant histological subtype (Table 21), 63 except that regardless of histological subtype, atypical meningioma (grade II) is assigned if any of the following features are found: brain invasion, MC of 4 to 19 per 10 HPF (400×), or at least 3 of the 5 following histological features: necrosis, sheeting (loss of whirling or fascicular architecture), prominent nucleoli, high cellularity, and small cells (tumor clusters with high nuclear/cytoplasmic ratio). Anaplastic meningioma (grade III) is assigned to meningioma with overt malignant features (resembling carcinoma, melanoma, or sarcoma) or MC of 20 or more in 10 HPF (400×). Unfortunately, specific guidelines on the assessment of these morphological parameters are lacking and grading assessment is therefore highly subjective.
Grading System of Canine Meningiomas According to the Most Prevalent Histological Subtype.
To date, correlation between WHO grading and tumor behavior has not been validated in canine meningioma. One study demonstrated that canine papillary meningioma has aggressive behavior with high recurrence rate, analogous to human papillary meningioma (WHO grade 3). 65 Criteria of atypical meningioma, such as MC and necrosis, may need to be reconsidered to fit the biological behavior of canine meningioma. Future studies are needed to overcome these problems and develop a consistent grading system for canine meningiomas that provides relevant prognostic value.
Conclusion
Tumor grading schemes in animals remain inextricably linked to the histopathologic findings because these are the basis of what anatomic pathologists do and are the sample that we are most used to assessing. However, histologic assessment is fraught with subjective challenges including interpathologist variation in MC, degrees of atypia, and pleomorphism. The lack of a detailed description of the methods used to assess some of the histopathological parameters included in the grading systems limits the possibility of applying some of them in diagnostic routine activity. Additional challenges are faced with small sample size or variations in how a sample is trimmed for histologic analysis. This can impact, for example, the estimation of necrosis. Necrosis seems to be assessed mainly at the microscopic level, even if in many studies it is not clearly stated if a gross estimation was performed. A major weakness of the veterinary literature is the accuracy of outcome data (including the impact of euthanasia on the assessment of survival time), mainly because prospective studies in animals are more difficult than in humans. Finally, most tumor grading systems for animals have not been validated by replicating the studies using an independent caseload. Some grading schemes are reported in more than one paper, but studies applying the same method and specifically designed to validating the grading system (Table 22) are rare. 112 Furthermore, several papers apply the same grading but are difficult or unfeasible to compare because of slight differences in the methods (such as endpoint chosen or type of statistical analysis used).
Validation of Grading Systems in Veterinary Medicine.
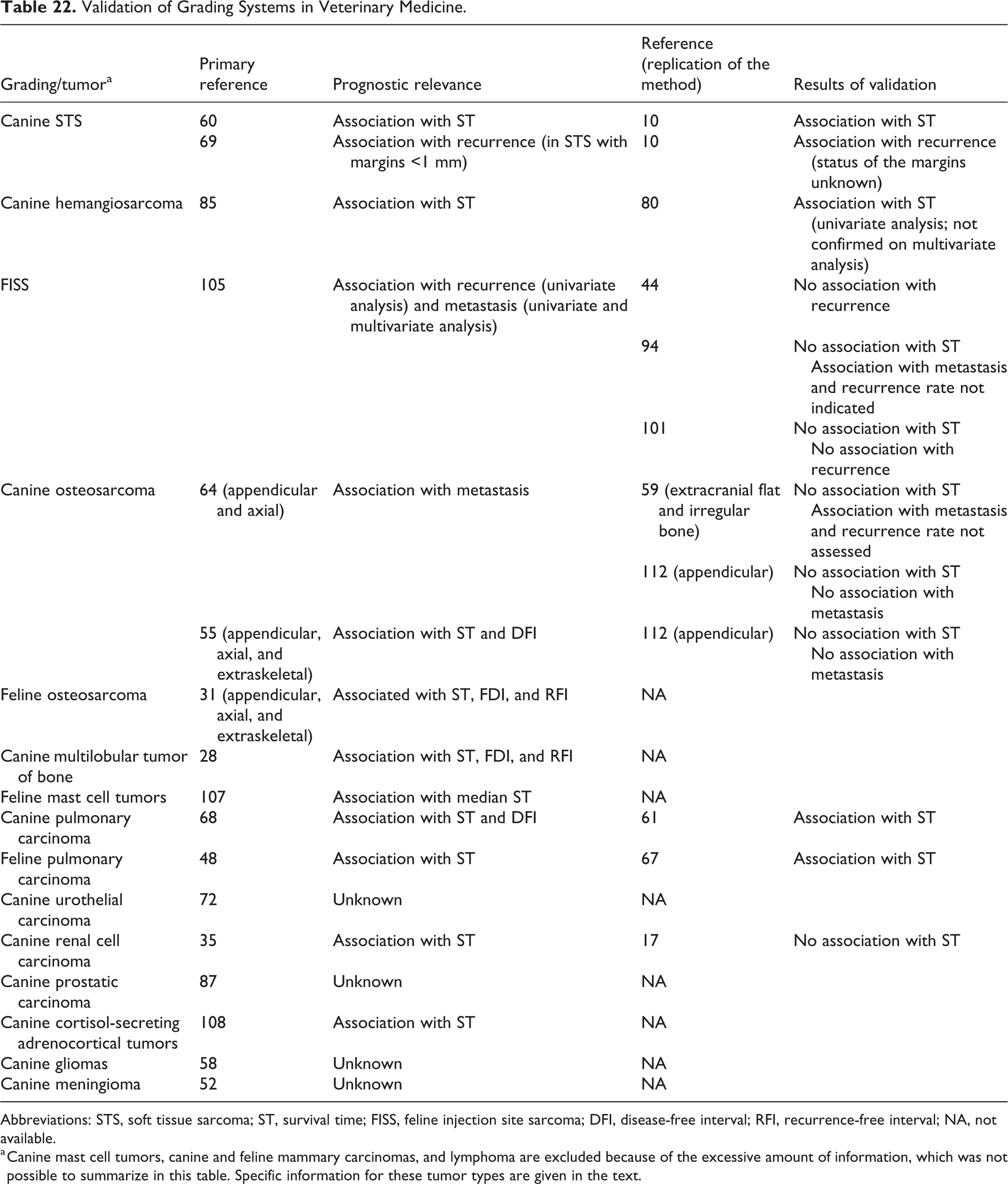
Abbreviations: STS, soft tissue sarcoma; ST, survival time; FISS, feline injection site sarcoma; DFI, disease-free interval; RFI, recurrence-free interval; NA, not available.
a Canine mast cell tumors, canine and feline mammary carcinomas, and lymphoma are excluded because of the excessive amount of information, which was not possible to summarize in this table. Specific information for these tumor types are given in the text.
These issues represent some of the future challenges in veterinary oncological pathology, considering that any grading scheme has clinical usefulness only when correlated to accurately assessed outcome.
In human pathology, histologic grading schemes are being augmented and, in some cases, supplanted by molecular diagnostics that often guide treatment and ultimately prognosis. In the future, veterinary pathology will likely be able to incorporate molecular data with histologic assessment to yield detailed and accurate information regarding the biology of tumors. However, this can only be done through concerted and effective collaborative, multicenter studies that standardize tumor collection and assessment and produce large datasets that serve to guide future research paths. The dog and the cat are effective natural models for many malignancies that afflict human and animals alike and through radical and transformative collaborative research, veterinary pathologists will be at the forefront of the coming molecular wave.
Less emphasis has been paid to developing cytological grading schemes that are predictive of tumor behavior. Given the minimally invasive nature, rapid turnaround time, and lower cost of a find needle aspiration compared to a tissue biopsy, this area warrants further investigation. Those histological grading schemes that heavily weigh features that can only be assessed in tissue sections—such as area of necrosis, blood vessel density, areas of fibrosis, or vascular invasion—could be anticipated to have poor correlation to cytology.
Tumor grading is a powerful and widely used tool to predict tumor behavior and it should be considered in conjunction with other prognostic variables rather than as a single prognostic parameter. It is also pivotal, for both pathologists and oncologists, to be aware of the weaknesses of some of these systems, such as the tumors for which the grade has no or little impact, the controversial data on the prognostic power of some systems, as well as lack of data on methods and reproducibility in some grading schemes. Furthermore, some grading systems (urothelial carcinoma, prostatic carcinomas, gliomas, and meningiomas) currently have unknown significance regarding the clinical outcome. In the authors’ opinion, future studies should focus on addressing the above-mentioned controversies and limitations, fill the gaps in knowledge, and try to overcome common limitations such as the retrospective nature and the lack of uniformity in study design, reporting outcomes, and treatment in order to improve the use and value of tumor grading systems for animals.
Supplemental Material
Supplemental Material, sj-pdf-1-vet-10.1177_0300985821999831 - Review of Histological Grading Systems in Veterinary Medicine
Supplemental Material, sj-pdf-1-vet-10.1177_0300985821999831 for Review of Histological Grading Systems in Veterinary Medicine by Giancarlo Avallone, Roberta Rasotto, James K. Chambers, Andrew D. Miller, Erica Behling-Kelly, Paola Monti, Davide Berlato, Paola Valenti and Paola Roccabianca in Veterinary Pathology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.