
Abstract
Evasion of the immune response is an integral part of the pathogenesis of glioma. In humans, important mechanisms of immune evasion include recruitment of regulatory T cells (Tregs) and polarization of macrophages toward an M2 phenotype. Canine glioma has a robust immune cell infiltrate that has not been extensively characterized. The purpose of this study was to determine the distribution of immune cells infiltrating spontaneous intracranial canine gliomas. Seventy-three formalin-fixed, paraffin-embedded tumor samples were evaluated using immunohistochemistry for CD3, forkhead box 3 (FOXP3), CD20, Iba1, calprotectin (Mac387), CD163, and indoleamine 2,3-dioxygenase (IDO). Immune cell infiltration was present in all tumors. Low-grade and high-grade gliomas significantly differed in the numbers of FoxP3+ cells, Mac387+ cells, and CD163+ cells (P = .006, .01, and .01, respectively). Considering all tumors, there was a significant increase in tumor area fraction of CD163 compared to Mac387 (P < .0001), and this ratio was greater in high-grade tumors than in low-grade tumors (P = .005). These data warrant further exploration into the roles of macrophage repolarization or Treg interference therapy in canine glioma.
Keywords
Gliomas are a group of devastating brain tumors that affect both dogs and humans. 1,3,11,50,64,69,72 They represent approximately 35% of primary intracranial tumors in the dog and are overrepresented in brachycephalic breeds such as the boxer, Boston terrier, and English and French bulldog. 49,64,73 Glioma subtypes in humans include oligodendroglioma, astrocytoma, and glioblastoma, and in dogs are oligodendroglioma, astrocytoma, and undefined glioma. 39,44,49 Median survival for glioblastoma, the most common and most aggressive brain tumor in humans, is approximately 14 months with current standard of care (maximal surgical resection followed by radiation and temozolomide chemotherapy). 70 Median survival for dogs with suspected glioma (based on imaging) receiving radiation therapy is similar, ranging from 9 to 14 months. 5,7,67 Treatment failure in both species occurs due to the failure of local therapy, and neoplastic cells can survive within grossly normal brain parenchyma several centimeters from the main tumor mass. 22,27,81 Therefore, novel therapies for these devastating cancers are desperately needed. One group of treatments that hold tremendous promise are immunotherapies, which have the potential to harness the immune system to seek out and destroy neoplastic cells in brain regions distant from the main tumor mass. An essential function of the immune system is to recognize and eliminate foreign cells. However, a hallmark of cancer is evasion of the immune system, and gliomas are particularly adept at such evasion. 23,28,82 Important components of immune evasion by gliomas in humans include recruitment of regulatory T cells (Tregs) to the tumor and polarization of tumor-associated macrophages toward an M2 phenotype. 54,56,83
The primary function of Tregs is to inhibit the functions of effector immune cells, which prevents the development of autoimmunity in healthy individuals. However, Tregs can be recruited and coopted by tumors, and play a role in glioma pathogenesis by suppressing the adaptive immune response to invading tumor cells. 15,16,25,32,45,54,65 Indoleamine 2,3-dioxygenase (IDO) is an enzyme responsible for the catabolism of tryptophan, an amino acid essential to effector lymphocyte function. 35,89 In addition to tryptophan depletion, tryptophan metabolites, including kynurenine, contribute to Treg expansion and effector T cell suppression. 35,89 Studies in humans and experimental rodent models have shown that IDO is highly expressed in gliomas, contributes to intratumoral Treg expansion, is associated with survival, and may serve as a viable therapeutic target. 29,35,78 –80,89
Macrophages are also increasingly recognized as important in tumor immunology and can be polarized along a spectrum from an M1 to an M2 phenotype. 2 M1 macrophages are associated with a pro-inflammatory, normoxic state, and have antitumor properties associated with longer survival in human glioblastoma patients, while M2 macrophages are associated with an anti-inflammatory, hypoxic state, with pro-tumor functions and shorter survival in these patients. 21,56,83,87 The designation of macrophages as M1/pro-inflammatory or M2/anti-inflammatory would ideally be made using a test of cellular function. However, such tests are difficult to perform when evaluating samples from either human or veterinary patients and surrogate markers of function are frequently used. Calprotectin and CD163 have been used as markers of M1/pro-inflammatory and M2/anti-inflammatory macrophages (respectively) in a number of species, including dogs. 9,13,20,31,53,76,77,85
Successful understanding of canine glioma pathogenesis and implementation of immune therapies will require characterization of the tumor immunological landscape within this species. However, such studies have been limited to date, particularly with regard to microglia, macrophages, and IDO. 1,18,55,63 In this study, our objectives were to characterize the infiltration of canine intracranial gliomas by T cells, B cells, Tregs, microglia, macrophages, M1-like macrophages, and M2-like macrophages, to compare immune cell infiltration between glioma subtypes and grades, and to determine if IDO is expressed in canine gliomas.
Materials and Methods
Sample Preparation and Diagnostic Review
A search was performed for canine glioma cases from the pathology archives at North Carolina State University’s College of Veterinary Medicine spanning years 2006 to 2018. Case demographic data (age at sample collection, weight, sex) and time from death to necropsy examination were obtained from the medical records. Brains were fixed whole in 10% neutral buffered formalin (standard protocol of 48–72 hours), routinely processed for histology, and embedded in paraffin. Paraffin-embedded samples were sectioned at 5 μm, mounted on charged glass slides, stained with hematoxylin and eosin (H&E) or used for immunohistochemistry, and digitally scanned to an electronic database (Aperio AT Turbo, Leica Biosystems).
A panel of 4 board-certified (American College of Veterinary Pathologists) veterinary anatomic pathologists (GAK, DEM, ADM, DAT) and one physician neuropathologist (CRM) independently reviewed the H&E-stained sections, as well as immunohistochemistry for oligodendrocyte transcription factor (Olig2), glial fibrillary acidic protein (GFAP), 2′,3′-cyclic-nucleotide 3′-phosphodiesterase (CNPase), and Ki-67. Pathologists diagnosed each case as oligodendroglioma, astrocytoma, undefined glioma, or other (non-glioma) and also determined grade (low-grade or high-grade) for cases diagnosed as glioma. Classification was based on diagnostic criteria from recently published consensus guidelines for canine glioma. 39 Briefly, tumors were classified as oligodendroglioma or astrocytoma if >80% of the tumor reflected characteristics typical of these neoplasms (Suppl. Figs. S1, S2). Undefined glioma was diagnosed if features of both neoplasms were present and the minority phenotype composed more than 20% of the tumor. Features that designated a high-grade status were geographic necrosis (Suppl. Fig. S3), microvascular proliferation (Suppl. Fig. S4), presence of mitoses, overt cellular or nuclear pleomorphism, or atypia. A majority diagnosis (agreement between ≥3 pathologists) was required to define each tumor with a glioma subtype and corresponding grade and to include further analysis for immune cell infiltration and IDO expression.
Case Details and Tumor Samples
A majority diagnosis of glioma subtype and grade was achieved for 73 cases, which included 9 low-grade oligodendrogliomas (12%), 8 low-grade astrocytomas (11%), 44 high-grade oligodendrogliomas (60%), 10 high-grade astrocytomas (14%), and 2 high-grade undefined gliomas (3%). Given the low prevalence of undefined gliomas, comparisons between tumor subtypes were limited to oligodendrogliomas and astrocytomas. Undefined gliomas were included in statistical analyses when comparing data across tumor grades. All tumor samples were collected at necropsy. The time from death until necropsy, which was available for 69 cases, ranged from 0 to 120 hours (0–24 hours, n = 24; 24–48 hours, n = 39; 48–72 hours, n = 4; 72–96 hours, n = 1; 96–120 hours, n = 1). The mean age of the cases was 8.2 years (range 2.9–14.5 years) and the mean body weight was 23.6 kg (range 3.7–50.9 kg). There were 39 spayed females, 28 castrated males, and 6 intact males represented.
Immunohistochemistry
Slides were deparaffinized in xylene, and the tissues were rehydrated through graded ethanols. Antigen retrieval was performed using various buffers within a heated Decloaker pressure chamber (Biocare Medical) or using an enzymatic technique, depending on antibody requirements (Suppl. Table S1). Endogenous peroxidase was blocked with 3% hydrogen peroxide, and nonspecific binding was blocked by incubating slides with normal serum from the appropriate species. Immunohistochemistry was performed using primary antibodies against a variety of immune cell markers, and positive control tissue was canine in origin (Suppl. Table S1). Immune cell markers and their intended targets were CD3 (T cells), forkhead box 3 (FoxP3, Tregs), CD20 (B cells), Iba1 (macrophages/microglia), calprotectin (Mac387, M1-like macrophages), CD163 (M2-like macrophages), and IDO. Isotype-matched antibodies were used for negative control tissues. 33 Antigen-antibody complexes were detected using 3,3-diaminobenzidine (DAB; Dako, Agilent). Slides were counterstained with hematoxylin, dehydrated in graded ethanols, cleared with xylenes, and cover-slipped.
Immune Cell Infiltrate Analysis
The immunohistochemically labeled brain tumor slides were scanned at 200× magnification using a whole slide scanner (Hamamatsu Nanozoomer NDP.scan) and imported into a database for quantitative image analysis, using commercially available software (Visiopharm Version 2020.05.0.7761, Visiopharm). A region of interest (ROI) was manually generated around the entire tumor within each section, excluding areas of geographic necrosis.
Immunolabeled cells were characterized by DAB binding and hematoxylin counterstaining. Labeled cells were segmented from negative cells, fibers, and background using an artificial intelligence machine learning decision forest classifier or by applying a threshold (the method was dependent on the cellular marker), and processing steps were performed to separate cells that were close together and count them as individual cells (Suppl. Figs. S5–S8). False positives based on the size of the cell of interest were removed, as was background staining and artifact.
For CD3, FoxP3, and CD20, cell counts were derived by dividing the total immunolabeled cell count by the total area of the defined ROI (cells/μm2). This was then converted to a standard high-powered light microscopy field (HPF; 400×, FN 22 mm, 0.237 mm2). 47 Manual cell counts per 10 HPF in each tumor, as well as manual assessment of cellular and nuclear morphology of immunolabeled cells, were also performed as a means of quality control.
Although the algorithms for Iba1, Mac387, and CD163 were robust in identifying immunolabeled cells, frequent dense clustering of cells created difficulty in separating cells and establishing accurate cell counts. Therefore, in order to more accurately capture microglial and macrophage infiltration, area fractions were determined for Iba1, Mac387, and CD163 by dividing the immunolabeled area by the total ROI area. Manual counts, as well as manual assessment of cellular and nuclear morphology, of immunolabeled cells were performed as a means of quality control. In addition, the preponderant microglial phenotype (ramified, reactive, or amoeboid) was recorded manually for each tumor.
Assessment of IDO immunolabeling was performed manually. Cases were recorded as positive or negative with zero threshold.
Statistical Analysis
Descriptive statistics were generated for dog ages and weights. A D’Agostino-Pearson test for normality was used to determine that the cell counts and area fractions did not follow Gaussian distributions, and nonparametric tests were used to compare differences in cell populations across tumor subtypes and grades. Comparisons made between 2 groups were evaluated using a Mann-Whitney test, and comparisons between greater than 2 groups were evaluated using a Kruskal-Wallis test. Comparisons between paired samples (Mac387 and CD163) were evaluated using a Wilcoxon matched-pairs signed rank test. The correlation between FoxP3 and CD163 counts was performed using Spearman correlation testing. Statistical calculations were performed using commercially available software (Graphpad Prism), and a P value <.05 was considered to be significant.
Data Availability
The raw data analyzed in this study are not available as supplemental materials, though requests to the corresponding author can be made for those interested in further information.
Results
Lymphocyte and IDO Immunohistochemistry
Subcellular localization of antibody immunolabeling was appropriate for all antibodies (membranous for CD3 and CD20; nuclear for FoxP3; cytoplasmic for IDO). Cells immunolabeled for each of the lymphocyte markers were detected in all tumors. CD3+ lymphocytes were generally dispersed throughout the tumors (Fig. 1), though they were also present in dense clusters around foci of microvascular proliferation (Fig. 2) and occasionally surrounding normal blood vessels. FoxP3+ lymphocytes were quite variable in number and these cells were generally scattered throughout the tumors (Fig. 3). They occasionally extended beyond the tumor margin into the adjacent brain but were not otherwise detected in normal brain (Fig. 4). CD20+ lymphocytes were scattered throughout the tumor or limited to perivascular aggregates (Fig. 5). Manual cell counts of lymphocyte subtypes concorded with the automated counts (data not shown).
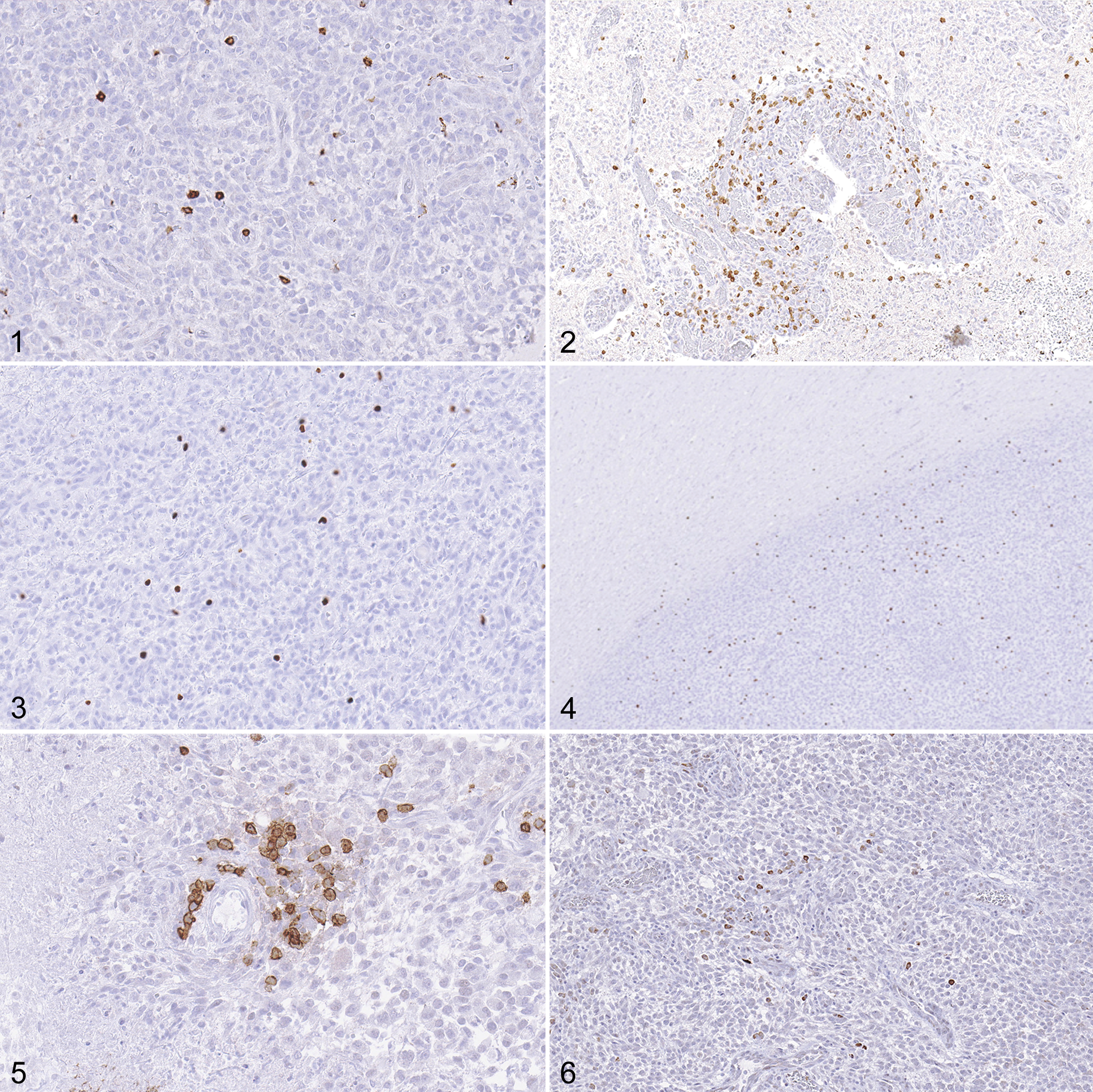
High-grade oligodendroglioma, brain, dog. Immunohistochemistry.
All cells immunolabeled for IDO were morphologically consistent with neoplastic glial cells, and immunolabeled cells were detected in 8/73 tumors (11%), comprising 7/44 (16%) high-grade oligodendrogliomas and 1/10 (10%) high-grade astrocytomas. Immunolabeled cells were generally sporadic, although they occasionally occurred in clusters (Fig. 6). The distribution of FoxP3 cell counts per HPF in IDO+ tumors was 0.2, 0.3, 0.4, 0.9, 1.1, 2.1, 2.1, and 58.1. The tumor with 58.1 FoxP3+ cells per HPF was a high-grade astrocytoma, and the remainder of the tumors were high-grade oligodendrogliomas.
No significant differences were found in CD3+ cell counts between different tumor subtypes (P = .67) or grades (P = .10, Fig. 7). There was a significant difference in FoxP3+ lymphocyte counts between different tumor grades, with increased counts in high-grade tumors (Fig. 8, P = .006). There was no difference in FoxP3+ lymphocyte counts between oligodendrogliomas and astrocytomas (P = .33). No significant differences were found in CD20+ cell counts between different tumor subtypes or grades (Fig. 9, P = .14 and P = .18, respectively).
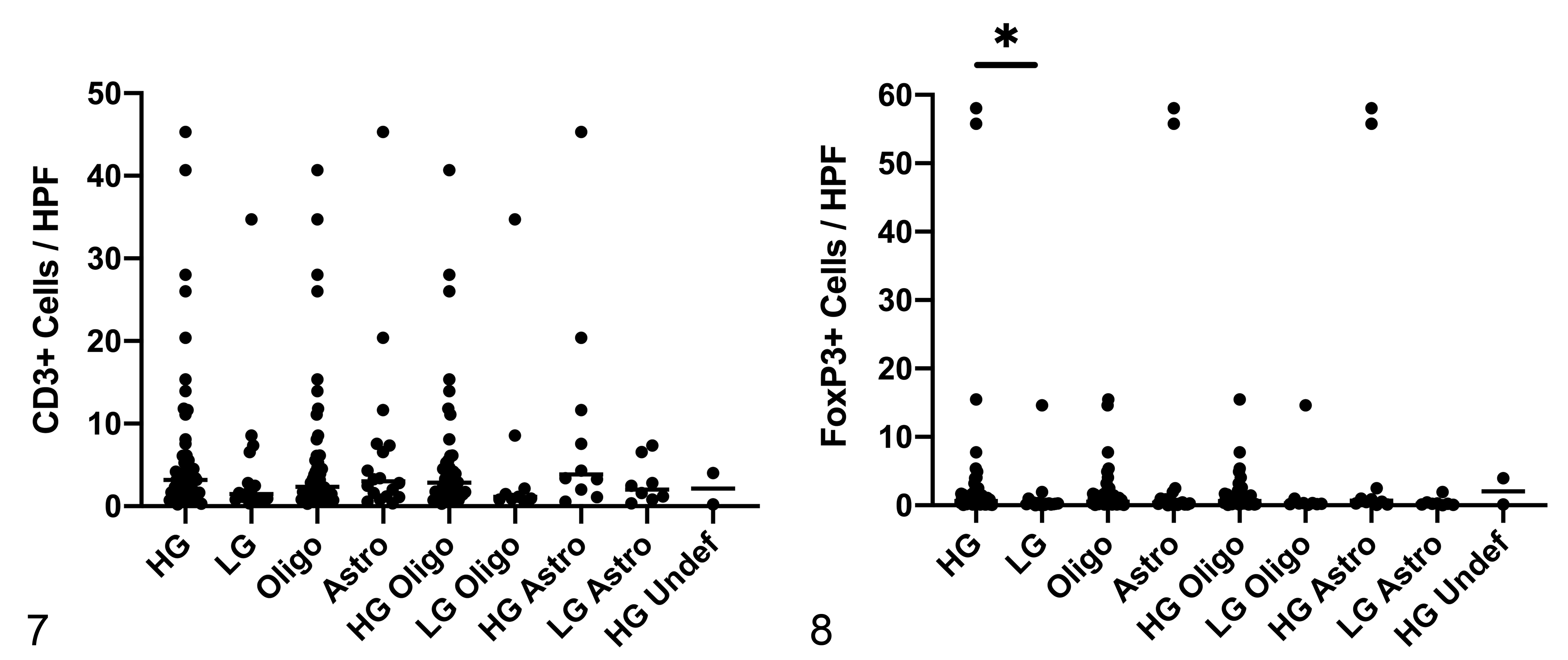
Numbers of CD3+ and Foxp3+ cells in canine glioma. HG = high-grade; LG = low-grade; oligo = oligodendroglioma; astro = astrocytoma; undef = undefined glioma.
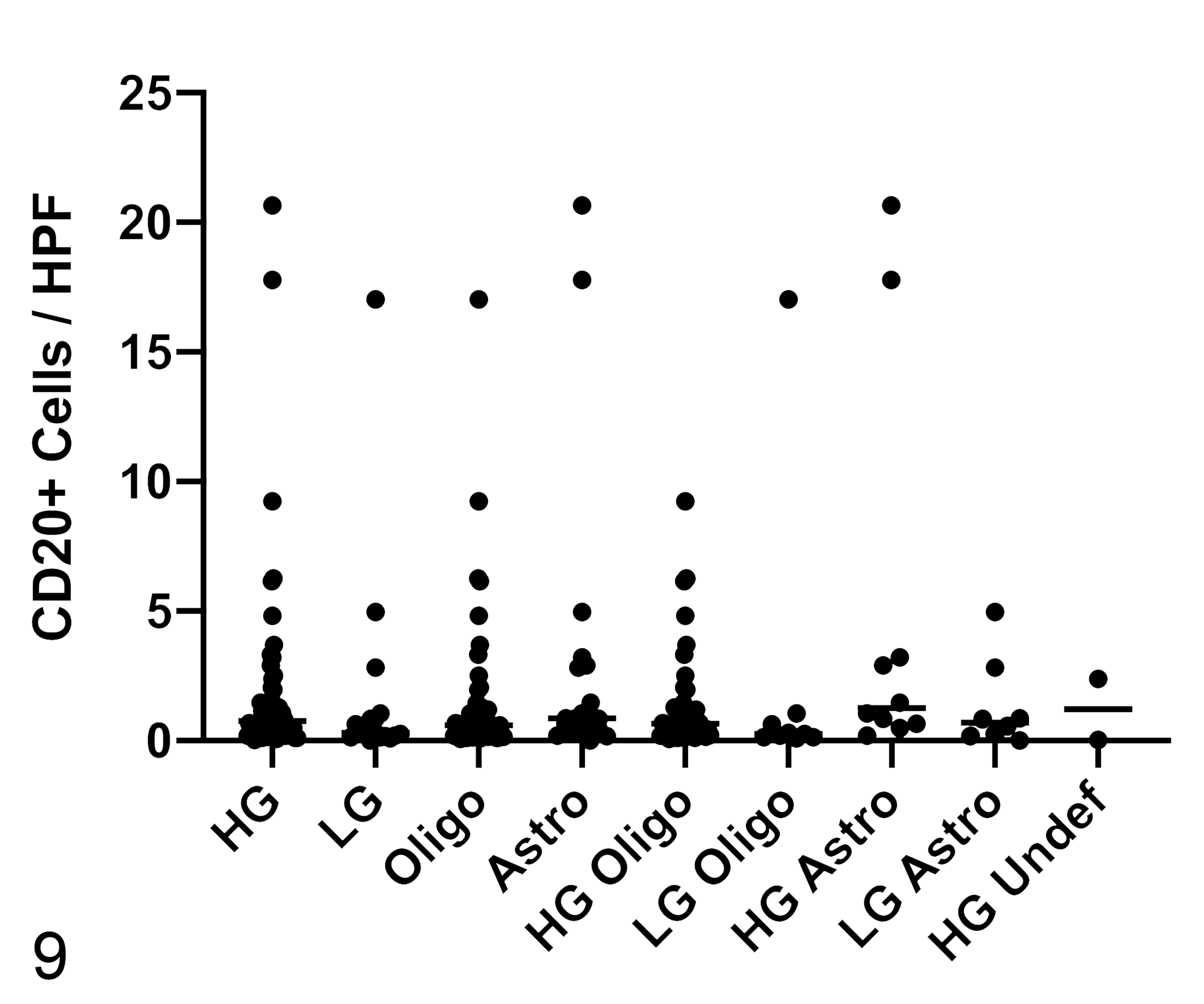
Numbers of CD20+ cells in canine glioma. HG = high-grade; LG = low-grade; oligo = oligodendroglioma; astro = astrocytoma; undef = undefined glioma. There are no significant differences in CD20+ cell counts between tumor subtypes or grade. Bar = median.
Microglia and Macrophage Immunohistochemistry
Subcellular localization of antibody immunolabeling was appropriate for all antibodies (cytoplasmic for Iba1 and Mac387; membranous for CD163). Cells immunolabeled for each of the macrophage markers were detected in all tumors.
Numerous Iba1-immunolabeled macrophages and microglia were scattered throughout the tumors. Ramified microglia had small cell bodies and multiple long, branching processes (Fig. 10). Reactive microglia were similar to ramified cells, though they had more robust cell bodies and diminished cell processes (Fig. 11). Amoeboid microglia and macrophages had even larger cell bodies with very small to undetectable cell processes (Fig. 12). The preponderant morphology recorded in these tumors was amoeboid, with much fewer and almost equal numbers of ramified and reactive morphologies (Table 1). This was particularly true of high-grade tumors. In adjacent normal brain and at the brain-tumor interface, microglia generally exhibited a ramified phenotype, even if the majority phenotype within the tumor was amoeboid (Fig. 13). Mac387+ and CD163+ cells were scattered throughout the tumor and exhibited amoeboid morphologies (Figs. 14, 15).
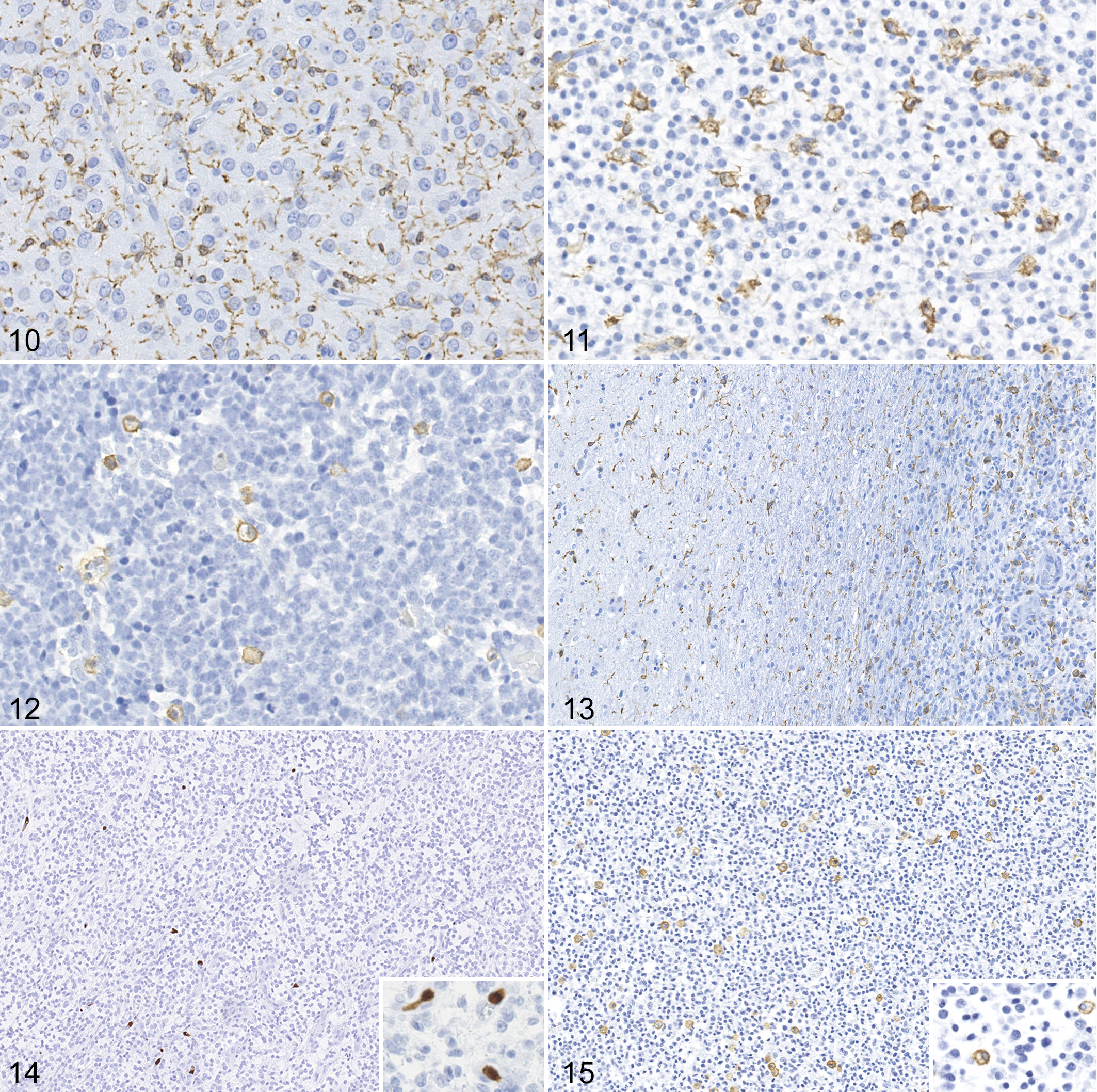
High-grade oligodendroglioma, brain, dog. Immunohistochemistry.
Predominance of ramified, reactive, and amoeboid macrophage morphologies in 73 canine gliomasa.
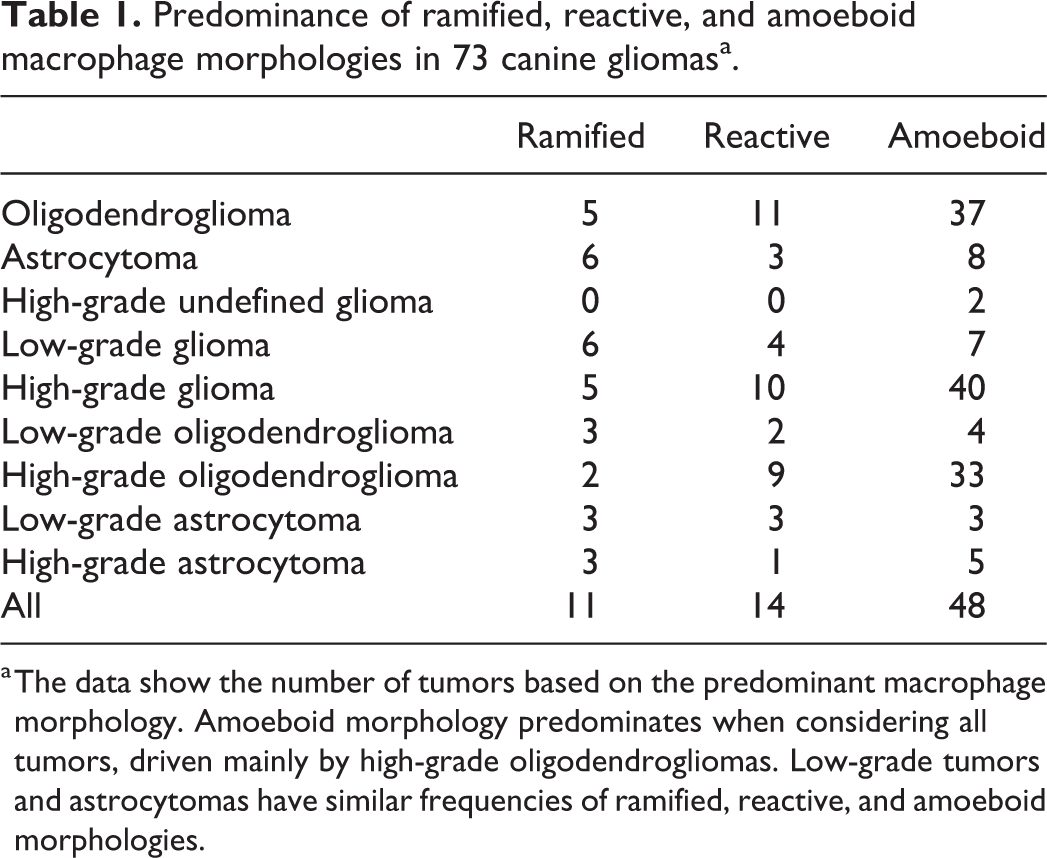
a The data show the number of tumors based on the predominant macrophage morphology. Amoeboid morphology predominates when considering all tumors, driven mainly by high-grade oligodendrogliomas. Low-grade tumors and astrocytomas have similar frequencies of ramified, reactive, and amoeboid morphologies.
Iba1+ macrophages/microglia were present in high numbers, but there were no significant differences in Iba1 labeling between different tumor subtypes or grades (P = .43 and P = .46, respectively; Fig. 16). Both the Mac387 and CD163 area fractions were significantly larger in high-grade than in low-grade tumors (P = .01 for both markers, Figs. 17, 18) and were driven by the differences between high and low-grade oligodendrogliomas (P = .0006 for Mac387 and P = .02 for CD163), with no such difference within astrocytic tumors (P = .97 for Mac387 and P = .36 for CD163). However, no differences between oligodendrogliomas and astrocytomas were found for Mac387+ or CD163+ area fractions (P = .74 and .79, respectively). Manual cell counts of microglia and macrophage subtypes concorded with the automated counts (data not shown).
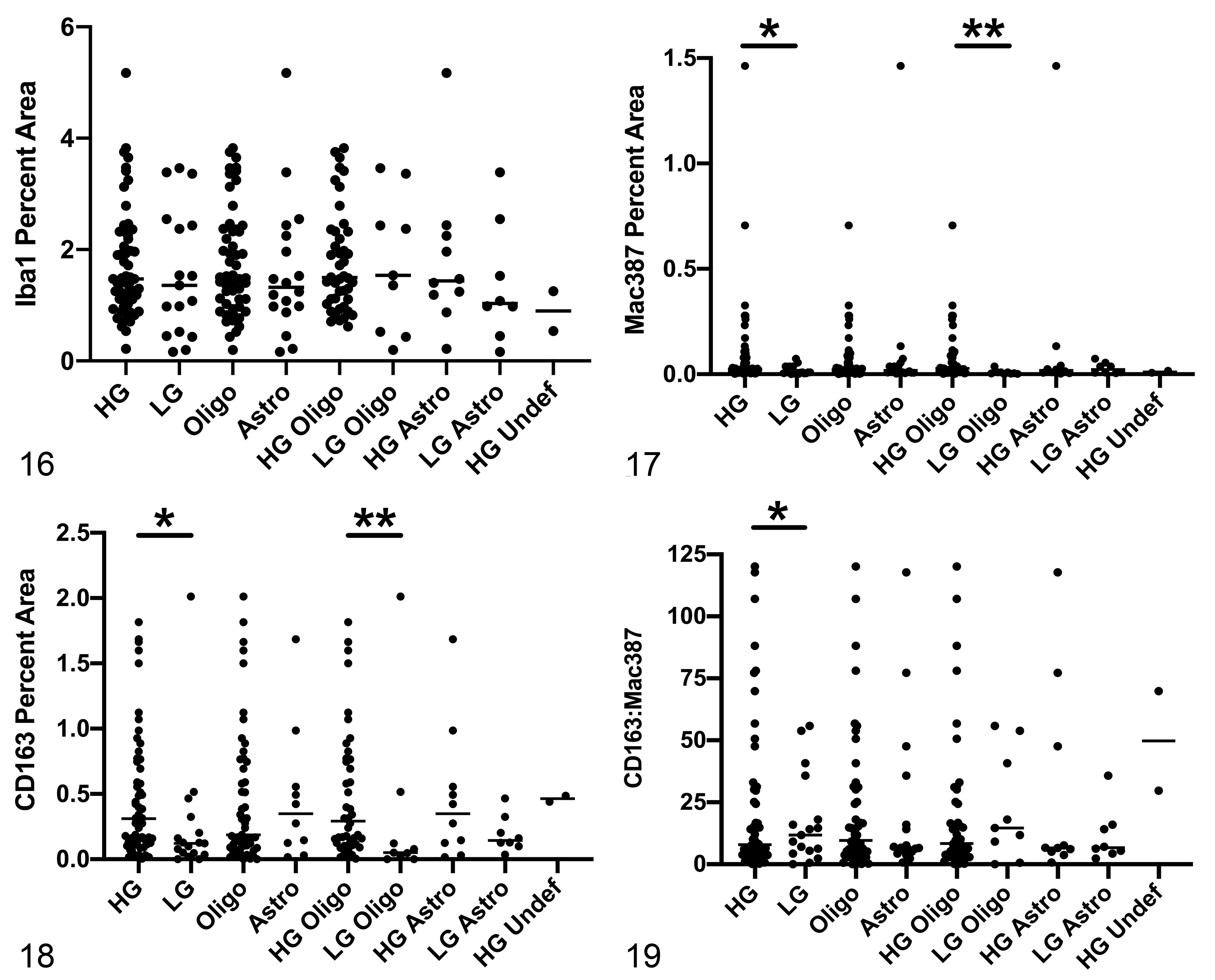
Quantification of immunolabeling for immune cells based on area fraction in canine glioma. HG = high-grade; LG = low-grade; oligo = oligodendroglioma; astro = astrocytoma; undef = undefined glioma.
Considering all tumors, CD163+ area fraction was significantly greater than Mac387+ area fraction (P < .0001) (mean ratio CD163: Mac387 = 21.45, median 8.49, range 0.09–120.10, standard deviation 28.33). This ratio was greater in high-grade tumors compared to low-grade tumors (P = .005, Fig. 19), but it did not differ between tumor subtypes (P = .12, Fig. 19). There was a weak correlation between FoxP3 counts and CD163 counts (r = 0.49, P < .0001).
Discussion
This study is the largest and most comprehensive characterization of inflammatory infiltrates in canine glioma to date, adding to the few previous studies in the dog. 1,18,55,63 In this study, we found robust infiltration of Iba1+ microglia and macrophages into gliomas, with smaller numbers of CD3+ and CD20+ lymphocytes. FoxP3+ cells were found in all cases but were more numerous in high-grade tumors. Most Iba1+ microglia/macrophages exhibited an amoeboid morphology, particularly in high-grade gliomas. Both Mac387+ and CD163+ macrophages were found in greater numbers in high-grade versus low-grade gliomas, driven mainly by the difference in oligodendroglial tumors. However, CD163+ cell numbers were greater than Mac387+ counts in all tumors, a discrepancy that became wider in high-grade gliomas. We found a correlation, albeit a weak one, between CD163+ cell counts and FoxP3+ cell counts. Only a small subset of these gliomas was found to express IDO, consisting primarily of high-grade oligodendrogliomas.
We found CD3+ T cells in all tumors, both dispersed throughout the neoplasms and clustered around normal and glomeruloid vasculature, consistent with previous studies of canine gliomas. 55,63 Pi Castro et al found higher numbers of T cells in high-grade tumors, 55 a finding we did not replicate. One potential reason for this discrepancy is use of a different cell counting methodology, as Pi Castro et al manually counted regions with the highest concentrations of immunolabeled cells, 55 while we analyzed entire tumor sections via computerized image analysis. Although present in lower numbers, we also found CD20+ B cells in all tumors, while these prior studies have only identified B cells in a subset of canine gliomas. 55,63 Although we did see some individual B cells scattered throughout tumors, a prominent perivascular pattern was noted, as in these other studies. Differences in cell counting methodologies may also explain some of these B cell discrepancies. There is literature that demonstrates a relationship between B cells and T cells in experimental glioma models, with B cells serving as antigen-presenting cells and involved in the immune system’s response to glioma. 8 Further work is necessary to explore such a relationship in the dog.
T cell infiltration is also a consistent feature of human gliomas. 36,37,43,58,59,68 Most studies have focused on T cells, with less investigation of B cells and fewer of these cells identified when analyzed, although this has not been the case in all reports. 86 Further subset analysis in several human studies have shown a predominance of CD8+ cells within this T cell subset, suggesting an attempt at a cytotoxic response that is ultimately ineffective. 37,84 A lack of antibodies suitable for use in formalin-fixed, paraffin-embedded tissue sections has hampered further subset analysis in canine tumors, although one study of gliomas has shown a predominance of CD8+ cells with smaller numbers of CD4+ cells using in situ hybridization. 18 Several analyses have found an association between T cell infiltration of gliomas and longer survival times in human patients, 37,38,43 although contradictory results were found in other studies. 59 Such discrepancies are likely related to discrete T cell subsets with variable functions within these larger cell populations.
One important subgroup that has emerged is the Treg subset, traditionally defined as CD4+CD25+FoxP3+ lymphocytes and often identified in tissue by immunohistochemical labeling of FoxP3. Our study identified FoxP3+ cells in all canine gliomas examined. Though intratumoral FoxP3+ cells were generally low in number, these counts were quite variable, with robust infiltration in a number of tumors. We found greater Treg counts in high-grade tumors, consistent with another recent study of canine glioma, though that study found higher numbers of FoxP3+ cells in astrocytomas when compared to oligodendrogliomas, a finding not replicated here. 55 Interestingly, in our study, the 2 highest Treg cell counts were from dogs with high-grade astrocytomas, and it is possible that our findings may be impacted by a limited number of astrocytomas in this study cohort. The presence of Tregs in all gliomas examined in our study and in this previous study contrasts with a study of canine intracranial meningiomas, in which only 39% of tumors had FoxP3+ cells identified via manual cell counting. 6
Tregs inhibit immune system effector cells, impairing their attacks on tumor cells, and their recruitment from peripheral blood to the tumor is thought to play a role in glioma pathogenesis in humans. 15,16,25,32,45,54,65 Though high-grade gliomas contain more Tregs than low-grade gliomas in humans, there are conflicting data regarding the effect of the magnitude of Treg infiltration on prognosis. 30,32,71 Additional studies have demonstrated that the proportion of T effector cells to Tregs is more important than absolute numbers of either subset to T effector cell function and ultimately to prognosis. 17,61 Similar studies are warranted in dogs, but are hampered by a lack of antibodies suitable for immunohistochemistry in formalin-fixed, paraffin-embedded tissue. Alternative methods such as in-situ hybridization and flow cytometry may facilitate such studies, especially with prospective collection of fresh or frozen tissue. 18 Though the association of Treg infiltration with prognosis has not yet been investigated in canine glioma, the links between increased intratumoral Tregs and poor prognoses have been established in other canine cancers, including oral malignant melanoma, oral squamous cell carcinoma, pulmonary adenocarcinoma, malignant mammary carcinoma, and intestinal lymphoma. 10,36,46,60
We detected expression of IDO with immunohistochemistry in only 11% of canine gliomas in this study, all of which were high grade tumors. This enzyme converts tryptophan to kynurenine, is highly expressed in human glioma, and is involved in activation of Tregs. 14,51,78,88,89 In human glioma, high IDO expression has been associated with decreased survival in glioblastoma, and inhibition of IDO has been shown to be synergistic with other therapies in the treatment of glioma. 29,35,78 –80,88 We could not identify any relationship between IDO expression and Tregs, as the number of Tregs in IDO-expressing tumors was highly variable. Our data suggest that IDO may not play a significant role in the pathogenesis of canine glioma, though studies using other detection techniques may be necessary to further explore such a hypothesis.
Resident microglia and macrophages account for 5% to 10% of cells in the normal central nervous system, 41 though they can comprise up to 30% of cells in gliomas. 38,40,57 We found robust infiltration of tumors by Iba1+ microglia and macrophages, which has been documented in other studies of canine brain tumors including gliomas, meningiomas, and choroid plexus tumors. 1,6,12,63 Macrophages and microglia demonstrated a predominantly amoeboid phenotype in most gliomas, and this was particularly true in high grade oligodendrogliomas, with higher relative numbers of ramified and reactive microglial phenotypes in lower grade tumors and astrocytomas (Table 1). The changes in morphology of microglia from ramified through activated to amoeboid phenotypes are generally believed to correlate to a transition from a resting state to a more activated one in which the cells acquire more phagocytic properties. 19,24,52,63 However, the true functional capabilities of these tumor-associated microglia and macrophages are unclear in the setting of canine intracranial gliomas.
We attempted to contribute to the emerging body of knowledge surrounding the immune response to these tumors by evaluating infiltration of cells immunolabeled for markers considered to represent relative polarization of macrophages toward an M1 or an M2 phenotype. This M1-M2 paradigm is an oversimplification, as macrophages exist along a continuum of function between these 2 extremes 4 and cells can switch between M1 and M2 polarization. 2 Mac387 is considered to be a marker of M1-polarized macrophages associated with a pro-inflammatory, normoxic, antitumor state, while M2-polarized macrophages, identified in part by CD163 expression, are associated with an anti-inflammatory, hypoxic, pro-tumor state. 26,56,66,83,87,90,91 Other canine studies also have utilized these markers to identify macrophages with proposed M1/pro-inflammatory (Mac387) or M2/anti-inflammatory (CD163) functions. 9,13,20,31,53,62,76,77,85
In our study, the CD163+ area fraction was greater than the Mac387+ area fraction, with a mean ratio of 21.45 (median 8.49) across all gliomas, suggesting general polarization of tumor-associated macrophages toward an M2-like phenotype. This polarization was even more apparent in high-grade gliomas (mean CD163: Mac387 ratio = 22.67). These findings mirror several studies of human gliomas, which have demonstrated an increased M2-macrophage infiltrate in gliomas 48 that becomes more prominent with higher tumor grades 74,92 and has been associated with shorter survival in some studies. 21,42,74
Previous studies of canine glioma have documented the presence of either Mac387+ or CD163+ cells, although not ratios between the two. 1,63 Sloma et al demonstrated relatively sparse numbers of Mac387+ macrophages within canine oligodendrogliomas and determined that most of these cells were in the intravascular compartment. 63 Indeed, our counts of Mac387+ cells likely overestimated the numbers of cells within tumor parenchyma, as the automated platform used did not distinguish these from intravascular cells. Other studies have demonstrated that Mac387 can immunolabel neutrophils in dogs. 75 However, the cellular and nuclear morphologies of Mac387+ cells in our study were not consistent with neutrophils and these cells are consistent with macrophages. Amin et al demonstrated infiltration of CD163+ cells in a small number of canine gliomas (n = 11) but did not examine a potential M1 phenotype. 1 Our study supports the hypothesis that macrophages within canine glioma are polarized toward an M2-like phenotype, and that this polarization is greater in high-grade tumors. We also found a correlation between FoxP3+ cell counts and CD163+ cell counts in our study, suggesting a relationship between these cell types, as demonstrated in humans. 4 Such a relationship warrants further study in canine tumors.
There are a number of limitations associated with this study. Dogs received a variety of different antemortem treatments, including glucocorticoids, nonsteroidal anti-inflammatory drugs, or radiation therapy, which were not always possible to document due to the retrospective nature of the study. It is possible that these treatments affected the immune cell infiltrate within some of the tumors. The retrospective nature of the sample identification also led to some variation in the time from death to necropsy, as well as tissue fixation time. However, we believe that the effects of this variation were minimal due to similar death to necropsy intervals in most cases and the use of a standard fixation time. Additionally, immunolabeled cells were seen in all tumors. Intravascular monocytes, which are typically Mac387+, 63 could not be excluded from automated digital counting and may have spuriously increased cell counts. However, the automated method allowed for unbiased analysis of all tumor tissue on a slide (with the intentional exclusion of geographic regions of necrosis), instead of the standard selection of certain high-power fields, which is subject to inaccuracies due to sampling errors and investigator bias. 61 Another limitation is the use of single markers for Tregs (FoxP3), M1-like macrophages (Mac387) and M2-like macrophages (CD163). A panel of immune labels is likely to be more accurate in identifying immune cell subtypes and might include CD4, CD25, CD62L, CTLA-4, and GITR for Tregs, 16,17 ADAM10, ADAM17, iNOS, TNF-α, IL-1β, and IL-12 for M1 polarization, and CD206, CCL13, MMP-9, MMP14, IL-10, IL-6, and TGF-β for M2 polarization. 18,21,26,34,42,48,87 Ultimately, the most relevant assessment of both lymphocyte and macrophage phenotype would be a functional one, and this aspect of immune-glioma interactions in dogs awaits further study.
Our ultimate goal is to further knowledge that will help determine prognosis and guide appropriate therapies in dogs with gliomas. As canine glioma is increasingly recognized as a relevant model of the human condition, 1,3 this work may have implications for the design of future studies and clinical trials investigating novel glioma therapeutics in both species.
Supplemental Material
Supplemental Material, sj-pdf-1-vet-10.1177_03009858211023946 - Immunohistochemical evaluation of immune cell infiltration in canine gliomas
Supplemental Material, sj-pdf-1-vet-10.1177_03009858211023946 for Immunohistochemical evaluation of immune cell infiltration in canine gliomas by Gregory A. Krane, Carly A. O’Dea, David E. Malarkey, Andrew D. Miller, C. Ryan Miller, Debra A. Tokarz, Heather L. Jensen, Kyathanahalli S. Janardhan, Keith R. Shockley, Norris Flagler, Brittani A. Rainess and Christopher L. Mariani in Veterinary Pathology
Footnotes
Acknowledgements
We thank Ms Eli Ney of the National Toxicology Program at the National Institute of Environmental Health Sciences (NIEHS/NTP) for assistance with figure preparation, the NIEHS/NTP histology and immunohistochemistry core laboratories for technical support, and Drs Daven Jackson-Humbles and Charan Ganta of the NIEHS/NTP for providing internal review of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work presented in this article was funded by North Carolina State University’s College of Veterinary Medicine, the NIEHS/NTP, and Charles River Laboratories.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.