
Abstract
Oligodendroglioma is one of the most common primary central nervous system neoplasms of dogs. It is often diagnosed in older, brachycephalic breeds, and although its typical clinical features and neuroanatomic location have been well described, less common presentations may hinder its diagnosis. We describe 3 cases of canine cerebral oligodendroglioma that clinically and grossly present as intraventricular tumors. Histologic findings in all cases were typical of oligodendroglioma. Neoplastic cells were uniformly immunoreactive for Olig2 and negative for neuron-specific enolase, neurofilament, and glial fibrillary acidic protein. In addition to the immunopositivity for Olig2, a cluster of morphologically distinct neoplastic cells in one of the cases was immunoreactive for synaptophysin, and the case was diagnosed as an oligodendroglioma with neurocytic differentiation. Based on these findings, oligodendroglioma should be included as a differential diagnosis for intraventricular neoplasia in dogs. Furthermore, oligodendroglioma with ventricular involvement should be differentiated from central neurocytoma by immunohistochemistry.
Oligodendroglioma is one of the most common primary central nervous system (CNS) neoplasms of dogs. It is often diagnosed in older, brachycephalic breeds and typically appears as a focal, well-demarcated, pale tan, soft, gelatinous mass in the telencephalic or diencephalic white matter, and less often in the brainstem and spinal cord.4,7,10–12,16,18,19,23,25 Typical clinical features and neuroanatomic location of oligodendrogliomas have been well described in the human and veterinary medical literature, but uncommon manifestations of these tumors may interfere with an accurate clinical diagnosis.11,13 Examples of these uncommon presentations include the following: 1) multiple, concurrent oligodendrogliomas; 2) diffuse leptomeningeal oligodendrogliomatosis; and 3) oligodendrogliomas associated with the ventricular system (truly intraventricular oligodendrogliomas or parenchymal, periventricular oligodendrogliomas with ventricular invasion).1,5,11,13,19,25 Multiple, concurrent oligodendrogliomas occur as a result of neoplastic spread through the cerebrospinal fluid from a primary tumor within the CNS, a well-known metastatic mechanism referred to as “drop metastasis” in human medicine. Similar cases have been described only rarely in veterinary medicine.3,11 Diffuse leptomeningeal oligodendrogliomatosis is a rare presentation of human and canine oligodendroglioma wherein widespread invasion of the subarachnoid spinal spaces occurs without evidence of a primary mass. 13 Intraventricular oligodendrogliomas occur as unilateral or bilateral masses typically involving the anterior portions of the lateral ventricles and are rarely described in humans.1,2 To the best of our knowledge, intraventricular oligodendrogliomas have not been described in the veterinary medical literature, although parenchymal tumors that break through the ependymal lining and consequently invade the ventricular space are described.6,12,19,25 Although secondary ventricular invasion may be easily interpreted as such when a main parenchymal mass is detected, cases with more extensive ventricular compromise and only minor parenchymal involvement make differentiation from other primary intraventricular tumors more challenging.2,4,8,9,21,29 In this study, we briefly describe the clinical, pathologic, and immunohistochemical findings of 3 cases of canine cerebral oligodendroglioma clinically and grossly occurring as intraventricular masses with minor parenchymal involvement.
Case 1 was a 5-year-old, neutered male French Bulldog with a history of seizures followed by disorientation and blindness. Magnetic resonance imaging (MRI) of the brain revealed a left intraventricular mass (Fig. 1). An image-guided brain biopsy was performed through a lateral craniotomy, but the dog was euthanized because of postoperative complications of cerebral herniation and hemorrhage. Grossly, a well-demarcated, gray to dark red, soft, ~2 cm in diameter mass was present within the left lateral ventricle, with only minor involvement of the adjacent white matter (Fig. 2). Case 2 was a 5-year-old, female Bulldog with a 4-day history of lethargy, aggressive behavior, ataxia, and lateral recumbency. The dog was euthanized because of the progressive nature of the neurologic signs. Gross findings consisted of a well-demarcated, tan to pink, soft, gelatinous, 2.3 cm in diameter mass within the caudal left lateral ventricle (Fig. 3). The adjacent parenchyma was compressed, and the lateral ventricles were bilaterally expanded (secondary obstructive hydrocephalus), but tumor was not observed in the adjacent white matter. Case 3 was a 7-year-old, neutered male mixed-breed dog with a 2-day history of seizures that culminated in spontaneous death. MRI of the brain revealed a left intraventricular mass. Gross findings included a well-demarcated, red, soft, 2.5 cm in diameter, gelatinous mass within the caudal portion of the right lateral ventricle. The adjacent cerebral parenchyma was compressed by the mass, but no tumor was observed in that area.
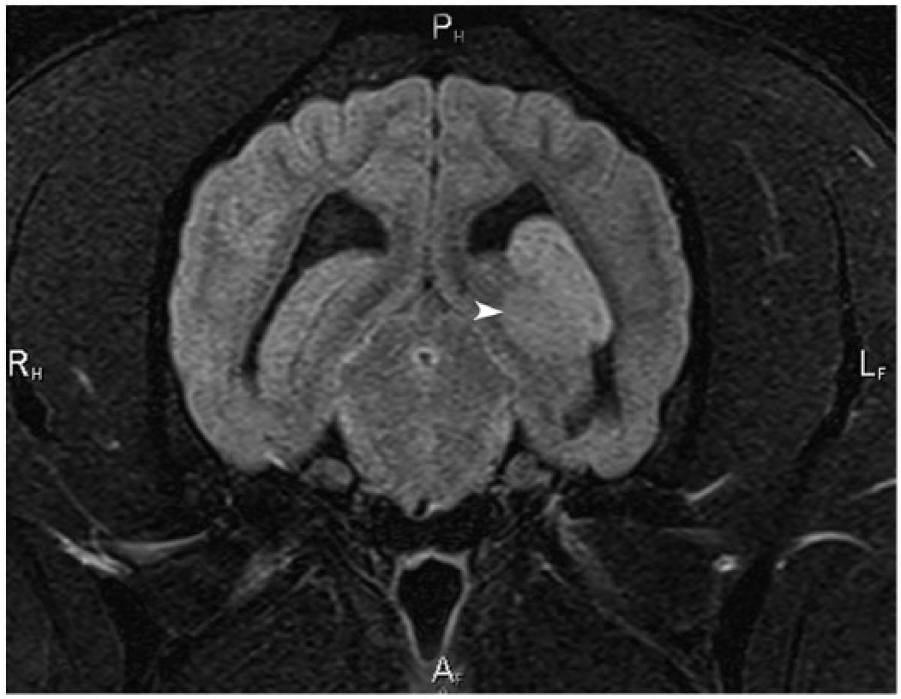
Magnetic resonance image (MRI), dog 1. Transverse plane T2-weighted fluid attenuated inversion recovery (FLAIR) MRI of the brain at the level of the occipital lobes. There is a well-circumscribed mass within the caudal aspect of the left lateral ventricle (arrowhead). The mass is hyperintense to gray matter and invades and compresses the periventricular white matter of the hippocampus and the left ventricle. Imaging differential diagnosis includes choroid plexus tumor, ependymoma, intraventricular meningioma, and atypical oligodendroglioma.
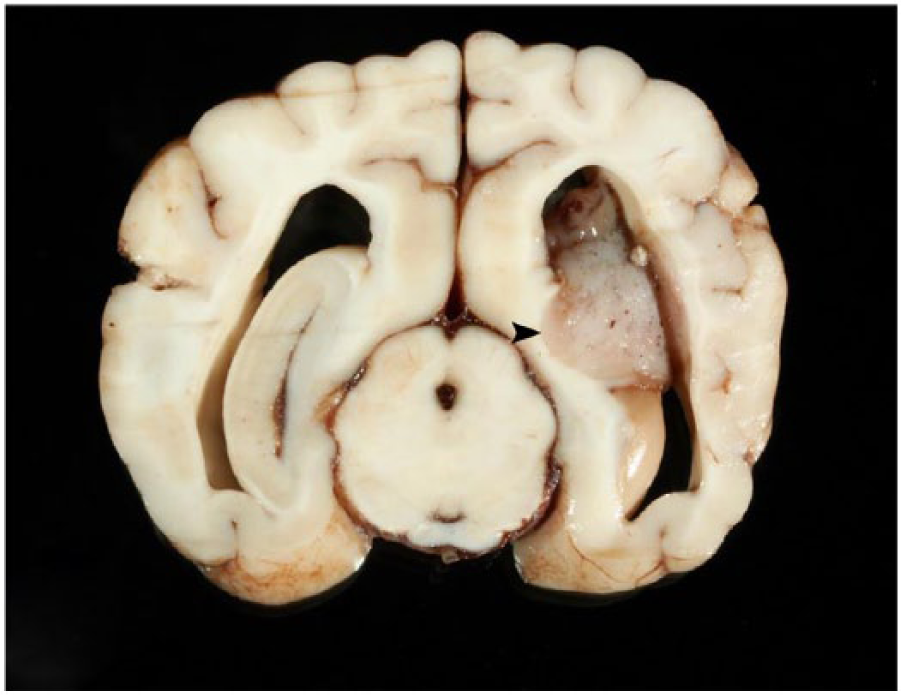
Brain, dog 1. A well-demarcated, gray to dark red, soft mass is present within the left lateral ventricle. The periventricular white matter is partially effaced by the tumor (arrowhead).
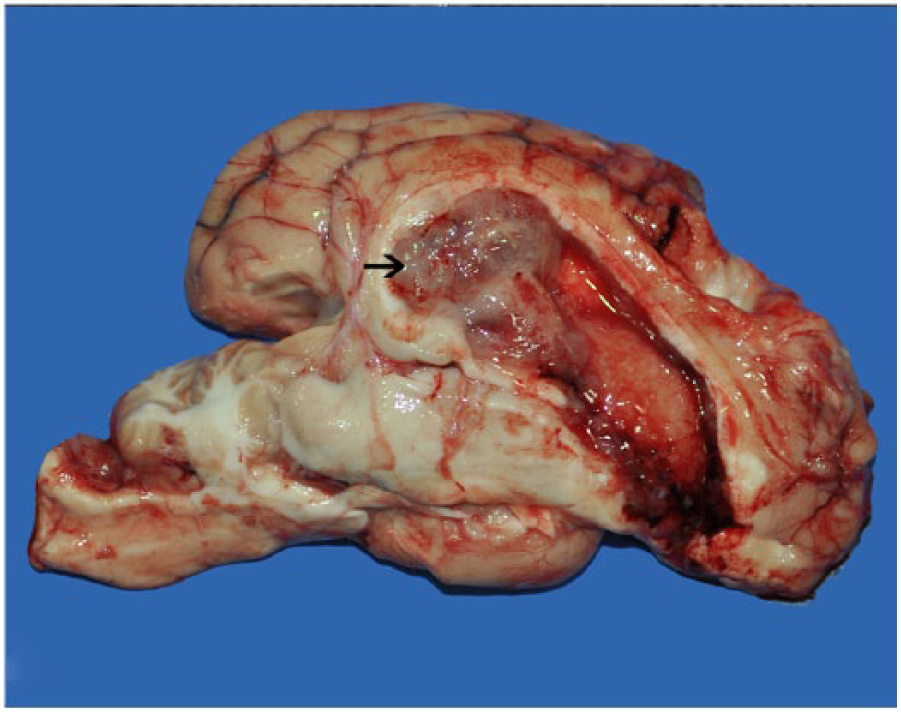
Brain, dog 3. A well-demarcated, tan to pink, soft, gelatinous mass is present within the caudal left lateral ventricle (arrow). The affected ventricle is expanded because of outflow obstruction by the mass.
Histologically, all cases had similar features. In cases 1 and 2, the tumor almost completely occluded the left lateral ventricle, with only minor involvement of the adjacent white matter. The neoplasm in case 3 diffusely effaced the right lateral ventricle. The ependymal lining was completely obscured by neoplastic infiltration, and a distinction between the ventricular lumen and the adjacent white matter could no longer be appreciated. All 3 neoplasms were composed of closely packed sheets of round to oval cells supported by a fine fibrovascular stroma. Faintly basophilic, fibrillar, mucinous-like material occasionally filled small, discrete microcystic areas (Fig. 4). Neoplastic cells were moderately pleomorphic, with variably distinct cytoplasmic borders and a moderate amount of eosinophilic, finely granular cytoplasm with a variably prominent perinuclear clear halo (Fig. 5). Nuclei were round to oval and had finely stippled to coarse chromatin and 1–3 nucleoli. The mitotic rate in cases 1 and 3 was low, ranging from 0 to 1 per 40× field. Case 2 had a cluster of neoplastic cells morphologically distinct from the surrounding neoplastic oligodendrocytes. These cells were characterized by closely packed, round to polygonal neoplastic cells with a moderate amount of eosinophilic, homogeneous cytoplasm with distinct cell borders, and round nuclei with finely stippled chromatin and 1–2 nucleoli. Mitotic activity was higher in this case, with 1–4 mitoses in each 40× field. Clusters of microvascular proliferation were observed at the margins of all tumors. Areas of hemorrhage and necrosis were observed within all 3 neoplasms or affecting the adjacent neuroparenchyma. Immunohistochemical staining (IHC) for Olig2, neuron-specific enolase (NSE), synaptophysin (SYP), neurofilament, and glial fibrillary acidic protein (GFAP) was conducted in sections of all 3 tumors. The IHC results are summarized in Table 1 and shown in Figure 6. Control tissues for all 3 samples consisted of normal canine spinal cord.
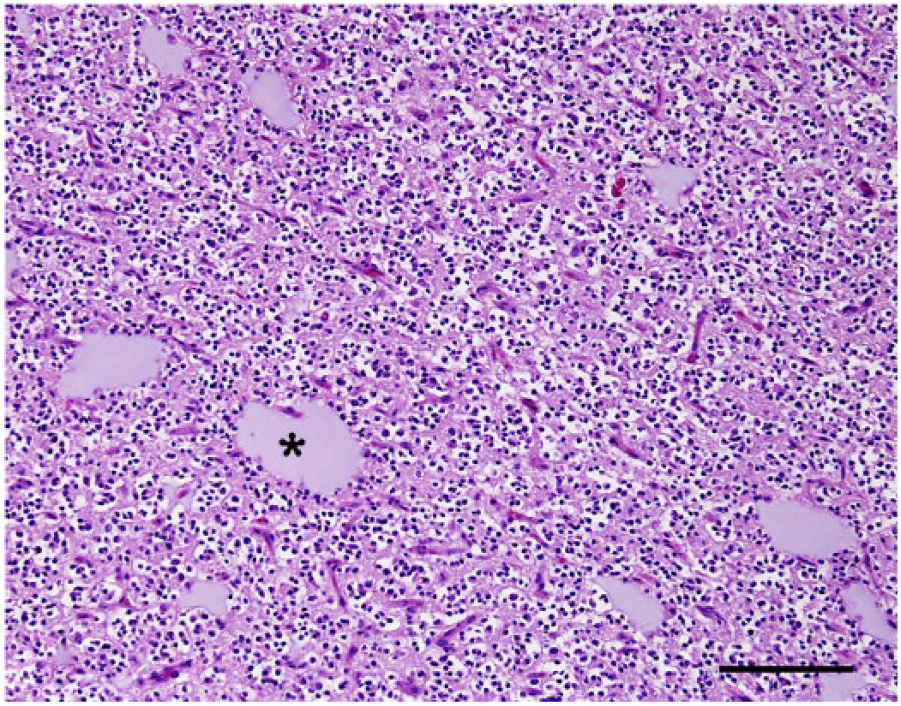
Brain, dog 3. All 3 neoplasms have similar histologic features and are composed of closely packed sheets of round to oval neoplastic cells supported by a fine fibrovascular stroma and multiple accumulations of mucinous-like material (asterisk). Hematoxylin and eosin. Bar = 200 µm.
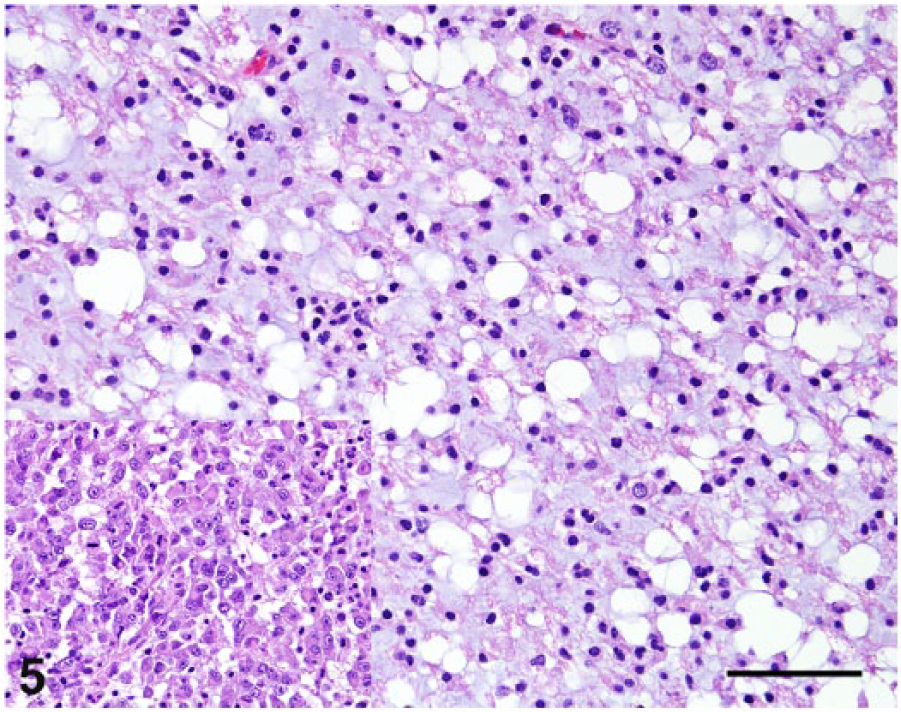
Brain, dog 2. Neoplastic cells have variably distinct cytoplasmic borders, a moderate amount of eosinophilic, finely granular cytoplasm, and a variably prominent perinuclear clear halo. Inset: central areas of the tumor have a distinct population of closely packed, round to polygonal neoplastic cells with eosinophilic, homogeneous cytoplasm and round nuclei with finely stippled chromatin and 1–2 nucleoli. Hematoxylin and eosin. Bar = 100 µm.
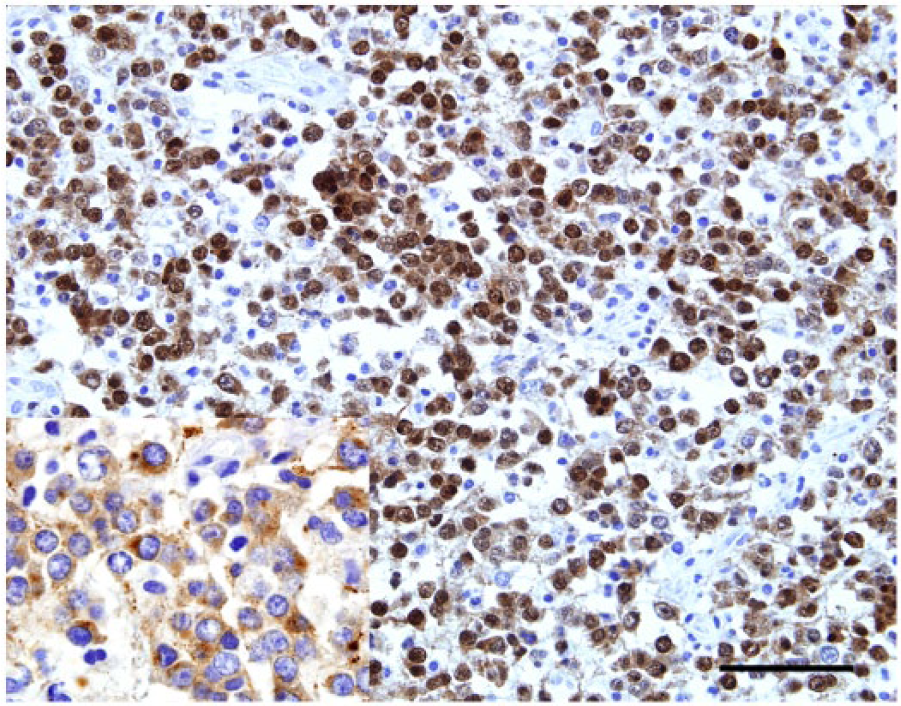
Brain, dog 2. Positive immunoreaction for Olig-2 is evident in all tumors. Inset: a central cluster of distinct neoplastic cells in case 2 are immunoreactive for synaptophysin. Bar = 100 µm.
Antibodies and immunohistochemical findings in 3 cases of canine oligodendroglioma occurring as intraventricular tumors. *
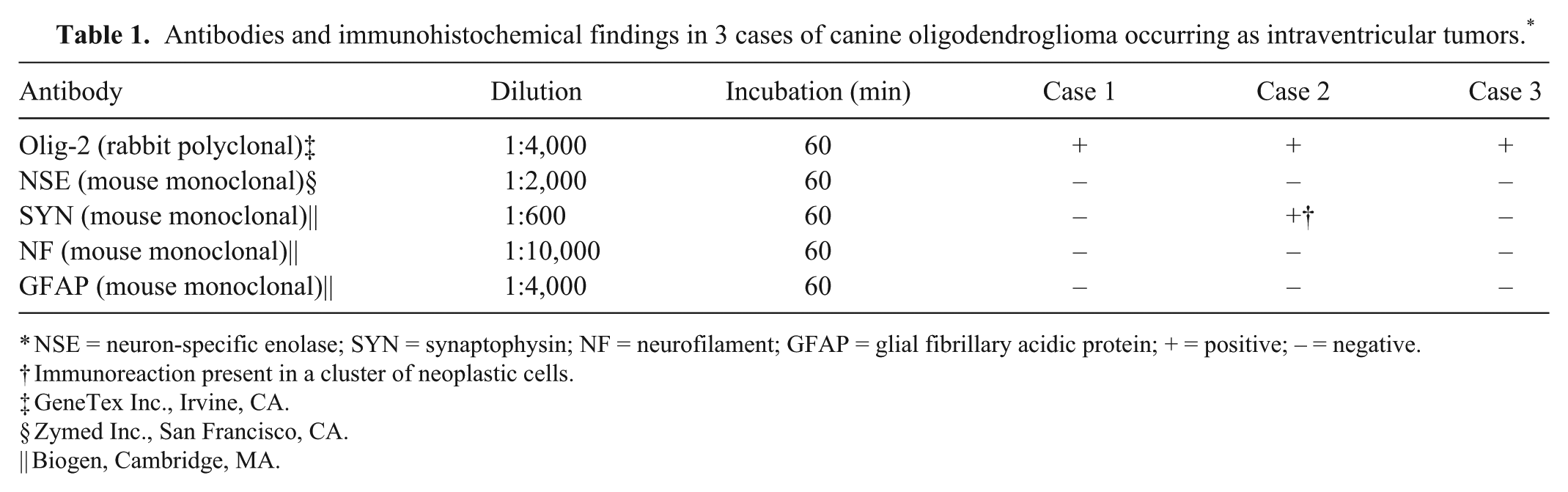
NSE = neuron-specific enolase; SYN = synaptophysin; NF = neurofilament; GFAP = glial fibrillary acidic protein; + = positive; – = negative.
Immunoreaction present in a cluster of neoplastic cells.
GeneTex Inc., Irvine, CA.
Zymed Inc., San Francisco, CA.
Biogen, Cambridge, MA.
All 3 canine oligodendrogliomas in this study occurred as single masses that were clinically (cases 1 and 3) and grossly (cases 1–3) identified as intraventricular tumors affecting the lateral ventricles, with minor involvement of the adjacent white matter that was grossly detected only in case 3. Histologically, more extensive involvement of the adjacent white matter was detected in case 3, with less periventricular involvement detected in cases 1 and 2.
Most human and canine oligodendrogliomas occur as single masses in the telencephalic or diencephalic white matter, with less frequent involvement of the brainstem and spinal cord.12,18,25,26,30 Intraventricular oligodendroglioma is a rare subset of human oligodendroglioma and occurs as unilateral or bilateral masses involving the anterior portions of the lateral ventricles.1,2,5 Intraventricular oligodendrogliomas are typically slow-growing tumors, and most affected patients develop clinical signs associated with ventricular outflow obstruction and consequent elevated intracranial pressure rather than related to the mass itself. 30 We found no descriptions of true intraventricular oligodendrogliomas in the veterinary medical literature, but oligodendrogliomas that break through the ventricular lining and invade the ventricular spaces, occurring as intraventricular tumors with involvement of the adjacent white matter, are reported.5,12,25 It remains undetermined whether these 3 tumors arose from the periventricular white matter and grew into the ventricles or were primarily intraventricular tumors that secondarily invaded the adjacent white matter, although the former hypothesis seems more plausible. Because of their location and infiltration through the subependymal area, it is possible that these tumors arose from remnants of the germinal matrix that reside in the subventricular white matter and subsequently invaded the ventricles.15,24 Regardless of their primary neuroanatomic origin, it is important to consider that oligodendrogliomas are typically not included as a differential diagnosis for cerebral ventricular tumors during clinical evaluation using MRI and computed tomography.21,28 The location of these 3 tumors indicates that oligodendrogliomas may share MRI and gross pathologic features with other CNS neoplasms that arise within the ventricles, such as ependymomas, choroid plexus tumors, neurocytomas, and meningiomas.11,27 Therefore, although differentiation of these tumors may be relatively easy based on histology and IHC, clinical features may overlap and hinder an accurate antemortem diagnosis.
Histologically, the most important differential diagnosis for the current cases is neurocytoma. Central neurocytoma has been rarely described in dogs. The tumor may occur intraventricularly or in the spinal cord, and it has histologic features that closely resemble those of oligodendroglioma.8,21 It is also possible that oligodendrogliomas and neurocytomas share a common progenitor cell that will give rise to morphologically similar neoplasms. 20 Morphologic features of central neurocytoma that are not typically seen with oligodendroglioma include fibrillary areas mimicking neuropil, cells arranged in a streaming pattern, mineralization, and perivascular pseudorosettes.14,21,29 Canine neurocytomas are NSE- and SYP-positive and consistently negative for oligodendroglial and astrocytic markers such as Olig2 and GFAP, respectively.8,21 Although currently there is no definitive IHC marker for oligodendrocytes, the IHC profile in the cases of this study is consistent with reports in the veterinary and human medicine for the differentiation of oligodendroglioma and central neurocytoma.8,21,29 The lack of specific IHC markers for oligodendrocytes in human medicine has brought great emphasis on molecular genetic criteria for a more accurate diagnosis of oligodendrogliomas, particularly allelic deletion on chromosomes 1p and 19q. 22 The morphologically distinct subpopulation of SYP-positive cells in one dog (case 2) is consistent with the diagnosis of oligodendroglioma with neurocytic differentiation. 17
In summary, we describe the clinical and pathologic features of 3 cases of canine cerebral oligodendroglioma occurring as an intraventricular mass. This subset of oligodendroglioma should be included in the differential diagnoses for canine intraventricular neoplasms.
Footnotes
Acknowledgements
We thank Abbie Butler and Patricia Rowe at the College of Veterinary Medicine, The University of Georgia, for their outstanding support with immunohistochemistry.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.