
Abstract
Feline mammary carcinomas are highly malignant tumors usually associated with poor outcome. Nevertheless, survival times can differ significantly according to various prognostic factors. The Elston and Ellis (EE) histologic grading system, originally developed for human breast cancer, is commonly used to grade feline mammary carcinomas, although it is not really adapted for this species, hence the need of a more relevant grading system. Although few veterinary studies attempted to validate previously published results in an independent cohort, the aim of our study was to evaluate the prognostic value of different histologic grading systems in feline invasive mammary carcinomas, including the EE grading system applicable to human breast cancers and the modified and newly designed histologic grading systems recently proposed by Mills et al. Survey data and histologic features of 342 feline invasive mammary carcinomas were analyzed with respect to overall and cancer-specific survival. The histological grading system with best prognostic value was the mitotic-modified Elston and Ellis (MMEE) grading system: grade III carcinomas (P = .04, hazard ratio [HR] = 1.46, 95% CI, 1.01–2.11), grade II (P = .03, HR = 1.39, 95% CI, 1.03–1.88), and grade I carcinomas (HR = 1.00, reference), with decreasing hazard ratios significantly were associated with a worse overall survival, independently from the pathologic tumor size (pT ≥ 20 mm: P = .002, HR = 1.45, 95% CI, 1.15–1.83) and positive nodal stage (P = .001, HR = 1.51, 95% CI, 1.18–1.94). This retrospective study validates Mills et al’s proposal to adapt the thresholds for mitotic counts to better assess the histological grade of the highly proliferative mammary carcinomas encountered in the cat.
Keywords
Mammary tumors are common in cats and constitute approximately 17% of all feline neoplasms, 7,16 with reported malignancy rates ranging between 80% and 90%. 6,9 Feline mammary carcinomas (FMCs) have a tendency to be biologically aggressive, with a median reported overall survival time of 8 to 12 months postdiagnosis in most studies with follow-up. 2 –4,11,23 However, survival times can differ significantly according to various prognostic factors, reviewed by Zappulli et al 31 and others, 6 such as the pathologic tumor size, 8,10,23,26,29 lymphovascular invasion, 19,21,23,28,29 the presence of nodal or distant metastasis, 23,29 the clinical stage according to the World Health Organization (WHO), 8 the histological type, 22 –25 histological grade, 2,12,14,15,23 margin status, 29 skin ulceration, 29 peritumoral lymphoplasmacytic inflammation, 29 and some immunohistochemical markers such as cyclooxygenase-2 expression, 13 the Ki-67 proliferation index, 4,20,23,26 and the molecular subtypes defined by estrogen receptor alpha (ER), progesterone receptor (PR), the feline homolog of human epidermal growth factor receptor-2 (HER2), Ki-67, and cytokeratins 5 and 6 (CK5/6) expression. 26,27
The most widely accepted grading system for FMCs was adapted from the grading system used in human breast cancer and is based on 3 parameters: tubule formation, nuclear pleomorphism, and mitotic count. 5 According to Castagnaro et al, 2 the Elston and Ellis (EE) grading system has good prognostic value for well-differentiated (grade I) and poorly differentiated (grade III) feline mammary carcinomas but not grade II tumors. The same grading method was found to have high prognostic value in queens with invasive carcinomas by Millanta et al. 14 Seixas et al 23 found the EE grading system to be a significant prognostic factor by multivariate analysis for middle-aged to elderly queens with mammary carcinomas, independent from lymphovascular invasion in terms of disease-free survival and independent from lymph node metastasis in terms of overall survival. These studies present persuasive evidence in support of histologic grading using the EE grading system as a predictor of overall survival in cats with FMCs.
Recently, Mills et al 15 reevaluated the classic EE grading system that failed to correlate significantly with cancer-specific survival in their study. Using multivariate analysis, they found that lymphovascular invasion, nuclear form, and mitotic count each demonstrated independent prognostic significance regarding cancer-specific survival of cats with invasive mammary carcinomas. Modifications of the EE system and a novel grading system were then proposed, and all showed significant correlation with cancer-specific survival. 15
Few veterinary studies attempted to validate previously published results in an independent cohort. Therefore, the aim of our study was to evaluate the prognostic value of different histologic grading systems, including the EE grading system applicable to human breast cancers, and the modified and newly designed histologic grading systems recently proposed by Mills et al. 15 for feline invasive mammary carcinomas in an independent retrospective cohort of 342 female cats with stages I–III invasive mammary carcinoma.
Materials and Methods
Case Origin and Data Collection
This retrospective study included 342 cases of feline mammary carcinomas that were diagnosed between 2007 and 2010 in 2 laboratories for veterinary diagnostic pathology: the Laboratoire d’Histopathologie Animale (LHA) at Oniris, Nantes, and the Laboratoire d’Anatomie Pathologique Veterinaire (LAPV) of Amboise, France. The owners’ written consent and approval from the local animal welfare committee of Oniris were obtained prior to inclusion. Collected information regarding the cases included signalment (age, breed, spaying status), history of contraception and parity, and medical history.
Tumors were staged according to the modified WHO staging system. 17,18 Stage I included cats with primary tumors less than 20 mm of largest diameter on histological sections (pathologic tumor size), with no evidence of regional or distant metastases; stage II included cats with tumors 20 to 30 mm in diameter on histological sections, with no evidence of regional or distant metastases. Stage III included cats with primary tumors less than 30 mm of tumor size, with evidence of regional metastases, or cats with tumors greater than 30 mm in diameter, with or without evidence of regional metastases but without evidence of distant metastases. Stage IV FMCs (with evidence of distant metastases at diagnosis, regardless of tumor size or regional metastases) were excluded from the present study.
Inclusion/Exclusion Criteria
Feline patients were eligible for inclusion when an invasive mammary carcinoma was the only primary malignant tumor evident at time of diagnosis, the animal was treated solely by surgery (no chemotherapy or radiation therapy pre- or postmastectomy), there was no evidence of distant metastasis at diagnosis, and follow-up was available for at least 48 months postsurgery.
Exclusion criteria included patients with noninvasive in situ mammary carcinomas, those who had presented another malignant tumor than the mammary carcinoma either before or at the time of diagnosis, the animals whose outcome was unknown after the diagnosis of mammary carcinoma, cats treated with adjuvant chemotherapy or radiation therapy, stage IV disease, and the carcinomas that were improper for adequate immunohistochemical staining. A total of 342 female cats with stages I–III invasive mammary carcinoma were included in this study.
Processing of Tissues and Immunohistochemistry for Histologic Staging Purposes
The tumor samples were fixed in 10% formalin and embedded in paraffin, cut into 3 μm–thick sections, and then stained with hematoxylin-eosin-saffron (HES). Automated immunohistochemistry (Benchmark XT Ventana Medical Systems, Roche Diagnostics) was used on 3 μm–thick sections for confirmation of lymphovascular invasion using LMO2 as a lymphatic endothelium marker (LIM domain-only protein-2, clone SP51, Spring M351) and evaluation of invasiveness using p63 as a myoepithelial cell marker (clone 4A4, Abcam ab735). Mammary carcinomas limited by a continuous layer of p63-positive myoepithelial cells were defined as mammary carcinomas in situ and excluded from the present study. Mammary carcinomas with a focal interruption of their p63-positive myoepithelial cell lining, less than 1 mm long, were considered micro-invasive and also excluded from the present study. Mammary carcinomas lacking a p63-positive myoepithelial cell layer over at least 1 mm of their circumference were defined as invasive and were included. This technique was used only when invasiveness was doubtful on HES-stained slides.
Histologic Assessment Criteria Except Histological Grade
In case of multiple (within a given mammary gland) or multicentric (within different mammary glands) invasive mammary carcinomas, the carcinoma with the largest diameter on histological section was selected for analysis. The histological types included tubulopapillary (tubular, papillary, and tubulopapillary), solid (including adenosquamous, squamous cell, and anaplastic), cribriform (containing small hole-like lumens within a solid background), and mucinous, with most of the cases demonstrating more than 1 growth pattern. In these instances, the less differentiated pattern of the tumor (ie, anaplastic or solid) determined the subtype; or when 2 patterns that could be considered equally well differentiated coexisted (ie, cribriform and mucinous), the largest growth pattern determined the subtype.
The pathologic tumor size (pT) was measured on HES-stained histological sections as the largest tumor dimension in millimeters. Lymphovascular invasion (LVI), the presence of lymph and/or blood vessel emboli, was assessed on HES-stained slides and confirmed by LMO2 immunohistochemistry in case of doubt. Positive lymphovascular invasion was confirmed if neoplastic emboli were clearly seen within an LMO2-positive row of lymphatic endothelial cells. Central necrosis of any type (coagulative, lytic, or comedonecrosis) affecting groups of neoplastic cells (but not single scattered cells) was assessed as present/absent regardless of extension. Squamous differentiation affecting groups of viable neoplastic cells (not directly adjacent to necrotic foci), manifested by an eosinophilic glassy appearance of the cytoplasm, not necessarily with keratin pearl formation, was assessed as present/absent regardless of extension. Peritumoral tumor-associated lymphoplasmacytic and macrophagic inflammation was quantified as absent (0), minimal (1), mild (2), moderate (3), marked (4), or severe (5) and then considered negative for scores 0 to 2 and positive for scores 3 to 5. To be considered moderate, peritumoral mononuclear inflammation had to involve at least half of the circumference of the mammary carcinoma, marked peritumoral inflammation had to be multifocally observed along all the circumference, and severe peritumoral inflammation had to contain nodular lymphohistiocytic infiltrates resembling lymphoid follicles.
EE: Elston and Ellis Histologic Grading System
At first, tumors were graded according to the EE grading system described for human breast cancer (Table 1), 5 where carcinomas were scored according to 3 criteria: the percentage of tubule formation, subjectively assessed at low-power magnification and quantified as a percentage of the tumor parenchyma; the degree of nuclear pleomorphism, assessed at high power (400×) magnification in the least differentiated and/or most invasive portion of the tumor, typically along the periphery; and the mitotic count in 10 high-power fields (400×). A total score was calculated for each tumor by summing the points of the 3 categories to determine the grade (I: 3–5 points, II: 6 or 7 points, or III: 8 or 9 points), indicating respectively well-differentiated, moderately differentiated, or poorly differentiated carcinomas.
Elston and Ellis (EE), Mitotic-Modified Elston and Ellis (MMEE), and Revised Elston and Ellis (REE) Grading Systems for Invasive Mammary Carcinoma in Female Cats.
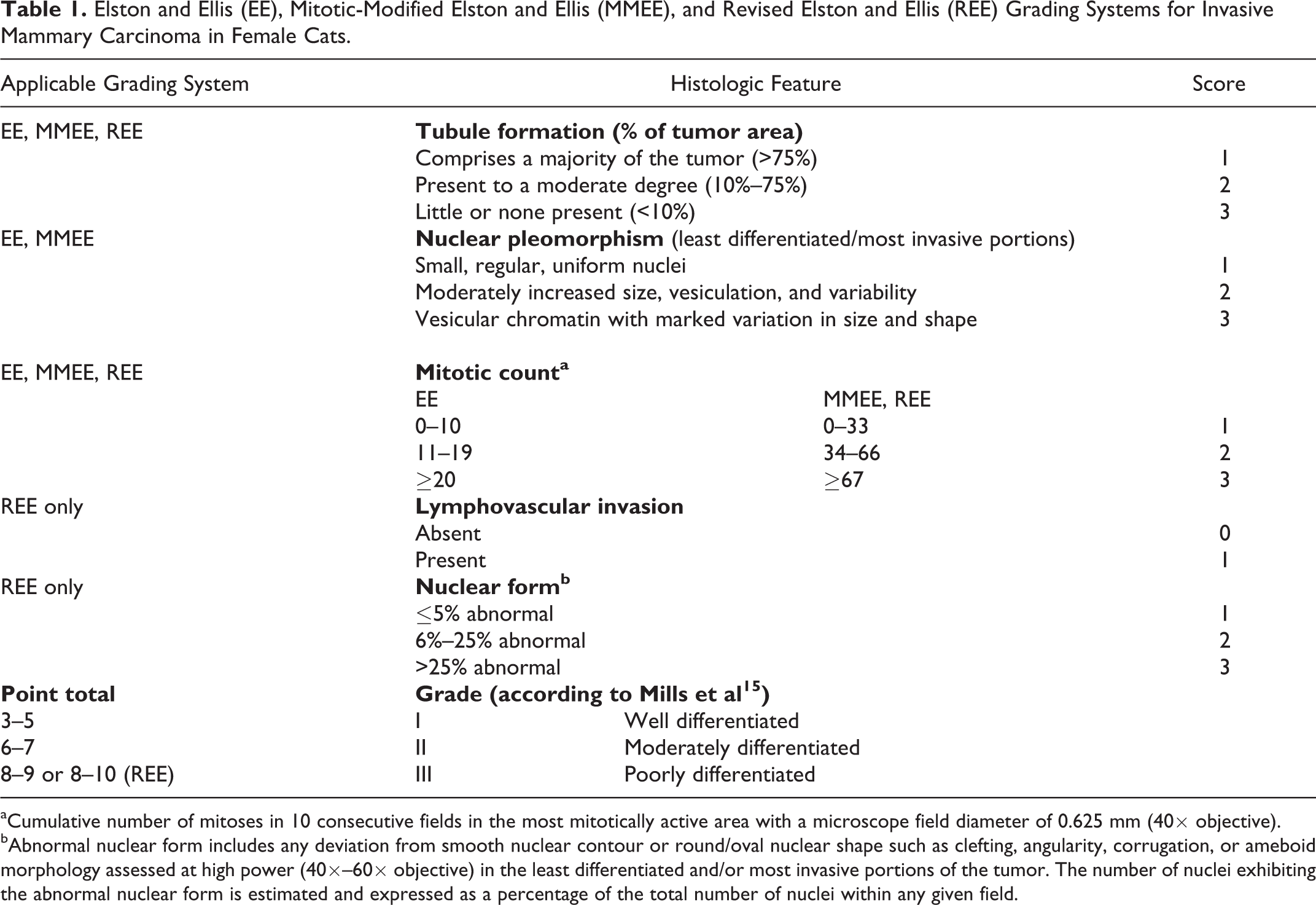
aCumulative number of mitoses in 10 consecutive fields in the most mitotically active area with a microscope field diameter of 0.625 mm (40× objective).
bAbnormal nuclear form includes any deviation from smooth nuclear contour or round/oval nuclear shape such as clefting, angularity, corrugation, or ameboid morphology assessed at high power (40×–60× objective) in the least differentiated and/or most invasive portions of the tumor. The number of nuclei exhibiting the abnormal nuclear form is estimated and expressed as a percentage of the total number of nuclei within any given field.
Three grading systems were then applied to our cohort using the grading systems designed by Mills et al. 15
MMEE: Mitotic-Modified Elston and Ellis Histologic Grading System
In the mitotic-modified Elston and Ellis (MMEE) grading system proposed by Mills et al 15 (Table 1), mitotic figures were counted in 10 consecutive fields at the periphery of the tumor in the areas of highest proliferative activity. The mitotic count categories of the EE grading system were modified to better accommodate the wide range and high magnitude of mitotic counts observed within feline mammary carcinomas (Fig. 1). In Mills et al’s 15 original publication, the thresholds for the mitotic counts were ≥51 and ≥71 mitoses in 10 high-power fields according to the observed tertiles in their population. In the present study, the corresponding thresholds for the mitotic counts were ≥34 and ≥67 to take into account the differences in field diameter (0.53 mm in Mills et al’s 15 study, 0.625 mm in the present study). Furthermore, the threshold of ≥33 mitoses in 10 high-power fields was also evaluated, according to the receiver-operating characteristic (ROC) curve for 2-year overall survival of the cats included in the present study.
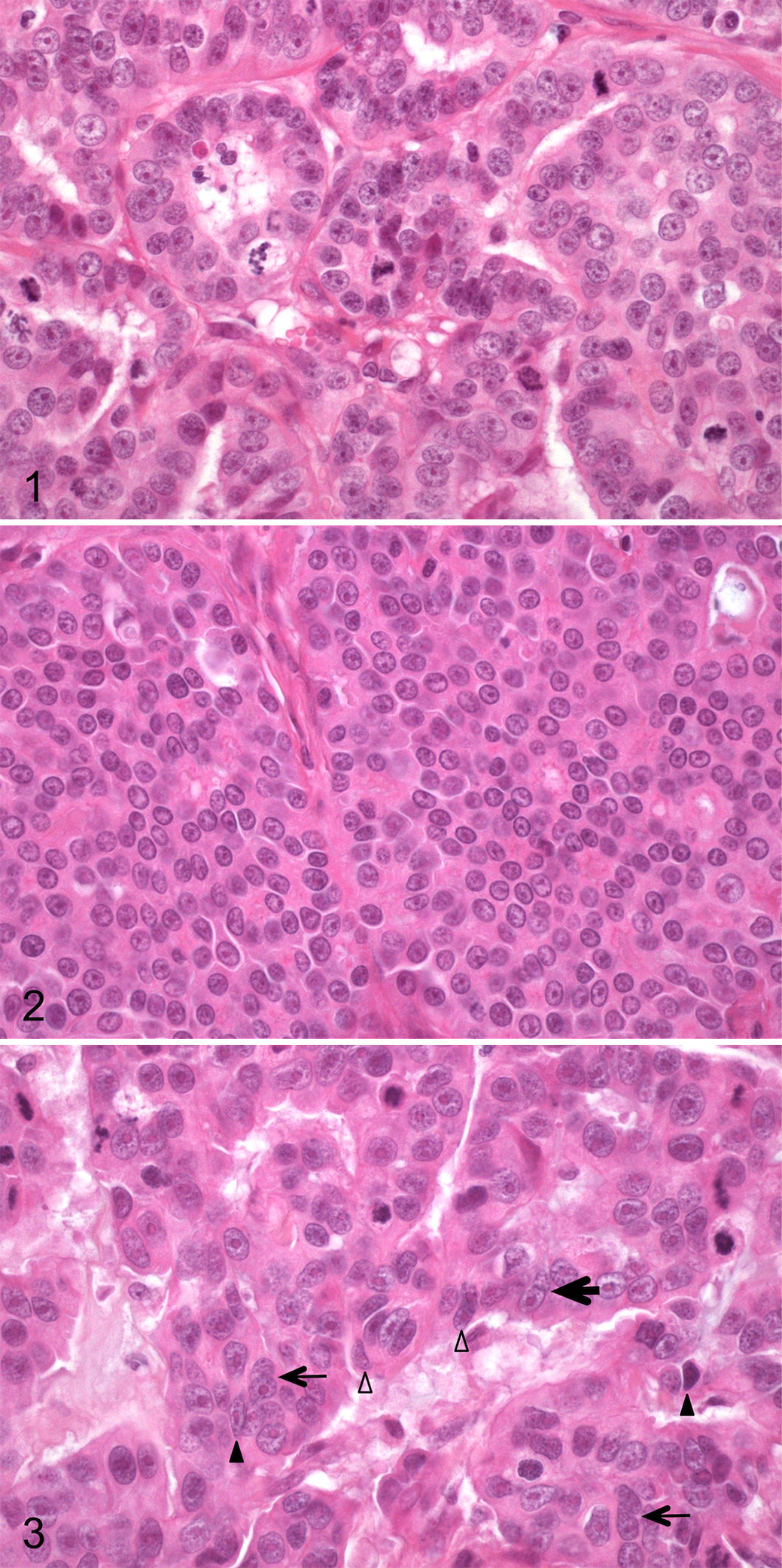
Invasive mammary carcinoma, mammary gland, cat. Hematoxylin, eosin and saffron (HES).
REE: Revised Elston and Ellis Histologic Grading System
In the revised Elston and Ellis (REE) grading system (Table 1) proposed by Mills et al, 15 the EE grading system was modified further to include nuclear form instead of nuclear pleomorphism.
The nuclear form assessment was evaluated according to Mills et al 15 using a high-power (40×) objective in the least differentiated and/or most invasive portion of the carcinoma. Subjective evaluation of nuclear shape independent of other nuclear features or artifactual changes was performed. Deviations from a smooth nuclear contour and oval/round shape such as corrugation, angularity, clefting (indentation), or overtly ameboid shape were considered abnormal. The number of nuclei exhibiting abnormal form was estimated relative to the total number of nuclei within a given field and expressed as a percentage. Subgroups of 5% (Fig. 2), 6% to 25%, or >25% (Fig. 3) abnormal were then assigned.
In the REE/LVI scoring system, lymphovascular invasion was also taken into account, with an additional point when present.
Mills-2015 Histologic Grading System
Finally, the grading system proposed by Mills et al 15 that included lymphovascular invasion, nuclear form, and mitotic count was evaluated (Mills-2015). In the present study, the Mills-2015 grading system was analyzed using a mitotic count cutoff of ≥33 mitoses in 10 high-power fields, according to a ROC curve for the 2-year overall survival rate of the cats included in the present cohort. The chosen cutoff was different from the >62 cutoff originally proposed by Mills et al, 15 which corresponded to the median mitotic count observed in their cohort (by comparison, the median mitotic count in the present cohort was 44 mitoses in 10 high-power fields).
Using this Mills-2015 grading system (Table 2), the absence of lymphovascular invasion together with less than or equal to 5% abnormal nuclear form and a mitotic count less than or equal to 33 mitoses in 10 high-power fields corresponded to grade I (low-grade carcinoma). The presence of any 1 of lymphovascular invasion, greater than 5% abnormal nuclear form, or a cumulative mitotic count greater than 33 yielded grade II (intermediate-grade carcinoma). Finally, if any 2 or all 3 of the aforementioned features were present, grade III (high-grade carcinoma) was assigned. Afterward, grade II and III tumors were grouped together for survival analyses.
Mills-2015 Grading System for Evaluation of Invasive Mammary Carcinoma in Female Cats.
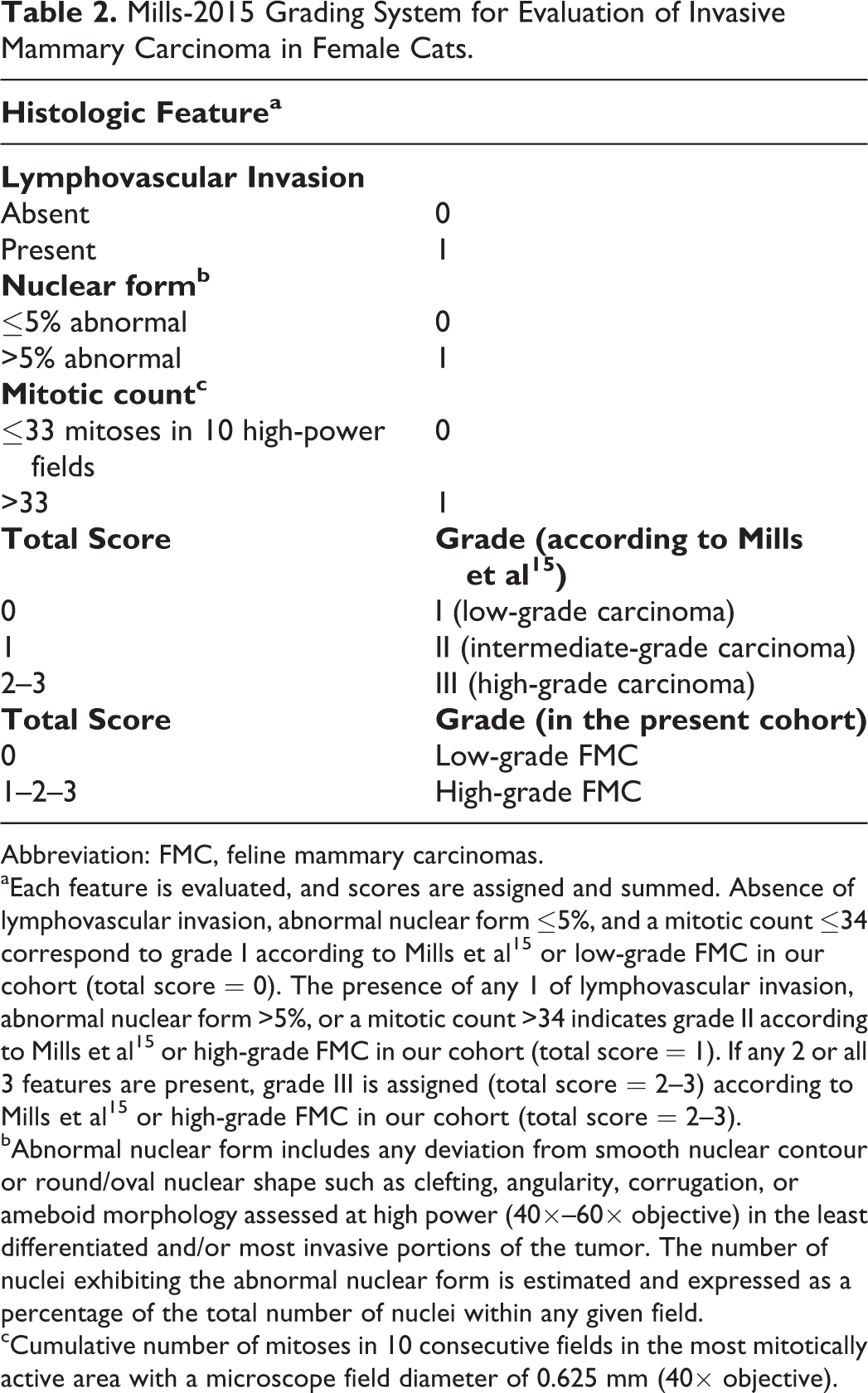
Abbreviation: FMC, feline mammary carcinomas.
aEach feature is evaluated, and scores are assigned and summed. Absence of lymphovascular invasion, abnormal nuclear form ≤5%, and a mitotic count ≤34 correspond to grade I according to Mills et al 15 or low-grade FMC in our cohort (total score = 0). The presence of any 1 of lymphovascular invasion, abnormal nuclear form >5%, or a mitotic count >34 indicates grade II according to Mills et al 15 or high-grade FMC in our cohort (total score = 1). If any 2 or all 3 features are present, grade III is assigned (total score = 2–3) according to Mills et al 15 or high-grade FMC in our cohort (total score = 2–3).
bAbnormal nuclear form includes any deviation from smooth nuclear contour or round/oval nuclear shape such as clefting, angularity, corrugation, or ameboid morphology assessed at high power (40×–60× objective) in the least differentiated and/or most invasive portions of the tumor. The number of nuclei exhibiting the abnormal nuclear form is estimated and expressed as a percentage of the total number of nuclei within any given field.
cCumulative number of mitoses in 10 consecutive fields in the most mitotically active area with a microscope field diameter of 0.625 mm (40× objective).
Survival Analysis
All cases were followed up for at least 2 years with meticulous emphasis on locoregional relapse (local recurrence and/or lymph node metastasis) and distant metastasis. Overall survival was defined as the time period between mastectomy and death from any cause, including death attributable to the mammary carcinoma. Specific survival was defined as the time period between mastectomy and death attributable to the mammary carcinoma. Uncensored cases in overall survival analyses corresponded to animals that died during the follow-up period (ie, uncensored cases are those in which the studied event, death from any cause, occurred during the follow-up period). Censored cases in overall survival analyses (ie, in which the studied event was not observed) corresponded to animals alive at the end of the follow-up period, which in this study was not shorter than 730 days (2 years). Uncensored cases in specific survival analyses corresponded to animals that died from cancer during the follow-up period. Censored cases in specific survival analyses corresponded to animals alive at the end of the follow-up period, animals that died from a cause unrelated to cancer, and animals that died from unknown cause.
Statistical Analyses
Statistical analyses were conducted using the MedCalc statistical software (Ostend, Belgium). The Kaplan-Meier method and log-rank tests were used to assess overall survival and cancer-specific survival in univariate survival analyses, and Cox proportional hazards models were used for multivariate survival analyses. The results are reported using the hazard ratio (HR), its 95% confidence interval (95% CI), and the P value of each covariate. A P value equal or less than .05 was considered significant. The data analyzed in this study are available from the corresponding author on reasonable request.
Results
Epidemiologic Data
The cohort comprised 342 female cats with stages I through III invasive feline mammary carcinomas. The mean age at diagnosis was 11.2 ± 2.7 years (median = 11.1, range, 4.0–21.3 years). The cats were mainly European (297/342, 86.8%), 34 were pure-breed cats, including Siamese (n = 17), Persians (n = 6), Chartreux (n = 4), Birman (n = 3), Bombay, British Short Hair, Norwegian, and Oriental (n = 1 each). Eleven cats were mixed-bred, including 5 cross-Siamese and 4 cross-Persian cats.
Almost half of the cohort (163/342, 48%) were spayed (by ovariectomy or ovariohysterectomy) before the diagnosis of mammary carcinoma, and slightly more than half of the cats were intact females (179/342, 52%). Among intact female cats, it should be noted that 59 cats were spayed at the time of diagnosis of mammary carcinoma. Very few cats were sterilized early, before the age of 2 years (15/342, 4%). More than one-third of the cats (120/342, 35%) were not spayed all.
Clinicopathologic Data
The cohort comprised 293 of 342 (85.7%) single invasive mammary carcinomas and 49 of 342 (14.3%) multiple (within a given mammary gland) and multicentric (affecting more than 1 mammary gland) invasive mammary carcinomas. The histological types encountered in decreasing order of frequency were cribriform (171/342, 50.0%), solid (78/342, 22.8%), tubulopapillary (56/342, 16.3%), and mucinous (37/342, 10.8%). The mean pathologic tumor size was 17.9 ± 7.4 mm, with a median of 17.0 mm and a range of 3.0 to 48.0 mm. Lymphovascular invasion was confirmed in 168 of 342 cases (49.1%), central necrosis in 307 of 342 cases (89.7%), squamous differentiation in 157 of 342 cases (45.9%), and moderate to severe tumor-associated lymphohistiocytic and plasmacytic inflammation in 176 of 342 cases (51.4%).
Histological Grading Systems
According to the EE grading system, the cohort comprised 10 of 342 (3.0%) grade I feline invasive mammary carcinomas, 172 of 342 (50.2%) grade II cases, and 160 of 342 (46.8%) grade III cases. In the MMEE grading system, the cohort comprised 75 of 342 (21.9%) MMEE-grade I cases, 204 of 342 (59.7%) MMEE-grade II cases, and 63 of 342 (18.4%) MMEE-grade III cases. In the REE system, there were 104 of 342 (30.4%) REE-grade I carcinomas, 196 of 342 (57.3%) REE-grade II carcinomas, and 42 of 342 (12.3%) REE-grade III carcinomas. In the REE/LVI grading system, there were 69 of 342 (20.2%) REE/LVI-grade I cases, 179 of 342 (52.3%) REE/LVI-grade II cases, and 94 of 342 (27.5%) REE/LVI-grade III cases. Finally, based on the grading system proposed by Mills et al, 15 which takes into account lymphovascular invasion, the nuclear form at threshold >5% abnormal, and the mitotic count at threshold >33 mitoses in 10 high-power fields (Table 2), there were 15 of 342 (4.4%) Mills-2015 grade I carcinomas, 78 of 342 (22.8%) Mills-2015 grade II carcinomas, and 249 of 342 (72.8%) Mills-2015 grade III carcinomas.
Survival Analyses
Results of Kaplan-Meier survival analyses and log-rank tests regarding overall and cancer-specific survival according to patient age at diagnosis, spaying status, pathologic tumor size, lymph node metastasis, WHO stage, histologic type, lymphovascular invasion, tumor-associated inflammation, central necrosis, squamous differentiation, tubule formation, nuclear pleomorphism, nuclear form, and mitotic count are listed in Table 3.
Univariate Survival Analysis of Selected Clinicopathologic Criteria With Respect to Overall Survival and Specific Survival in Female Cats With Invasive Mammary Carcinoma.
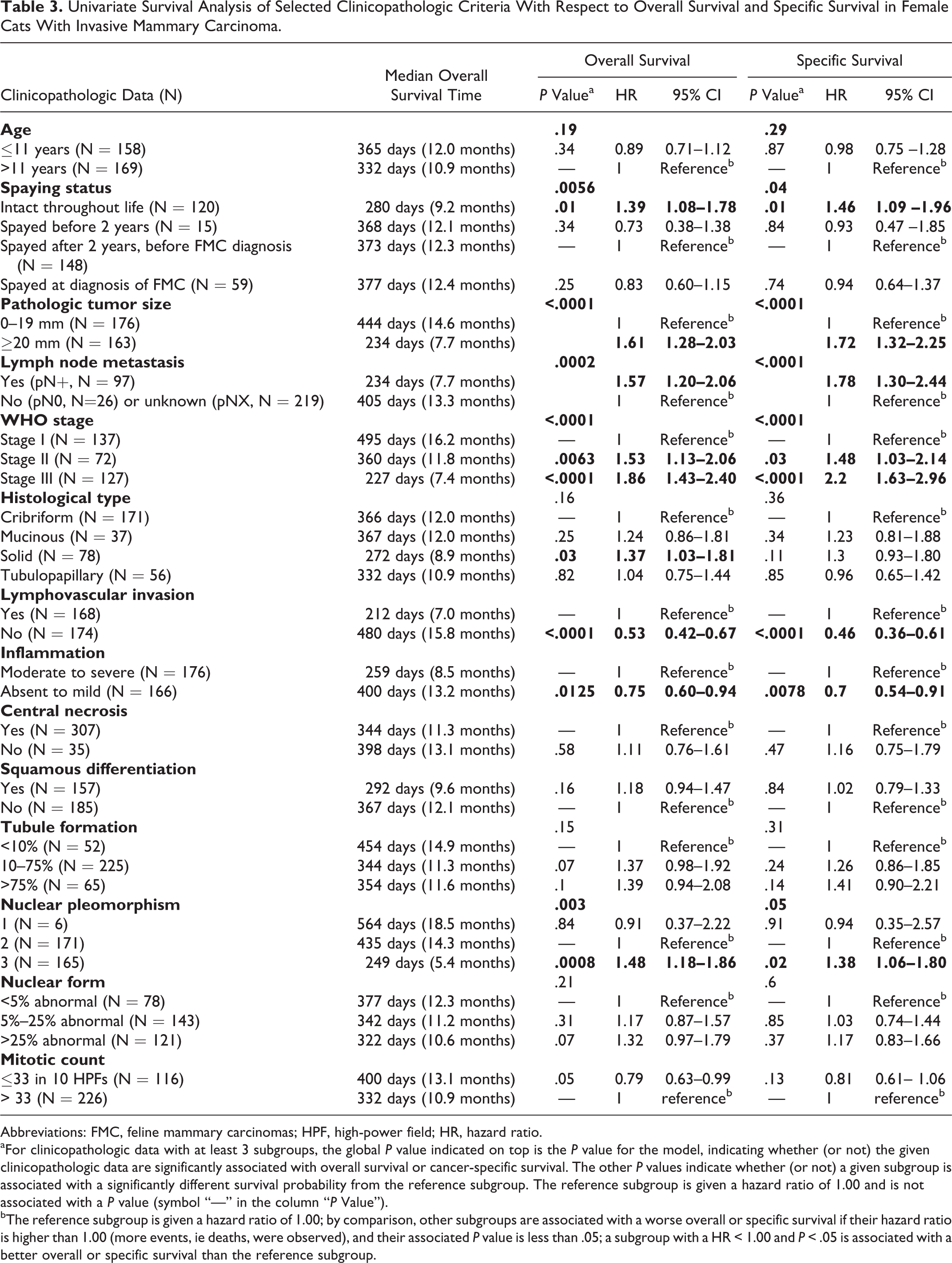
Abbreviations: FMC, feline mammary carcinomas; HPF, high-power field; HR, hazard ratio.
aFor clinicopathologic data with at least 3 subgroups, the global P value indicated on top is the P value for the model, indicating whether (or not) the given clinicopathologic data are significantly associated with overall survival or cancer-specific survival. The other P values indicate whether (or not) a given subgroup is associated with a significantly different survival probability from the reference subgroup. The reference subgroup is given a hazard ratio of 1.00 and is not associated with a P value (symbol “—” in the column “P Value”).
bThe reference subgroup is given a hazard ratio of 1.00; by comparison, other subgroups are associated with a worse overall or specific survival if their hazard ratio is higher than 1.00 (more events, ie deaths, were observed), and their associated P value is less than .05; a subgroup with a HR < 1.00 and P < .05 is associated with a better overall or specific survival than the reference subgroup.
Regarding overall survival, a larger pathologic tumor size (≥20 mm, HR = 1.61; P < .0001), the presence of lymphovascular invasion (HR = 1.89; P < .0001), lymph node metastasis (pN+, HR = 1.57; P = .0002), a more advanced WHO stage (P < .0001), a moderate to severe tumor-associated inflammation (HR = 1.33; P = .0125), and a higher mitotic count (cutoff value of 33, HR = 1.27; P = .05 being almost significant) were all associated with a worse overall survival (Table 3). Regarding cancer-specific survival, a larger pathologic tumor size (≥20 mm, HR = 1.72; P < .0001), the presence of lymphovascular invasion (HR = 2.17; P < .0001), lymph node metastasis (pN+, HR = 1.78; P < .0001), a more advanced WHO stage (P < .0001), and a moderate to severe tumor-associated inflammation (HR = 1.43; P = .0078) were all associated with a worse specific survival (Table 3).
The EE grading system was significantly associated with overall survival (P = .0194, Cox proportional-hazards model, Fig. 4). More precisely, the 160 histological grade III carcinomas (HR = 1.37; 95% CI, 1.09–1.73) were significantly associated with a worse overall survival than grade II feline mammary carcinomas (HR = 1.00, reference), whereas there was no significant difference in overall survival between the 10 cats with grade I carcinomas and the 172 cats with grade II carcinomas. The EE grading system was not significantly associated with specific survival (P = .0752, Cox proportional hazards model).
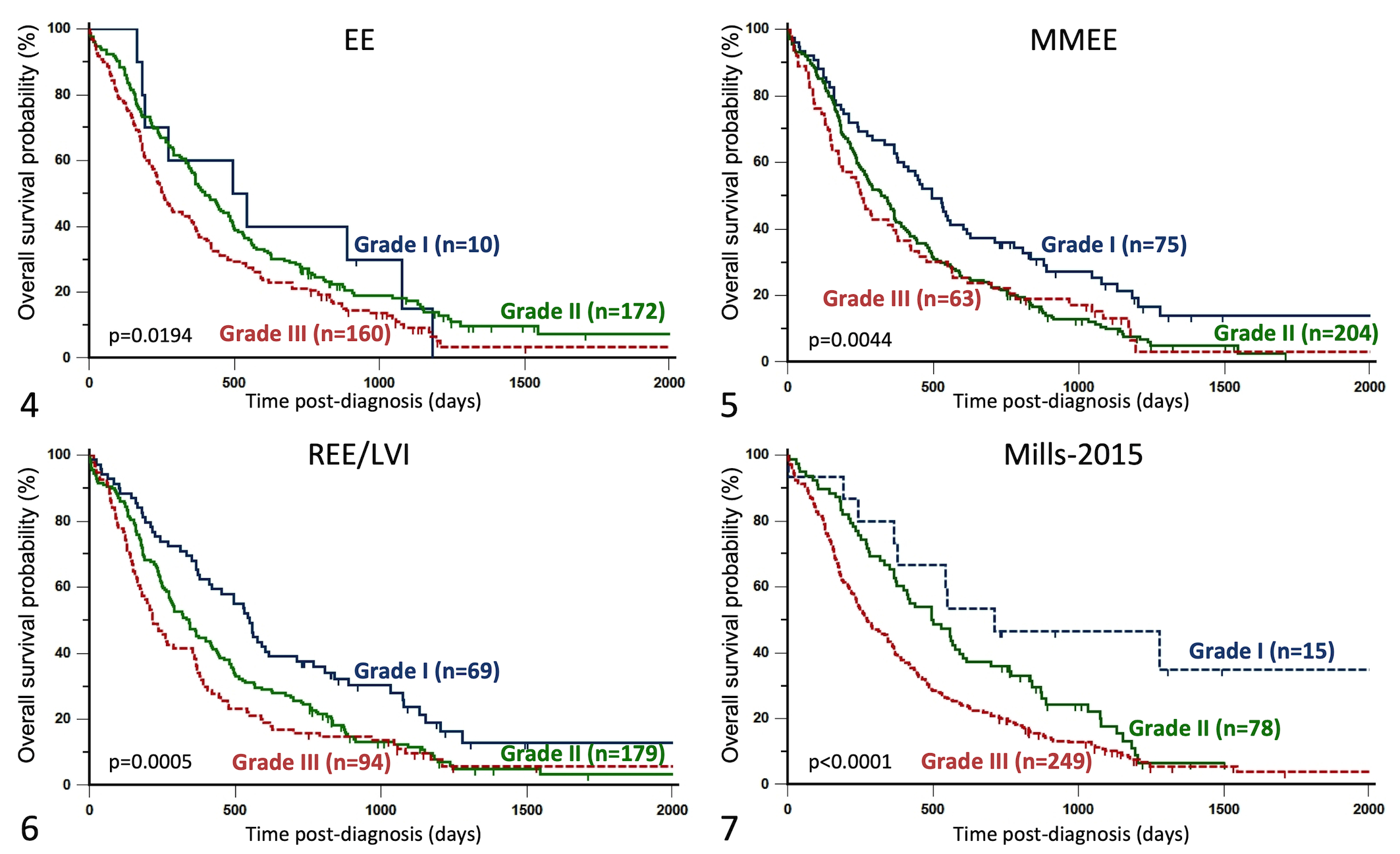
Kaplan-Meier curves depicting overall survival of female cats with invasive mammary carcinomas.
The MMEE grading system was significantly associated with overall survival (P = .0044), MMEE-grade III carcinomas were significantly (P = .0062; HR = 1.66; 95% CI, 1.16–2.38) associated with poorer overall survival than MMEE-grade I carcinomas, whereas MMEE-grade II carcinomas (P = .0034; HR = 1.55; 95% CI, 1.16–2.08) were significantly different from MMEE-grade I carcinomas with respect to overall survival (Fig. 5). The MMEE grading system was also significantly associated with specific survival (P = .0408); MMEE-grade III carcinomas were significantly (P = .0309; HR = 1.59; 95% CI, 1.05–2.41) associated with poorer specific survival than MMEE-grade I carcinomas, and MMEE-grade II carcinomas (P = .0265; HR = 1.47; 95% CI, 1.05–2.06) were significantly different from MMEE-grade I carcinomas with respect to specific survival.
By multivariate survival analysis, according to the MMEE grading system, MMEE-grade III carcinomas (P = .0466, HR = 1.46, 95% CI, 1.01–2.11), MMEE-grade II carcinomas (P = .0329, HR = 1.39, 95% CI, 1.03–1.88), and MMEE-grade I carcinomas (HR = 1.00, reference) with decreasing hazard ratios were significantly associated with a worse overall survival, independently from the pathologic tumor size (pT ≥20 mm: P = .0021, HR = 1.45, 95% CI, 1.15–1.83) and positive nodal stage (P = .0012, HR = 1.51, 95% CI, 1.18–1.94). By multivariate analysis regarding cancer-specific survival, MMEE-grade III carcinomas (P = .0303, HR = 1.59, 95% CI, 1.05–2.41), MMEE-grade II carcinomas (P = .0220, HR = 1.49, 95% CI, 1.06–2.08), and MMEE-grade I carcinomas (HR = 1.00, reference) with decreasing hazard ratios were significantly associated with a worse specific survival, independently from a positive nodal stage (P < .0001, HR = 1.82, 95% CI, 1.38–2.41).
The REE grading system was first analyzed without including lymphovascular invasion, and the results were significantly associated with overall survival (P = .0364), but the 42 REE-grade III FMCs did not significantly differ from the 104 REE-grade I FMCs (P = .2577); there was a significantly worse overall survival for the 196 REE-grade II FMCs compared to REE-grade I FMCs (P = .0114, HR = 1.40, 95% CI, 1.08–1.80). The REE grading system without including lymphovascular invasion was not significantly associated with specific survival (P = .0746, Cox proportional-hazards model).
The REE grading system that included lymphovascular invasion (REE/LVI) was significantly associated with overall survival (P = .0005), with its 3 grading categories (I, II, and III) being of increasing risk for all-cause mortality (Fig. 6). Compared to REE/LVI-grade I mammary carcinomas considered as the reference category (HR=1.00), REE/LVI-grade II carcinomas (HR = 1.56; 95% CI, 1.14–2.11; P = .0050) and REE/LVI-grade III carcinomas (HR = 1.93; 95% CI, 1.38–2.71; P = .0002) were associated with a significantly poorer overall survival. The REE grading system that included lymphovascular invasion (REE/LVI) was also significantly associated with specific survival (P = .0018). Compared to REE/LVI-grade I mammary carcinomas considered as the reference category (HR = 1.00), REE/LVI-grade II carcinomas (HR = 1.60; 95% CI, 1.11–2.30; P = .0118) and REE/LVI-grade III carcinomas (HR = 2.02; 95% CI, 1.35–3.00; P = .0006) were associated with a significantly greater risk of cancer-related death.
By multivariate analysis regarding overall survival, according to the REE/LVI grading system, REE/LVI-grade III carcinomas (P = .0099, HR = 1.58, 95% CI, 1.12–2.24), REE/LVI-grade II carcinomas (P = .0285, HR = 1.42, 95% CI, 1.04–1.93), and REE/LVI-grade I carcinomas (HR = 1.00, reference) with decreasing hazard ratios were significantly associated with a worse overall survival, independently from the pathologic tumor size (pT ≥20 mm: P = .0010, HR = 1.47, 95% CI, 1.17–1.85) and a positive nodal status (pN+, P = .0052, HR = 1.43, 95% CI, 1.11–1.83). Regarding cancer-specific survival by multivariate analysis, REE/LVI-grade III carcinomas (P = .0262, HR = 1.59, 95% CI, 1.06–2.40), REE/LVI-grade II carcinomas (P = .0505, HR = 1.44, 95% CI, 1.00–2.09), and REE/LVI-grade I carcinomas (HR = 1.00, reference) with decreasing hazard ratios were associated with a worse specific survival, independently from the pathologic tumor size (pT ≥20 mm: P = .0014, HR = 1.55, 95% CI, 1.19–2.02) and a positive nodal status (pN+, P = .0009, HR = 1.61, 95% CI, 1.22–2.14).
The Mills-2015 grading system was significantly associated with overall survival (P < .0001; Cox proportional hazards regression). The 249 Mills-2015 grade III FMCs were associated with shorter overall survival (HR = 2.94; 95% CI, 1.51–5.73; P = .0017) compared to the 15 Mills-2015 grade I FMCs (HR = 1.00, reference); however, the 78 Mills-2015 grade II FMCs did not significantly differ in overall survival (HR = 1.94; 95% CI, 0.96–3.91; P = .0643) from Mills-2015 grade I FMCs (Fig. 7). The Mills-2015 grading system at ≥33 mitoses cutoff was also significantly associated with specific survival (P < .0001; Cox proportional hazards regression). The 249 Mills-2015 grade III FMCs were associated with shorter specific survival (HR = 2.28; 95% CI, 1.35–3.83; P = .0020) compared to the 15 Mills-2015 grade I FMCs (HR = 1.00, reference); however, the 78 Mills-2015 grade II FMCs did not significantly differ in specific survival (HR = 1.15; 95% CI, 0.68–1.96; P = .6049) from Mills-2015 grade I FMCs.
Afterward, Mills-2015 grade II and III tumors were merged together, and the results were significantly associated with overall survival (univariate survival analysis, P = .0031; HR = 2.43; 95% CI, 1.59–3.71 for high-grade FMCs compared to low-grade FMCs) and specific survival (univariate survival analysis, P = .0040; HR = 2.76; 95% CI, 1.22–6.20 for high-grade FMCs compared to low-grade FMCs).
By multivariate survival analysis, the high-grade carcinomas (grades II and III according to Mills-2015 grading system with adapted mitotic count cutoff value of 33) were significantly associated with a worse overall survival (P = .0139, HR = 2.33, 95% CI, 1.19–4.54), independently from the pathologic tumor size (pT ≥20 mm, P = .0008, HR = 1.48, 95% CI, 1.18–1.86) and a positive nodal status (pN+, P = .0018, HR = 1.49, 95% CI, 1.16–1.91). Also, the high-grade carcinomas (grades II and III according to Mills-2015 grading system with adapted mitotic count cutoff value of 33) were significantly associated with a worse specific survival (P = .0364, HR = 2.40, 95% CI, 1.06–5.43), independently from the pathologic tumor size (pT ≥20 mm, P = .0012, HR = 1.55, 95% CI, 1.19–2.03) and a positive nodal status (pN+, P = .0003, HR = 1.68, 95% CI, 1.27–2.23).
Discussion
Few veterinary studies have attempted to validate previously published tumor grading schemes in an independent cohort. The aim of our study was to evaluate and if possible validate the prognostic value of different histologic grading systems, including the EE grading system designed for human breast cancers, 5 and the modified and newly designed histologic grading systems published lately by Mills et al 15 for feline invasive mammary carcinomas. 15 In this purpose, we studied 342 stages I through III invasive mammary carcinomas in female cats (the largest retrospective FMC cohort described so far).
The histologic grade of invasive mammary carcinomas is defined minimally by 3 histologic parameters: tubule formation, nuclear pleomorphism, and mitotic count, although there exists variations in the criteria used to quantify these histological features. In human breast pathology for instance, the original Bloom and Richardson 1 grading system was modified by Elston and Ellis 5 to improve consistency and reproducibility. 5 In feline mammary carcinomas, there was a need to revise the classically used criteria defined by Elston and Ellis, notably because very few cases fall into the grade I subgroup. 15,30,31
In this study, the classic EE grading system 5 was applied, and although it was significantly associated with overall survival, the difference between grade I and grade II FMCs was not significant, as previously reported in feline mammary carcinomas. 2,11,14,23 However, grade I carcinomas were rare (10/342) and underrepresented when compared with grade II (172/342) and grade III (160/342) carcinomas. The low frequency of grade I FMCs was also reported by Mills et al 15 and Soares et al 26 and might be the consequence of the high mitotic counts of feline mammary carcinomas compared to human breast cancers. In Mills et al’s 15 study, only 2 of 108 (1.9%) FMCs were grade I, and the classic EE grading system was not significantly associated with cancer-specific survival. 15
The classic EE grading system has been previously used to grade FMCs. Castagnaro et al 2 and Millanta et al 14 associated the histological grade with postsurgery survival of queens with mammary carcinomas in univariate analysis but failed to demonstrate an independent prognostic value of the histological grade by multivariate analysis. Seixas et al 23 demonstrated by multivariate analysis that the histologic grade defined according to EE was an independent prognostic factor related to overall survival, with the presence of nodal metastasis as the independent covariate; but again, only a minority of the carcinomas were grade I (5/92, 5.4%). These findings warrant a more adapted and compatible grading system for feline invasive mammary carcinomas.
When analyzed separately, 2 of the histological criteria used to define the histological grade had or almost had prognostic significance in the present cohort: the mitotic count (with a cutoff value of 33 mitoses in 10 400× fields) was almost significantly associated with overall survival by univariate analysis (P = .050), and nuclear pleomorphism was significantly associated with overall survival (P = .003), similar to findings in previous studies, 23 including that of Mills et al 15 with respect to cancer-specific survival. In our study, the nuclear pleomorphism scores showed a significant correlation with overall survival for the second and third subcategories (5%–25% and ≥25% abnormal nuclei, respectively) in univariate survival analysis, whereas nuclear form was not significantly associated with overall survival. In the study performed by Mills et al, 15 nuclear pleomorphism and nuclear form scores were both found to be associated with specific survival in univariate survival analysis. There is thus a rationale for improving the definitions of the mitotic count scores and nuclear pleomorphism/nuclear form scores in feline mammary carcinomas. Three new grading systems were proposed by Mills et al 15 in an attempt to improve the histologic grading of feline mammary carcinoma.
First, the MMEE grading system adapts the range of mitotic count subcategories to better accommodate the high median and broad range of mitotic counts encountered within feline invasive mammary carcinomas, as described by Mills et al. 15 This modification improves the detection of the previously underrepresented grade I carcinomas in the classic EE grading system. In the present study, we confirm that an adaptation of the mitotic count threshold for feline mammary carcinomas has prognostic value with respect to overall and cancer-specific survival. Of note, the calculated threshold for the mitotic index in our cohort (≥33 mitoses in 10 high-power fields) differs from the threshold published by Mills et al 15 (>62 mitoses in 10 high-power fields). The >62 cutoff corresponds to the median mitotic count in Mills et al’s 15 cohort. In the present study, the median mitotic count was 44 mitoses in 10 high-power fields; the ≥33 mitoses cutoff was calculated by ROC curve analysis according to the 2-year survival rates of female cats included in the present study. This suggests that the thresholds used for the mitotic index in feline mammary carcinomas probably need in-house validation in a given laboratory for veterinary pathology before they can be used in prognostic purposes.
Then, the REE grading system proposed by Mills et al 15 was evaluated in our cohort. In this design, nuclear pleomorphism was replaced by a score for nuclear form in an attempt to reduce subjectivity, 15 although we felt that nuclear form is in practice as subjective as nuclear polymorphism to evaluate. In this REE grading system proposed by Mills et al, 15 lymphovascular invasion was also added. In our cohort, the REE system was associated with overall survival in univariate analysis, and the REE/LVI grading system was significantly associated with overall and cancer-specific survival in both univariate and multivariate analyses, independently from increased pathologic tumor size and positive nodal stage. Of note, the REE/LVI grading system was associated with overall survival although 1 of its main parameters (nuclear form) was not significantly associated with overall survival (P = .21). This is probably mainly due to robustness of lymphovascular invasion as a prognostic factor in feline mammary carcinomas in general 19,21,23,28 and in our cohort more specifically. Although valuable prognostically, lymphovascular invasion represents a main weakness of this grading system because it refers to the histological stage of feline mammary carcinomas (ie, the extent of cancer within the host) rather than to the histological grade (which is a reflection of cancer cell differentiation, proliferation, and atypia).
A novel grading system was also developed by Mills et al 15 and included lymphovascular invasion, mitotic count, and nuclear form. As explained in the methods, mitotic count was adapted to our cohort with a cutoff value of 33 in contrast to 62 mitoses in 10 high-power fields in the study of Mills et al. 15 Using the Mills-2015 grading system and after gathering grade II and III carcinomas for analysis, the Mills-2015 grading system proved to be associated with overall and cancer-specific survival in univariate and multivariate analyses, independently from the pathologic tumor size, nodal stage, and distant metastasis. In their study, Mills et al 15 also observed, by univariate survival analysis, the association of their grading system with specific survival. However, with this Mills-2015 grading system, grade I carcinomas were underrepresented in our cohort (n = 15/342, 4.4%), whereas they constituted 20.3% (22/108) of Mills et al’s 15 cohort. A low frequency of grade I FMCs according to Mills-2015 grading system (n = 5/61, 8.2%) was also reported by Soares et al. 26 Although we found that the Mills-2015 grading system was significantly associated with overall and cancer-specific survival, the nuclear form, which is part of its definition, was not of prognostic value in our retrospective study. Thus, again, the strong prognostic value of the Mills-2015 grading system is possibly due to the robustness of lymphovascular invasion as a prognostic factor, but lymphovascular invasion is a feature of the pathologic stage of invasive mammary carcinomas rather than a feature of histological grade of malignancy.
Lymphovascular invasion, the presence of neoplastic emboli within lymph and/or blood vessels, is one of the strongest prognostic factors in female cats with invasive mammary carcinomas. 15,19,21,23,28,29 In this study, in case of doubt on HES slides, lymphovascular invasion was confirmed (or not) using immunohistochemistry to the LMO2 (LIM domain-only protein-2) transcription factor, which gives a nuclear signal in lymphatic endothelial cells, whereas in Mills et al’s 15 study, lymphovascular invasion was assessed by immunohistochemistry to von Willebrand factor. Indeed, lymphovascular invasion may be difficult to objectify, either because it may resemble technical retraction artifacts on paraffin sections or the lymphatic vessels may be completely obstructed by carcinoma cells. In our opinion, the immunolabeling of lymphatic endothelial cells is very helpful for lymphovascular invasion confirmation and represents a helpful prognostic tool, especially when the regional lymph node was not sampled, to assess whether metastatic spread by the lymphatic route was in process.
In conclusion, the classic EE grading system, originally designed for human breast cancers but commonly used in cats, can be adapted to feline invasive mammary carcinomas, especially regarding the 3 points attributed to the mitotic count. Its application in our retrospective cohort showed a significant association with overall survival, although grade I carcinomas are underrepresented in cats. Lymphovascular invasion is a robust prognostic factor in feline mammary carcinomas, but its use as a prognostic factor should be independent from any grading system. Adapting the number of mitoses might be the best strategy to better categorize the highly proliferative mammary carcinomas encountered in the feline species, so the MMEE grading system seems to be a good way to improve routine diagnostic evaluation and prognostication of female cats with invasive mammary carcinoma.
Footnotes
Acknowledgements
We deeply acknowledge Dr. Anne Patsouris (medical oncologist, ICO Integrated Center for Oncology, Angers, France) and Dr. Catherine Ibisch (veterinary oncologist, AMaROC, Oniris, Nantes, France) for their help in reviewing the manuscript. The authors thank Dr. Mélanie Pohu, Dr. Floriane Morio, and Dr. Clotilde de Brito, who helped in collecting the clinical and follow-up data. The authors also thank the veterinary pathologists (Dr. Jean-Loïc Le Net, Dr. Virginie Théau, Dr. Pierre Lagourette, Dr. Olivier Albaric, and Dr. Sophie Labrut) who performed the initial diagnoses of feline mammary carcinomas as well as the technicians in histopathology (Mr. Bernard Fernandez, Mrs. Florence Lézin, and Mrs. Catherine Guéreaud), who made the slides. Finally, we thank the referring veterinarians and the owners of the cats included in this study, who gave us the clinical and follow-up data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the French National Cancer Institute (INCa, Institut National du Cancer) with a grant for translational research (INCa-DHOS 2010, Pr. M. Campone); by a grant for PhD students from the Ministry of Education and Higher Education of Lebanon (Dr. Elie Dagher); and by Roche Diagnostics GmbH, Germany, which provided financial and technical support for the immunohistochemical characterization of the carcinomas. The funders had no role in study design, data collection, analysis and interpretation, decision to publish, or preparation of the manuscript.