
Abstract
This report describes the clinical presentation, diagnosis, and histopathologic features of oculodermal melanocytosis in a young dog. A 3-year-old male neutered Labrador Retriever presented with conjunctival and scleral hyperpigmentation of the right eye, with concurrent ipsilateral cutaneous hyperpigmentation involving the right side of the face. Initial skin and conjunctival biopsies revealed an accumulation of histologically benign melanocytes within the dermis and conjunctival stroma, respectively. Enucleation was elected 19 months later by the referring veterinarian due to the progression of ocular pigmentation with concurrent marked corneal lipidosis and the suspicion of a scleral mass. On gross and histopathologic examination of the globe, there was marked panuveal melanocytosis with extension into the sclera, bulbar conjunctiva, and connective tissue surrounding the optic nerve, as well as sharply demarcated ipsilateral hyperpigmentation of the facial skin. The findings are characteristic of oculodermal melanocytosis (nevus of Ota), a dermal melanocytic hamartoma presenting as cutaneous facial hyperpigmentation that corresponds to the distribution of the ophthalmic and maxillary branches of the trigeminal nerve, often with ipsilateral ocular involvement.
Nevus of Ota describes an uncommon dermal melanocytic hamartoma that presents as unilateral bluish facial cutaneous hyperpigmentation corresponding to the distribution of the ophthalmic and maxillary branches of the trigeminal nerve. The pathogenesis is suspected to involve aberrant migration of melanocytes from the neural crest to the epidermis at the embryonic stage of development. 20 Concurrent ipsilateral ocular and/or oral hyperpigmentation is commonly reported in human patients characterizing the histopathologic lesion as oculodermal melanocytosis. These patients are at increased risk of developing uveal melanoma, as well as melanoma of the ipsilateral skin, orbit, and meninges. The clinical findings of nevus of Ota have previously been reported in a young dog. 11
A 3-year-old, male neutered Labrador Retriever dog was referred for evaluation of abnormal ocular pigmentation in the right eye. At initial presentation, the referring veterinary surgeon reported a 2-mm white opacity affecting the central cornea as well as dark pigmentation at the level of the dorsolateral limbus and sclera of the right eye. Intraocular pressure readings of 11 and 12 mm Hg were recorded in the left and right eye, respectively, at the time. Despite the fact that no obvious ocular discomfort was observed, the dog was referred due to the concern that these changes could represent a neoplastic process (ocular melanoma).
A complete ophthalmic examination revealed that both eyes were visual comfortable and free of discharge with normal menace response as well as dazzle reflex. Direct and indirect pupillary light reflexes were also present. Schirmer tear test was within reference interval in both eyes (15–25 mm/min). Slit-lamp examination showed the presence of corneal lipidosis affecting the axial cornea of the right eye. Extensive pigmentation involving all aspects of the conjunctiva, sclera, limbus, and peripheral corneal epithelium was present in the right eye. Examination of the left eye was within normal limits. Aqueous flare was absent in both eyes. Intraocular pressure readings of 13 mm Hg and 14 mm Hg were recorded in the right and left eye, respectively, obtained using applanation tonometry (Tono Pen Avia Vet; Reichert, Depew, NY). Direct and indirect ophthalmoscopy following pupil dilation was consistent with a healthy optic nerve head and a normal retina in the left eye but revealed a pigmented peripapillary area affecting the retina around the optic nerve of the right eye. Fluorescein staining was negative in both eyes. B-mode ocular ultrasound revealed a mildly raised and thickened optic nerve head but an otherwise normal right globe.
In addition, the hair color of the frontal area of the head was slightly darker on the right side of the face with a clear demarcation especially in the midline. According to the owner, this pigmentation pattern had been present since the dog was a puppy but had become more obvious in the past year (Figs. 1, 2). Physical examination was within normal limits, and examination of the oral mucosa did not reveal any hyperpigmentation in either side of the face. At this time, differential diagnosis included nevus of Ota, ocular melanosis, ocular melanoma, or limbal melanoma.
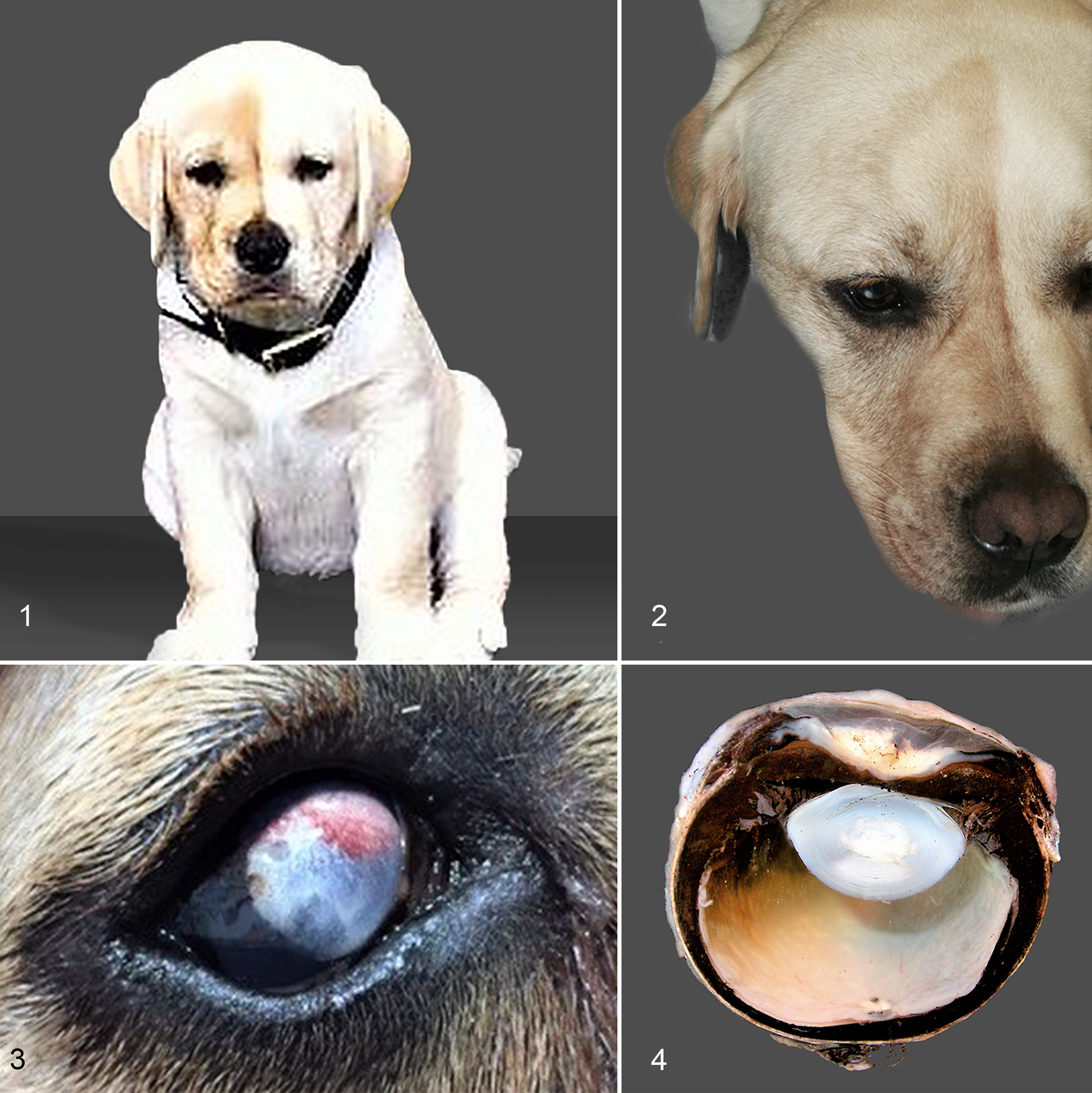
Oculodermal melanocytosis, dog.
After discussion with the owner, further investigation and workup for this condition were recommended to rule out neoplasia. Hematology and biochemistry were within their reference intervals, and skin and conjunctival biopsies were performed under general anesthesia. The area of the pigmented skin and the right eye were aseptically prepared with 4% w/v chlorhexidine gluconate (Hibitane) and 1:10 povidone iodine solution, respectively. One conjunctival and 3 punch skin biopsies were obtained for histological evaluation. The patient was discharged the same day with a plan to monitor the intraocular pressures and the progress of the pigmentation every 2 months.
Histopathologic examination of the conjunctival biopsy specimen revealed numerous polygonal to fusiform melanocytes within the superficial stroma, with absence of atypia. A similar dermal population of melanocytes was identified in the skin biopsy specimen accompanied by mild epidermal pigmentation.
Nineteen months after initial presentation, a firm scleral mass was noticed on the dorsal limbus of the right eye, and the eye was considered nonvisual by the referring veterinarian (Fig. 3). At this stage, the owner declined further referral, and it was elected to enucleate the eye.
Gross examination of the formalin-fixed globe showed marked pigmentation and thickening of the choroid that extended to the ciliary body and iris (Fig. 4). Histologically, the uveal tract was diffusely expanded by densely packed, heavily pigmented polygonal cells (Fig. 6). These cells partially effaced the drainage angle, dissected beneath the terminus of Descemet’s membrane (Fig. 6), extended into the anterior to mid-sclera and bulbar conjunctiva, surrounded the optic nerve, and were also evident in the perivascular interstitium of the optic nerve head. In addition, low numbers of pigmented cells were evident in the peripapillary retina (Fig. 5). The pigmented cells contained abundant melanin and single small, round bland nuclei with indistinct nucleoli. Mitotic figures were not present (Fig. 7). A bleached section highlighted a uniform nuclear morphology and absence of mitotic activity (Fig. 8).
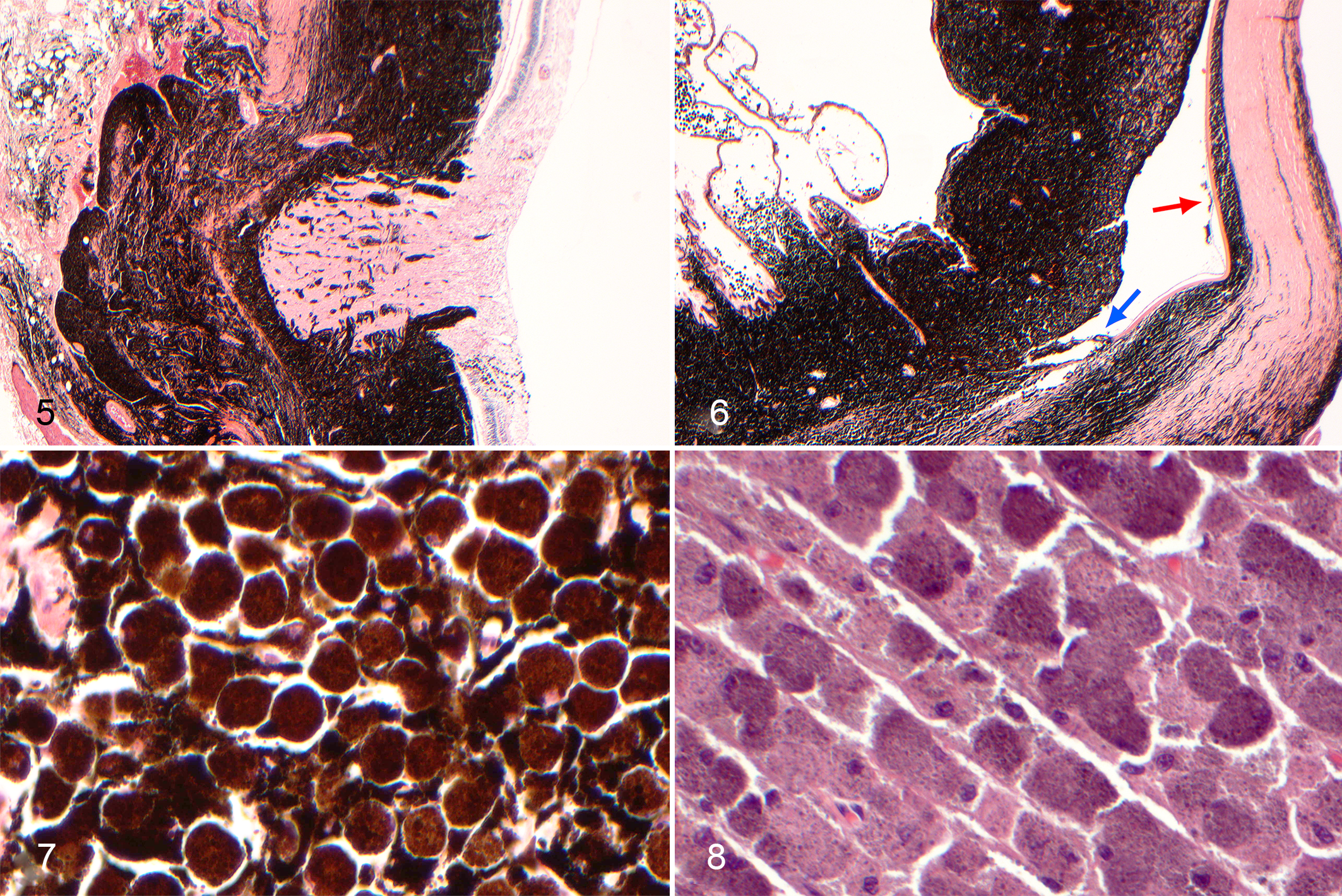
Oculodermal melanocytosis, right eye, dog, hematoxylin and eosin.
A histopathologic diagnosis of uveal melanosis was made. Additional findings in the posterior segment included pathological detachment of the ventral retina and mild inner retinal atrophy with some ganglion cell loss in the nontapetal retina, suggestive of glaucoma. Additional findings in the anterior segment included corneal lipidosis associated with stromal neovascularization, mild keratitis, and fibrosis.
Given the young age at initial presentation, as well as the location of the pigment along the branches of the ophthalmic and maxillary divisions of the trigeminal nerve in combination with the ocular changes and the histopathologic appearance of both the skin and the globe, the diagnosis of nevus of Ota was made. The dog remained healthy at 46 months after initial presentation with no signs of pain or discomfort and a normotensive and visual left eye.
The presentation of this case is similar to that previously reported in humans. Nevus of Ota is widely considered to be a form of dermal melanocytic hamartoma. This unusual syndrome typically occurs as a grayish-blue, macular discoloration affecting the ipsilateral facial skin in the area of the distribution of the corresponding ophthalmic and maxillary branches of the trigeminal nerve. 10 Therefore, early diagnosis and recognition of this condition will help prevent unnecessarily aggressive treatment as this condition may cause an animal no issues in its lifetime.
This condition was defined as an entity by Ota, in 1939, who named it nevus fuscocaeruleus ophthalmomaxillaris. 3,4 Since then, this melanocytic nevus has been widely known as nevus of Ota. Other names for the same condition include congenital melanosis bulbi, melanosis bulborum and aberrant Mongolian spots, progressive melanosis oculi, persistent aberrant Mongolian spots, patch-like pigmentation, oculodermal melanocytosis, melanocytosis dermo-ocular, and oculomuco-dermal melanocytosis. 10,18
The condition in humans occurs commonly in Asians (0.014%–0.034% prevalence) but rarely in whites, suggesting genetic influences. 4,19 It usually appears at birth and is more common in females, with a male/female ratio of 1:4.8. 1 It is unilateral in 95% of cases and may involve ocular and oral mucosal surfaces in addition to skin. 5,16,17 The condition is generally benign and persists for life. However, this rare disorder has been associated with ocular complications, such as glaucoma (10.3%) and uveal melanoma (1:400), that may be vision- or life-threatening. 21 Among the ocular complications, orbital melanoma has also been reported, 8,14 hence the need for detailed ophthalmic and systemic examination. Cases where the nevus of Ota involves all 3 branches of the trigeminal nerve have also been reported. 9
Nevus of Ota and other dermal melanocytic disorders such as blue nevus or Mongolian spots are believed to develop from melanocytes that have not migrated completely on their way to the epidermis from the neural crest during development. 20 These conditions may represent different stages of the same process. 7 It has also been suggested that the nevoid cells originate from Schwann cells or other neural elements and that abnormalities of neural crest migration lead to the development of these congenital dermal melanoses. 10 The exact embryologic events that result in such abnormalities are unknown, but changes in the local embryonic environment could be important. 2 The phenotype (nevus of Ota, Mongolian spot, or blue nevus) and the extent of involvement depend upon the stage at which the change occurs, as well as the extent of that change. 4,6
With regard to current veterinary terminology, distinction between benign uveal melanosis and diffuse uveal melanocytoma is based on the absence of a clear proliferative spindle melanocyte population in the former. Both, however, reflect benign melanocytic proliferation.
Congenital ocular melanocytosis can be broadly divided into ocular melanocytosis and oculodermal melanocytosis (nevus of Ota). Both conditions have similar increased scleral and uveal pigmentation, but the nevus of Ota has periocular hyperpigmentation as well. 25 Both conditions can predispose the patient to melanoma. The histopathology of ocular melanocytosis is characterized by densely packed and heavily pigmented melanocytes within the affected uveal tract, similar to what is described in this case. 22 The terms melanosis and melanocytosis appear to be interchangeable throughout the human and veterinary literature.
Enucleation in not common in human patients. In the few cases where histopathology of the globe was available, examination revealed melanocytic proliferation in the conjunctiva, iris, ciliary body, choroid, and sclera. 15,20
A similar condition where ocular melanosis occurs in combination with secondary glaucoma has been well documented in Cairn Terriers 23 with unilateral or bilateral involvement. Histologically, this is similar to ocular melanocytosis reported in human patients and is not considered neoplastic. 12,13
Treatment options in human patients include laser therapy, surgical removal, skin grafting, dermabrasion, and cryotherapy, but none of these have ever been satisfactory. 1,24 In animals, cosmetic camouflage of the marking does not seem necessary. However, if the eye is involved, it is appropriate to monitor the pigmentation progress, and regular ophthalmic examinations appear to be essential to detect early a secondary glaucoma or evidence that would support neoplastic transformation.
Nevus of Ota involves hyperpigmentation along the branches of the ophthalmic and maxillary divisions of the trigeminal nerve. Diagnosis is largely clinical but may be confirmed by histopathology and immunohistochemistry. Possible concomitant involvement of the ocular and buccal mucosa warrants a thorough ophthalmic examination and examination of the oral cavity. Histopathology is essential to confirm this condition as well as to exclude melanoma.
Footnotes
Acknowledgements
We thank Andrew Ketteridge, BVSc, BSc, MRCVS, for providing the clinical photographs (Figs. 1, 3) used with permission in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.