
Abstract
Canine splenic lymphoid nodules are currently classified as indolent lymphomas (marginal zone lymphoma [MZL], mantle cell lymphoma [MCL]) or nodular hyperplasia (lymphoid [LNH] or complex [CNH] type). Their differentiation can be difficult on morphology, because of similar histologic appearance and poorly defined diagnostic criteria. Thirty-five surgical samples of splenic lymphoid nodules were reviewed in order to assess the diagnostic contribution of immunophenotyping, proliferative activity and clonality (PARR) in differentiating between hyperplastic and neoplastic lesions. Proliferative activity was evaluated by double immunolabeling for Ki-67 and CD79a, in order to separately assess the proliferative activity of B cells and non-B cells. Definitive diagnoses were MZL (n = 11), MCL (n = 4), LNH (n = 10), and CNH (n = 10). The overall concordance between histology and PARR was above 90%. Lymphomas had a significantly higher percentage of CD79a-positive areas (mean, 36.30%; P = .0004) and a higher B-cell proliferative activity (median Ki-67 index, 5.49%; P = .0012). The threshold value most accurately predicting a diagnosis of lymphoma was ≥28% of B-cell areas, with a Ki-67 index above 3%. Dogs were monitored for a median follow-up time of 870 days (IQR, 569-1225), and no relapses were documented. Overall median survival time was 1282 days. The combination of histology, immunohistochemistry and PARR can improve the diagnostic accuracy for canine splenic lymphoid nodules, although the long-term behavior of these lesions appears similar.
Canine splenic nodular lymphoid lesions are primarily composed of follicular aggregates of lymphocytes associated with a variable proportion of extravasated erythrocytes, hematopoietic precursors, plasma cells and stromal elements (fibroblasts, smooth muscle cells and histiocytes). 28 In the past, the majority of these lesions have fallen under the umbrella term of splenic fibrohistiocytic nodule (SFHN) and graded I-III based on the relative proportion of lymphoid and stromal cells. 4,24 More recently, the reclassification of canine splenic lymphoma has led to the identification of two types of low-grade (indolent) B cell lymphoma, namely marginal zone lymphoma (MZL) and mantle cell lymphoma (MCL). 26 –28 Moreover, Moore et al have proposed to categorize the hyperplastic lesions as lymphoid nodular hyperplasia (LNH) and complex nodular hyperplasia (CNH). 17
While these lesions are frequent in dogs, little information is available about their biologic behavior, because of the limited number of well-documented cases with a long-term follow-up in veterinary literature and of poorly standardized diagnostic criteria. Consequently, in the cases diagnosed as indolent lymphoma, the utility of adjuvant chemotherapy following splenectomy is still debated. 7,18,25,26,29
Immunophenotyping and clonality testing by PCR for antigen receptor rearrangement (PARR) are further diagnostic methods commonly used alongside histology to confirm a suspected lymphoma, but in the case of splenic indolent lymphoma, the presence of an accompanying polymorphic cell population could limit the accuracy of these techniques. The estimation of neoplastic cell proliferative activity with immunohistochemical markers like Ki-67 can be valuable in identifying tumors with a more aggressive biologic behavior. 3,14,30 The assessment of tumor growth fraction has proven prognostic significance in both human high- and low-grade lymphomas, and was correlated with tumor grade in canine lymphoma. 8,9,16,20 Ki-67 proliferation index has also been applied to differentiate canine nodal and intestinal lymphoma from benign hyperplastic/inflammatory lesions. 2,6
The main purpose of this study was to determine whether Ki-67 index, immunophenotyping and clonality assessment would be helpful in differentiating canine splenic indolent lymphoma from hyperplastic lymphoid or complex lesions. An additional aim was to assess the prognostic relevance of these diagnoses by gathering information on the long-term clinical course of the affected dogs.
Materials and Methods
Study Design and Inclusion Criteria
Medical records of the Veterinary Hospital at the Department of Veterinary Medical Sciences (University of Bologna, Italy) were retrospectively reviewed to identify dogs with splenic nodular lesions surgically removed between January 2008 and June 2017. The corresponding 4-μm-thick formalin-fixed and paraffin-embedded (FFPE) histologic samples, stained with hematoxylin and eosin (HE), were microscopically examined and only the nodules with a lymphoid component above 40% and arranged in follicular structures were included.
Clinical information recorded in all cases included signalment, clinical signs, number of splenic nodules, nodule diameter, additional abdominal ultrasound findings, hematologic abnormalities and clinical course. Dogs receiving adjuvant chemotherapy were excluded from the study.
Serial histologic sections were examined by immunohistochemistry for CD3 and CD79a for immunophenotype determination. Based on histologic and immunohistochemical findings, cases were classified as one of: – Lymphoid nodular hyperplasia: lesions composed of ≥70% lymphocytes with interspersed stromal/histiocytic cells (grade I SFHN); lymphocytes arranged in discrete to merging follicular structures, quite regular in shape and size, composed of both small and intermediate/large lymphocytes; regular presence of an outer ring of T-cells surrounding follicles. – Complex nodular hyperplasia: lymphoid component with characteristics similar to LNH, associated with proliferation of splenic stromal elements (fibroblasts, smooth muscle cells, histiocytes) accounting for more than 30% of the nodule section (grade II SFHN). – Marginal zone lymphoma: irregular and coalescing follicular structures composed predominantly of intermediate-sized B cells with a moderate amount of cytoplasm and single, large nucleoli; loss of T cells between merging follicles. – Mantle cell lymphoma: irregular and coalescing follicular structures composed predominantly of small B cells with a scant amount of cytoplasm and round or indented deeply stained nuclei lacking obvious nucleoli; loss of T cells between merging follicles.
The aforementioned diagnostic categories were obtained by combining the previously published criteria. The percentage of lymphoid cells proposed by Spangler and Kass to differentiate between grade I (70-99%) and grade II (40-69%) SFHNs was used in the present paper to classify cases as LNH or CNH, respectively. 17,24 Grade III SFHN (0-39% of lymphoid cells) or nodules with prominent stromal cell anisokaryosis and anisocytosis suggesting a splenic stromal sarcoma or a histiocytic sarcoma were not included in the study. 17,24
Replicate histologic sections were submitted to the laboratories of the Department of Comparative Biomedicine and Food Science (University of Padua, Italy) for clonality testing by PARR in the B-cell receptor immunoglobulin heavy chain (IgH) gene. Cases with no amplifiable DNA were excluded from the study. A new diagnosis was then established, by combining the histopathologic-immunohistochemical diagnosis with the results of clonality testing. The cases with a straightforward histologic diagnosis of lymphoma were all confirmed, regardless of PARR results. Conversely, the cases histologically diagnosed as LNH or CNH were reclassified as nodular lymphoma if the PARR indicated clonality, assuming a higher sensitivity of PARR in detecting the early cases of lymphoma. 12,13 In the cases with a polyclonal result despite a histological and immunohistochemical diagnosis of lymphoma, a PCR for T-cell receptor gamma (TCRγ) was also performed to exclude cross-lineage rearrangement.
For each case, the percentage of CD3- and CD79a-positive areas was assessed on image analysis, with the aim to identify a threshold value to discriminate lymphoma from other hyperplastic lesions. In addition, CD79a/Ki-67 double immunohistochemistry was performed to compare the proliferative activity of B cells and non-B cells between lymphoma and hyperplastic lesions.
The methods for each employed technique are fully detailed in the following paragraphs.
Immunohistochemistry
Three replicate sections from each case were immunolabelled for CD3, CD79a and a CD79a/Ki-67 double staining. Commercial mouse monoclonal anti-human antibodies (CD3, clone CD3-12, Leukocyte Antigen Biology Laboratory, Peter F. Moore, University of California, Davis, CA, USA; CD79a, clone HM57, Santa Cruz Biotechnology Inc., Dallas, TX, USA; Ki-67, clone MIB-1; Dako, Glostrup, Denmark) with validated reactivity in canine tissues were employed. 22,26
Endogenous peroxidase activity was blocked by incubation for 30 minutes with 0.3% hydrogen peroxide in methanol. For antigen retrieval, slides were microwaved at 750 W in pH 8.0 EDTA buffer for two cycles of 5 minutes (CD3, CD79a) or in pH 6.0 citrate buffer for 4 cycles of 5 minutes (CD79a/Ki-67 double staining). Sections were incubated overnight at 4°C in a humid chamber with the primary antibody. CD3 was diluted 1:20 in a blocking solution (10% goat serum in phosphate-buffered saline); CD79a was diluted 1:750 in blocking solution; for CD79a/Ki-67 double staining, antibodies were mixed together at a dilution of 1:1200 (CD79a) and 1:400 (Ki-67) in blocking solution.
Sites of primary antibody binding were identified by incubation with appropriate biotinylated secondary antibody (Dako) at a dilution of 1:200 in blocking solution. Sections were incubated with a commercial streptavidin-biotin-peroxidase kit (Vectastain Elite ABC Kit, Vector Laboratories, Burlingame, CA, USA) for 30 minutes; 3,3′-diaminobenzidine (DAB tablets, Diagnostic BioSystems, Pleasanton, CA, USA) was used as chromogen. Sections were counterstained with Papanicolaou’s hematoxylin, dehydrated and mounted.
Sections of canine lymph node were used as positive controls. Negative controls were obtained by omitting the primary antibody.
Image Analysis
Sections stained with CD3 and CD79a were entirely scanned at low magnification (40x) with a Coolscope digital microscope (Nikon, Minato, Japan). The obtained images were processed with an image analysis software (ImageJ, National Institutes of Health, USA) to calculate the amount of CD3 and CD79a-positive areas, expressed as percentage of the total area of the nodule in the section that was positively immunolabeled.
The sections with CD79a/Ki-67 double labelling were examined at medium magnification (100x) in order to select the areas of highest proliferative activity. Within these areas, 10 fields at 400x were photographed; 5 photographs each were taken in the CD79a-positive and CD79a-negative areas. In every image, the number of Ki-67 positive and negative nuclei was assessed with a digital cell counter (ImageJ). The Ki-67 index of CD79a-positive and -negative cells was calculated as the mean percentage of Ki-67-positive nuclei in the 5 photographed fields.
PARR
Genomic DNA was extracted from 10 µm sections of FFPE tissues (2-5 for each sample) by QIAamp DNA FFPE Tissue Kit (Qiagen, Hilden, Germany), according to the manufacturer’s instructions. DNA yield and purity were assessed by Nanodrop ND-1000 spectrophotometer (NanoDrop Technologies, Wilmington, DE, USA).
To test genomic DNA integrity and amplificability, a region of 130 bp in the constant region of the IgM gene was amplified according to Burnett et al using the following couple of primers: Sigmf1: 5’-TTCCCC CTCATCACCTGTGA-3’ and Srμ3: 5’-GGTTGTTGATTGCACTGAGG-3’. 5
The clonality of the IgH region was investigated by two different assays. The first was derived from Burnett et al 5 with some modifications: the forward primer CB1 (5’-CAGCCTGAGAGCCGAGGACAC-3’) for the VH region was maintained, while the reverse primer JHrev (5’-CAGACCCAGACACCCTCATT-3’) for the JH region was designed ex novo by Aricò A. (personal data). This new primer was designed by the consensus sequence obtained from the IgH clones of five dogs affected by B-cell lymphoma (caseload reported in Aresu et al). 1 The assay was set up and the condition of amplification were reported below. For each primer, 12.5 pmoles in a final reaction volume of 25 µl were used. The specificity of the assay was tested in positive controls (CLBL1 cell line, diagnosed B-cell lymphoma samples) 21 and negative controls (hyperplastic lymph nodes, T-cell lymphoma samples and OSW cell line). 12 The sensitivity of this new assay was evaluated by an aqueous serial dilution of CLBL-1 cell line DNA from a starting amount of 80 ng/µL; each dilution level was tested in duplicate. The last repeatable result with a sharp single band was obtained with 1.25 ng of DNA in a reaction volume of 25 µL. The second assay used the primers previously published by Valli et al. 26 The expected amplicons were nearly 200 and 180 bp for the first and second assay, respectively.
For the first assay, after an initial denaturation at 98°C for 45 seconds (s), the reaction consisted in 8 cycles of 98°C for 5 s; an annealing step at a decreasing temperature from 65.5°C to 61.5°C for 5 s and 72°C for 5 s. Then 28 cycles of 98°C for 5 s, 60.5°C for 5 s, 72°C for 5 s and a final extension at 72°C for 60 s. For the second assay, the thermal profile was the following: 98°C for 45 s, then 7 cycles of 98°C for 5 s; an annealing step at a temperature varying from 67.5°C to 64.5°C for 5 s; 72°C for 5 s; then 28 cycles of 98°C for 5 s, 64.0°C for 5 s, 72°C for 5 s and a final extension at 72°C for 60 s.
Furthermore, two different assays were used for testing TCRγ clonality. In the first one, the primers published by Valli et al were used and minor modifications were applied to the thermal protocol (a denaturation step at 98°C for 45 s; 7 cycles of denaturation at 98°C, annealing for 5 s at a decreasing temperature from 66°C to 60.5°C, elongation at 72°C for 5 s; 28 cycles of: 98°C for 7 s, 59.5°C for 7 s, 72°C for 7 s; final elongation at 72°C for 60 s. 26 The expected PCR product was nearly 111 bp. In the second assay, the 6 forward (V2-1, V2-2, V3-1, V3-2, V7-1, V7-2) and the 6 reverse (Ja, Jb, Jc, J2-1, J5-1, J6-2) primers published by Keller and Moore (2012) were used in a multiplex PCR. 10 An initial denaturation (98°C, 45 s) was performed, followed by 4 cycles with decreasing temperature in the annealing step (98°C, 5 s; from 63°C to 61.5°C, 5 s; 72°C, 5 s), 28 cycle at: 98°C, 5 s; 61°C, 5 s; 72°C, 5 s, and a final elongation at 72°C for 90 s. Multiple amplicons different in size (from 65 to 170 bp) were expected.
All the PCRs were performed in a final volume of 25 μL, with 80-100 ng genomic DNA; the Taq Phire Hot Start II DNA Polymerase (Thermo Fisher Scientific, Waltham, MA, USA) was used to perform touch down programs in a ProFlex thermal cycler (Applied Biosystem, Foster City, CA, USA).
The samples were subjected to heteroduplex analysis: denaturation at 95°C for 10 minutes into a T-1 Personal Thermal cycler (Biometra, Göttingen, Germany) followed by a slow re-annealing on ice for 1 hour. Each sample was amplified in duplicate together with a negative (water) and a positive (CLBL-1 cells for IgH and OSW cells for TCRγ) control.
Ten μL of each sample were analyzed in a 4% TBE agarose gel (UltraPure Agarose 1000, Invitrogen, LifeTechnologies, Carlsbad, CA, USA) on a Mini L horizontal gel electrophoresis system (Peqlab Biotechnologie GmbH, Erlangen, Germany), at 100 V for 70 minutes. Results were visualized and documented by a Gel Doc XR+ System (Bio-Rad, Hercules, CA, USA).
Polyclonal amplification, consistent with a non-neoplastic process, was identified by the presence of a broad smeared band or a laddering profile in at least one of the assays. A result was considered clonal (most consistent with lymphoma), in the presence of 1-4 sharp gel bands in both assays. Samples were judged pseudoclonal when the bands were not reproducible. 11
Statistical Analysis
Data were analyzed with SPSS software (SPSS, Inc., IBM, Chicago, IL, USA). P values ≤ .05 were considered significant.
When appropriate, data sets were tested for normality by use of the D’Agostino and Pearson omnibus normality test. Values were expressed as mean ± standard deviation in case of normal distribution, or as median with a range in case of nonnormal distribution. Differences in the examined variables according to the final diagnosis were assessed by Fisher’s exact test or Chi-square test (qualitative variables), Student’s t test (quantitative variables, normal distribution) and Mann-Whitney U test (quantitative variables, nonnormal distribution). Evaluated variables included sex, age, body weight, presence of clinical signs, detection of a palpable abdominal mass on physical examination, presence of multiple splenic nodules, presence of a diffuse splenic enlargement, nodule diameter, rupture of the mass, hematologic abnormalities, CD79a-positive areas, CD3-positive areas, and Ki-67 index.
The receiver operating characteristic (ROC) curve analysis was applied to detect the best threshold values of CD3-positive areas, CD79a-positive areas, and Ki-67 index to identify the cases of lymphoma.
The Kaplan-Meier product-limit method was applied to estimate survival after splenectomy and the prognostic relevance of the obtained diagnoses was assessed by means of the log-rank test. Survival time (ST) was defined as the number of days from the date of splenectomy to the last reported date that the patient was seen alive. Dogs dead of lymphoma-related or -unrelated causes were registered as events; dogs were censored if they were alive at the end of the study.
Results
The complete demographic, clinical and histopathologic details of the 35 cases of splenic nodular lymphoid lesions are provided as Supplemental Table 1.
Clinical Information
Thirty-five dogs were included in the study: 18 males (51%; 16 intact and 2 castrated) and 17 females (49%; 9 intact and 8 spayed). The mean age was 9.5 ± 2.8 years (range, 4-17). The most represented breed was Yorkshire terrier (n = 4). Eleven dogs were small (≤10 kg), 15 were medium (11-25 kg), and 9 dogs were large-sized (>25 kg). The mean body weight was 17.8 ± 10.8 kg (range, 3-45). Clinical signs were mentioned in 10 cases (29%) and included dysorexia, weight loss, asthenia, vomiting, and abdominal pain. In 7 of those dogs an abdominal mass was palpated on physical examination. In the remaining 25 cases, the splenic nodule was incidentally detected on abdominal ultrasound (AUS) examination performed for other causes (eg, staging of unrelated tumors, foreign body ingestion, pregnancy determination, enteropathy, cystitis, routine check-up for chronic diseases).
In 11 cases (31%), the spleen showed multiple (2-3) nodules. In 6 of them, only the largest nodule was submitted for histologic examination. In the remaining 5 cases, additional nodules were also examined and diagnosed as LNH or hematomas; however, only the largest nodule was included in the study. In 10 cases (29%), diffuse splenic enlargement was also reported. The mean diameter of the 35 selected nodules was 2.5 ± 1.6 cm (range, 0.6-6 cm). In 2 cases (6%) there was evidence of previous rupture of the capsule with omental adhesion.
In only one case, a mild enlargement of jejunal lymph node was detected ultrasonographically. No other cases of abdominal lymphadenomegaly were observed. In 8 cases, a diffuse hepatopathy of most likely degenerative origin was also reported. Four dogs each had signs of chronic enteropathy and nephropathy. Two had adrenal gland nodules, one dog had a cryptorchid neoplastic testicle. No other suspected neoplastic lesions were identified on AUS examination. In no case was abdominal effusion detected.
Hematological abnormalities were reported in 9 dogs (25.7%), including anemia (HCT <37%; n = 5), neutrophilia (>12,000/µL; n = 5), monocytosis (>1,400/µL; n = 2), and thrombocytosis (>500,000/µL; n = 4).
Diagnosis
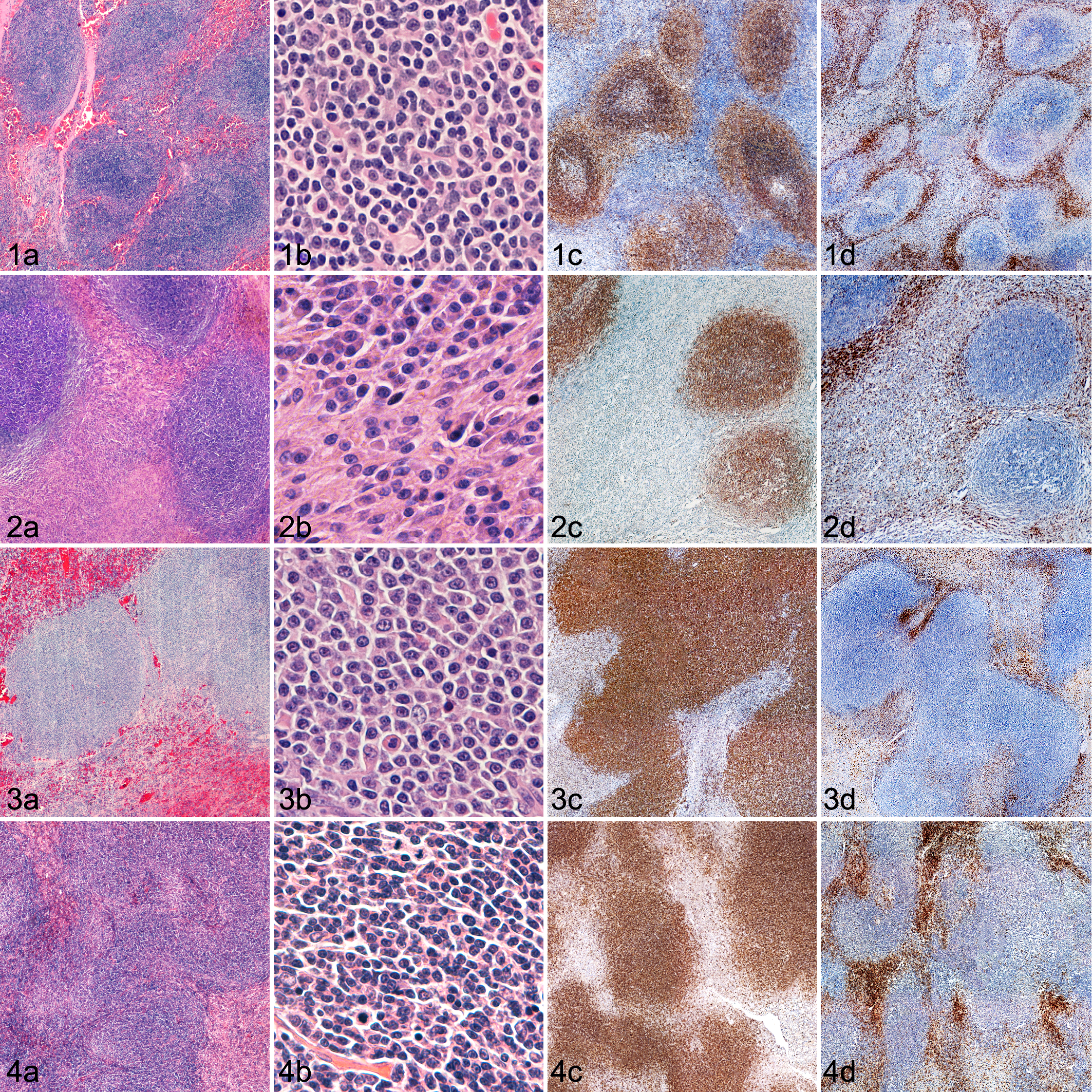
Based on histology and immunophenotyping, 10 nodules (29%) were diagnosed as LNH, 12 (34%) as CNH, 11 (31%) as MZL, and 2 (6%) as MCL (Figs. 1–4).
With PARR analysis, 14 cases (40%) showed a clonal IgH rearrangement: 12 of them (86%) had been histologically diagnosed as nodular lymphoma, whereas 2 had been diagnosed as CNH. The histological reexamination confirmed the presence of both mantle and marginal zone lymphocytes in the two cases previously diagnosed as CNH; however, based on the prevalent cell type, these lesions were reclassified as MCL. One case diagnosed as MZL based on histology and immunophenotyping was polyclonal for IgH gene rearrangement. The subsequent analysis for TCRγ returned a polyclonal result as well.
Based on the previously reported criteria, 15 cases (43%) were ultimately diagnosed as nodular lymphoma (11 MZL and 4 MCL), and 20 (57%) as hyperplastic lesions (10 LNH and 10 CNH).
According to the grading system proposed by Spangler and Kass, 19 nodules (54%) would have been classified as grade I and 16 (46%) as grade II, with grade I including all the LNH cases and 9 MZLs and grade II including all the CNH, all MCLs and 2 MZLs.
Statistical Analysis
Overall, the mean percentage of CD79a-positive areas was 28.2% ± 12.7%, whereas the mean percentage of CD3-positive areas was 14.0% ± 7.2%. The percentage of CD79a-positive cells was significantly higher in the cases ultimately classified as nodular lymphoma (mean ± SD, 36.3 ± 10.6%) compared with hyperplasia (mean, 22.1 ± 10.7%; P < .001; Fig. 5). No significant difference was observed between MZL and MCL or between LNH and CNH. The percentage CD3-positive areas was not associated with the final diagnosis.
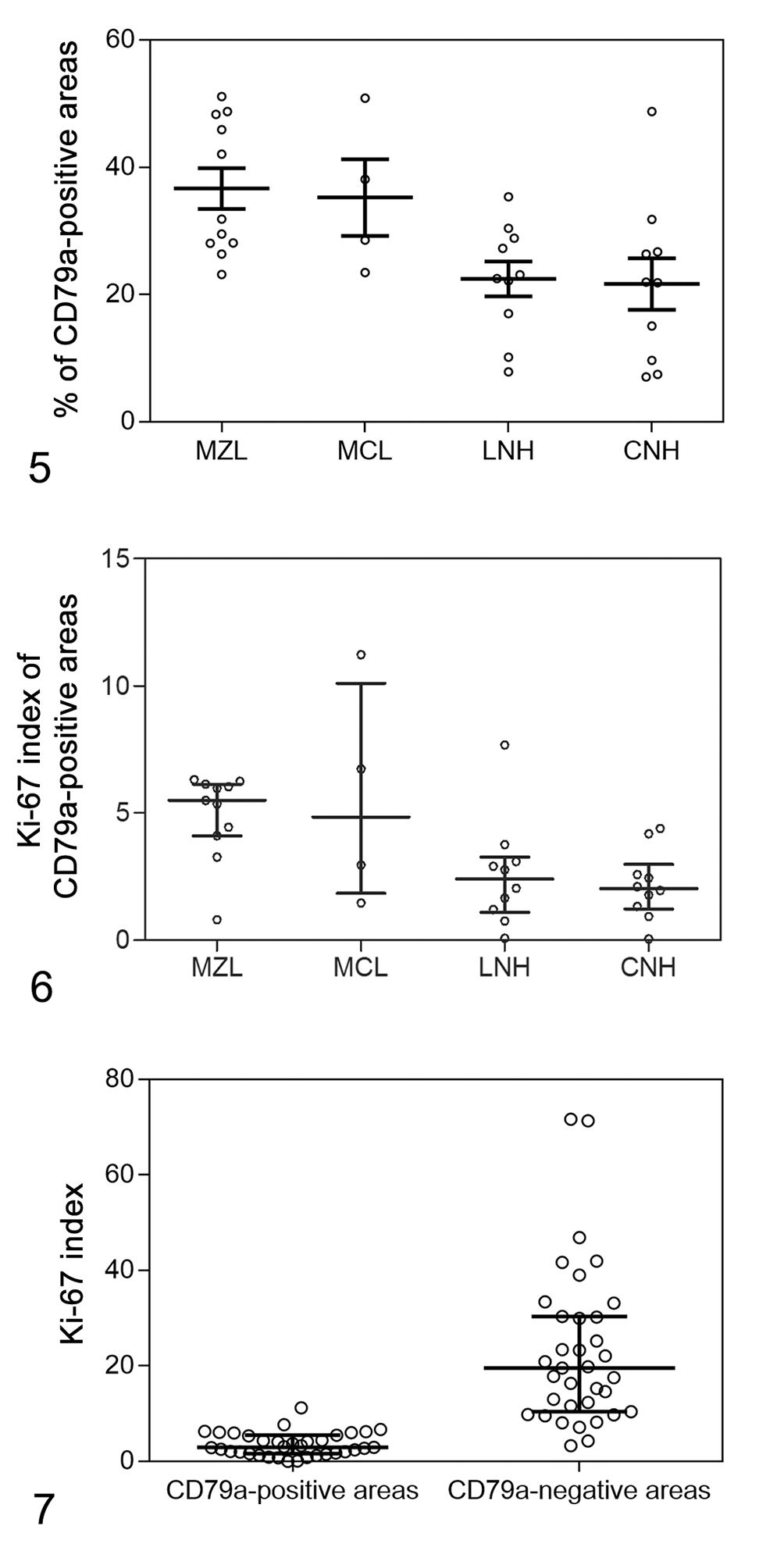
The median Ki-67 index of CD79a-positive areas was 3.0% (IQR, 1.7-5.5%). Ki-67 index was significantly higher in the cases ultimately classified as nodular lymphoma (median, 5.5%; IQR, 3.3-6.2%) compared with hyperplasia (median, 2.1%; IQR, 1.2-3.0%; P = .001; Fig. 6). No significant difference was observed between MZL and MCL or between LNH and CNH. The median Ki-67 index of CD79a-negative areas (19.6%; IQR, 10.4-30.4%) was significantly higher than observed in the CD79a-positive areas (P < .001). The Ki-67 index was not associated with the final diagnosis (P = .129; Figs. 7, 8).
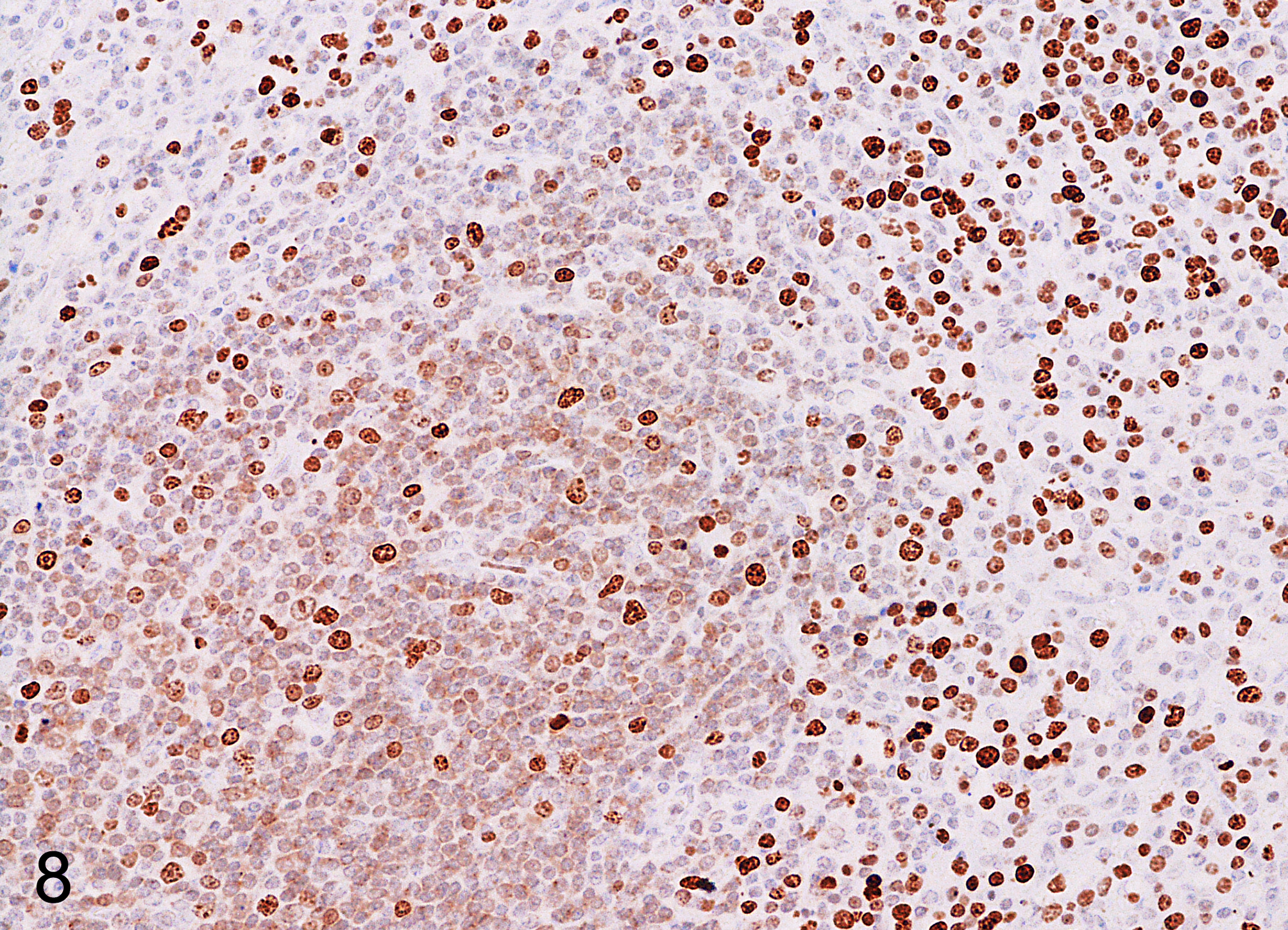
Complex nodular hyperplasia, spleen, dog. CD79a/Ki-67 double immunolabeling. The proliferative activity of the follicular area (CD79a-positive) is lower compared with the outer area (CD79a-negative). IHC for CD79a and Ki-67.
The ROC curve analysis identified the following threshold values as most indicative of nodular lymphoma: CD79a-positive areas > 28% (sensitivity, 75%; specificity, 80%; area under curve, 0.8; 95% CI, 0.7-1.0; P = .001); Ki-67 index > 3% (sensitivity, 87%; specificity, 75%; area under curve, 0.8; 95% CI, 0.7-1.0; P = .001).
Other variables significantly associated with a diagnosis of nodular lymphoma were the presence of clinical signs (P = .008) and a larger nodule diameter (median, 3.4 cm vs 1.8 cm; P = .002; Table 1). No significant difference in the considered clinicopathological variables was observed between LNH and CNH.
Distribution of Clinical and Pathological Variables According to Diagnosis in 35 Cases of Canine Splenic Nodular Lymphoid Lesions.
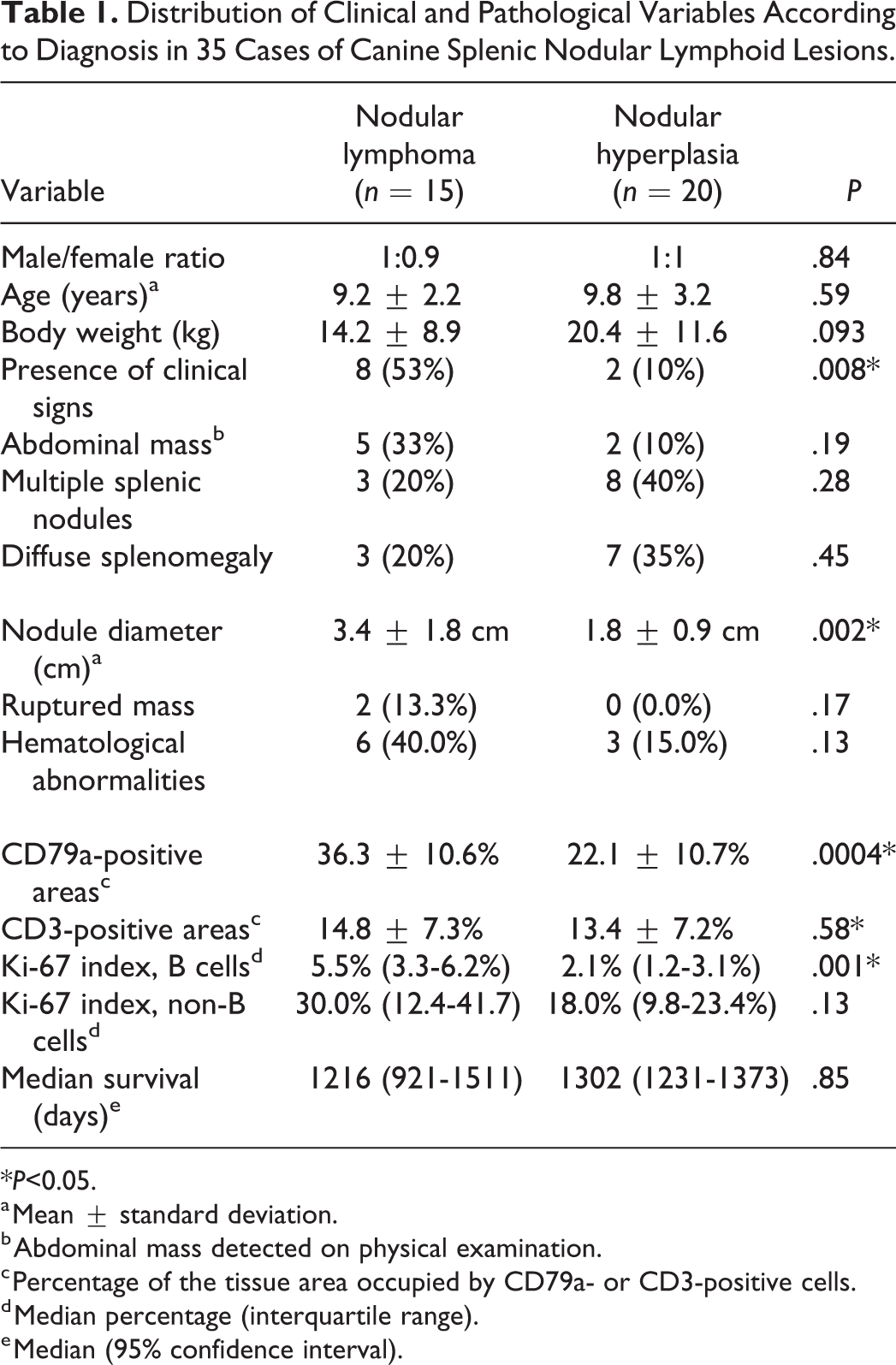
*P<0.05.
a Mean ± standard deviation.
b Abdominal mass detected on physical examination.
c Percentage of the tissue area occupied by CD79a- or CD3-positive cells.
d Median percentage (interquartile range).
e Median (95% confidence interval).
Survival Analysis
Seventeen dogs (49%) died for unrelated causes after a median of 1087 days from splenectomy (IQR, 633-1292 days). Causes of death included bacterial infections, chronic renal failure, cardiac failure, gastric dilation and volvulus, mammary tumors, prostatic tumor, chronic enteropathy, hyperadrenocorticism and hypoaldosteronism. The remaining 18 dogs were still alive at data analysis closure, with a median follow-up time of 870 days (IQR, 569-1225). Overall median survival time was 1282 days, with no significant outcome difference between nodular lymphoma (1216 days; 95% CI, 921-1511) and hyperplasia (1302 days; 95% CI, 1231-1373; P = .849; Table 1; Fig. 9).
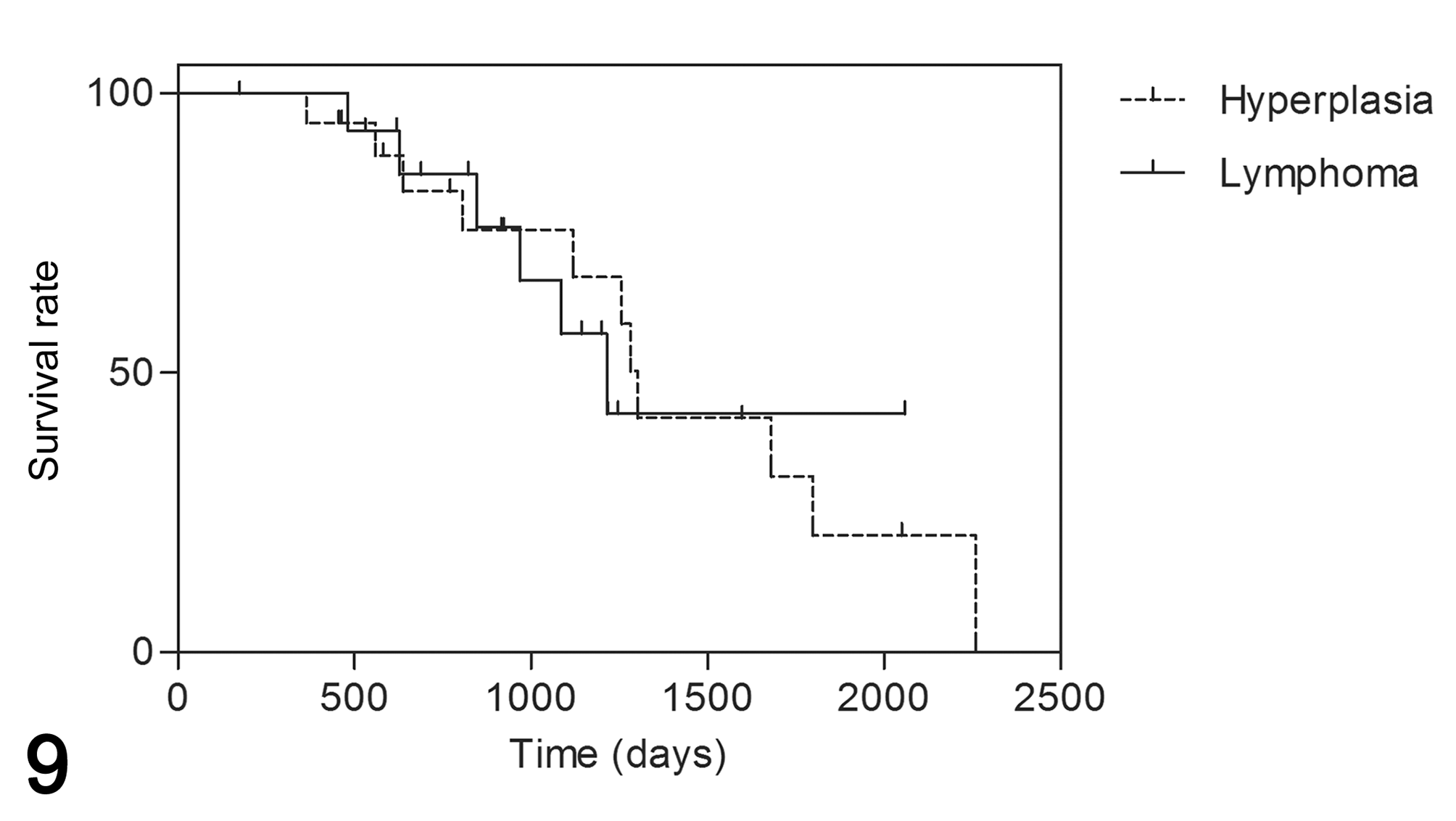
Survival curves of 35 dogs with splenic nodular lymphoid lesions. Overall median survival time was 3.5 years, with no significant outcome difference between nodular lymphoma (1216 days; 95% CI, 921-1511) and hyperplasia (1302 days; 95% CI, 1231-1373; P = .849). All deaths were recorded as events.
Discussion
This study describes the clinical and pathological findings in a group of dogs with splenic nodular lymphoid lesions treated with splenectomy alone. Approximately 40% of the cases were diagnosed as indolent lymphoma, while the remaining were referable to nodular hyperplasia, either purely lymphoid or complex type. Notably, none of the dogs with nodular lymphoma died due to their cancer during a median follow-up period of more than 3 years and there was no difference between the clinical course of the dogs with neoplastic disease and those with hyperplasia.
Human patients with splenic MZL also appear to do well with splenectomy alone and response to chemotherapy is rather disappointing. Overall, prognosis in humans is better for splenic MZL than for nodal MZL, with a 5-year survival rate of 81-95%. 15,19
In dogs, there is paucity of information on the long-term clinical course of indolent lymphoma. Purely splenic forms seem to have a better prognosis than nodal forms, 7,18,27 and splenectomy is currently considered the standard of care. 7,29 Nevertheless, evolution to diffuse lymphoma and spread to the liver or other lymphoid organs is reported, 26 and a few studies have hypothesized a benefit of adjuvant chemotherapy. 18,25
In the present study, the spleen was the only organ involved on abdominal ultrasound, and no dog showed splenic hilar or peripheral lymphadenomegaly. In addition, in no case did blood tests detect lymphocytosis, consistent with a leukemic phase, which had been previously reported in splenic MZL. 7,18 This could explain the exceptionally good clinical course of all the dogs in this study.
Overall, the survival data in the present study are very similar to those of the original paper by Spangler and Kass. In that study, a large series of splenic proliferative nodular lesions was related to outcome and none of 46 dogs with grade I or II lesions (ie, those with less than 60% of fibrohistiocytic cells) died spontaneously in the 12-month interval following splenectomy. 24
In a recent report on canine splenic lymphoma, poor prognostic indicators included hemoabdomen, abdominal distention, lethargy, and anorexia. 29 In the present study, clinical signs and large tumor size were significantly associated with a diagnosis of lymphoma, but did not affect survival time. Nevertheless, the number of cases reported here are too small for drawing definitive conclusions regarding outcome.
The histologic distinction between lymphoid hyperplasia and nodular lymphoma is considered challenging, due to the presence of large areas of morphological and architectural overlaps, which appear to support the hypothesis of a pathological continuum between these disorders. The confirmation of cell monomorphism and phenotype determination by immunohistochemistry (IHC) is considered essential in the diagnosis of diffuse lymphoma, 27 but might appear of limited utility in the case of splenic nodular lymphoma since monomorphism is lacking in early lesions and the follicular pattern suggests a B immunophenotype. Nevertheless, IHC can be useful in highlighting the limit between one follicle and another, thus allowing a more accurate evaluation of size, shape and confluence of follicles. Also in the study of Moore et al, IHC was essential to reclassify 32 splenic nodules previously diagnosed as fibrohistiocytic. 17 Therefore, a two-step approach including both histology and immunohistochemistry may be indicated in cases of canine splenic nodular lymphoid lesion. The consistency of this diagnostic approach was confirmed in the present study by the good degree of correlation with PARR, and with more objective parameters such as the quantification of B-cell areas and the assessment of proliferative activity by image analysis.
Flood-Knapik et al did not find any prognostic utility of Ki-67 index in a large case series of indolent lymphoma. 7 However, that study only included 6 splenic lymphomas. In addition, the diagnostic utility of Ki-67 index in differentiating canine splenic indolent lymphoma from hyperplasia has never been investigated. In this study, we had both goals in mind; however, as there was no relationship between these diagnoses and the clinical course, it was not possible to validate the utility of Ki-67 as a prognostic marker. Instead, a potential diagnostic utility was detected, by demonstrating a significantly higher proliferative activity of B-lymphocytes in MZL and MCL when compared to hyperplastic nodules. The addition of CD79a immunohistochemistry allowed the differentiation of proliferating B cells (positive cytoplasm and nuclei) from other proliferating cells (positive nuclei only). Surprisingly, there was a greater proliferative activity in the non-B areas, although not primarily involved in the hyperplastic/neoplastic process. From a practical point of view, these data suggest that simply evaluating the Ki-67 index in randomized fields or in the areas of highest proliferative activity (without double-labelling immunohistochemistry for identification of cell type) would likely lead to an overestimation of neoplastic proliferation and may erroneously orient toward a diagnosis of nodular lymphoma.
The detection of clonality in lymphoid proliferations is considered a useful adjunct to histologic examination. 6,13,23 However, according to the recently proposed guidelines, molecular clonality assays are not to be regarded as stand-alone tests, but must follow clinical, morphologic, and immunophenotypic assessment. In addition, lineage assignment based on clonality results is not recommended and is more accurately done by immunophenotyping, due to the possibility of cross-lineage rearrangements. 11 Finally, clonality testing is considered unnecessary in histologically obvious lymphoid neoplasms. 11
In the present paper, the clonality of the IgH region was investigated by two different previously published assays, the first according to Valli et al and the second according to Burnett et al. 5,26 Nevertheless, the latter was carried out with some modifications that in our laboratory conditions provided better results in terms of sensitivity/specificity. The overall concordance between PARR and the first histological diagnosis was good, with more than 90% of matching diagnoses. Of the cases histologically diagnosed as nodular lymphoma, only 1 had a negative test for clonality for IgH. In this case, cross-lineage rearrangement was also excluded with PCR for TCRγ. However, in view of convincing histologic findings, the case was still classified as lymphoma. This is consistent with the sensitivity of PARR, which may yield false-negative results in up to 30% of cases. False negatives can be attributed to multiple causes, including gene rearrangements not recognized by primers, partial rearrangements of IgH, chromosomal defects, or presence of a large polyclonal background. 26 Excessive DNA fragmentation due to formalin fixation could be another possible cause; however, in this study, the presence of amplifiable DNA was confirmed within each sample before clonality testing.
The initial histologic diagnosis of hyperplasia was altered on the basis of clonality results in 2 cases. These were considered possible debutant forms of nodular lymphoma not yet recognizable on a histologic basis, and therefore they were reclassified as neoplastic based on the finding of clonality. However, the possibility should also be considered of false positive results due to clonal expansion secondary to antigenic stimulation.
The present study does not provide novel diagnostic criteria to differentiate between lymphoid and complex nodular hyperplasia; this nomenclature has only been recently proposed, and the precise ratio of lymphoid and stromal proportions which should lead to each diagnosis has not been explicitly determined. 17 As a result, many pathologists may still feel more comfortable with the old terminology and classification. 24 In order to promote continuity and reproducibility, we adopted the new classification by applying the cut-off values proposed by the old one and we made LNH coincide with grade I SFHN and CNH with grade II SFHN. The choice to include CNH in the study derives from the consideration that both LNH and CNH should be included in the differential diagnosis of canine nodular lymphoma, especially of MCL, which may be associated with a prominent stromal component. Nevertheless, the distinction between splenic nodular lesions containing more or less than 70% of lymphoid elements appeared rather arbitrary in this study, since it was not supported by any difference in clinical outcome, PARR results or CD79a/Ki-67-double labelling.
In summary, this study provides encouraging data on the prognosis of dogs with splenic nodular lymphoid lesions, and proposes new elements for a more accurate differentiation of splenic nodular lymphoma and hyperplastic lesions. For a correct diagnosis, the morphological and architectural evaluation of HE-stained sections at medium-low magnification should still be considered the most valuable option, but immunophenotyping and PARR can support the diagnosis of early lesions. The assessment of proliferative activity with Ki-67 immunohistochemistry can also assist the differentiation between hyperplastic and neoplastic forms, if specifically evaluated within the B cell compartment. In particular, lesions with more than 28% of B lymphocytes with a growth fraction above 3% are more likely to be neoplastic.
Supplemental Material
Supplemental Material, DS1_VET_10.1177_0300985818777035 - Canine Splenic Nodular Lymphoid Lesions: Immunophenotyping, Proliferative Activity, and Clonality Assessment
Supplemental Material, DS1_VET_10.1177_0300985818777035 for Canine Splenic Nodular Lymphoid Lesions: Immunophenotyping, Proliferative Activity, and Clonality Assessment by Silvia Sabattini, Rosa Maria Lopparelli, Antonella Rigillo, Mery Giantin, Andrea Renzi, Chiara Matteo, Ombretta Capitani, Mauro Dacasto, Marisa Mengoli, and Giuliano Bettini in Veterinary Pathology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.