
Abstract
A striking form of lymphocytic mural folliculitis is described in 6 tigers (Panthera tigris). Clinically, all tigers exhibited regionally extensive chronic, variably waxing and waning alopecia with minimal scaling and crusting most pronounced over the head, neck, and shoulders. More severely affected tigers exhibited marked hyperpigmentation and lichenification. Pruritus was not a feature. Tigers generally lacked signs of systemic illness and clinical pathology findings were unremarkable. Histologic examination of skin biopsies revealed infiltrative lymphocytic mural folliculitis extending the length of the hair follicle. Mild epidermal lymphocytic infiltrates were frequent. The surrounding dermis was histologically unremarkable in 4 of 6 tigers or associated with mild perifollicular and periadnexal mixed inflammation in 2 of 6 tigers. The cause of the mural folliculitis was not identified, and tigers responded poorly to immunomodulatory therapy. Lymphocytic mural folliculitis might be a nonspecific hypersensitivity reaction pattern in tigers, and care should be taken to differentiate this reaction pattern from epitheliotropic T-cell lymphoma.
Lymphocytic mural folliculitis is characterized by lymphocyte-predominant inflammation directed toward the follicular epithelium. This histological pattern is recognized in domestic cats associated with infectious dermatoses (dermatophytosis, demodicosis). 7 It is also a minor, usually focal, reaction pattern occurring in 70% of dermatoses, with a significantly higher prevalence in allergic conditions. 15 However, diffuse infiltrative lymphocytic mural folliculitis is a rare reaction pattern in domestic cats, associated with a wide spectrum of dermatoses including pseudopalade-like syndrome, sebaceous adenitis, exfoliative dermatitis, mucinotic mural folliculitis, adverse food and drug reactions, alopecia areata, and as an idiopathic condition. 2,5,7,8,13 Infiltrative lymphocytic mural folliculitis has also been described as a feature of paraneoplastic skin conditions concomitant with pancreatic carcinoma 9 and in conjunction with an epidermal interface pattern in cats with thymoma-associated exfoliative dermatitis. 16 In addition, infiltrative lymphocytic mural folliculitis, often paired with infiltration of apocrine glands, is the hallmark feature of epitheliotropic T-cell lymphoma. 3,6 We describe a series of 6 tigers (Panthera tigris) with a major histologic pattern of infiltrative lymphocytic mural folliculitis redolent of epitheliotropic T-cell lymphoma, but with a protracted nonprogressive clinical course.
From 2008 to 2017, 6 adult tigers showed patchy alopecia over the trunk, neck, and head (Table 1). Five tigers lived at a large cat sanctuary in rural east Tennessee and 1 tiger (case 6) lived at an east Tennessee zoo. Tigers were not genetically related and none had spent time together prior to their arrival at the large cat sanctuary. All tigers had year-round access to outdoor pens with turf substrate. Alopecia initially occurred during the summer in 3 tigers (cases 1–3), and progressed to year-round signs in cases 1 and 2. Early lesions were discrete, 1–2 cm diameter patchy areas of alopecia progressing to coalescing areas preferentially around the head, neck, and ventral trunk (Fig. 1) and less commonly extending along the ventrum and distal limbs. Pruritus was uncommon, presenting only in case 5, which exhibited extensive barbering along the trunk, ventrum and inguinal areas. The pruritus, however, was not directed at the alopecic areas. Lichenification was common in long standing cases, typically accompanied by variable hyperpigmentation and rarely depigmentation. Differential diagnoses included demodicosis, dermatophytosis, sebaceous adenitis, pseudopelade, mucinotic mural folliculitis, alopecia areata, and epitheliotropic T-cell lymphoma.
Clinical Data for Tigers With Lymphocytic Mural Folliculitis.
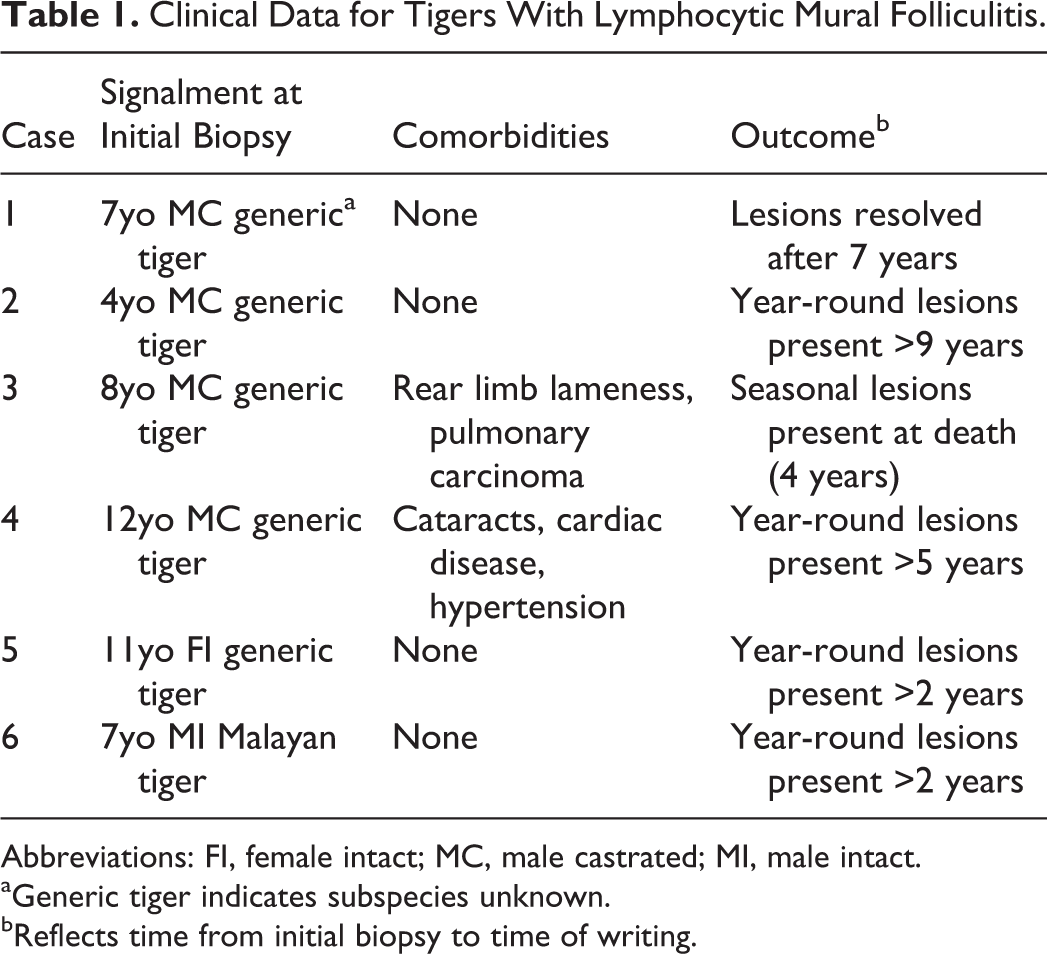
Abbreviations: FI, female intact; MC, male castrated; MI, male intact.
aGeneric tiger indicates subspecies unknown.
bReflects time from initial biopsy to time of writing.

Infiltrating lymphocytic mural folliculitis, tiger, case 3. Regionally extensive, characteristically punctate circular (arrowheads) to coalescing areas of alopecia, lichenification, and hyperpigmentation are most severe around the head, neck, and forelimbs.
One to 3 general health screenings, including physical examination, complete blood cell counts, and plasma biochemistry panels were performed on cases 1–4 while they exhibited alopecia, and no clinically important abnormalities were found. Ancillary diagnostic tests performed included urinalysis (cases 2–4), feline leukemia virus and feline immunodeficiency virus screening (cases 2–4), and total thyroxine analysis (case 5). All were negative or within reference intervals for domestic cats. Fungal cultures of the skin were performed on cases 1, 2, 4, and 5 and were negative. In addition, PCR for dermatophyte and Demodex sp. 4 was performed on cases 1, 2, and 4, and were negative. Skin scrapings were performed on cases 1–3 and were negative. Aerobic skin cultures were performed on cases 1, 2, and 4 and identified predominantly Staphylococcus spp.
A variety of treatments were attempted on 5 tigers including several months of prednisolone alone or in combination with the antihistamine chlorpheniramine, amoxicillin-clavulanic acid, itraconazole, and/or lomustine; no therapeutic regime had an appreciable effect. A novel diet of rabbit meat in a single animal resulted in no clinical improvement after 7 months. Signs have persisted until the time of writing (duration 2–9 years) in 4 of 5 surviving tigers and resolved in 1 animal (case 1) 7 years after onset. Since their initial diagnosis, 1 tiger (case 3) showed rear limb lameness and later died due to aspiration pneumonia. Another tiger (case 4) had cataracts, ventricular flutter, and presumptive hypertension, prior to developing alopecia, and had been treated with oral sotalol. No tigers died or had significant clinical deterioration associated with their skin disease.
Skin biopsies from all 6 tigers were formalin-fixed, paraffin-embedded, and routinely processed for light microscopy. Lesional skin from all tigers had similar microscopic features. All exhibited moderate acanthosis of the overlying epidermis with mild orthokeratotic hyperkeratosis. The epidermis had diffuse, often marked hyperpigmentation which extended into the follicular infundibula. Frequently, hair follicles and adnexal structures were atrophied. In all sections, hair follicles and fewer apocrine glands were infiltrated with small lymphocytes (Fig. 2), which affected the length of the follicle. Inflammatory infiltrates were most intense within the isthmus and infundibular regions (Fig. 3), with relative sparing of the deeper hair follicle and hair bulb (Fig. 4). In the most severe cases, infiltrates obliterated these structures which were then surrounded by small amounts of edema, early fibroplasia and mixed lymphocytes, macrophages, and few neutrophils (Fig. 5). In less severely affected animals, lymphocytic infiltrates were limited to hair follicles, and occasionally infiltrated only a few follicles in any given section. Small infiltrates of lymphocytes were within the overlying epidermis in all sections. Sebaceous glands were spared in all cases. Immunohistochemistry for CD3, CD20 or CD79 (Dako) and CD18 (laboratory of PF Moore, Davis, CA) were completed on cases 1–4. Infiltrating lymphocytes were immunoreactive to CD3 (Fig. 6) and rarely CD18 consistent with a T-cell phenotype. Infiltrating cells were not immunoreactive for CD20 or CD79.
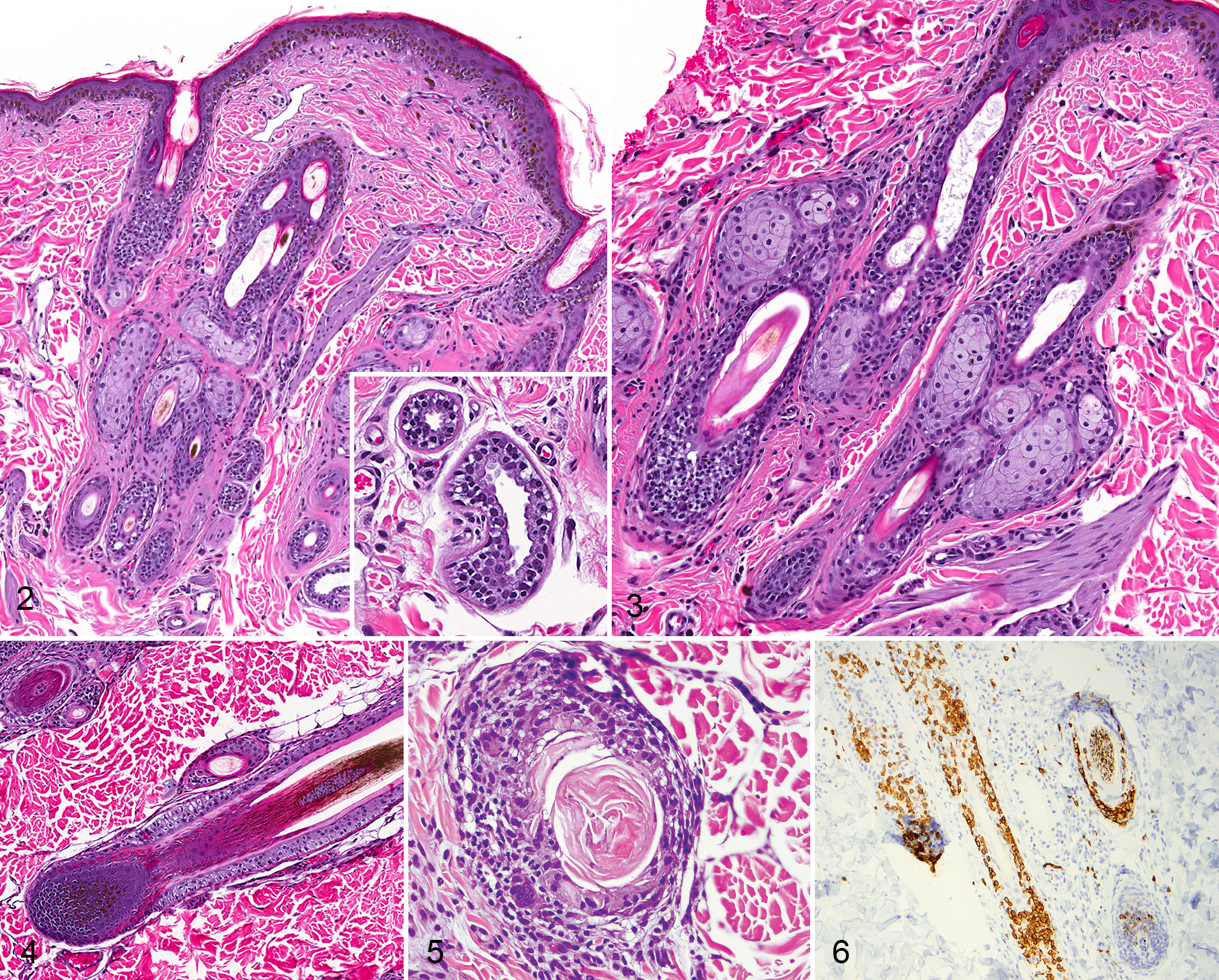
Dermal changes were mild and in all samples were composed of low to occasionally moderate numbers of perivascular to periadnexal mast cells. Mixed periadnexal mononuclear dermal infiltrates composed of lymphocytes, rare plasma cells, and few macrophages, were minimal. Moderate numbers of superficial dermal melanomacrophages (pigmentary incontinence) were present in most severely affected sections. Dermal edema was minimal and limited to areas of most severe folliculitis. In a few tigers, there was mild superficial to middermal fibrosis. Infectious organisms were not identified with the use of Gomori’s methenamine silver (cases 1–3) and periodic acid-Schiff (case 1) stains.
The finding of infiltrative lymphocytic mural folliculitis as a primary histologic finding in a number of tigers sharply contrasts with domestic cats, where lymphocytic mural folliculitis is typically focal, present in association with other dermal inflammatory changes, and frequently a minor reaction pattern. 15 Save for the fairly consistent, mild dermal infiltrates of mast cells, the nearly complete lack of accompanying dermal changes in 4 of 6 animals appears unique to this reaction pattern in tigers, and may erroneously lead to an initial diagnosis of epitheliotropic T-cell lymphoma. Indeed, epitheliotropic T-cell lymphoma was the initial concern of each pathologist reading these biopsies.
The clinical presentation of epitheliotropic T-cell lymphoma can be quite pleomorphic in domestic cats, with 4 primary clinical presentations: exfoliative erythroderma, mucocutaneous localization, solitary or multiple plaques or nodules, and oral mucosal ulceration 6 (the latter is rare in cats). 3 Clinically, the patchy alopecia with mild scaling and crusting often starting around the head, as seen in these tigers, may have initially appeared similar to an exfoliative erythroderma. As it was critical to differentiate epitheliotropic T-cell lymphoma from inflammatory lymphocytic folliculitis, immunohistochemistry was employed to further characterize the lymphocyte population. Infiltrating lymphocytes were strongly immunoreactive to CD3, consistent with a T-cell phenotype. Inflammatory lymphocytes in dogs, 11,12 cats, 14 and horses 18 are also predominantly T cells, which are important in the cutaneous immune response to a variety of microbial, chemical, and auto antigens. Thus, in cases where the inflammatory lymphocytes are entirely of T cell origin, as in these tigers, immunohistochemistry alone is unlikely to be diagnostically discriminatory. The lack of clinical progression over multiple years remains the strongest argument against epitheliotropic T-cell lymphoma; however, PCR-based immunoglobulin and T-cell receptor clonality testing, which has not been established in tigers, would help more definitively rule out slowly progressive epitheliotropic T-cell lymphoma.
The cause of the lymphocytic mural folliculitis in this series of tigers has not been established. Infectious causes such as pyoderma, demodicosis, or dermatophytosis were eliminated based on negative skin scraping, cytology, dermatophyte cultures and PCR. Sebaceous glands were unaffected, ruling out sebaceous adenitis. Alopecia areata was given consideration due to the characteristically well-demarcated lesions of alopecia initially oriented to the head and neck; however, a predominance of infiltrates within the mid to superficial portions of the hair follicles, involvement of the overlying epidermis, and lack of significant hair bulb involvement in multiple cases make this unlikely. In 13 cases of naturally occurring alopecia areata in dogs, hair bulb involvement, almost exclusively of anagen hair follicles, was the hallmark feature and present in 100% of cases, while involvement of the isthmus occurred in only 54% of cases. 18 In these tigers, few lymphocytes were present within hair bulbs in only 3 of 6 cases while superficial portions including the isthmus, infundibular and nonfollicular epidermis were involved in all 6 cases. In cases where hair bulbs were affected, infiltrates were mild and not associated with typical degenerative changes in matrical cells, melanosome clumping, depigmentation, or dysplastic follicular changes. In addition, involvement of the apocrine glands in the majority of these cases would be unusual for alopecia areata where the autoantibody is against hair follicle antigens including those composing the trichohyalin granules as well as other inner root sheath proteins. 17,18 Pseudopelade is a possible differential diagnosis, but the seasonality in some tigers with lack of permanent scarring make this unlikely. A paraneoplastic condition also seems unlikely based on the seasonality of the alopecia in some tigers and the longevity of affected tigers. While case 3 died of pneumonia, the alopecia in this case had been seasonal and relatively stable for 3 years after initial diagnosis. In addition, in most cases of thymoma-associated and non-thymoma-associated exfoliative dermatitis and folliculitis, loss of sebaceous glands is a frequent feature, 8,16 which was absent in all of these tigers. Hypersensitivity remains a possible underlying cause, despite 3 tigers failing to respond to anti-inflammatory doses of prednisolone. One report identifies lymphocytic mural folliculitis in a high percentage of allergic dermatoses of domestic cats, with 85% of food-allergic domestic cats having infiltrative lymphocytic mural folliculitis. 15 Rare, probable diet-related, lymphocytic mural folliculitis has also been described in 2 domestic cats. 1,2 Food allergy in domestic cats is not always steroid-responsive, 10 and thus a hypersensitivity reaction cannot be ruled out. Only 1 tiger (case 4) completed a restricted diet trial and this was without benefit. Immunosuppressive doses of corticosteroids were not attempted in these tigers; thus, we cannot rule out an immune-mediated condition in these animals.
Between 2005 and 2017, the University of Tennessee pathobiology archives include 30 biopsies of nonneoplastic skin disease in tigers. Nineteen of the biopsies (63%) reflected inflammatory dermatoses; of these 18 (95%) presented for clinical alopecia, and 1 for a mass. Although the logistical challenges of anesthetizing large nondomestic felids may result in an overrepresentation of dermatoses presenting clinically with chronic alopecia, it is striking that 32% of biopsied inflammatory conditions were primarily or solely manifested as infiltrative lymphocytic mural folliculitis, suggesting that this is an important and relatively common inflammatory cutaneous reaction pattern in tigers. Perhaps, even more striking, this uniquely patchy, punctate, and circular alopecia (Fig. 1) was found only in tigers with this lymphocytic mural folliculitis pattern.
In conclusion, infiltrative lymphocytic mural folliculitis, frequently without significant accompanying dermal changes, may be a unique, possibly hypersensitivity or immune-mediated reaction pattern in tigers. It is essential that the pathologist is aware of this reaction pattern in tigers and, when paired with an appropriate history of chronic, nonprogressive alopecia avoids the mistaken diagnosis of epitheliotropic T-cell lymphoma. Further work is needed to determine the cause or causes of this unique clinical and histological presentation.
Footnotes
Acknowledgements
We would like to thank Dr Stephen Kania and the University of Tennessee College of Veterinary Medicine Immunology laboratory for running the dermatophyte and demodex PCR, Ms Michelle Story for technical assistance with the immunohistochemistry, and Dr Gregory Campbell for consultation on one of these cases.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.