
Abstract
Severe equine asthma, formerly recurrent airway obstruction (RAO), is the horse counterpart of human asthma, affecting horses maintained indoors in continental climates. Equine pasture asthma, formerly summer pasture RAO, is clinically similar but affects grazing horses during hot, humid conditions in the southeastern United States and United Kingdom. To advance translational relevance of equine pasture asthma to human asthma, histologic features of airway remodeling in human asthma were scored in lung lobes from 15 pasture asthma-affected and 9 control horses of mixed breeds. All noncartilaginous airways were scored using a standardized grading rubric (0–3) in hematoxylin and eosin (HE) and Movat’s pentachrome-stained sections; 15 airways were chosen randomly from each lobe for analysis. Logistic regression identified disease, age, and lobe effects on probability of histologic outcomes. Airway smooth muscle (odds ratio [OR] = 2.5, P < .001), goblet cell hyperplasia/metaplasia (OR = 37.6, P < .0001), peribronchiolar elastic system fibers (OR = 4.2, P < .001), peribronchiolar fibrosis (OR = 3.8, P = .01), airway occlusion by mucus/inflammation (OR = 4.2, P = .04), and airway adventitial inflammation (OR = 3.0, P = .01) were significantly greater in diseased airways. A novel complex tissue disorganization, designated terminal bronchiolar remodeling, was overrepresented in diseased airways (OR = 3.7, P < .0001). Distribution of terminal bronchiolar remodeling corresponded to putative sites of air trapping in human asthma, at secondary pulmonary lobules. Age (>15 years) was an independent risk factor for increased peribronchiolar fibrosis, elastic system fibers, and terminal bronchiolar remodeling. Remodeling differed significantly between lung lobes, congruent with nonhomogeneous remodeling in human asthma. Equine pasture asthma recapitulates airway remodeling in human asthma in a manner not achieved in induced animal asthma models, endorsing its translational relevance for human asthma investigation.
Keywords
Rodent models have provided important insights for human disease research, yet the majority of discoveries made in rodent models fail to translate to effective therapies for their human disease counterparts. 60,73,97,107 Asthma is no exception. Rodents do not naturally develop asthma, and rodent models fail to reproduce critical facets of human asthma, including airway hyperresponsiveness that persists without chronic antigen challenge, and spontaneous bronchoconstriction. 78,79,137 Rodents also fail to develop comprehensive histopathologic changes of asthma that are collectively termed airway remodeling. 97,118,137 Only cats and horses spontaneously develop asthma-like disease. 76,130,146
Heaves, or recurrent airway obstruction (RAO), is an asthma-like disease that manifests in horses housed indoors in continental climates and is reliably elicited by exposure to molds that grow in damp hay. 14,83,114 Based upon evidence of shared pathobiology between RAO and human asthma, the name “equine asthma” has been adopted. 109 A second asthma-like disease, formerly termed summer pasture-associated recurrent airway obstruction (SPARAO) or “pasture heaves,” manifests in adult horses housed on grass pastures in the southeastern United States during conditions of high heat and humidity. 26,119,121 Disease remission occurs during cool seasons. This condition has also been described in the United Kingdom. 29,87 For clarity herein, RAO is referred to as barn dust asthma, and SPARAO is referred to as equine pasture asthma.
Several lines of evidence support the relevance of equine pasture asthma as a translational asthma model. Exacerbations of equine pasture asthma are characterized by spontaneous bronchoconstriction and are temporally associated with increased grass pollen and fungal spores, including basidiospores, Botrytis spp., and Helminthosporium spp. that elicit asthma exacerbation in mold-sensitive human asthmatics. 7,26,59,64 Seasonally induced disease also persists for life in horses with pasture asthma, worsening in successive summers if affected individuals continue to reside in the offending environment. 26,27,121 As with human asthma, episodic airway obstruction in equine pasture asthma is reversible with appropriate treatment, including parasympatholytic and sympathomimetic bronchodilatory therapy, corticosteroids, and segregation from the offending pasture particulates. 129 In horses with severe pasture asthma, extreme sensitivity to pasture particulates may necessitate a climate-controlled environment to effectively limit pasture-associated particulates. 129 Diseased horses demonstrate airway inflammation that is predominantly neutrophilic and airway hyperresponsiveness to methacholine (≤1 mg/ml), findings that correlate to severe and treatment-refractory human asthma. 28,52,58,71,129 Early investigations of equine pasture asthma identified mixed cytokine responses, including increases in interleukin (IL)–4, IL-13, and interferon-γ (IFNγ), as well as absence of IgE in bronchoalveolar lavage fluid (BALF). 6,65,106 Collectively, these phenotypic characteristics align to late-onset and nonallergic subtypes of severe human asthma.
Human asthma is now viewed as a collection of asthma conditions with molecular mechanisms (endotypes) and clinical characteristics (phenotypes) that vary widely, are not necessarily static, may overlap, and are modified by treatment. 4 This challenges human asthma investigation because, despite exhaustive selection for overt asthma attributes, asthma cohorts are likely to be composed of individuals that differ in their underlying pathophysiologic mechanisms and genetic, environmental, and treatment factors. Naturally occurring asthma models, such as equine pasture asthma, can control for these factors while recapitulating complexities of human asthma that are not adequately induced in other animal asthma models, providing a strong rationale for investigations of equine pasture asthma to inform targeted investigations of human asthma. To this end, human studies have identified a need to investigate the role of environmental factors in regional severe asthma disparities in the southeastern United States, where equine pasture asthma is also concentrated. 1,27,47,116
Because pathobiologic events responsible for disease are reflected in tissue, the degree to which lesions in an animal model mirror those of its human disease counterpart is foundational to the model’s biologic relevance. Knowledge of human asthma pathobiology has been primarily derived from small endobronchial biopsies of central cartilaginous bronchi, where structural changes, collectively termed airway remodeling, correlate to disease progression and a nonreversible component of airflow obstruction. 5,19,104,105,133 Airway remodeling includes increased airway smooth muscle mass, goblet cell hyperplasia/metaplasia, fibrosis, airway obstruction by mucus and inflammatory cells, inflammation of the airway adventitia, loss of epithelial integrity, vascular remodeling, and alterations in the peribronchial elastic fiber system.*
In human asthmatics, remodeling also occurs in peripheral noncartilaginous airways, which, by virtue of their smaller caliber and greater total cross-sectional area, account for the majority of airflow impairment during asthma exacerbations. 25,77,133,144 Mucus metaplasia, airway smooth muscle mass, airway obstruction by mucus and inflammatory cells, and neutrophil infiltration of the submucosa are significantly increased in noncartilaginous airways of severe and fatal asthma relative to other asthma phenotypes. 16,77,80,117,133 However, remodeling in noncartilaginous airways is poorly characterized in severe nonfatal human asthma, which accounts for less than 15% of human asthmatics yet constitutes the majority of human asthma morbidity and health expenditures. 24,35,36,124,126,133 To refine the biologic relevance of equine pasture asthma to human asthma, the objective of this investigation was to systematically characterize small noncartilaginous airways from each lung lobe of horses with pasture asthma for structural changes collectively termed airway remodeling.
Materials and Methods
Animals and Sample Collection
Formalin-fixed archived lung tissues used in this study were collected from 15 horses with pasture asthma and 9 clinically normal control horses of mixed breeds between 1996 and 2004. Horses had been maintained in a research herd and shared the same environment for periods ranging from 3 to 48 months. Experimental procedures had been approved by the Animal Care and Use Committee of Louisiana State University. Diseased horses ranged from 10 to 27 years of age (mean ± SD, 15.4 ± 5.3 years, 9 females and 6 castrated males). Control horses ranged from 7 to 22 years of age (mean 15.6 ± 5.3 years, 3 females and 5 castrated males). Criteria for horse selection, clinical evaluation, and gross postmortem findings in horses with pasture asthma have been described in a prior investigation by Costa et al. 28 Seven diseased and 5 control horses in the current investigation were also employed in that prior investigation.
Briefly, diagnosis of equine pasture asthma was based on a history of seasonal remission of clinical disease during cool seasons, followed by episodic and reversible obstructive respiratory disease while grazing pasture during hot, humid conditions. Overt respiratory distress was characterized by a clinical score of respiratory effort (CSRE) ≥4.5, maximal change in pleural pressure (ΔPplmax) ≥12 cm H2O, audible expiratory wheezes in the lung fields, and neutrophilic airway inflammation (≥10%) in BALF. Criteria for the CSRE have been previously described. 108 Two of the 15 pasture asthma-affected horses were euthanized during disease remission, as defined by normal bronchovesicular sounds during lung auscultation with a rebreathing bag, CRSE ≤3.5, ΔPplmax of 6 to 6.5 cm H2O, and <3% neutrophils in BALF. Control horses lacked historical episodic pasture-associated respiratory disease during the summer and had normal bronchovesicular sounds during lung auscultation with a rebreathing bag, CRSE ≤3, ΔPplmax of 5 to 9 cm H2O, and <15% neutrophils in BALF. Five horses in which ΔPplmax was not measured were categorized as control and diseased based upon the remaining criteria. Negative bacteriologic culture of BALF was a criterion for inclusion of diseased and affected horses in this investigation. Supplemental Table S1 shows the characteristics of individual horses, designating them as in disease exacerbation, remission, or control, including respiratory distress as measured by the CSRE, ΔPplmax, percentage of neutrophils in BALF, thoracic auscultation, and the presence of intercurrent disease.
Horses were euthanized by intravenous (IV) administration of sodium pentobarbital (100 mg/kg, IV) at least 24 hours after BALF sample collection. Lung specimens measuring 3 × 3 × 3 cm were sampled from the right apical, left apical, right diaphragmatic, left diaphragmatic, and accessory lung lobes. Each specimen was selected to contain at least 1 bronchus of 4 to 8 mm diameter. Specimens were immediately immersed in aqueous buffered zinc formalin for 24 hours prior to routine processing, embedding in paraffin, and sectioning.
Histological Staining
Histological sections were cut at 5 μm. Two stains were employed: HE and a modified Movat’s pentachrome I stain. With Movat’s pentachrome I stain, cytoplasm is stained pink, collagen stains yellow, elastic fibers stain black, ground substance stains indigo, nuclei stain dark blue, muscle stains red, and mucin and cartilage stain bright blue. The elastic system in airways is composed of elastic, elaunin, and oxytalan fibers. Our pentachrome staining protocol was modified by the addition of orcein and fuchsin to detect elaunin and oxytalan in addition to elastic fibers, because the elastic system fiber composition within the lung has been demonstrated to vary with airway size and the airway layer being evaluated. 11
Lesion Grading
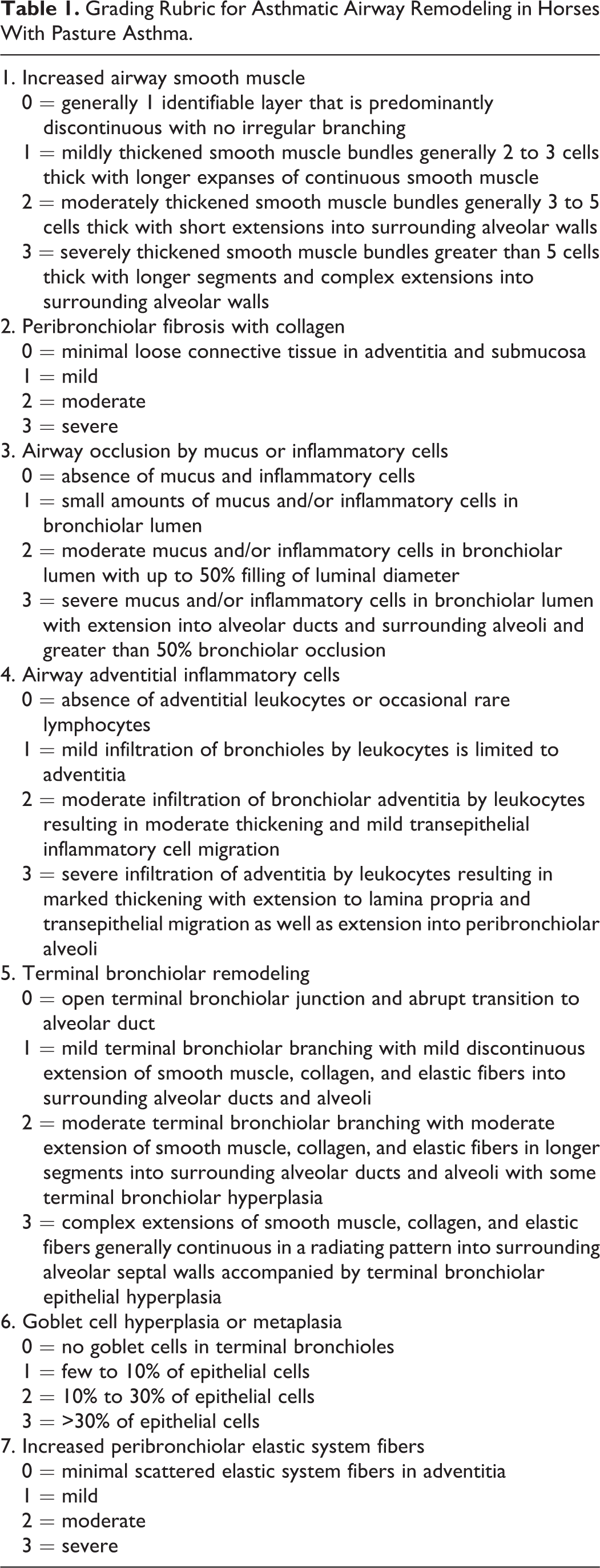
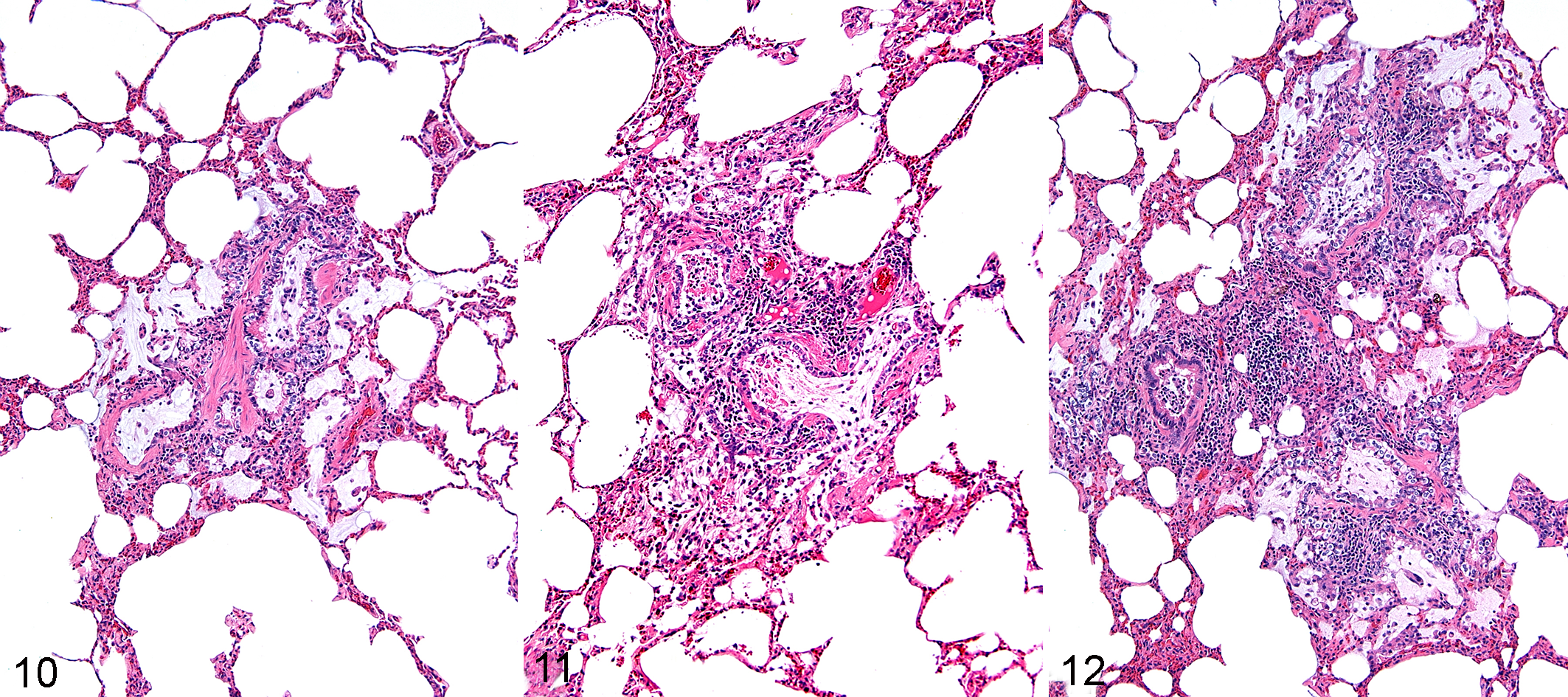
To create a rubric suited to scoring morphologic changes of human asthma in the noncartilaginous airways (ie, bronchioles) of necropsy specimens from horses with pasture asthma, characteristic structural changes termed airway remodeling in human asthma were employed. 3,5,13,33,104 These characteristic changes included increased airway smooth muscle, airway adventitial infiltration by leukocytes, peribronchiolar fibrosis with collagen, goblet cell hyperplasia and metaplasia, airway occlusion by mucus or inflammatory cells, and increased number of peribronchiolar elastic system fibers. Routine HE-stained histologic lung sections from horses with pasture asthma were surveyed for these characteristic lesions. From the spectrum of identified lesions, scoring criteria were established for increased airway smooth muscle, peribronchiolar fibrosis with collagen, airway occlusion by mucus or inflammatory cells, airway adventitial inflammatory cells, goblet cell hyperplasia and metaplasia, and increased peribronchiolar elastic system fibers (Table 1). Scoring criteria were adapted from previous descriptions of airway remodeling in human asthma and rubrics adapted for lung tissue from equine necropsy samples. † Moreover, in the survey phase, a lesion herein termed terminal bronchiolar remodeling was identified. After the rubric was established, 2 observers (C.F. and J.C.) repetitively graded noncartilaginous airways in a subset of sections from pasture asthma and nondiseased control horses until scoring variations were <1 grade for all lesions.
Grading Rubric for Asthmatic Airway Remodeling in Horses With Pasture Asthma.
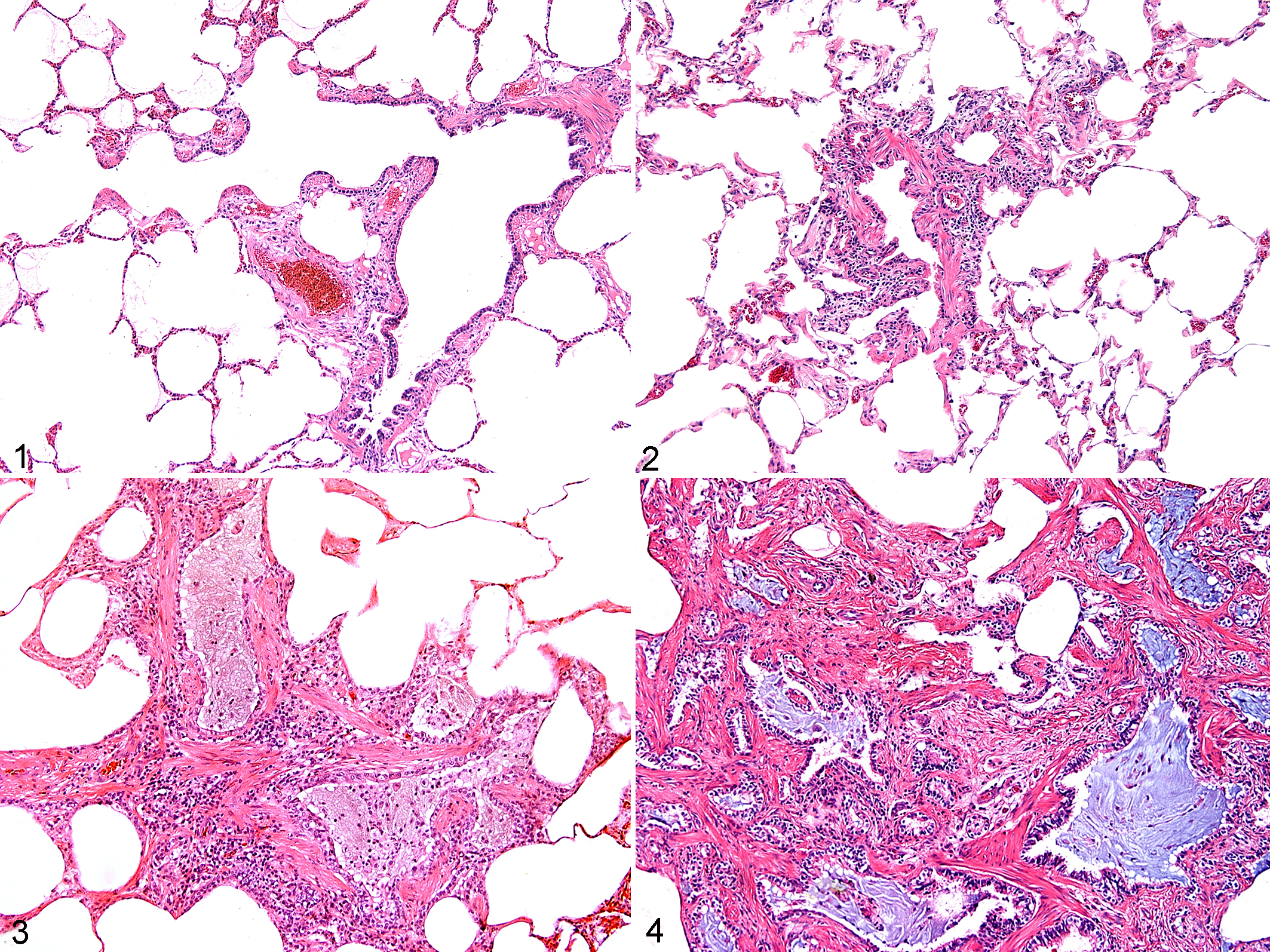
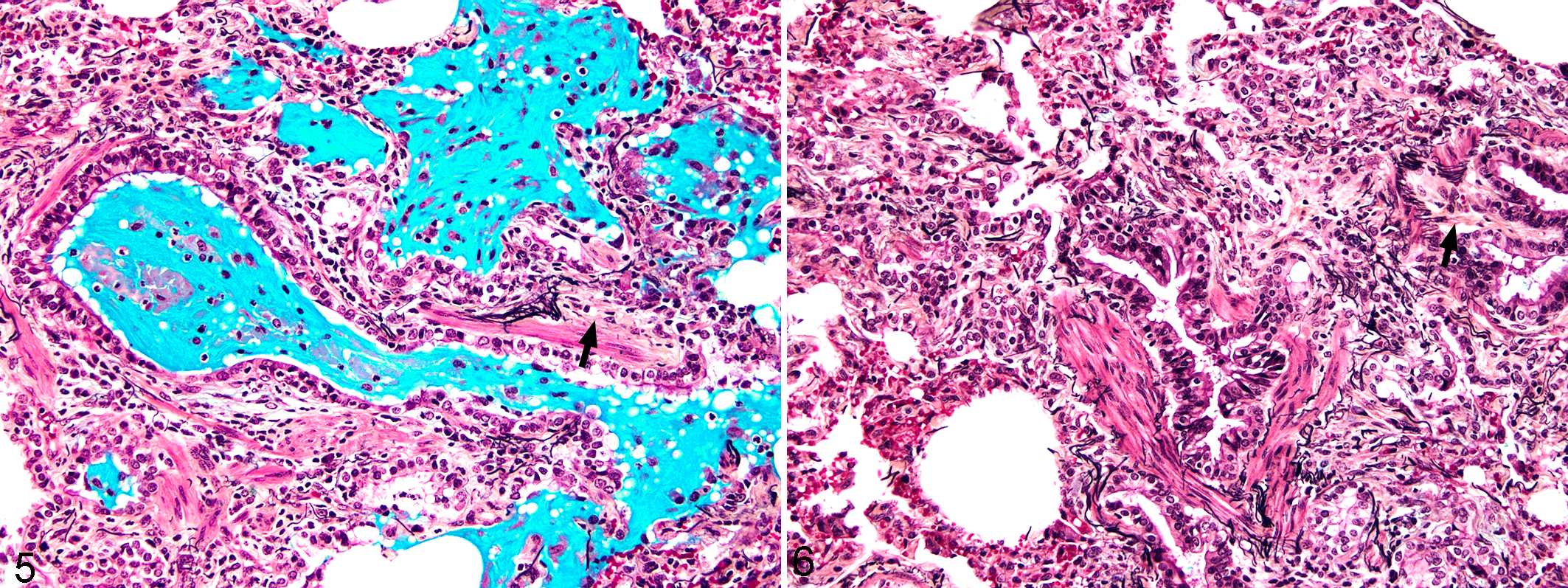
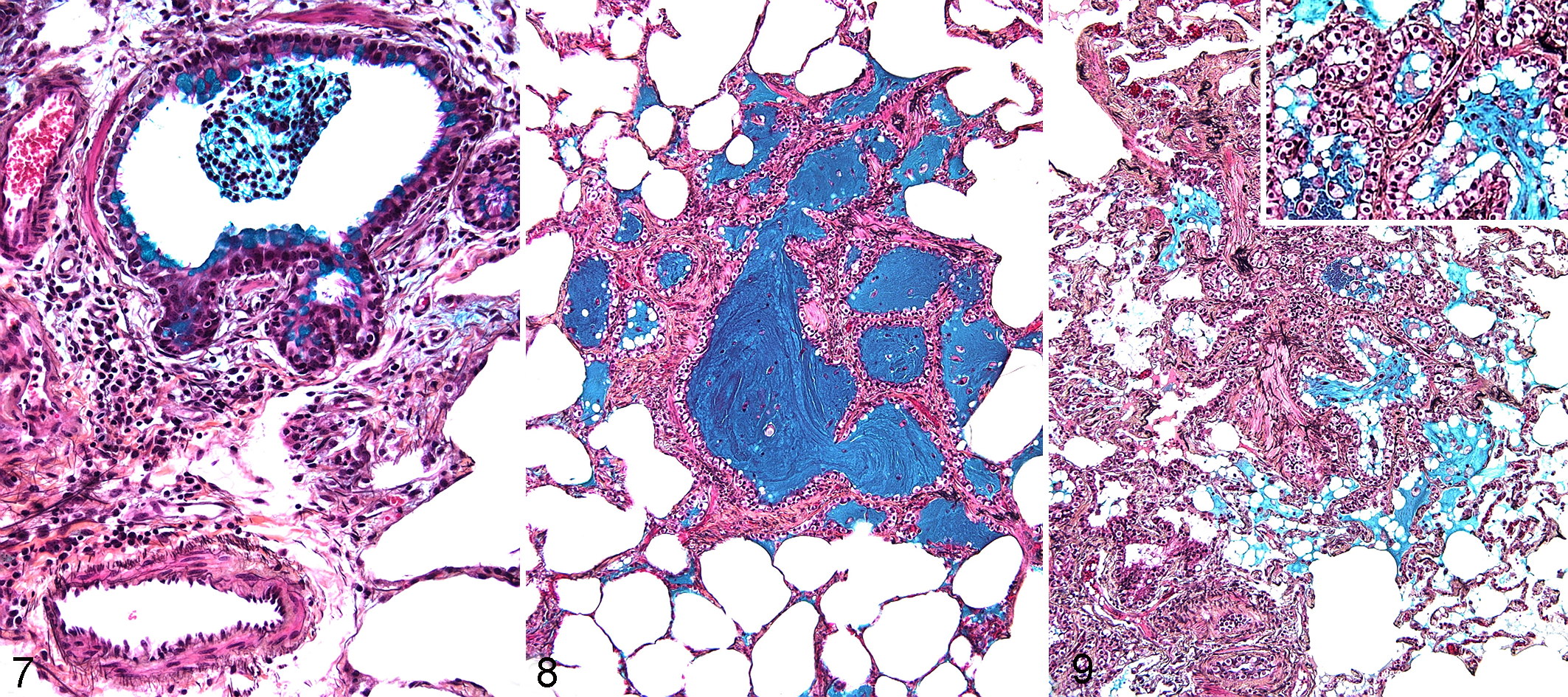
To compare airway remodeling changes in the lungs of horses with pasture asthma to controls, histologic sections were digitally imaged at 15×, enlarged to fill a standard 8.5 × 11-inch page, and printed using a color printer. A grid comprising 7 equal rows and 7 equal columns (49 sectors) was overlaid on the image. All noncartilaginous airways were identified by their grid position for each histological section and scored. Microscopic evaluation was initially made at 100× and was varied for appropriate evaluation of features in Table 1. Scores reflect the comprehensive presence of features in each airway and were not restricted to a single field at a specified magnification. Increased airway smooth muscle, peribronchiolar fibrosis with collagen, airway occlusion by mucus or inflammatory cells, airway adventitial inflammatory cells, terminal bronchiolar remodeling, goblet cell hyperplasia and metaplasia, and increased peribronchiolar elastic system fibers were scored using a scale of 0 to 3 where 0 = normal, 1 = mild, 2 = moderate, and 3 = severe according to criteria listed in Table 1 and Figs. 1 to 15. Percentages of goblet cells were determined by counting all epithelial cells in the bronchiole. Identification and differentiation of scoring parameters, including mucin in goblet cells, collagen, and elastic fibers, were facilitated by pentachrome staining. Terminal bronchioles were distinguished by observation of a discernable bronchiole opening into a region of alveoli. 86,98,108,134 Where observers differed, the final score was assigned after reviewing the image and averaging the scores by the observers.
Statistical Analysis
For statistical analysis, airways were randomized using random numbers. A mixed-effects logistic regression model was used to describe the effect of independent variables on the occurrence of histologic outcomes using PROC GLIMMIX (SAS 9.1 for Windows; SAS Institute, Cary, NC). Histological parameter scores were dichotomized with scores of 0 considered negative (0) and scores of 1, 2, or 3 considered positive. The independent variables in the model were disease status (pasture asthma vs control), lung lobe, and age, where horses were grouped as ≤15 years and >15 years. Hierarchical data structure was accounted for by including lung lobe (horse ID) and horse ID as random effects. Pairwise comparisons of lobe effects were determined using least squares means with the Tukey-Kramer adjustment for multiple comparisons. The threshold for statistical significance was P < .05.
Results
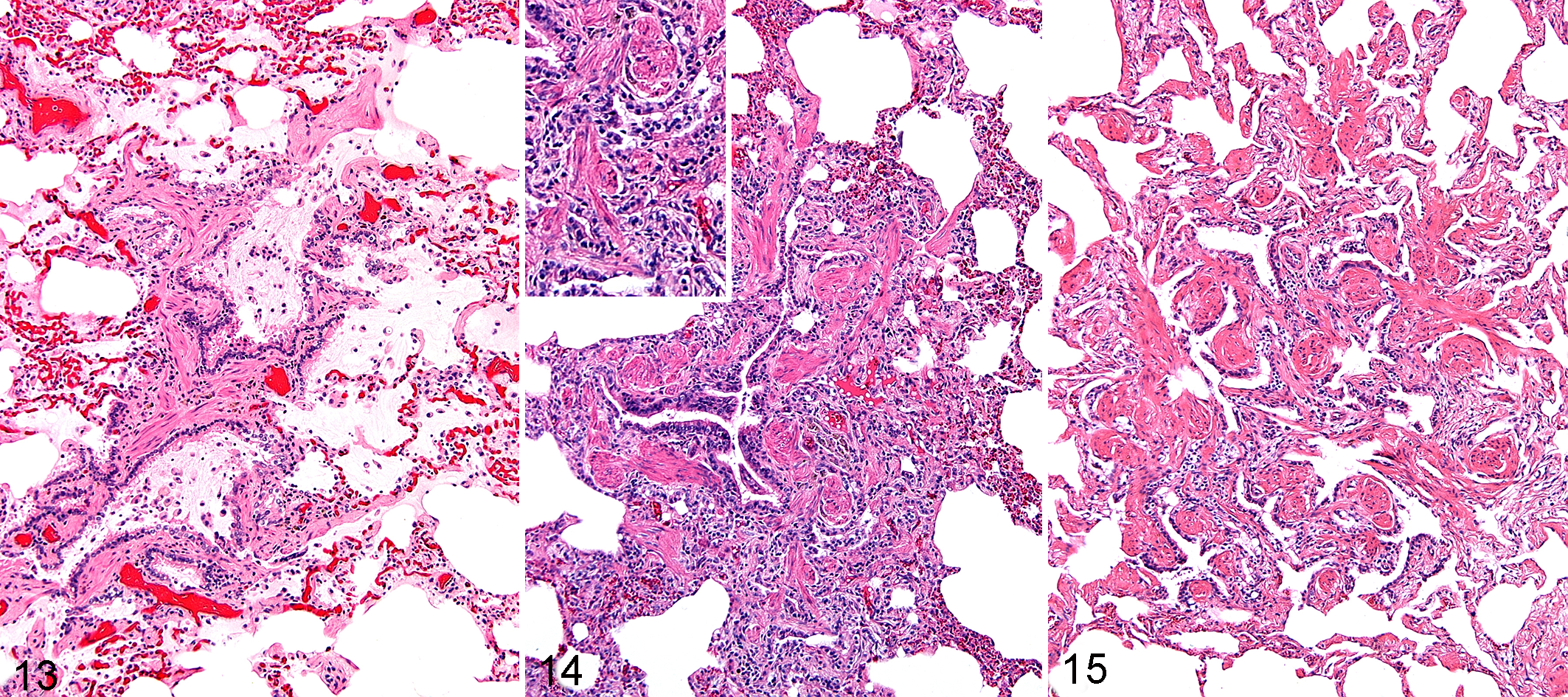
During the survey of HE-stained lung sections from pasture asthma-affected horses, lesions of airway remodeling in human asthma were identified, including increased airway smooth muscle, peribronchiolar fibrosis with collagen, airway occlusion by mucus or inflammatory cells, airway adventitial inflammatory cells, goblet cell hyperplasia and metaplasia, and increased peribronchiolar elastic system fibers (Figs. 1 –12). In addition, a lesion herein termed terminal bronchiolar remodeling (Figs. 13–15) was identified. Terminal bronchiolar remodeling is observed as a complex tissue disorganization at the level of the terminal bronchiole, characterized by varying degrees of extension of smooth muscle, collagen, and fibers into surrounding alveolar ducts, alveoli, and alveolar septal walls and accompanied by varying degrees of terminal bronchiolar epithelial hyperplasia.
A total of 1078 airways were evaluated and scored in 74 lung lobes from 15 horses with pasture asthma. One left diaphragmatic lobe was not available for evaluation in the diseased group. A total of 537 airways were similarly evaluated in 37 lung lobes from 9 control horses. In the control group, 5 right diaphragmatic, 2 accessory, and 1 left apical lobe were not available for evaluation. The disease status, location, and assigned lesion scores for each airway are provided in Supplemental Table S1. Employing a statistical model that accounted for age, disease status, and lung lobe, the frequencies of each of the 7 histologic lesions were significantly increased in horses with pasture asthma relative to control horses (Table 2). Increases in airway smooth muscle, terminal bronchiolar remodeling, goblet cell hyperplasia/metaplasia, and the peribronchiolar elastic fiber system were highly significant (P < .001) in pasture asthma horses. Increases in peribronchiolar fibrosis, airway occlusion by mucus and inflammation, and airway adventitial inflammatory cells also met the criteria established for statistical significance (P < .04). In horses with pasture asthma, the airway adventitial inflammatory response consisted of lymphocytes and neutrophils in which lymphocytes predominated. Eosinophils were uncommon, and intraluminal cells were predominantly neutrophils.
Effects of Pasture Asthma Status and Age Group (>15 Years) on the Frequency of Asthmatic Airway Remodeling Lesions.a
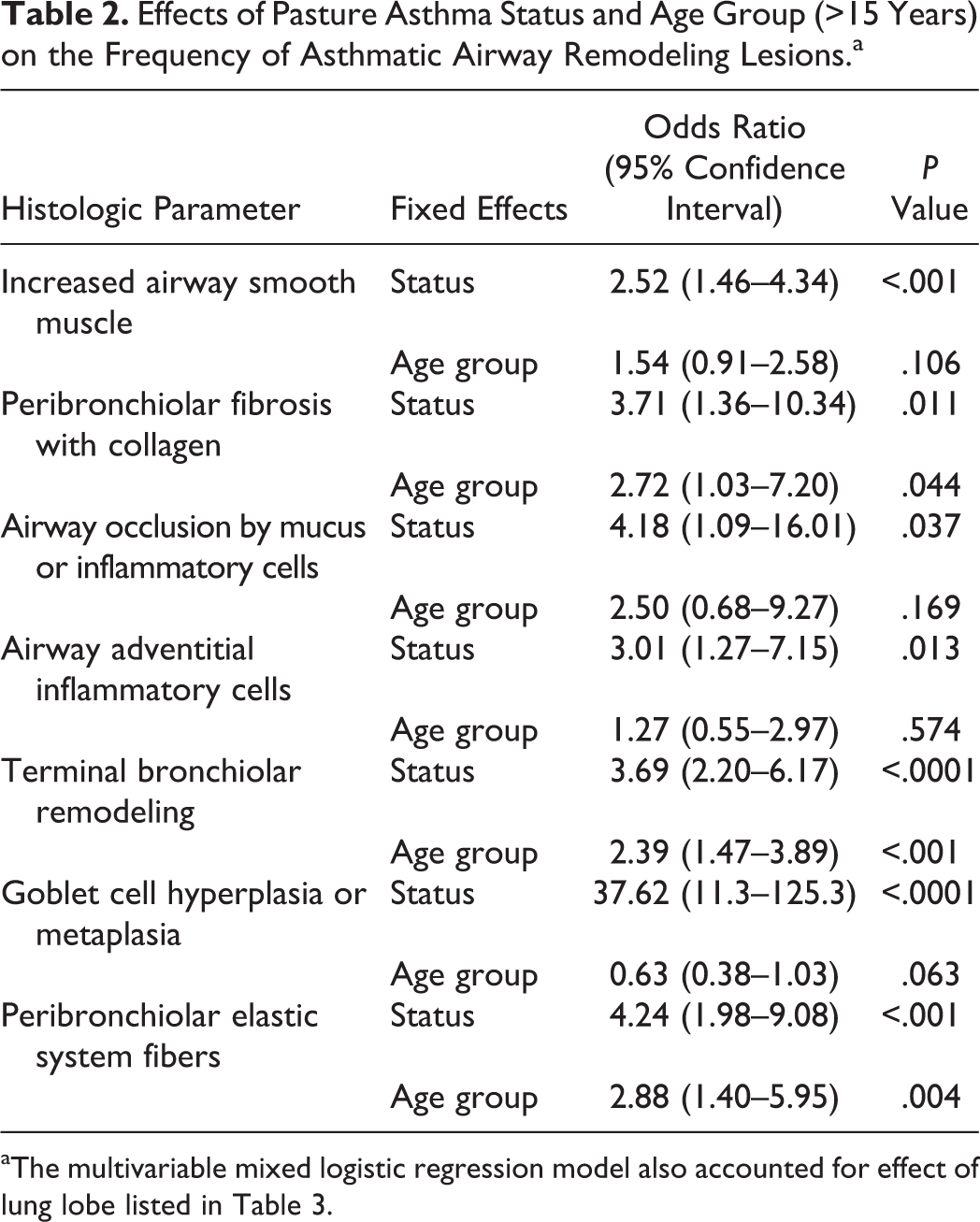
aThe multivariable mixed logistic regression model also accounted for effect of lung lobe listed in Table 3.
The frequency of histologic lesions was not significantly different between age groups for increased airway smooth muscle, airway occlusion by mucus and inflammation, airway adventitial inflammation, and goblet cell hyperplasia/metaplasia. In contrast, older horses had significantly greater (P < .05) peribronchiolar fibrosis, terminal bronchiolar remodeling, and peribronchiolar elastic system fibers relative to younger horses.
Of the 7 criteria evaluated, significant differences in the frequency of increased airway smooth muscle (P = .001), terminal bronchiolar remodeling (P = .0001), and peribronchiolar elastic system fibers (P < .0001) were identified between lung lobes (Table 3). Increased airway smooth muscle, terminal bronchiolar remodeling, and peribronchiolar elastic system fibers were identified in the diaphragmatic lobes based on pairwise comparisons of the right or left diaphragmatic lobes to the accessory, left, or right apical lobes. These differences reached statistical significance in 12 of these 18 (66%) possible pairwise comparisons to the diaphragmatic lobes. In contrast, the same lesions did not differ significantly in all pairwise comparisons between the accessory and the right and left apical lobes. The occurrence of peribronchiolar elastic system fibers in the accessory lobe was not significantly different from the right diaphragmatic lung lobe, to which it is anatomically opposed. This contrasts with the relative increase in elastic system fibers in airways of the left diaphragmatic lobe relative to accessory lobe airways, which was highly significant (P < .0001).
Comparison of Equine Asthma Lesion Frequency Between Lung Lobes.a
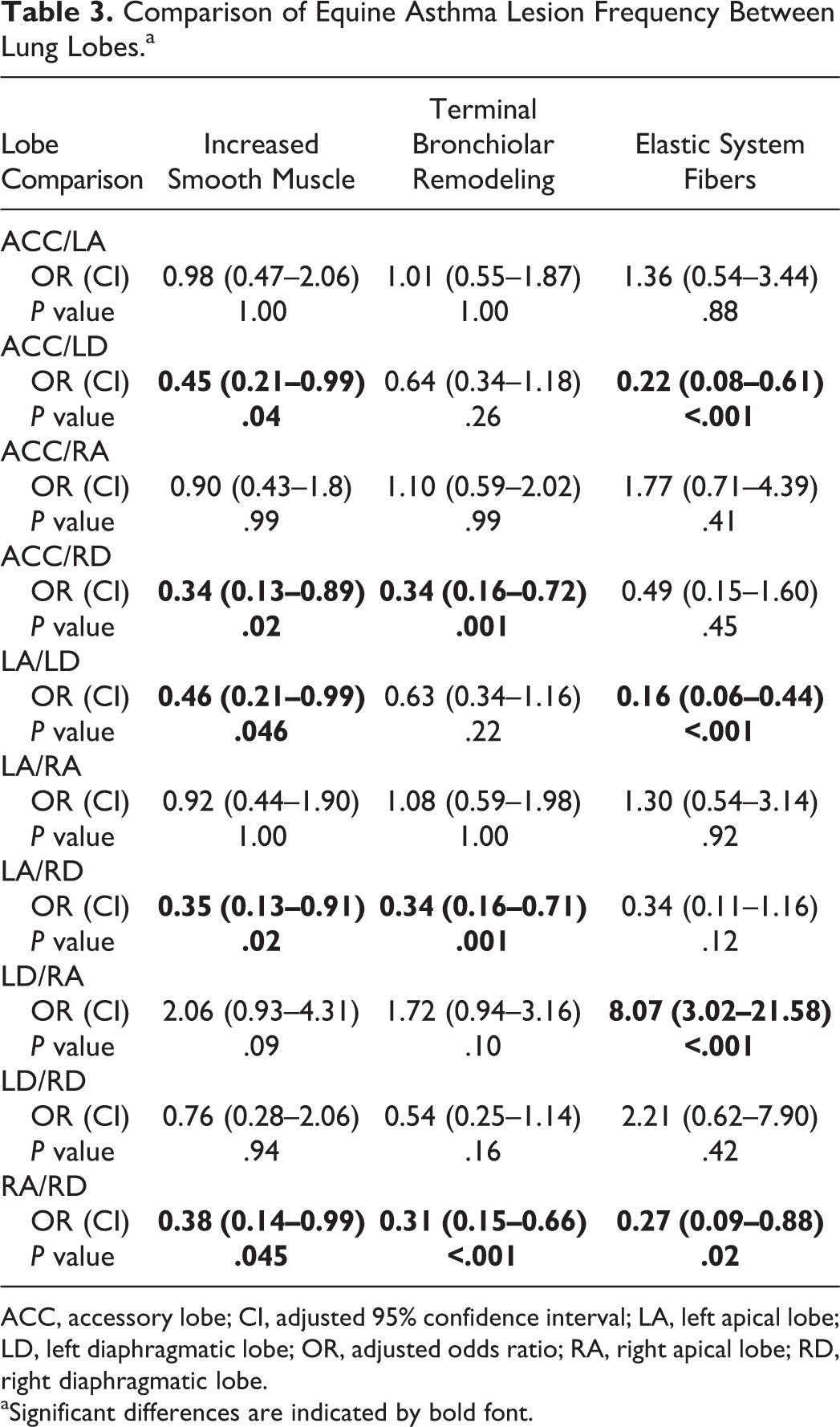
ACC, accessory lobe; CI, adjusted 95% confidence interval; LA, left apical lobe; LD, left diaphragmatic lobe; OR, adjusted odds ratio; RA, right apical lobe; RD, right diaphragmatic lobe.
aSignificant differences are indicated by bold font.
Discussion
In this investigation, histologic lesions that characterize airway remodeling in human asthma, including goblet cell hyperplasia/metaplasia, increased airway smooth muscle, increased fibers of the peribronchiolar elastic system, adventitial inflammation, peribronchiolar fibrosis, and airway occlusion by mucus, were significantly overrepresented in noncartilaginous airways of horses with pasture asthma. The identified morphologic homology between airway structural changes in equine pasture asthma and human asthma builds upon published epidemiologic, clinical, and molecular homologies between equine pasture asthma and adult-onset, nonallergic, neutrophilic, and severe phenotypes of human asthma, as previously detailed. ‡ These airway structural changes, which are known to correlate to airflow obstruction, progression, and severity of human asthma, reflect pathophysiologic events occurring during disease and support the translational relevance of equine pasture asthma for investigating the pathobiology of airway remodeling and progressive airflow obstruction in human asthma. § More broadly, this homology supports translational relevance of equine pasture asthma to other aspects of human asthma pathobiology, where research that can affect the human condition is urgently needed.
Asthma is a clinical syndrome characterized by variable airway hyperresponsiveness leading to respiratory distress and airway obstruction. Airway wall remodeling and intraluminal obstruction in small noncartilaginous airways of horses with pasture asthma are described in this study that align to small noncartilagenous airway lesions reported in human asthma and in horses with barn dust asthma. || Intraluminal inflammatory infiltrates and mucus from metaplastic goblet cells cause airway obstruction, which increases with bronchoconstriction. 28,113,114 In horses with barn dust asthma, composite histologic scores that included measures of bronchiolar obstruction as well as airway wall thickening have been correlated to measures of respiratory impairment using multiple breath nitrogen washout. 41 Computational airway modeling predicts that modest increases in airway wall thickness anticipated from airway wall lesions described in this study have little effect on ventilation in relaxed airways but precipitate marked decreases in airway lumen size during mild bronchoconstriction. 95 By modeling increases in small airway wall thickness throughout the lung, small airways are predicted to cause precipitous increases in airway resistance that result in small noncartilagenous airway closure and cause air trapping in subtending airways at physiologically relevant levels of bronchoconstriction. 70,140,141 These computational predictions align to clinical findings in human asthma that small airways provide the majority of airflow limitation during asthma, that increased airway wall thickness worsens airway obstruction during bronchoconstriction, and that wall area and degree of air trapping are the strongest predictors of the magnitude of lung function impairment with moderate and severe obstruction, respectively. 19,56,100,136,132,144
Despite physiologic and histopathologic evidence that human asthma involves both central and small noncartilaginous airways to the level of terminal bronchiolar regions, small airway pathology in severe human asthma has not been as extensively investigated. ¶ This is in part due to difficulty in accessing these regions, relative to the ease of attaining biopsies from the larger airways via bronchoscopy. Most investigations of small airway lesions in severe human asthma are derived from patients that died of asthma, which may not be reflective of patients with severe asthma. 133
In human and equine asthma, perfusion of poorly ventilated alveoli subtending bronchiolar obstruction that results from lesions, including those described in this study, causes ventilation to perfusion (V/Q) inequality and hypoxemia. 18,45,99,114 Hypoxemia is a reliable finding from which compensatory increases in ventilation result in normal to decreased PaCO2 in both horses and humans. 10,18,44,99,114 In horses with barn dust asthma and decreased PaCO2, Nyman et al 99 demonstrated scattered increased V/Q inequality, congruent with hyperinflation of the lung, which compromises pulmonary capillary beds. This has been well characterized in human asthma. 18 As predicted by airway modeling experiments, progressive obstruction, which can cause airway closure with true air trapping in alveoli subtending closed bronchioles, causes progressive decreases in V/Q and more profound hypoxemia, raising PaCO2 toward or above normal levels in both human asthma and horses with barn dust asthma. 84,85 Air trapping, as described in horses with pasture asthma and barn dust–associated asthma, is difficult to identify premortem because of the requirement for methods such as inert gas washout and inhaled radiotracers that can identify nonventilated portions of the lung. 28,38,41
Goblet cell hyperplasia/metaplasia, which was 38 times more likely in diseased vs control airways, has been repeatedly identified as the most significant change in the epithelium of human asthmatics across all disease severities. 2,50,101 Goblet cells are the source of mucus production that causes airway obstruction in small noncartilaginous airways in asthma, and goblet cell hyperplasia/metaplasia has been similarly identified in the bronchioles of horses with barn dust asthma. 2,75,86,110 In addition to mucus production, which contributes to airway obstruction, goblet cell hyperplasia/metaplasia reduces airway caliber. Large increases in goblet cells have also been identified in severe and fatal human asthma, with the degree of mucus plugging reflective of the severity of airflow obstruction. 2,31,117,123 Similar correlation between mucus plugging and the severity of airway obstruction has been documented in horses with pasture asthma. 28 Age was not a factor in the frequency of goblet cells, indicating that goblet cell hyperplasia/metaplasia can be helpful in the differentiation of pasture asthma from other causes of respiratory impairment, particularly in horses over 15 years of age.
We note a discrepancy in peer-reviewed literature regarding the terms goblet cell metaplasia and goblet cell hyperplasia. Whereas hyperplasia refers to increases in cell numbers, metaplasia refers to the change from one mature cell type to another. Goblet cells were extremely rare in noncartilaginous airways from control horses in our observations. Of the 537 airways, goblet cells were identified in only 3 airways and at a score of 1 (<10% of all epithelial cells, Suppl. Table S1). This finding aligns to published observations that did not identify goblet cells in equine bronchioles (ie, noncartilaginous airways), indicating that goblet cell metaplasia is an accurate term for the presence of goblet cells in equine bronchioles. 98,110 This absence of goblet cells in normal equine bronchioles is analogous to normal human bronchioles. Goblet cells were also not identified in the terminal bronchioles of nondiseased horses, in agreement with prior characterizations of equine terminal bronchioles. 98,108,134
Horses with pasture asthma in this investigation were 4.2 times more likely to have increased elastic system fibers in their noncartilaginous airways, relative to nondiseased controls. Age was a factor in increasing elastic system fibers, with horses over 15 years of age having significantly more elastic system fibers. Abnormalities in the airway elastic fiber system are identified in human asthmatic airways and are believed to alter tethering, distensibility, and elastic recoil of the extracellular matrix. 94,112 This relationship is supported by correlations between pulmonary elastance and increases in the peribronchiolar elastic fibers reported in horses with barn dust asthma. 122 Increases in the peribronchiolar elastic fiber system have been identified in both noncartilaginous peripheral and large airways of severe and fatal human asthmatics. 11,17,48,89,90,133 However, examinations of the elastic fiber system in noncartilaginous airways from fatal asthmatics, in a manner analogous to this investigation, did not differ from nonrespiratory acute deaths. 17,48,90
In human asthma, elastic system injury has been shown to contribute to air trapping—a phenomenon that correlates to human asthma severity. 56 This trapping of air in the terminal airways has also been described in the lungs of equine pasture asthma and barn dust asthma cases that fail to collapse at necropsy. 15,28,38,43,131 Air trapping was presumed to account for normal ventilation using multiple breath nitrogen washout in horses with barn dust asthma, despite severe lung lesions and clinical evidence of pulmonary overinflation (expanded lung borders). 41 This is because nitrogen washout cannot identify sections of the lung that lack ventilation. Increased airway neutrophils, which are a defining characteristic of equine pasture asthma, are also an independent risk factor for air trapping in human asthma that is attributed to neutrophil-derived matrix metalloproteinase–induced fragmentation of elastic system fibers and matrikine activities of these fragments that drive chemotaxis, inflammation, cellular proliferation, and remodeling. 15,30,39,67,115 Differences in airway size, the airway layer being evaluated, and the staining method employed all contribute to variability in investigations of fibers of the airway elastic system. To comprehensively stain the 3 primary fibers of the elastic network, pentachrome stain, which only stains elastic fibers, was modified in this investigation by the addition of orcein and fuchsin to stain elaunin and oxytalan. We did not attempt to differentiate superficial fibers that tether the basement membrane (predominantly oxytalan fibers) from deeper elastic fibers near airway smooth muscle due to their intimate relationship in small noncartilaginous airways. 11,90
Horses with pasture asthma were 2.5 times more likely than nondiseased horses to have increased airway smooth muscle in their noncartilaginous airways. We have previously described increases in bronchiolar smooth muscle in postmortem samples from horses with pasture asthma. 28,96 Increases in airway smooth muscle and smooth muscle proliferation have also been identified in the noncartilaginous airways from horses with barn dust asthma. 61 Increased airway smooth muscle is a defining criterion of airway remodeling in human asthma and is considered the primary factor leading to airflow obstruction in human asthma. 69,88 Mathematical modeling also predicts increased airway smooth muscle mass as the most probable cause of airway hyperresponsiveness. 8,88 Increases in airway smooth muscle are well characterized in bronchi and small noncartilaginous airways from human asthmatics of all severities, including severe and fatal asthma. 8,46,62,57,69,80,133
In conducting airways of human asthmatics, there is evidence that hyperplasia, hypertrophy, and increased numbers of myofibroblasts contribute to the increase in muscle mass and that both hyperplasia and hypertrophy correlate to asthma severity. 8,9,62,74 Many investigations indicate that airway smooth muscle hyperplasia is a key structural change in the progression from less severe to more severe forms of human asthma. 8,106,132 Although staining to identify smooth muscle proliferation was not performed in this investigation, we identified smooth muscle extending into the terminal bronchioles of diseased horses. This observation was rarely identified in airways from nondiseased horses at this anatomic level. While very small amounts of smooth muscle are present and can sometimes be observed at the entrance to the acinar airways, our failure to identify smooth muscle in terminal airways is congruent with observations in human airways, suggesting that increased smooth muscle at this level is more indicative of hyperplasia or metaplasia/transdifferentiation and not airway smooth muscle hypertrophy. 69 Extension of airway smooth muscle toward the acinar airway is anticipated to limit alveolar ventilation and was recently described by Trejo Bittar et al 133 in a transbronchial biopsy from a patient with severe asthma.
We identified a previously unreported complex tissue disorganization at the level of the terminal bronchiole, herein termed terminal bronchiolar remodeling, as overrepresented in airways of horses with pasture asthma in a highly significant manner. Terminal bronchiolar remodeling is characterized by varying degrees of smooth muscle, collagen, and elastic fiber extension into the septa of surrounding alveolar ducts and alveoli, accompanied by varying degrees of terminal bronchiolar epithelial hyperplasia. Smooth muscle was a prominent feature of this lesion. To our knowledge, this is the first report of this lesion. The occurrence of this lesion at the terminal bronchiole, which supplies the secondary lobule, together with the observed progression of terminal bronchiolar remodeling into the acinar areas, is of particular interest because several lines of evidence implicate structural abnormalities in this region in the previously described phenomenon of air trapping. # Based on an associated compromise of the terminal bronchiole, which is the functional gateway to the alveolus, we postulate that terminal bronchiolar remodeling impairs alveolar ventilation in a fashion that is proportional to lesion severity. Functional studies are necessary to address this possibility. A similar lesion in human asthma, although not currently identified, could also result in air trapping in human asthmatics.
Peribronchiolar collagen deposition was 3.7 times more likely in airways from horses with pasture asthma vs controls, a finding congruent with increased matrix deposition in the airways in human asthma. 19,142 Furness and colleagues 40 did not identify differences in the quantities of type I and III collagen in the lamina propria or the adventitia of noncartilaginous airways from horses with barn dust asthma using immunohistochemistry, but Setlawke et al 122 reported significant increases in collagen in the lamina propria using pentachrome stain, as well as increases in type I and III collagen based on immunohistochemistry. As with this latter investigation, our recognition of peribronchiolar fibrosis in the adventitia of noncartilaginous airways from pasture asthma horses was likely facilitated by the use of pentachrome staining. 122 Two types of collagen deposition are typically characterized in bronchial biopsies of human asthmatics: subepithelial thickening of the lamina reticularis region of the basement membrane and submucosal fibrosis. 19,133,142 Airway fibrosis contributes to airway obstruction that is incompletely reversible with administration of a bronchodilating agent in some human asthmatics. 5,143 However, collagen proliferation in large cartilaginous airways does not differentiate severe from mild and moderate human asthma. 5,23,106,143 Fibrosis that was evident in noncartilaginous airways from horses with pasture asthma in this study is described as peribronchiolar, as it was identified both within the submucosa and external to the airway smooth muscle layer (adventitial). The latter is not typically evaluated in human endobronchial biopsies. We did not observe thickening of the lamina reticularis region in noncartilaginous airways of horses with pasture asthma, which is congruent with a recognition that lamina reticularis thickening segregates with eosinophilic airway inflammation, proeosinophilic cytokines, and transforming growth factor (TGF)–β signaling in human asthma. 20,22,23,37,92 Although lamina reticularis thickening has been associated with severity, frequency, duration of symptoms, and the degree of airway hyperreactivity in human asthmatics, it is not observed in human asthma with the neutrophilic airway inflammation that is characteristic of equine pasture asthma. 12,19,20,66,72,93,133
Odds of airway occlusion by mucus and/or inflammatory cells in horses with pasture asthma were 4.2 times greater than in nondiseased horses and did not differ in horses over 15 years of age. Airway occlusion by mucus and inflammatory cell plugs contributes to ventilation impairment in human asthma and is reported to increase 30-fold in fatal asthma. 2,16,31,34,81,117,123 Mucus accumulation has been previously described as a predominant histopathologic alteration in small airways of horses with pasture asthma and barn dust asthma, with strong correlations between disease exacerbation and mucus hypersecretion and airway plugging. 27,28,101,106 Airway occlusion can persist in diseased horses even during clinical disease remission, when inflammation, clinical signs, and bronchospasm are reduced or nonexistent. 42 Cough frequency has been demonstrated to strongly correlate to the magnitude of neutrophil counts in BALF from horses with barn dust asthma. 101 BALF from pasture asthma-affected horses demonstrates inflammatory exudate consisting primarily of neutrophils and lymphocytes, whereas eosinophils are uncommon. 25 These collective findings indicate that airway obstruction by mucus and inflammatory cells observed in asthma and severe asthma in humans is appropriately modeled in horses with pasture asthma.
Our morphologic investigation indicated that airway adventitial inflammation was predominantly lymphocytic in horses with pasture asthma, while neutrophilic inflammation predominated in the airway lumen. Horses with pasture asthma had 3.0 times greater odds of having airway adventitial inflammation than nondiseased control horses, independent of advancing age (>15 years). In severe human asthma, the most accentuated inflammatory process occurs in the noncartilaginous airways, contributing to small airways as the major location of airway obstruction. 54,55 While lymphocytic inflammation of the bronchioles is also a feature in severe human asthma, diverse samples from severe asthmatics (both fatal and nonfatal), including BALF, tracheal aspirates, sputum, airway mucosa, and submucosa/muscularis, demonstrate a relationship between an increase in neutrophils in asthmatic airways (relative to nondiseased individuals) and asthma severity. 16,91,102,127,139 This distinction has not been characterized in equine pasture asthma. Neutrophils are also a major inflammatory cell in acute severe asthma that necessitates mechanical ventilation. 88,114 In fatal asthma attacks, bronchiolar neutrophilic inflammation predominates and eosinophilic inflammation is less prevalent, especially if the interval between onset of attack and death is short. 127 This finding has led to the hypothesis that fatal attacks of asthma may be triggered by stimuli that elicit neutrophilic inflammatory responses. 16 Similarities between the predominance of lymphocytic airway inflammation and increases in neutrophils in pasture asthma, barn dust asthma, and certain subtypes of severe human asthma suggest that these spontaneous equine diseases are relevant to investigate the pathobiology of neutrophilic inflammation in severe human asthma.
In comparing noncartilaginous airway remodeling between lung lobes, highly significant differences in the frequencies of increased airway smooth muscle, terminal bronchiolar remodeling, and fibers of the peribronchiolar elastic fiber system were identified. While these findings warrant further characterization, their distribution suggests an anatomic predisposition to more severe lesions in the diaphragmatic lobes. We hypothesize that this is attributable to the increased length and associated increases in resistance of airways supplying the diaphragmatic relative to the apical lobes. This nonhomogeneous distribution of airway remodeling in the lungs of horses with pasture asthma is, to our knowledge, the first description of this phenomenon in an animal asthma model and is congruent with evidence of structural changes in the airways in human asthma that are not homogeneously distributed. Specifically, heterogeneously distributed changes in airway wall thickness and wall area have been identified in the central and peripheral airways of human asthmatics using high-resolution thoracic computed tomography (CT) and noble gas magnetic resonance imaging (MRI). 53,56 The nonhomogeneous distribution of lesions identified in the lungs of horses with pasture asthma provides a unique facet of this animal asthma model for investigations of airway remodeling and ventilation heterogeneity in asthma.
Inclusion of disease and age as independent risk factors for lesion frequency was influenced by recognition of dynamic strain/damage and repair mechanisms that occur naturally in the airway epithelial-mesenchymal trophic unit and cause airway structural changes during aging that are accelerated with disease. 21,51,63,128,145 Age (>15 years) was an independent risk factor that increased the frequencies of terminal bronchiolar remodeling, peribronchiolar elastic system fibers, and peribronchiolar fibrosis by 2- to 3-fold. Similarly, degradation of elastic system fibers has been described in nondiseased human airways with advancing age, and patients over 40 years of age are overrepresented among fatal asthmatics while also having significant increases in elastic fibers in the central airways. 68,90 Practically, these age effects highlight the relevance of increases in airway smooth muscle, goblet cell metaplasia, airway adventitial inflammation, and airway occlusion by mucus and inflammation for refining the histologic diagnosis of pasture asthma in older horses, as well as the importance of age and factors relevant to dynamic damage and repair of the lung when selecting nondiseased control populations.
In conclusion, horses with pasture asthma exhibit key clinical features of human asthma and develop lesions of asthmatic airway remodeling in their noncartilaginous airways that include increases in airway smooth muscle, goblet cell hyperplasia/metaplasia, increased elastic system fibers, inflammation of the adventitia, airway occlusion by mucus and inflammatory cells, and peribronchiolar “submucosal” fibrosis. A lesion herein termed terminal bronchiolar remodeling was identified that bears anatomic and physiologic relevance to ventilation heterogeneities described in asthma. Increased airway smooth muscle, airway occlusion by mucus and inflammatory cells, airway adventitial inflammation, and goblet cell hyperplasia/metaplasia were identified to be significantly associated with disease status but not advancing age. Conversely, elastic fibers, terminal bronchiolar remodeling, and peribronchiolar fibrosis were significantly more frequent in horses over 15 years of age and in horses with pasture asthma compared to controls. While proving useful for the diagnosis of pasture asthma, these structural changes in noncartilaginous airways from horses with pasture asthma also correlate to advancing airway impairment in human asthma and support the pathobiologic relevance of equine pasture asthma to human asthma.
Footnotes
Notes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Financial support for this research and its publication was provided by the Office of Graduate Research and the Departments of Clinical Sciences and Population and Preventative Medicine, College of Veterinary Medicine, Mississippi State University.
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.