
Abstract
Invasive urothelial (transitional cell) carcinoma (UC) is the most common cancer in the canine urinary tract. Prolonged survival of dogs with UC due to better management of the primary tumor and prevention of urethral obstruction might have contributed to an apparent increase in distant metastasis. Metastasis to bone is particularly concerning because the ensuing pain often leads to euthanasia; however, little is known of the frequency, site, or nature of UC skeletal metastasis. In a retrospective analysis, 17 (9%) of 188 canine UC cases had histologically confirmed skeletal metastasis, mainly to the vertebrae. In a prospective analysis of 21 dogs with UC that underwent total body computed tomography (CT) at euthanasia followed by a standardized pathologic examination, skeletal lesions detected on CT were suspected to be metastatic in 4 dogs and were confirmed as metastatic UC histologically in 3 (14%) dogs. In all 3 cases, skeletal metastasis had been suspected based on history and physical examination; however, 1 dog had additional CT-detected skeletal metastases in a clinically unsuspected location, and 2 dogs had histologically confirmed skeletal metastases that corresponded to nonspecific osseous lesions on CT. These findings suggest that total body CT could be helpful in detecting skeletal metastasis as a cause of bone pain in dogs with UC as well as in identifying clinically “silent” sites of skeletal metastasis.
Keywords
Invasive urothelial carcinoma (UC), also known as transitional cell carcinoma, is the most common urinary tract cancer in dogs. 9 Dogs of all breeds can be affected, but Scottish Terriers, West Highland White Terriers, Wire Hair Fox Terriers, Shetland Sheepdogs, and Beagles are especially susceptible. 9 Most dogs with UC in the Purdue University Veterinary Teaching Hospital (PUVTH) participate in clinical trials, with most surviving several months to over a year with good quality of life. The prolonged survival is due, at least in part, to better control of the primary neoplasm and better management of urethral obstruction. 10 However, with longer survival, distant metastases appear to be more common and could become a more frequent reason for euthanasia of dogs with UC. 10 Historically, distant metastases of UC were typically found in 16% of dogs at diagnosis and 50% of dogs at death; more recently, however, the prevalence of distant metastasis, predominantly to lungs, identified at autopsy in dogs treated for UC in the PUVTH was 58%. 9,10
Skeletal metastasis is of special concern because bone pain and the rapid decline in quality of life often lead to euthanasia, yet little information on skeletal metastasis in dogs with UC is available. In a retrospective study of medical records from 5 veterinary teaching hospitals in the United States and Canada, 115 dogs were documented to have neoplasia of the lower urinary tract. 16,22 Of 101 cases with abdominal radiographs, 8 (7.9%) had lumbar vertebral and pelvic bone metastases. 16 The authors concluded that abdominal radiography would facilitate the detection of these metastatic lesions. 16 In another report, using the same study set, skeletal metastases were confirmed in 4 of 42 (9.5%) dogs with UC that were necropsied. 22 These metastases were detected based on clinical signs and examination findings, but “silent” metastases (not associated with clinical signs), or those not evident on clinical or postmortem examination, may go undetected. Thus, the exact rate of skeletal metastasis, the most common sites, whether the metastases are predominantly lytic or sclerotic, or whether current therapies influence their development or progression are still unknown. The purpose of this analysis was to determine the frequency and the characteristics of skeletal metastases in dogs with UC, using computed tomography (CT) and autopsy, and to evaluate the potential role of total body CT in their detection. The expectation was that CT would facilitate the detection (with histology for confirmation) of UC skeletal metastases, even those without clinical signs, palpable masses, or macroscopic lesions.
Materials and Methods
Study Overview
The study included 2 components: (1) a retrospective analysis of archival canine UC autopsy cases at the Indiana Animal Disease Diagnostic Laboratory (ADDL) between July 2000 and February 2013 and (2) a prospective analysis of dogs with UC in the PUVTH that underwent total body CT at euthanasia followed by a standardized pathologic examination to detect and characterize skeletal metastases by frequency, location, and imaging and pathologic features from February 2013 to March 2014.
Tumor Grade
All primary UCs in the prospective analysis plus those with skeletal metastases in the retrospective analysis were classified as low grade or high grade based on modifications of the World Health Organization/International Society of Urological Pathology Consensus Classification and application of the grading system to canine UC (J. A. Ramos-Vara, personal communication, spring 2014). 1,8,10,17,18 A UC was distinguished from benign urothelial proliferation by the presence of >7 cell layers. A UC was considered high grade if 1 or more of the following features were observed: loss of superficial umbrella cells, lamina proprial or tunica muscularis invasion, moderate to marked nuclear atypia (karyomegaly, loss of polarity, clumped chromatin, prominent nucleolus), more than 1 mitotic figure per 400× field, mitotic figures beyond the basilar layer, or atypical mitotic figures. The UC was considered low grade if the following features were present: maintenance of superficial umbrella cells, absent to rare lamina proprial invasion, orderly and well-differentiated cells, minimal cytologic variation, <1 mitotic figure per 400× field, and predominantly limited to the basilar layer.
Retrospective Analysis
Autopsy case records in the ADDL archives were searched for dogs with “transitional cell carcinoma” from July 2000 to February 2013. Pathology reports were reviewed for documentation of skeletal metastasis, and the anatomic location was recorded. Available histologic slides from the urinary tract and bone were evaluated to grade the primary UC and characterize the skeletal metastasis. Point estimate of prevalence with 95% confidence interval (CI) was reported. CIs were generated using exact binomial distribution to account for the small sample size.
Prospective Analysis
Participating Dogs
Following approval of the Purdue Animal Care and Use Committee and informed pet owner consent in writing, dogs with histologically confirmed UC were enrolled. These were dogs sequentially presented to the PUVTH when the dog owner had requested euthanasia due to declining quality of life relating to the UC or other conditions. Dogs were accepted regardless of the presence or absence of bone or joint pain or any radiographic or CT evidence of bone metastases. A complete physical examination, including palpation of bones and joints, along with radiographs in 7 dogs to assess for bone metastasis, were performed prior to euthanasia. The goal was to enroll a minimum of 20 dogs with the expectation that skeletal metastases would occur in at least 2 to 3 dogs according to the prevalence reported in previous studies. 16,23
CT Scan
Following euthanasia, a total body CT scan at 0.63-mm slice thickness was performed. The CT scanning parameters, such as kVp, mA, and field of view, were selected according to the size of the dog. Evaluation of CT images with a bone window was performed by a single radiologist (H.G.H.) prior to the autopsy to identify potentially metastatic bone lesions. Features noted included the presence of osteolysis, osteosclerosis, or a periosteal reaction; the size and location of the lesion; and the confidence level of metastasis (metastatic, potentially metastatic, nonmetastatic). Large (≥3 mm in diameter) osteolytic lesions with a concurrent periosteal reaction were classified as a metastatic lesion. Small (<3 mm diameter) osteosclerotic or osteolytic lesions with only a mild periosteal reaction, or a mild periosteal reaction without osteolysis, were classified as potentially metastatic (“uncertain” in level of confidence). Lesions that lacked osteosclerosis, osteolysis, or a periosteal reaction were classified as not a metastatic lesion.
Autopsy Protocol
Following the CT scan, dogs underwent an autopsy protocol standardized for this study. The autopsy was done with knowledge of the CT findings. In addition to major organs, the vertebral bodies and the right and left humerus and femur were grossly evaluated on longitudinal section. Any additional bone lesions identified by CT and areas associated with bone pain on physical examination were also evaluated grossly and histologically.
Histopathology Protocol
Samples of liver, kidney, spleen, lung, heart, pancreas, urinary bladder, urethra, prostate (for male dogs), iliac lymph nodes, lumbar vertebrae (L4–L6), femoral bone marrow, brain, and any grossly abnormal tissues were fixed in 10% neutral-buffered formalin for 24 to 48 hours, and sections were stained with hematoxylin and eosin (HE). Evidence of vascular (venous or lymphatic) invasion was documented in the primary bladder tumor. For the 21 cases in the study, bony tissue (lumbar vertebrae L4–L6 and any bone lesions identified by postmortem CT scan or gross examination) was evaluated histologically following decalcification with formic acid/formaldehyde solution (Surgipath Decalcifier I, Leica Biosystems, Richmond, IL) for up to 2.5 weeks. Femoral bone marrow was evaluated with HE and cytokeratin AE1/AE3 immunohistochemistry (IHC).
IHC Protocol
IHC with diaminobenzidine chromogen for cytokeratin AE1/AE3 (mouse monoclonal anti-human cytokeratin; DakoCytomation, Inc, Carpinteria, CA) and uroplakin III (mouse monoclonal antibody; Fitzgerald Industries International, Acton, MA) was performed as described 24 on selected soft tissue and bone metastases for confirmation of epithelial and urothelial origin, respectively. Uroplakin III IHC was also performed as needed on primary urinary bladder cancers to confirm urothelial origin. Uroplakin III expression has been documented in 91% of canine UCs and is generally considered specific for UC, 20 although possible immunoreactivity has been reported in canine prostatic carcinoma. 11
In selected cases, femoral bone marrow was evaluated with HE and cytokeratin AE1/AE3 IHC according to the above protocol. These were compared with the bone marrow of 3 adult dogs without epithelial cancer that were similarly evaluated with HE and cytokeratin AE1/AE3 IHC.
Immunohistochemical reactions were recorded as location of labeling (membrane vs cytoplasm), approximate percentage positive cells, and intensity of immunoreactivity (negative, weak-moderate, or strong). For uroplakin III expression, the section was considered positive if at least 5% of neoplastic cells were labeled. 20
Results
Retrospective Analysis
In the ADDL archives, 188 canine cases of UC were identified during the 12.5-year period. Of these, 17 (9%; 95% CI, 5%–14%) had histologically confirmed bone metastasis at autopsy (Supplemental Table S1). Ten were spayed female, 6 were castrated male, and 1 was a nonneutered male. Of the above-noted breeds with increased susceptibility, the breeds included 4 Scottish Terriers, 2 Shetland Sheepdogs, and 1 West Highland White Terrier.
In all 17 cases with bone metastasis, the primary UCs were classified as high grade. Vertebrae were a site of metastatic UC in 8 of the 17 dogs with skeletal metastasis and were the only site of bone metastasis in 5 of the 8 dogs, making this the most commonly detected skeletal site of metastatic UC, followed by appendicular bones, pelvis, ribs, and skull in 7, 4, 3, and 1 dog, respectively. Six dogs had more than 1 site of bone metastasis. One case of skeletal UC metastasis had histologic evidence of osteosclerosis indicated by a cortex thickened by new bone production; the remaining cases had osteolysis indicated by a thin, disrupted cortex with thin, scalloped, fragmented, or lost medullary trabeculae with periosteal new bone formation. Of the 17 dogs with skeletal metastasis, 13 (76%) also had pulmonary metastasis and 14 (82%) had lymph node metastasis.
Prospective Analysis
Twenty-one dogs, 10 castrated male and 11 spayed female, of various breeds and ages (range, 9-16 y; median, 11.5 y), with histologically confirmed UC were enrolled in the analysis (Supplemental Table 2). All 21 primary urinary bladder UCs were classified as high grade. Seven of the 21 dogs had pain by the time of death for which bone metastasis could be included in the differential diagnosis. Based on the CT examination, skeletal lesions were classified as metastatic in 4 of the 21 dogs (Nos. 1, 2, 20, and 21), and as potentially metastatic in 1 dog (No. 17). Histologically, skeletal metastasis of UC was confirmed in 3 of the 21 dogs (Nos. 1, 2, and 17). Pathologic and CT findings of histologically confirmed skeletal metastases are summarized in Supplemental Table 2 (see supplemental Supplemental Table 3 for complete CT findings).
Clinical, CT, and Pathologic Findings
In 13 of the 21 dogs, osseous lesions were found on CT scans (Supplemental Table S1). In 4 dogs (Nos. 1, 2, 20, 21), CT lesions were considered metastatic based on the presence of a large osteolytic lesion with a periosteal reaction. Osseous metastasis of UC was confirmed histologically in 2 (Nos. 1 and 2) of these dogs but not in the other 2 dogs (Nos. 20 and 21). One dog (No. 17) had multiple small osteolytic areas with a mild ventral periosteal reaction in the L7 vertebral body that were considered potentially metastatic on CT and were confirmed as metastatic UC histologically. Another 8 dogs (Dogs 3, 4, 5, 8, 13, 14, 15, 16) had potentially metastatic osseous lesions on CT, including focal osteosclerosis and osteolysis, with mild periosteal reaction or changes consistent with hypertrophic osteopathy; however, metastasis was not identified histologically in targeted sections of bone.
In Dog 1, lesions in the right humerus and left scapula were osteolytic with cortical destruction and a periosteal reaction (Figs. 1–4). A third lesion, in L3 vertebra, had only osteolysis. Histologically (Figs. 5 and 6), the 3 lesions in this dog corresponded to osteolytic metastasis, with periosteal proliferation in the right humerus and left scapula. In the same dog, no lesions were seen on CT in L4 vertebra; however, osteolytic metastasis was identified histologically.
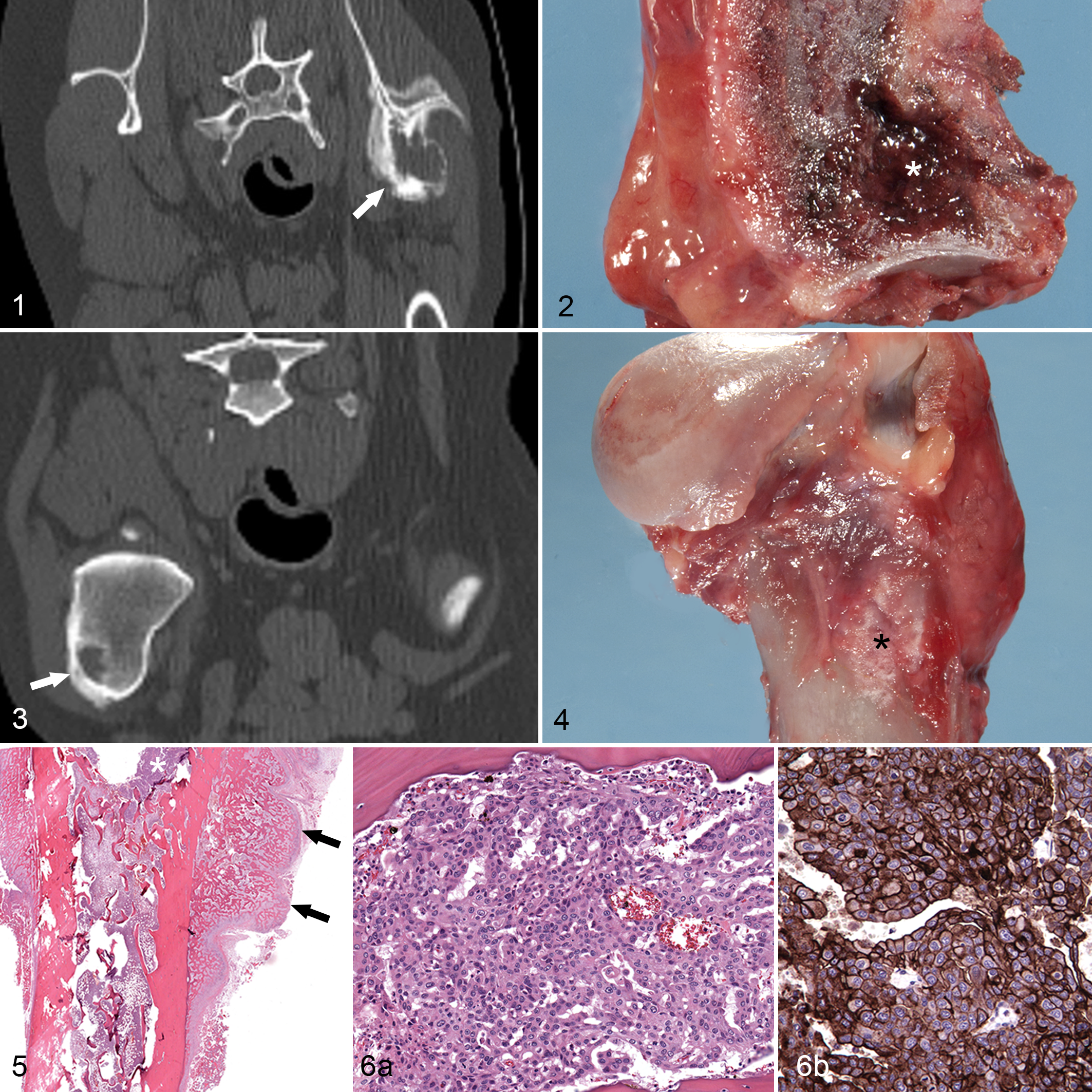
Urothelial carcinoma, metastases, dog No. 1.
In Dog 2 (Figs. 7–11), CT identified 9 osteolytic lesions with cortical destruction and a periosteal reaction in L4–L7, sacrum, right ileum, and 4 caudal vertebrae; all were confirmed as osteolytic metastasis histologically. This dog also had a focal osteolytic lesion in T7 considered on CT to be potentially metastatic and confirmed histologically as osteolytic metastasis.
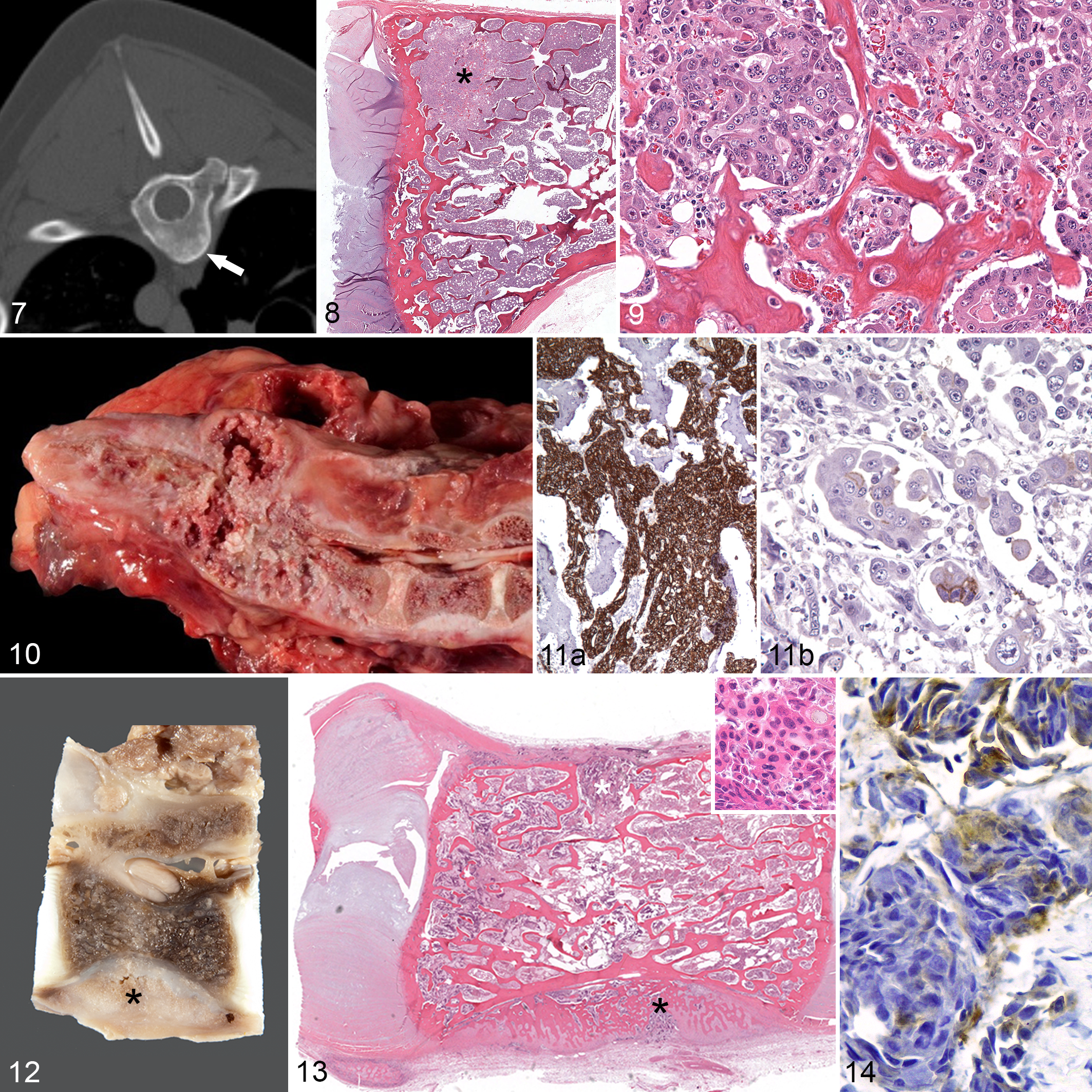
Urothelial carcinoma, metastases, dog No. 2.
In Dog 17 (Figs. 12–14), L7 and L6 had multiple small osteolytic lesions of the body and lamina with a mild smooth periosteal reaction ventrally that were classified on CT as potentially metastatic lesions. Histologically, the lesions corresponded to osteolytic metastasis with a periosteal reaction of L7.
Dogs 20 and 21 had lesions that were classified as metastatic on CT, but metastatic UC was not detected histologically in either dog. Dog 20 had multiple small areas of osteolysis with cortical destruction and a periosteal reaction of the spinous process of the first thoracic vertebra (T1). Dog 21 had multiple osteolytic areas with a periosteal reaction of T13 and L1 vertebral bodies.
Findings in Cases of Osseous Metastasis of UC
In summary, 3 (Nos. 1, 2, and 17) of the 21 dogs with UC had CT bone lesions that were confirmed histologically as metastatic UC. All osseous metastatic lesions were classified as osteolytic histologically with periosteal new bone formation.
Pulmonary metastasis was documented histologically in 10 of the 21 dogs and was detected with antemortem imaging in all but 2 cases (Nos. 5, 19). Iliac lymph node metastasis in 11 of 21 dogs was detected in all cases with antemortem imaging. Additional distant sites included kidney (2 dogs), adrenal gland (3 dogs), heart (1 dog), thyroid gland (1 dog), and pancreas (1 dog). In selected sections of femoral bone marrow evaluated with HE and cytokeratin AE1/AE3 IHC, individual or clusters of cells with positive membranous cytokeratin expression were seen, mainly along the periphery of the sample and rarely within hematopoietic tissue. When compared with the 3 control dogs (without epithelial cancer), there were similar IHC findings of individual or clusters of cytokeratin-positive cells, generally at the edges of the section. The presence of a few cytokeratin-positive cells in bone marrow was therefore attributed to contamination from autopsy instruments or the band saw.
Discussion
Canine UC is similar to human invasive bladder cancer in histopathologic features, biological behavior, and response to therapy. 7,9,10 Although studies in dogs have been limited, skeletal metastasis is accepted as a major complication of human UC because of its frequency, its negative effects on quality of life, and its typical resistance to conventional chemotherapy. 6,21,24 In separate studies, skeletal metastasis developed in about one-third of 179 21 and 367 23 human cases of invasive bladder cancer. The prevailing theory for skeletal metastasis is that neoplastic cells escape the primary site, travel through the blood to wide-channeled sinusoids of the bone marrow, migrate across the sinusoidal wall, invade the marrow stroma, generate their own blood supply, and travel to the endosteal surface, where they form solid metastases. 14 Here, the cells stimulate the activity of osteoclasts or osteoblasts, thereby determining whether the developing metastases will be predominantly osteolytic or sclerotic. Each of these steps involves important molecular interactions between the tumor cells and the normal host cells and pathways involving receptor activator of nuclear factor kappa-B ligand, parathyroid hormone-related protein, and other proteins. 14 These molecular targets have been used in developing new therapies for skeletal metastasis. In dogs, however, the processes involved in skeletal metastasis of UC have not been defined, so the application of molecularly targeted therapies has not been possible.
Results of the analyses presented here suggest that skeletal metastasis is also an important complication in canine UC. Skeletal metastases were found histologically in 9% of cases in the retrospective analysis and 14% of cases in the prospective analysis. Skeletal metastases could have been missed in the retrospective analysis because skeletal CT had not been performed and bones were not routinely evaluated grossly or histologically unless there was a suggestive clinical history.
Weaknesses in the prospective analysis include small sample size, lack of antemortem diagnostic imaging in most cases (and no nuclear scintigraphy), lack of antemortem blood or bone marrow samples for detection of circulating tumor cells, and the limited number of histologic sections of CT-targeted bone lesions. In all 3 dogs with CT-detected and histologically confirmed bone metastasis, some of the CT-detected lesions that were classified as metastatic or potentially metastatic were unrelated to clinically detected bone pain and therefore would probably have gone undetected at autopsy had CT not been performed. Results in these 3 dogs demonstrate that total body CT could facilitate the identification of UC skeletal metastases and that metastatic sites might be found antemortem even in the absence of associated clinical signs. Another 3 dogs (Nos. 4, 7, 18) had possible bone pain reported, yet evidence of bone metastasis was not detected on CT or histologic examination; thus, CT could also potentially help to rule out metastatic UC.
An unexpected result of the prospective analysis was the frequency of osseous changes on CT. Lesions that lacked osteosclerosis, osteolysis, or a periosteal reaction were classified as nonmetastatic and had no gross or histologic evidence of metastasis. Some of the small lucencies detected on CT could be attributed to adipose tissue in the medulla. Lesions were considered metastatic on CT if large areas of cortical lysis with concurrent periosteal reaction were identified. In 2 dogs (Nos. 20 and 21), bone lesions were classified on CT as metastatic, but no corresponding lesion was identified histologically. Histologic failure to detect bone metastasis or another lesion to explain the CT findings could be attributed to destruction or sectioning error with the band saw at autopsy or during tissue trimming and preparation of histologic sections. Nevertheless, documenting that the majority of osteolytic lesions with cortical destruction and a periosteal reaction were indeed metastatic UC and that the lumbar vertebrae may be the most common site of skeletal metastases could facilitate targeted diagnostic imaging for early detection and intervention. In humans, the use of positron emission tomography and CT for detection of abnormal bone physiology is recommended. 14,15
In human studies, the pelvis and vertebrae have been the most common sites of UC metastasis to bone. 21,23 In this canine analysis, the fourth to the sixth lumbar vertebrae were evaluated histologically in all 21 dogs. Each of the 3 dogs with identified skeletal metastasis had metastasis to a lumbar vertebral body, suggesting that this is also a common site for canine metastatic UC. This correlates with the results of the retrospective analysis and reported studies in which the vertebrae were also the most common bony site of canine UC metastasis. 16,22
The current analyses set the stage for further investigations that could lead to a better understanding of skeletal metastasis and how to prevent or treat it more effectively. In other types of human cancer, a significant positive association has been observed between the presence of cancer cells in the bone marrow and the development of distant metastasis and also the specific development of skeletal metastasis. 2,13,19 In humans with invasive bladder cancer, the presence of cancer cells, or more specifically cytokeratin-positive tumor cells, in the bone marrow has been significantly associated with distant metastasis, 5 although the specific relationship between skeletal metastasis and tumor cells in the marrow has not yet been determined. In the prospective analysis reported here, bone marrow was evaluated with cytokeratin AE1/AE3 IHC to look for (metastatic) epithelial cells, but the use of the band saw may have resulted in epithelial cell contamination of the marrow specimens. Future studies using core biopsy specimens may facilitate more accurate evaluation of bone marrow for metastatic cells. Cancer cells in peripheral blood (circulating tumor cells [CTCs]) have been identified in human patients with invasive bladder cancer and other cancers, although the relationship between CTCs and cancer outcome and the relationship between CTCs and cancer cells in bone marrow is likewise not fully defined. 3,4,12 Experimental models of bladder cancer metastasis do not fully replicate the process as it occurs in humans. Dogs with naturally occurring bladder cancer, however, could offer a unique opportunity to address unanswered questions. In addition, molecular characterization could aid in identifying specific pathways in skeletal metastasis for improved prevention, detection, and treatment. Drugs are available that target specific pathways of skeletal metastasis in human cancer; advancements in knowledge through studies in dogs could benefit both species.
Footnotes
Acknowledgements
We thank Patty Bonney and Chris Royce, Purdue Comparative Oncology Program, and Dee Dusold, Indiana ADDL histology laboratory, for technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.