
Abstract
Novel therapies, including molecular targeted therapies, are being developed for the treatment of human gliomas. To use such therapies for canine gliomas, more complete characterization of molecular targets is required. Epidermal growth factor receptor (EGFR) is one such therapeutic target used in human glioma trials, and the Ki-67 labeling index (LI) is a marker of proliferation and a prognostic indicator. The objectives of this cross-sectional study were to evaluate the expression of EGFR and Ki-67 in canine gliomas and to determine if immunopositivity is associated with tumor type and histologic grade. Thirty-one formalin-fixed, paraffin-embedded canine gliomas were evaluated for EGFR and Ki-67 expression by immunohistochemistry. EGFR immunopositivity was evaluated using a semi-quantitative score and the Ki-67 LI calculated based on the percentage of positive cells. EGFR and Ki-67 expression were identified in 16 of 31 (52%) and 28 of 31 (90%) tumors, respectively. EGFR expression was significantly greater in high-grade tumors compared with low-grade tumors (P = .04) and was significantly greater in gliomatosis cerebri compared with oligodendroglioma (P = .002), astrocytoma (P = .01), and oligoastrocytoma (P = .04). The Ki-67 LI was significantly greater in high-grade tumors compared with low grade tumors (P = .02); the median Ki-67 LI was 2.3% (range, 0%–17.6%) for low-grade tumors and 9.3% (range, 1.7%–41.0%) for high-grade tumors. A significant moderate correlation was identified between EGFR immunopositivity and Ki-67 LI (r = 0.47, P = .007). Overall, EGFR may be a suitable therapeutic target for some canine gliomas, particularly gliomatosis cerebri.
Keywords
Effective treatment of canine glial tumors remains frustratingly elusive despite numerous options becoming available over the past 20 years. These include palliative therapy, surgery for cytoreduction, radiation therapy, chemotherapy, convection-enhanced delivery of therapeutic agents, immunotherapy, and various combinations of these treatment modalities. 3,7,15,25,27 Despite the various treatment options available, the prognosis is poor, and the survival time ranges from days to months. 3,7,15,27,43 With a better understanding of the molecular pathogenesis of these tumors, new, more successful therapies may be developed.
Epidermal growth factor receptor (EGFR) is a transmembrane glycoprotein, which transduces signals across the plasma membrane to initiate signaling pathways involved in the cell cycle, cell proliferation and survival, cell migration and adhesion, and angiogenesis. 2,6,11,14,22,26,31,42 EGFR is expressed throughout development and life, being involved in neural development and migration, as well as the proliferation and differentiation of astrocytes; however, when dysregulated, EGFR promotes oncogenesis. 2,6,11,22,31 In human glial tumors, EGFR has been shown to stimulate the growth, invasion, and migration of glioma cells, thus contributing to self-sufficiency, insensitivity to growth inhibitory signals, evasion of apoptosis, unlimited replication potential, tissue invasion, and metastasis and sustained angiogenesis; these properties constitute the 6 hallmarks of cancer. 2,9,36,39
EGFR is an important therapeutic target in human oncology. 1,6 Expression of EGFR has been identified in human gliomas and is associated with tumor grade. 11,12,14,23 The use of EGFR as a potential therapeutic target in gliomas is being investigated in human clinical trials and includes the use of monoclonal antibodies, EGFR kinase inhibitors, vaccines, and RNA-based agents; data from some stage I and II clinical trials show positive results. 29,37,42 Therefore, if EGFR expression is identified in canine gliomas, EGFR-dependent human diagnostics, treatments, and prognostic factors may translate to dogs.
Ki-67 is expressed in all active phases of the cell cycle (G1, S, G2, and M phases) and is a well-documented marker of cell proliferation. 4,5,24,38 The Ki-67 labeling index (LI), which is expressed as a percentage of Ki-67–positive cells, has been reported to be a better predictor of survival time and prognosis in humans than glioma histologic grade. 5 While it is not currently used to grade glial tumors, the Ki-67 LI may aid in the development of an improved method of grading gliomas in the future.
Gliomas represent 27% to 37% of canine primary intracranial tumors, and there is an increasing demand from pet owners to definitively treat dogs with these tumors. The increasing availability of veterinary stereotactic biopsy systems and the ability to achieve antemortem diagnosis of these tumors have also led to an increased need to identify molecular therapeutic targets and predictors of prognosis. 27,33,35 Given the popularity of EGFR as a therapeutic target in human glioma trials, the objectives of this study were to document EGFR expression in canine gliomas and to determine if its expression is associated with tumor type and histologic grade. Further objectives were to determine if the Ki-67 LI is associated with tumor grade and compare tumor proliferation with EGFR expression.
Materials and Methods
Tissue Samples and Pathologic Examination
A retrospective search was performed of the anatomic pathology database at the Veterinary Teaching Hospital, The University of Melbourne, Australia, for canine glial tumor specimens obtained at surgical biopsy or necropsy between 1978 and 2014. Glioma specimens retrieved from the archives included formalin-fixed, paraffin-embedded oligodendrogliomas, astrocytomas, oligoastrocytomas, and gliomatosis cerebri. Archival specimens of normal canine gray and white matter from the cerebral cortex, canine hyperplastic lymph node, and canine skin were included as control tissues.
Formalin-fixed, paraffin-embedded glioma specimens were sectioned at 3 μm and stained with hematoxylin-eosin. Glial fibrillary acidic protein immunohistochemical labeling was performed to verify the tumor cell phenotype (oligodendroglial vs astrocytic). Specimens were reviewed by board-certified pathologists, classified according to the World Health Organization histological classification of tumors of the nervous system of domestic animals, and the human equivalent World Health Organization (WHO) grade was applied (Suppl. Table S1). 18,19,40
Immunohistochemistry
Paraffin blocks were sectioned (3 μm thick) and mounted onto positively charged glass slides. Sections were deparaffinized in 3 changes of xylene and rehydrated in graded alcohol solutions. For antigen retrieval, sections were treated with preheated citrate buffer (pH 6) and heated in the microwave oven for 15 minutes (Ki-67) or proteinase K (Dako North America, Carpinteria, CA) at room temperature in a humidified chamber for 15 minutes (EGFR). Endogenous peroxidase activity was blocked by immersing sections in 3% hydrogen peroxide for 5 minutes at room temperature. Sections were blocked with 20% (Ki-67) or 50% (EGFR) fetal bovine serum (Gibco by Life Technologies, Carlsbad, CA) in phosphate-buffered solution for 60 minutes at room temperature and then incubated with the primary antibody. The Ki-67 sections were incubated for 60 minutes at room temperature with monoclonal mouse anti-human Ki-67 antigen, clone MIB-1 (Dako Denmark A/S, Glostrup, Denmark), diluted 1:5 with phosphate-buffered solution. For EGFR, sections were incubated for 60 minutes at room temperature with anti-EGFR 528 monoclonal antibody (EnGenIC Ltd, Lane Cove West, New South Wales, Australia), diluted 1:200 with phosphate-buffered solution. Immunohistochemistry was performed using Dako EnVision+ Dual Link System-HRP (Dako North America) for 30 minutes at room temperature. Immunoreactivity was visualized with substrate chromogen using the Vector NovaRED Substrate Kit (Vector Laboratories, Burlingame, CA) and counterstained with hematoxylin and lithium carbonate. Negative controls were run simultaneously excluding the primary antibody step. Positive control tissues included formalin-fixed, paraffin-embedded sections of canine hyperplastic lymph node for Ki-67 and canine skin for EGFR and were run in parallel with the tumor sections.
Slides were digitized and images viewed using Pannoramic Viewer version 1.15.4 software (3DHISTECH Ltd, Budapest, Hungary; http://www.3dhistech.com/pannoramic_viewer). For Ki-67, a minimum of 1000 nuclei were counted per specimen. The area assessed was selected from the region with the highest concentration of Ki-67–positive nuclei based on visual inspection of the entire section. Counting of nuclei was performed with ImageJ 1.48v software (National Institutes of Health, Bethesda, MD; http://imagej.nih.gov.ij). The Ki-67 LI was calculated by expressing the number of positive Ki-67 nuclei as a percentage of the total number of nuclei counted.
For EGFR analysis, sections were evaluated for both membrane and cytoplasmic immunoreactivity and scored using a previously described method and semi-quantitative score. 10 Briefly, specimens with less than 5% immunopositive cells were scored as negative, 6% to 25% immunopositive cells scored as 1+, 26% to 50% immunopositive cells scored as 2+, and 51% to 100% immunopositive cells scored as 3+. Sections were further evaluated for the distribution of immunoreactivity and recorded as multifocal or diffuse.
Statistical Analysis
EGFR immunopositivity score (0, 1+, 2+, 3+) and Ki-67 LI (0%–100%) were compared between tumor histologic types (oligodendroglioma, astrocytoma, oligoastrocytoma, and gliomatosis cerebri) using Kruskal-Wallis analyses. When a significant difference was evident, Mann-Whitney tests were performed for pairwise comparisons. For comparison of EGFR immunopositivity score and Ki-67 LI with tumor grade (II or III), the Mann-Whitney test was used. Statistical significance was defined as P < .05.
Spearman rank correlation was used to explore associations between the EGFR immunopositivity score and Ki-67 LI; the level of significance was set at P < .01. Analyses were performed using SPSS Statistics for Windows version 22.0 (SPSS, Inc, an IBM Company, Chicago, IL).
Results
Tissue Samples and Histopathology
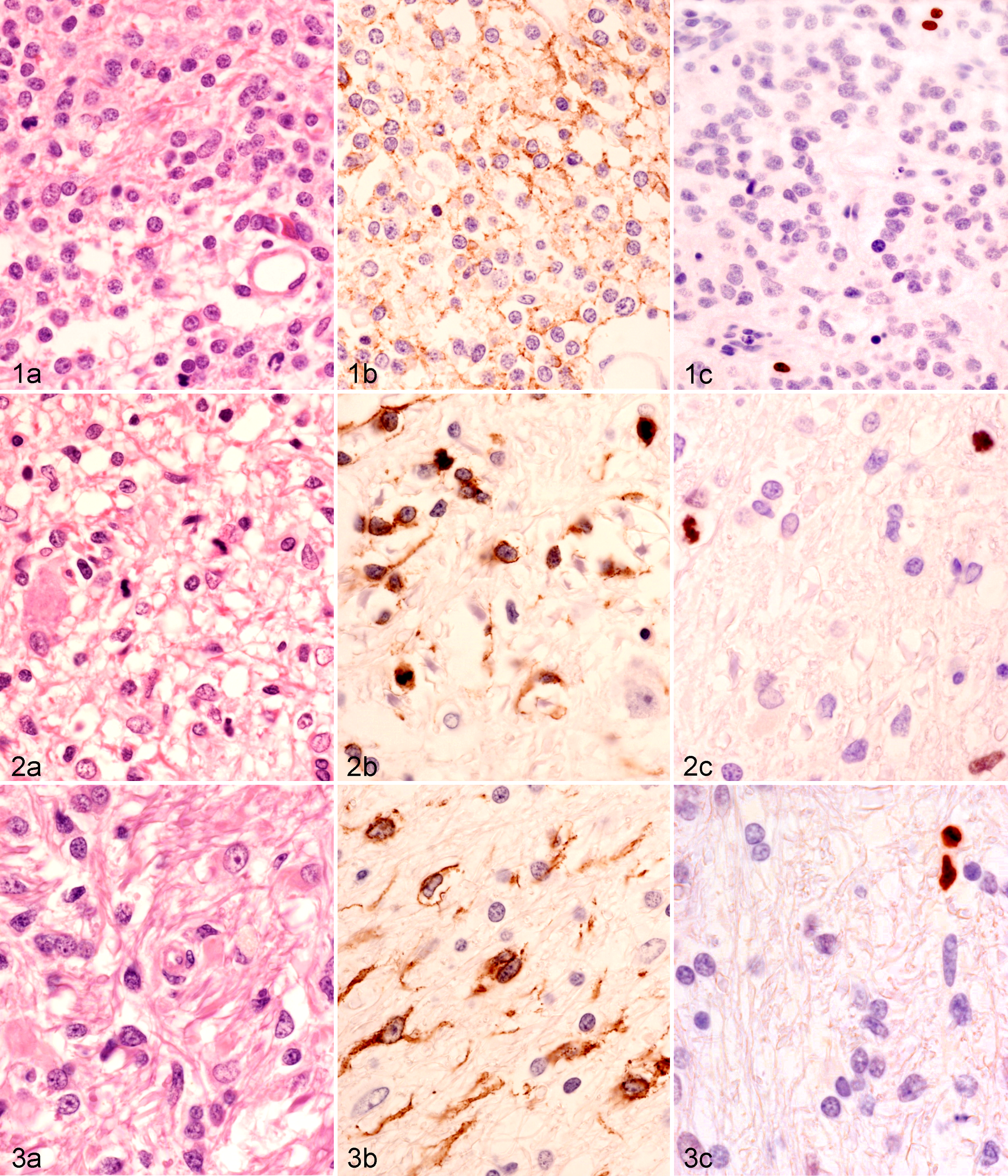
A total of 31 tumor specimens from 31 dogs of variable signalment (Suppl. Table S2) were analyzed. One specimen was obtained from surgical biopsy and 30 at necropsy. Twenty-nine tumors were intracranial and 2 were spinal (1 anaplastic oligodendroglioma and 1 anaplastic oligoastrocytoma). The tumor samples included 16 oligodendroglial tumors (9 oligodendrogliomas, 7 anaplastic oligodendrogliomas [Fig. 1a]), 7 astrocytomas (5 diffuse astrocytomas [Fig. 2a], 2 anaplastic astrocytomas), 3 oligoastrocytomas (2 oligoastrocytomas, 1 anaplastic oligoastrocytoma), and 5 gliomatosis cerebri (Fig. 3a).
One dog had 2 surgical biopsies obtained 286 days apart, followed by necropsy evaluation 357 days after the initial surgery; all of the tissue specimens were classified as oligodendroglioma. For the purposes of statistical analysis, only the necropsy specimen was included in the study as it was considered more representative of the tumor compared with the smaller biopsy specimens.
Immunohistochemistry
EGFR expression was identified in 16 of 31 (52%) tumors, and the immunopositivity scores varied across tumor histologic type (Suppl. Table S2 and Table 1). All positive tumors had immunolabeling of the cell membrane and, to a lesser extent, the cytoplasm (Figs. 1b, 2b, and 3b). The distribution of immunoreactivity was variable (Suppl. Table S2). Gliomatosis cerebri consistently had diffuse immunoreactivity. Tumors with an EGFR immunopositivity score of 1+ or 2+ typically had multifocal immunoreactivity, while those with a score of 3+ had more diffuse immunoreactivity. EGFR expression was significantly greater in gliomatosis cerebri (median EGFR immunopositivity score 3+) compared with oligodendroglioma (P = .002; median EGFR immunopositivity score falling between 0 and 1+), astrocytoma (P = .01; median immunopositivity score 0), and oligoastrocytoma (P = .04; median immunopositivity score 0). Expression of EGFR was significantly increased in high-grade (III) tumors compared with low-grade (II) tumors (P = .04).
Epidermal Growth Factor Receptor (EGFR) Expression Scores in 31 Canine Gliomas.a

EGFR, epidermal growth factor receptor; NA, insufficient sample size.
a P values are for the comparison between tumor grade and EGFR immunopositivity score.
Positive immunolabeling for Ki-67 was identified in 28 of 31 (90%) tumors (Suppl. Table S2 and Table 2) and was confined to the nucleus (Figs. 1c, 2c, and 3c) for all tumor specimens. There was marked variation in the Ki-67 LI across all tumor histologic types (Suppl. Table S2), with no statistical association between tumor histologic type and Ki-67 LI. The median Ki-67 LI was 2.3% (range, 0%–17.6%) for low-grade (II) tumors and 9.3% (range, 1.7%–41.0%) for high-grade (III) tumors (Table 2), and this difference was significant (P = .02).
Ki-67 LI Results for 31 Canine Gliomas.a
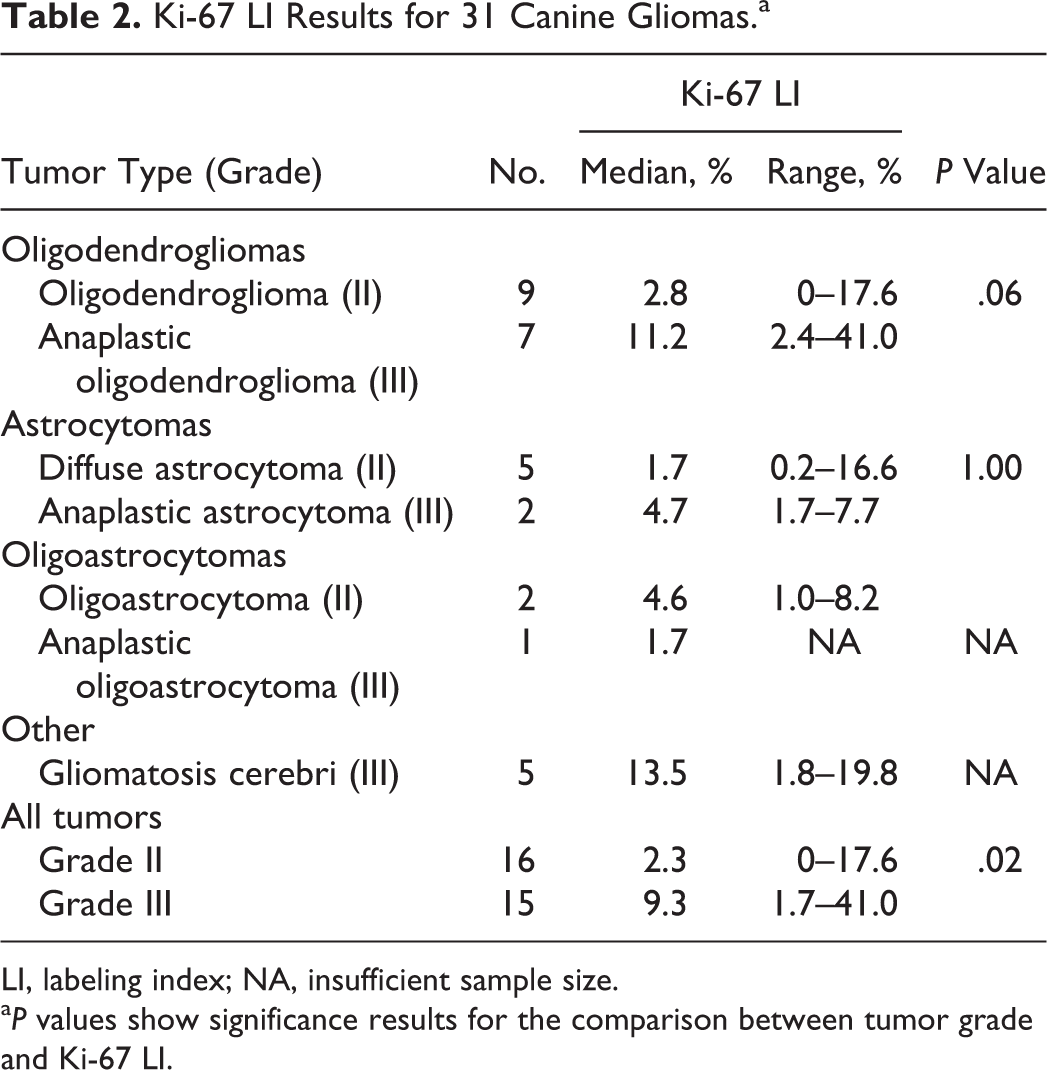
LI, labeling index; NA, insufficient sample size.
a P values show significance results for the comparison between tumor grade and Ki-67 LI.
There was a significant moderate correlation between EGFR immunopositivity score and the Ki-67 LI (r = 0.472, P = .007). For the 1 dog with tumor specimens obtained at different time intervals (days 0, 286, and 357), the EGFR immunopositivity score changed with time (0, 0, and 1+, respectively) as did the Ki-67 LI (3.7%, 18.5%, and 17.6%, respectively).
Discussion
In the present study, EGFR expression was demonstrated in 16 of 31 (52%) canine gliomas, with high-grade (III) gliomas having significantly greater EGFR expression compared with low-grade (II) gliomas. Furthermore, expression of EGFR was significantly greater in the gliomatosis cerebri group compared with the other tumor histologic types. The Ki-67 LI was significantly greater in grade III gliomas compared with grade II gliomas, and a significant moderate correlation was found between the EGFR immunopositivity score and the Ki-67 LI.
In humans, EGFR is expressed in a large portion of gliomas and is associated with glioma grade, with grade III and IV gliomas having a significantly higher frequency of EGFR immunopositivity than the lower grade tumors. 11,12,14,23 Furthermore, EGFR is the most commonly amplified gene, resulting in overexpression of this protein in glioblastoma multiforme, and is considered the most significant molecular marker for defining protein subtypes of gliomas. 2,17,26,30,36 Consequently, EGFR is a popular molecular target in human glioma therapeutic studies. 29
Previous immunohistochemistry studies have reported a combined total of 20% of canine gliomas investigated to be EGFR immunopositive, occurring most commonly in glioblastoma multiforme (11/25; 44%), followed by anaplastic astrocytoma (5/12; 42%), astrocytoma (4/20; 20%), anaplastic oligodendroglioma (1/38; 3%), oligodendroglioma (0/5), and gliomatosis cerebri (0/3). 10,13,20,36 While the percentage of EGFR-immunopositive canine astrocytomas appears to be less than that reported for humans, the data do follow a similar trend, with EGFR expressed more frequently in higher grade tumors. 11 This is contrary to the current study population where all (2/2) anaplastic astrocytomas were negative for EGFR and 3 of 5 (60%) astrocytomas were immunopositive. This conflicting result may be associated with the small sample size of astrocytomas in this series, particularly for the anaplastic astrocytoma group.
Previously, only 1 of 38 (3%) canine anaplastic oligodendrogliomas and 0 of 5 oligodendrogliomas have been reported immunopositive for EGFR. 10,13 In the current study, 8 of 16 (50%) oligodendrogliomas (5/7 anaplastic oligodendrogliomas and 3/9 oligodendrogliomas) were EGFR positive. 10,13 While this result is similar to the human findings where EGFR is expressed more frequently in higher grade gliomas, the overall frequency appears to be less. 11
Interestingly, 5 of 5 (100%) canine gliomatosis cerebri tumors were immunopositive for EGFR, and they all had an immunopositivity score of 3+. Consequently, gliomatosis cerebri is significantly more likely to express EGFR compared with all other glioma histologic types. Therefore, EGFR targeted therapy may be more effective in this group of canine tumors compared with other glial tumors, which do not reliably express EGFR or have a smaller percentage of EGFR-expressing cells.
Investigation of EGFR-1 in a series of 43 canine gliomas, using quantitative real-time polymerase chain reaction, revealed EGFR amplification in 19 of 23 (83%) astrocytomas and 20 of 20 (100%) oligodendrogliomas. 8 Amplification was greatest in the high-grade gliomas, including anaplastic oligodendroglioma and glioblastoma multiforme. 8 The disagreement between the polymerase chain reaction and immunohistochemical results in dogs has been suggested to be a result of posttranscriptional regulation of EGFR. 2 Conversely, in human studies, the immunohistochemical results for EGFR expression reflect the molecular genetic results and therefore are considered the most reliable assay for determining EGFR expression. 6,11,26,30
While immunohistochemistry is the most reliable means of assessing EGFR expression in tissue specimens, there is a lack of standardization with regard to the reagents used, the laboratory technique employed, and the assessment of the stained section across studies. 6 The variation in EGFR immunopositivity results between our study and previous canine glioma studies may be associated with the use of varied reagents, including differing antibodies and the laboratory technique employed. Previous studies have used mouse monoclonal EGFR antibody and rabbit polyclonal EGFR antibody. 10,13,20,36 In the current study, the antibody used was a mouse monoclonal antibody, which is known to cross-react with canine EGFR. The affinity of this and the other anti-EGFR antibodies for the canine receptor may vary, particularly if raised against human proteins. 10,13,36 Finally, the use of core samples for tissue microarray immunohistochemical analysis in previous studies may have given false-negative results if EGFR expression in canine gliomas has a multifocal rather than a diffuse distribution, as was seen in some of the specimens included in our study. 10 Certainly, the possibility of false negatives or falsely low immunoreactivity has been discussed in human reports due to the heterogeneous expression of EGFR. 6,14
In humans, the Ki-67 LI has been identified to correlate with increasing glioma histologic grade, but an overlap remains, with some high-grade tumors having a low Ki-67 LI and vice versa. 5,12,14,32 These findings are consistent with the results of the current study. Previous canine studies also report the Ki-67 LI to be associated with tumor grade; an overlap in the Ki-67 LI and tumor histologic grade, however, has not been previously reported. 13,21 The reason for the variation between these results is not known. It may be associated with the smaller sample size in the previous reports: 12 gliomas reported in one study and 22 in the other. 13,21 The Ki-67 LI results in our study more closely correlate with those of the Ki-67 LI in a series of 267 human gliomas (Suppl. Table S1). 32
In a meta-analysis of human gliomas, Ki-67 overexpression predicted poor progression-free survival and poor overall survival. 4 The relationship of the Ki-67 LI to prognosis, histologic grade, and aggressiveness has been investigated in canine mast cell tumors, lymphoma, and mammary tumors, among others. 16,28,34,41 To date, investigation of the Ki-67 LI as a predictor of outcome or survival in canine gliomas has not been undertaken. While the Ki-67 LI was documented in the current series of canine gliomas, incomplete clinical data prevented the investigation of its use as a predictor of survival. Further clinical research is therefore required in dogs to determine if the Ki-67 LI has a similar predictive value for outcome.
The Ki-67 LI and EGFR immunopositivity of human gliomas are significantly correlated, with EGFR-positive astrocytomas having a significantly higher mean Ki-67 LI compared with EGFR-negative tumors. 14 These results are consistent with those in our series of dogs where there was a significant moderate correlation between EGFR immunopositivity score and the Ki-67 LI. This result, however, is not overly surprising given the role EGFR plays in cell proliferation.
For the 1 dog that had 2 surgical biopsies followed by necropsy evaluation over a 12-month period, the EGFR immunopositivity score changed from being negative at the time of the 2 surgical biopsy procedures to a score of 1+ at necropsy. The Ki-67 LI also increased with time from 3.7% to 17.6%. This may indicate malignant transformation to an anaplastic tumor. Alternatively, the surgical biopsies, being smaller tissue samples compared with the necropsy sample, may not have been representative of the tumor.
Limitations of this report include the retrospective nature of the study and those inherent to immunohistochemistry, including determination of immunopositive cells, sampling and counting error, and the limitations specific to the EGFR and Ki-67 immunohistochemical techniques. 32 Furthermore, while 31 glioma tumors were included in the study, the sample size remains a limiting factor, particularly for the oligoastrocytoma group.
In summary, the role of EGFR in driving oncogenesis in canine gliomas may be less significant compared with human gliomas, with EGFR being expressed in only 52% of canine gliomas. Consequently, EGFR may only be a suitable therapeutic target in some canine gliomas, particularly gliomatosis cerebri, where expression was significantly greater compared with the other histologic tumor types. Investigation of other potential therapeutic targets that occur more frequently in gliomas requires consideration. The Ki-67 LI can be used to document tumor cell proliferation. However, further investigation is required to determine if the Ki-67 LI and presence of EGFR immunopositivity can be used in the development of a tumor grading system based on genetic events and biologic behavior, as well as act as predictors of prognosis.
Footnotes
Acknowledgements
We thank EnGenIC Ltd, Lane Cove, Australia, for supplying the EGFR antibody. We also thank Professor Brian Summers and Dr Andrew Stent for their contribution reviewing histopathological slides, Paul Benham for his assistance with the immunohistochemical labeling, and Andrew Woodward for his statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.