
Abstract
A 2-tiered histologic grading scheme for canine cutaneous mast cell tumors (MCTs) is based on morphologic characteristics of neoplastic cells, including karyomegaly, multinucleation, nuclear pleomorphism, and mitotic figures. Aspirates from MCTs may provide the same information more quickly, inexpensively, and less invasively. This study used these criteria to develop a cytologic grading scheme for canine MCTs to predict outcome. Three anatomic pathologists graded histologic samples from 152 canine MCTs. Three clinical pathologists evaluated aspirates from these masses using similar criteria. A cytologic grading scheme was created based on correlation with histologic grade and evaluated with a kappa statistic. Survival was evaluated with Kaplan-Meier survival curves. Cox proportional hazards regression was used to estimate hazard ratios for tumor grades and individual grading components. Simple logistic regression tested for relationships between risk factors and mortality. The cytologic grading scheme that best correlated with histology (kappa = 0.725 ± 0.085) classified a tumor as high grade if it was poorly granulated or had at least 2 of 4 findings: mitotic figures, binucleated or multinucleated cells, nuclear pleomorphism, or >50% anisokaryosis. The cytologic grading scheme had 88% sensitivity and 94% specificity relative to histologic grading. Dogs with histologic and cytologic high grade MCTs were 39 times and 25 times more likely to die within the 2-year follow-up period, respectively, than dogs with low grade MCTs. High tumor grade was associated with increased probability of additional tumors or tumor regrowth. This study concluded that cytologic grade is a useful predictor for treatment planning and prognostication.
Mast cell tumors (MCTs) are common cutaneous neoplasms in dogs, accounting for up to 21% of all canine skin tumors. 13 Biological behavior is predicted with clinical staging and histologic grading, with variable success. Although 3 histologic grading schemes exist, 2 are utilized commonly: the Patnaik system and the newer 2-tier system (Kiupel system). 4,8
The Patnaik system is a 3-tiered histologic grading scheme in which cellularity, cell morphology, mitotic index, extent of tissue involvement, and stromal reaction are assessed to assign a histologic grade of I to III, from well differentiated to poorly differentiated, respectively. 8 With this grading system, grade I tumors are generally associated with an excellent prognosis and are usually cured by complete surgical excision exclusively. Grade III tumors are predicted to be more biologically aggressive, with greater risk of invasion and distant metastasis and often require adjunct chemotherapy along with surgical removal. Grade II MCTs are overrepresented compared to grade I and grade III neoplasms, and their behavior is difficult to predict. 9 While most grade II MCTs are cured with surgical resection, between 5 and 22% of these tumors metastasize. 1 The variability in the behavior of the grade II tumors is problematic for oncologists deciding on treatment modalities and undermines the usefulness of this grading scheme. In addition, there is wide interobserver variability (only 62.1% agreement) when utilizing the Patnaik grading criteria. 7
The newer Kiupel system is a 2-tiered histologic grading scheme developed both to eliminate the nebulous Patnaik grade II category and to allow for improved interobserver variation. This system considers the presence of karyomegaly (defined as ≥2-fold variation in nuclear diameters in ≥10% of neoplastic cells), ≥7 mitotic figures per 10 high power fields (HPFs), ≥3 multinucleated cells per 10 HPF, and ≥3 bizarre nuclei in 10 HPF. 4 If any of these findings are present, the neoplasm is considered high grade, while MCTs lacking all of these findings are low grade. While no grading system is associated with 100% accuracy in predicting biological behavior, this 2-tiered system has high prognostic value and minimal interobserver variability (up to 96.8% agreement). 4,9
The criteria used for MCT grading in the 2-tier system (karyomegaly, number of mitotic figures, multinucleation, and bizarre nuclei) are all features that are easily identified with cytology, suggesting that a cytologic grading scheme for MCTs in dogs may be useful. The use of cytologic grading could help plan treatment and potentially provide valuable prognostic information prior to surgical intervention.
To the authors’ knowledge, only 1 published study has compared cytologic and histologic features using the 2-tiered histologic grading scheme as a gold standard. 10 In that study, histologic grade was correctly predicted in as many as 94% of cytology cases. However, the study did not investigate patient survival and applied the histologic criteria directly rather than create a unique cytologic grading system. 10 The purpose of this prospective, multi-institutional study was to use the 2-tier grading criteria as a guide to develop an accurate and reproducible cytologic grading scheme for MCTs that is predictive of patient outcome.
Materials and Methods
Sample Acquisition
Paired cytologic and histologic specimens from canine cutaneous MCTs submitted for routine analysis from November 2012 through December 2014 to the Georgia Veterinary Diagnostic Laboratories and the University of Georgia College of Veterinary Medicine Teaching Hospital were used in this study. Canine MCTs were included if a surgical biopsy was submitted within 8 weeks of the cytologic diagnosis of an aspirate. Cases were excluded if the cytologic sample had fewer than 100 intact mast cells. A total of 152 paired samples were included. Aspirates were processed routinely, stained with a modified Wright’s stain in a commercial stainer (Aerospray Hematology Slide Stainer, Wescor Inc, Logan, UT). Histologic samples were fixed in 10% neutral buffered formalin, embedded in paraffin, sectioned at 3 µm, and stained routinely with hematoxylin and eosin.
Sample Grading
All histologic slides from the original biopsy submission were reviewed by 1 pathologist (PMK), and additional sections were prepared from a representative block for inclusion in this study. All histologic sections were reviewed by 3 board-certified anatomic pathologists (EAD, MRI, JWK) without knowledge of the prior cytologic or histologic findings and graded using both the Patnaik and 2-tier histologic grading schemes. 4,9 Additional evaluation criteria included the presence or absence of greater than 25% eosinophils (as a percentage of the total cells) and necrosis affecting more than 10% of the tissue, and the width of margins. Margins were incomplete if the tumor extended to a margin, narrow if any margin was less than 2 mm, and wide if all margins were 2 mm or greater.
All cytologic specimens were blindly reviewed by 3 board-certified clinical pathologists (MSC, HLP, PMR). One entire adequately cellular cytology slide was evaluated for cell granularity, nuclear pleomorphism, collagen fibrils, mitotic figures, binucleation or multinucleation, and anisokaryosis. Granularity was scored as well granulated, poorly granulated, or mixed granulation (a mix of poorly granulated and well granulated cells). Nuclear pleomorphism was scored as present if nonrounded nuclear shapes were present, and absent if only round to ovoid shapes were noted. Collagen fibrils, mitotic figures, and binucleate or multinucleated cells were scored as present or absent. Anisokaryosis was defined as >50% variation in nuclear size.
Patient Outcomes
Submitting veterinarians were surveyed regarding patient outcomes including treatment modalities, recurrence of the original tumor, occurrence of tumors at other locations, current status (living or deceased), and cause of death if the animal was deceased. Outcomes were unavailable for 13 patients, and these were excluded from the prognostic analysis but were retained for the analyses correlating histologic and cytologic grades.
Development of the Grading Scheme and Statistical Analysis
All statistical analyses were performed in SAS v9.2 (Cary, NC). The median grade for histologic 2-tier and Patnaik grades were used for all analyses. Margins and Patnaik grade were analyzed as class variables.
A cytologic 2-tier grading scheme was created using forward stepwise discriminant analysis using the 2-tier histologic grade as the gold standard with samples where full 2 year survival was available. Analysis of variance (ANOVA) results were used to include or exclude cytologic parameters that were significantly associated with longer survival. Parameters with statistically significant P values (P > .05) were combined in various algorithms and these combinations evaluated for agreement with histologic grade using a kappa statistic. For each proposed cytologic grading scheme, the cytologic 2-tier score was calculated independently for each clinical pathologist, and the median result was compared to the median histologic 2-tier score. The median calculated cytologic grade for each tumor, using the proposed cytology grading scheme, was then used for further survival analysis.
Consistency among clinical pathologists and among anatomic pathologists was evaluated with the Cronbach’s alpha test. For anatomic pathologists, consistency for both the Patnaik and 2-tier grading scheme were calculated.
Kaplan-Meier survival curves for survival time were constructed to calculate median survival for all dogs. Dogs were considered censored in the survival analysis if alive at least 2 years after diagnosis, if they were lost-to-follow-up, or if their death was not tumor-related. A log-rank test was used to test if there was a difference in survival probability due to morphologic risk factors.
Cox proportional hazards regression was used to test for relationships of risk factors to 2-year survival probability and estimate hazard ratios. Multiple Cox proportional hazards regression was used to evaluate the relationship of various factors to survival probability individually and together. Factors included patient age, margins, the 4 subcomponents of the 2-tier histologic grade (mitotic figures, multinucleation, bizarre nuclei, and karyomegaly) and the 6 subcomponents of the median calculated cytologic grade (granularity, mitotic figures, binucleation, multinucleation, nuclear pleomorphism, and anisokaryosis). All risk factors were included initially included in the model with both histology and cytology subcomponents and a stepwise selection procedure was used to select risk factors in the final model. Cox proportional hazards regression was also used to compare 2-tier histological grade and surgical margins to survival probability and estimate hazard ratios.
Simple logistic regression was performed to test for relationships between risk factors and the probability of mortality. If quasi-separation of variables occurred, Firth’s penalized maximum likelihood estimation method was used to reduce bias in logistic model parameter estimation.
Whether a dog developed another MCT, referred to as the additional tumor rate, was evaluated with an odds ratio for the 2-tier histologic grade and calculated cytologic grade. All hypothesis tests were 2-sided and the significance level was α = .05.
Results
A total of 152 MCTs from 150 dogs were included in the overall study. The signalment and tumor grading details are provided in Supplemental Table 1. There were 10 intact females, 86 spayed females, 10 intact males, and 44 neutered males. The average age was 7.9 years(standard deviation: 2.9 years, range: to 17 years). Breeds with more than 2 dogs in the study included Labrador retrievers (n = 36), mixed breed dogs (n = 13), American bulldogs (n = 10), Golden retrievers (n = 9), boxers (n = 8), beagles (n = 7), pit bull/Staffordshire terriers (n = 6), pugs (n = 5), Boston terriers (n = 4), and Chihuahuas (n = 3), with a total of 40 breeds represented.
Tumor grading with the Patnaik system revealed 12 (7.9%) grade 1, 130 (85.5%) grade 2, and 10 (6.6%) grade 3 tumors. Using the 2-tier grading system, there were 135 (88.8%) low grade, and 17 (11.2%) high grade tumors. Application of the criterion for ‘bizarre nuclei’ in the 2-tier system are shown in Supplemental Figs. 1–4.
Selected cytologic grading criteria are presented in Figs. 1–4. The cytologic characteristic most associated with 2-year survival was granularity (R 2 = .40, P < .001), followed by anisokaryosis (R 2 = .27, P < .001), multinucleated cells (R 2 = .21, P < .001), binucleated cells (R 2 = .21, P < .001), and mitotic figures (R 2 = .16, P < .001). Bizarre nuclei/nuclear pleomorphism had a low correlation (R 2 = .06, P < .002), as did the presence of collagen fibrils (R 2 = .07, P < .001). Using this information, 9 algorithms for cytologic evaluation of aspirates were created and evaluated for agreement with the histologic grade of corresponding biopsies using a kappa statistic.
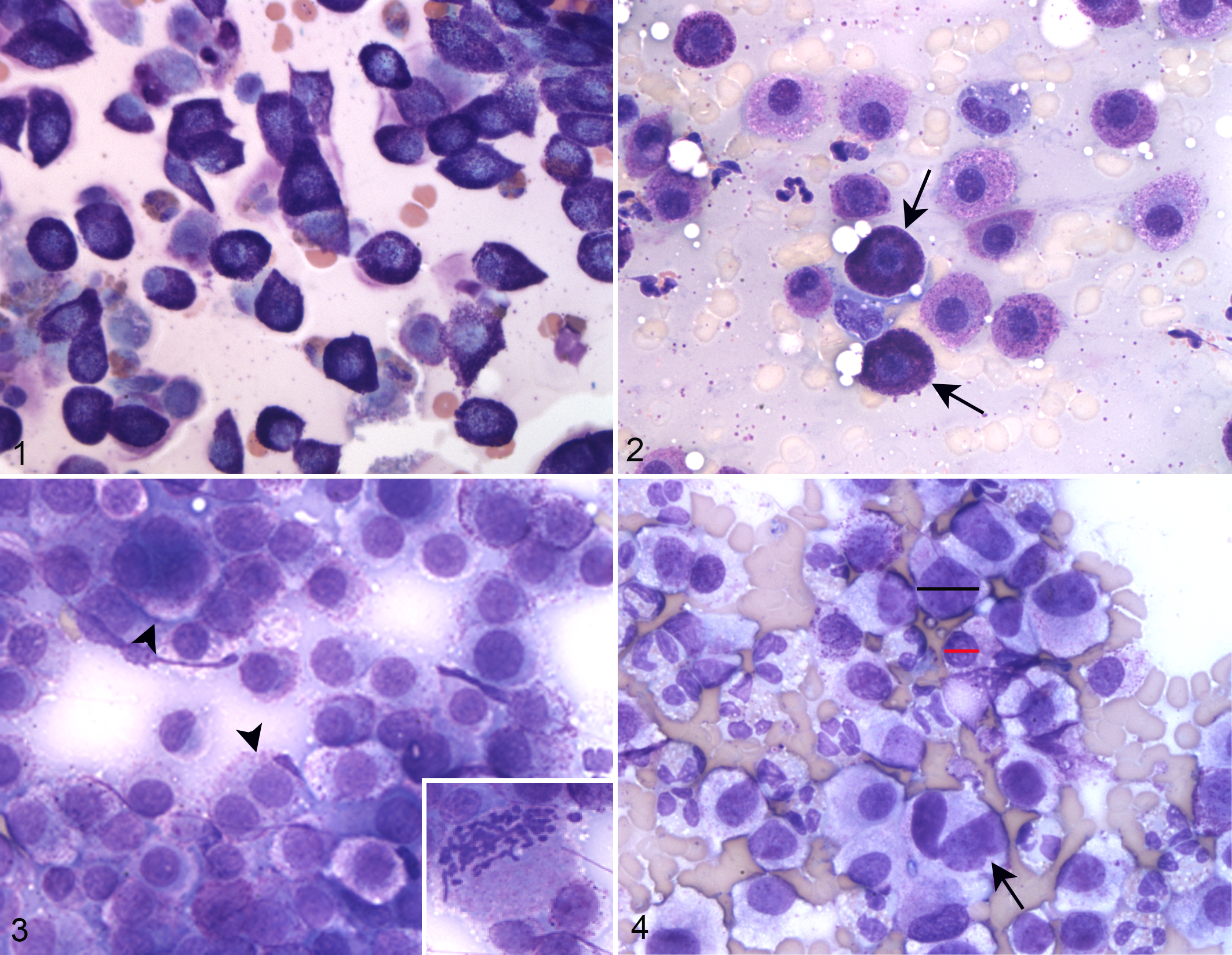
Mast cell tumors, skin, dog. Modified Wright’s stain.
The cytologic algorithm that most closely correlated with histologic grade, with a kappa score of 0.736, classified a tumor as high grade if it was (1) poorly granular or (2) had at least 2 of the following 4 features: presence of any mitotic figures, anisokaryosis, binucleation or multinucleation, or nuclear pleomorphism, as presented in Fig. 5. The 2 × 2 agreement table and corresponding calculated contingencies are presented in Table 1. Overall, cytology had a high specificity, with a high negative likelihood ratio (likelihood that a tumor classified as low grade truly is low grade). Approximately a third (31.8%) of tumors were false positives (ie, cytologically high grade but histologic low grade), while very few (1.6%) were false negatives (ie, cytologic low grade but histologic high grade).
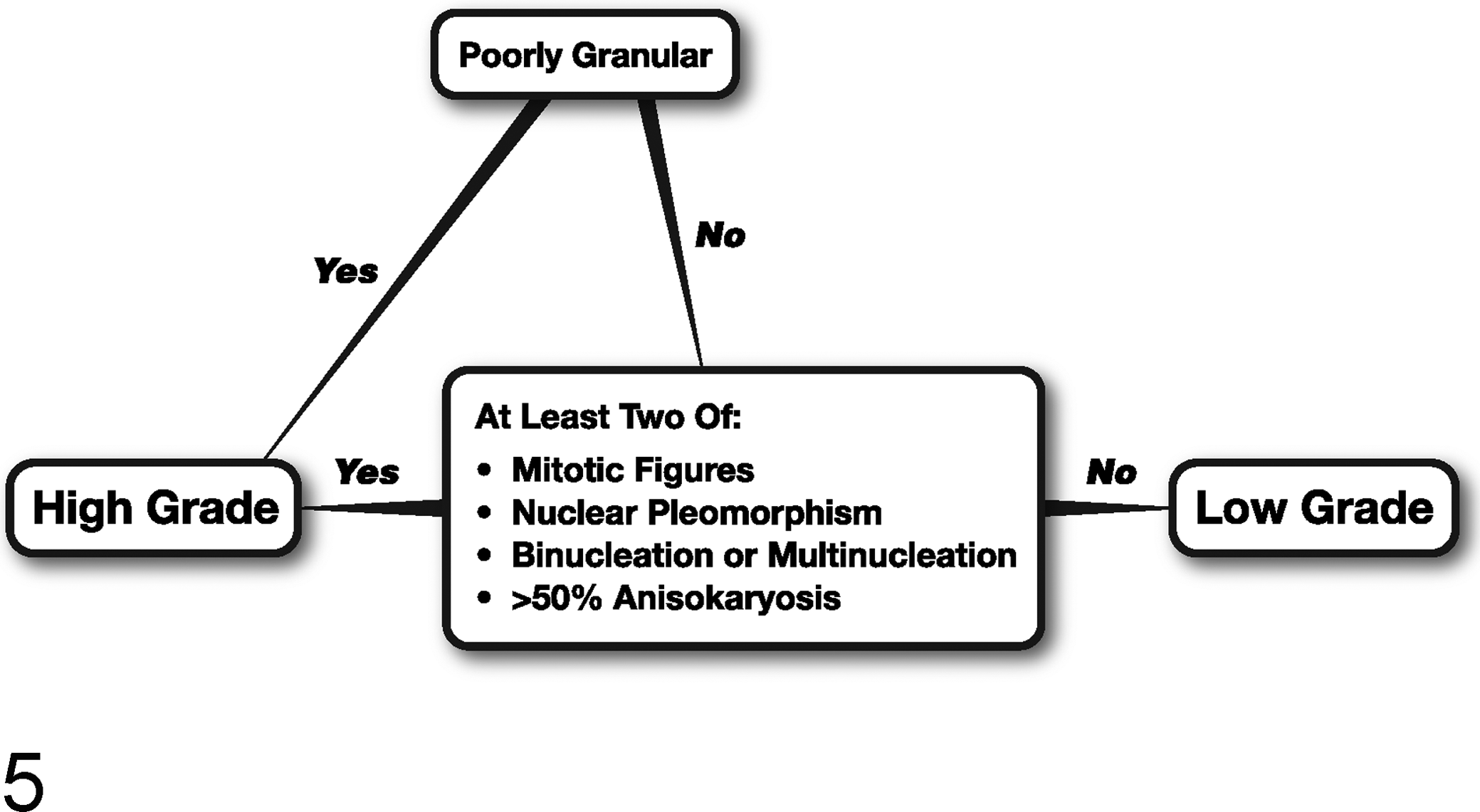
Algorithm for rapid application of the cytologic grading scheme for canine cutaneous mast cell tumors.
Contingency 2 × 2 Table for Proposed Cytologic Grading System in Canine Cutaneous Mast Cell Tumors Using the 2-Tier Histologic Grading System as the Gold Standard.
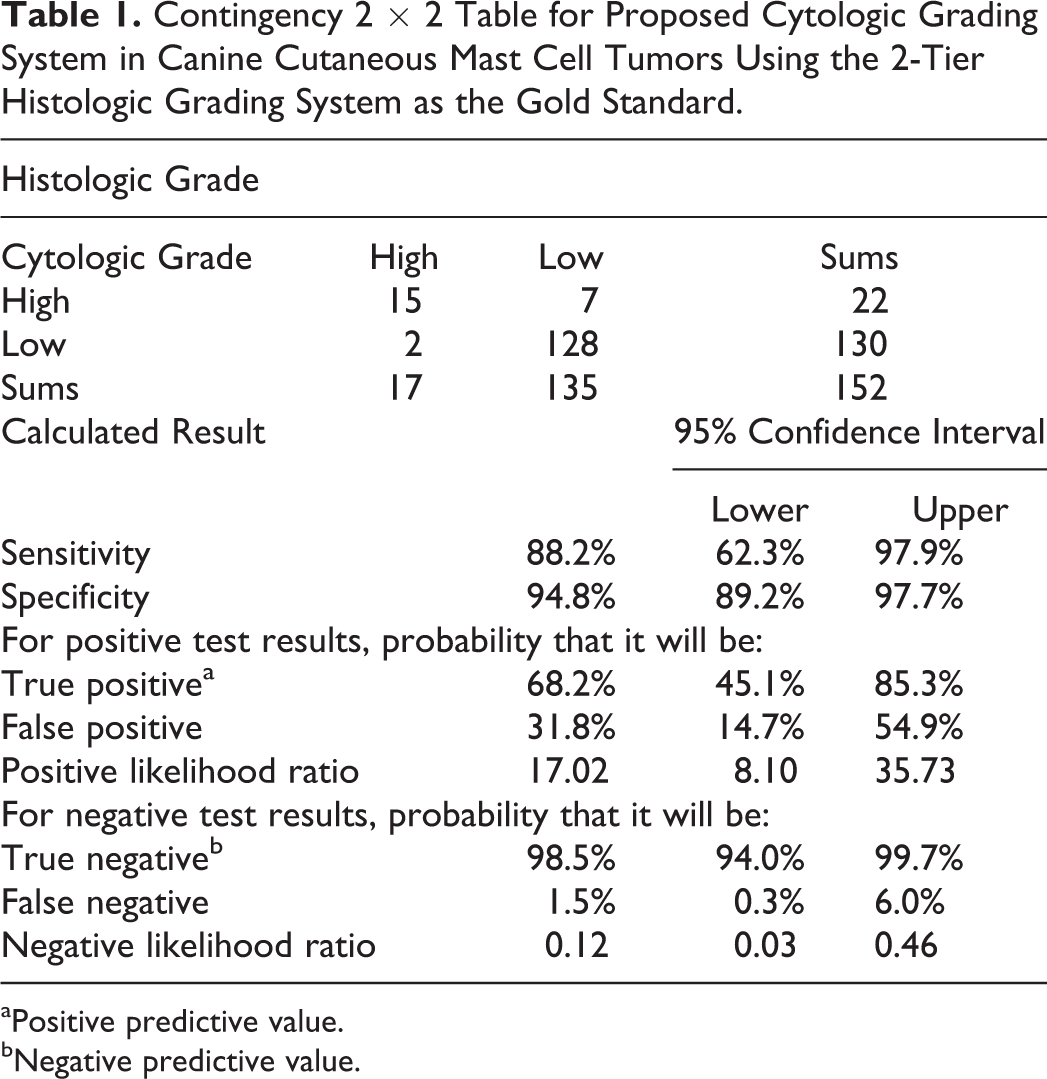
aPositive predictive value.
bNegative predictive value.
Overall consistency among histopathologists using the 2-tier grading system was 77.0% while overall consistency using the Patnaik system was 72.9%. With the 2-tier system, there was complete agreement on 107 of 135 (79.3%) histologic low grade tumors (79.3%) and on 13 of 17 (76.5%) histologic high grade tumors. Consistency among clinical pathologists for the newly proposed cytology grading system was 75.5%, with complete agreement on grade between clinical pathologists for 95 of 129 (73.6%) low grade tumors and 18 of 22 (81.8%) high grade tumors.
Mean survival for each risk factor with associated median survival times and P values are presented in Table 2. Kaplan-Meier survival curves for the 2-tier histological grade and calculated cytology grade are presented in Figs. 6 and 7, while those for the Patnaik grade and margins are presented in Supplemental Figs. 5 and 6. Histologic and cytologic high grade tumors were each associated with significantly decreased probability of survival (Table 2). A Patnaik grade of 3 significantly decreased survival probability compared to a Patnaik grade of 1 (P < .0001) or 2 (P < .0001). Incomplete margins were associated with significantly decreased survival compared to wide margins (P = .0133).
Associated Mean Survival Times for Cytologic and Histologic Grades.
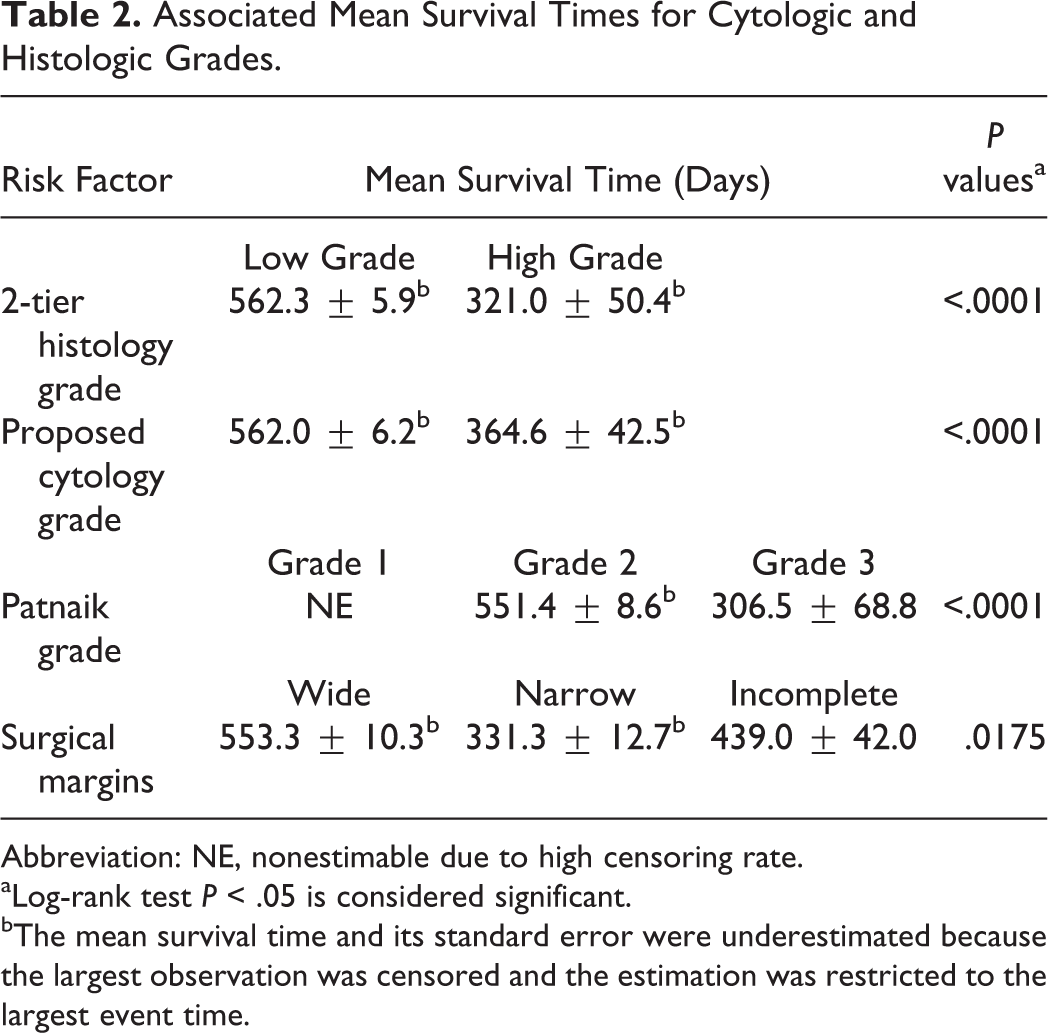
Abbreviation: NE, nonestimable due to high censoring rate.
aLog-rank test P < .05 is considered significant.
bThe mean survival time and its standard error were underestimated because the largest observation was censored and the estimation was restricted to the largest event time.
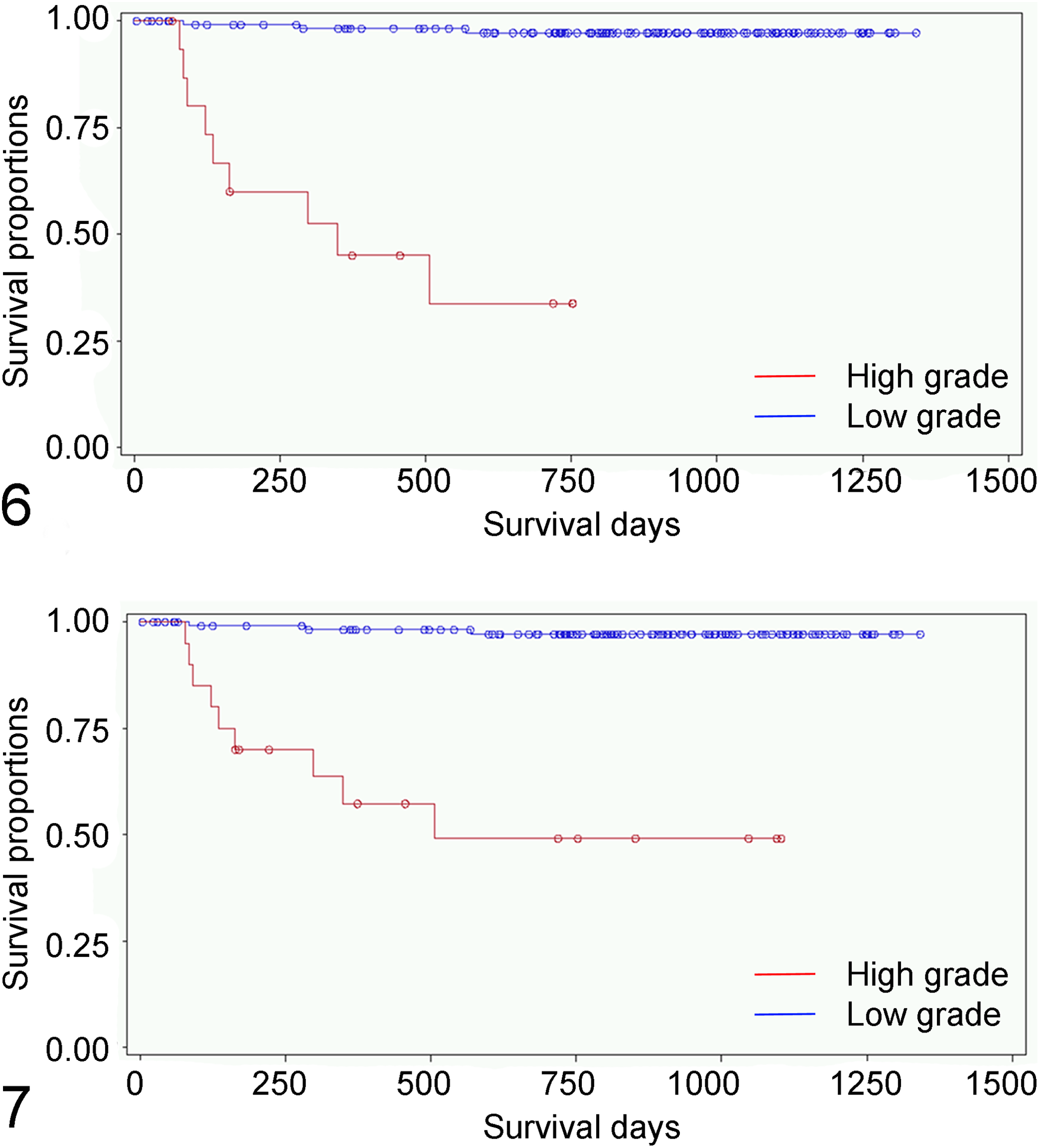
Kaplan-Meier curves demonstrating survival probability for canine cutaneous mast cell tumors with 2-tier histologic grade (Fig. 6) and with calculated cytologic grade (Fig. 7).
Hazard ratios and associated P values from the Cox proportional hazards regression are shown in Table 3, and results are consistent with the Kaplan- Meier survival analysis. The hazard ratio indicates the odds of the measured event, such as death or tumor recurrence, if a given condition, such as a high grade tumor, is present. Dogs with a histologic high grade MCT were 38 times more likely to die than dogs with a low grade MCT. Similarly, dogs with a cytologic high grade MCT were 25 times more likely to die than dogs with a low grade MCT. Dogs with a Patnaik grade 3 MCT were 20.5 times more likely to die than dogs with a grade 2 MCT, while dogs with Patnaik grade 2 MCT were 20.5 times more likely to die than dogs with a grade 1 MCT. Dogs with an incompletely excised MCT were 2.5 times more likely to die than dogs with a narrowly excised MCT. Dogs with a narrowly excised MCT were 2.5 times more likely to die than dogs with a more completely excised MCT. As surgical margins may be more difficult to achieve in high grade tumors and may not independently affect survival, 11 a Cox proportional hazards regression was performed, and yielded a result of 2.4 (CI 1.2–4.7) with P = .0125, confirming surgical margins as an independent prognostic factor for survival as shown in Supplemental Fig. 6.
Hazard Ratios and Associated P values for Risk Factors From Cox Proportional Hazards Regression.
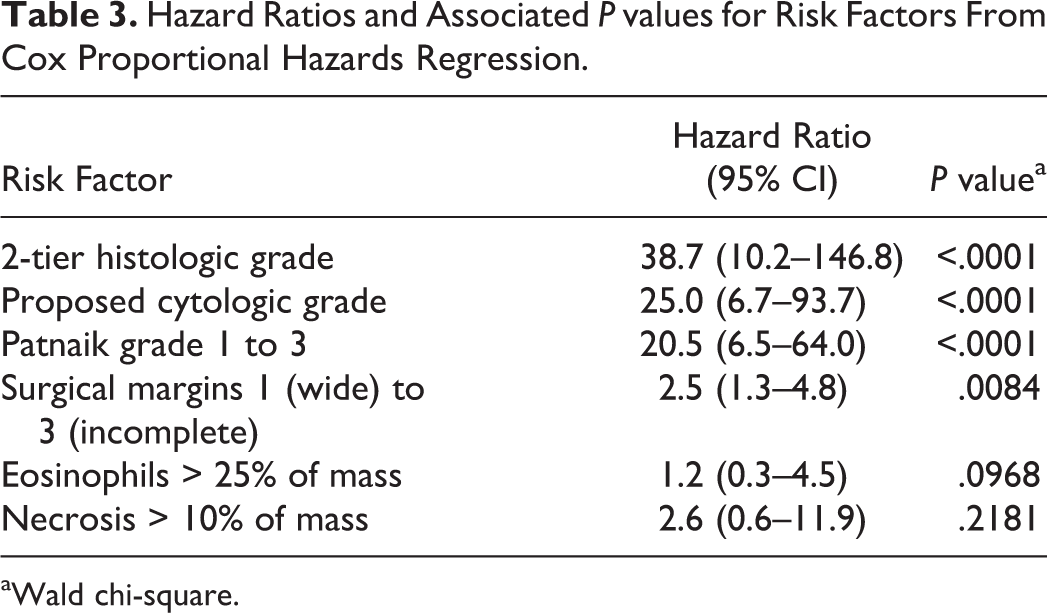
aWald chi-square.
Survival hazard ratios for the subcomponents of the histology 2-tier grading system, the proposed cytology grading system, and the combination of both are shown in Supplemental Tables 2–4. Wide surgical margins were important survival characteristics in all models. Cytologic subcomponents that were significantly associated with survival included granularity, mitotic figures, and multinucleation (with hazard ratios of 5.2, 37.6, and 6.7, respectively; Supplemental Table 3). Within the histologic subcomponents, only mitotic figures correlated with survival with a hazard ratio of 36.0 (CI 7.2–179.6) (Supplemental Table 2). When subcomponents of both cytologic and histologic grading criteria are included in a survival model, only histologic determination of mitotic figures and the cytologic determination of multinucleated cells were still significant (Supplemental Table 4).
Tumor grade was associated with increased probability of additional tumors or recurrence of the primary tumor (Supplemental Tables 5 and 6). The probability of developing additional tumors was 37.5% for cases with high histologic compared to 8.9% for those with low histologic grade. This difference was significant (OR 6.1 [CI 1.9–20.0], P = .0028; Supplemental Table 5). Similarly, the probability of developing additional tumors was 35.0% for cases with high cytologic grade compared to 8,4% for those with low cytologic grade. This difference was significant (OR 5.9 [CI 91.9–18.1], P = .0020; Supplemental Table 6).
Discussion
This study found that cytology was useful for predicting the behavior of canine cutaneous MCTs, when adequately cellular samples were evaluated. In the proposed cytologic grading scheme, MCT were considered high grade if poor granulation was identified, or if there were 2 of the following 4 cytologic features: presence of any mitotic figures, anisokaryosis >50%, binucleation or multinucleation, or nuclear pleomorphism. This proposed cytologic grading scheme was found to be predictive of survival and correlated well with the 2-tier histologic grading system. Cytologic evaluation is typically performed prior to histopathology, and as such can be considered a screening test. This grading system could be used at no additional expense or trauma to the patient beyond that already used for diagnosis, and the results may help an owner and surgeon to create an individualized treatment plan.
More MCTs were found to be high grade by cytology than by histology. While a higher false positive rate on cytology than histology is not ideal, it is preferable for a screening test to have low false negatives so that high grade tumors requiring more aggressive treatment are unlikely to be missed. The consequences of a false positive could result in more aggressive surgery than is necessary or, in a worst case scenario, euthanasia, while a false negative may allow an aggressive tumor to go untreated.
Nuclear pleomorphism was the least useful cytological feature for prediction of survival. It also had relatively low correlation with histologic grade, as previously reported. 10 This may not be a useful feature of malignancy on cytology as cells are flattened during preparation and histological features such as lobulation and indentation may not be maintained. On histology, nuclei are viewed as a cross-section of a 3-dimensional shape. Conversely, binucleation or multinucleation may be more readily visible on cytology for the same reason, as a 2-dimensional plane of a 3-dimensional cell could miss nuclei stacked perpendicular to the section plane of the tissue. Binucleation is not a criterion used in the histological 2-tier grade. However, a high correlation between binucleation and multinucleation has been documented. High numbers of binucleated cells increase the probability that multinucleated cells are also present on cytology. 10
The presence of significant numbers of eosinophils and necrosis, detected by histology, were not indicators of survival. The presence of collagen fibrils on cytologic samples also failed to correlate with survival. Though not currently used to evaluate prognosis, it is helpful to confirm (at least in this population of tumors) that these were not important features to evaluate. Samples that are too necrotic for grading may have a worse prognosis, or should not be graded at all, but were not included or evaluated separately in this study. Age was a significant risk factor inversely proportional to survival, but this is expected as older dogs may be at increased risk for euthanasia, and they also have less of their potential natural lifespan remaining.
Surgical margins were an important risk factor for survival in all models. Previous studies have not always found that wide surgical margins are more likely to result in prolonged survival in high grade tumors. 2 However, this is difficult to evaluate completely as margin width is not always specifically addressed. 4 Wider surgical margins may be easier to achieve with low grade tumors, as these may have more distinct margins. In addition, less complete excision may leave residual tumor that has the potential to transform into an aggressive phenotype. As such, surgeons should ensure that excisional margins are as wide as possible with all canine MCTs, especially those found on cytology to be high grade.
The odds ratio for development of additional tumors or recurrence of the primary tumor was higher for both histologic and cytologic high grade tumors, consistent with previous studies. 2 Recurrence of a tumor has also been reported to be unrelated to tumor margins 15 but there were insufficient incidences of local recurrence of a tumor in this study to evaluate this possibility.
This study found a similar proportion of high grade tumors using the 2-tiered grading system (11%) as previously reported (10.5%), though agreement between pathologists was lower in our study. This was possibly due to using only 3 examiners per tumor, where the tendency of any single reviewer to over-grade or under-grade would have significant impact. The lack of practice using an established cytological grading system may also have negatively impacted agreement between clinical pathologists. As seen in previous reports, this study found a high proportion of grade 2 tumors using the Patnaik system and a lower agreement between pathologists using this grading scheme compared with the others tested. 7 In fact, overall interobserver agreement in our study was highest using the calculated cytologic grading system.
Conclusions
We proposed a cytologic grading system in which MCT are considered high grade if there is either poor granulation or 2 of the other 4 features (presence of any mitotic figures, nuclear pleomorphism, binucleation or multinucleation, or marked anisokaryosis [>50% variation in nuclear size]), as illustrated in Fig. 5. This cytologic grading system correlated well with both survival and with the histologic grading system. Cytologically low grade tumors have prolonged survival and are very unlikely to be histologically high grade. Not only tumor grade but also clinical staging has been significant in predicting patient survival. 12 External verification of the proposed cytologic grading scheme along with further investigations into how clinical staging, other MCT markers such as CD25, 5,6 interleukin-2 receptor, 5 c-kit mutations, 3 and proliferation markers such as AgNOR and Ki67 14 complement cytologic and histologic grades may add additional prognostic information.
Footnotes
Authors’ Note
The manuscript was prepared in accordance with Uniform Requirements for Manuscripts.
Acknowledgements
We wish to thank Deb Keys for providing statistical assistance, Erica Behling-Kelly and Shauna Corsaro for help with image preparation, Cathie Cabe for help with algorithm image design, and all of the practitioners who provided follow-up information for the dogs in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.