
Abstract
An unusual lymphoproliferative disease was identified in multiple closely related British Shorthair (BSH) kittens, suggesting an inherited predisposition to disease. Affected kittens typically developed rapidly progressive and marked generalized lymphadenopathy, moderate splenomegaly, and regenerative and likely hemolytic anemia from 6 weeks of age. Microscopic findings were suggestive of multicentric T-cell lymphoma, but additional testing revealed a polyclonal population of CD3+/CD4–/CD8– “double negative” T cells (DNT cells). This is a novel disease presentation with similarities to the human disorder autoimmune lymphoproliferative syndrome (ALPS), a rare inherited disease causing lymphoproliferation and variable manifestations of autoimmunity. The human disease is most commonly due to the presence of Fas gene mutations causing defective lymphocyte apoptosis, and further investigations of both the mode of inheritance and genetic basis for disease in affected cats are currently in progress.
Keywords
In people, lymphoproliferative diseases (LPDs) are a diverse group of conditions involving abnormal lymphocyte proliferation that include lymphomas as well as a range of less common nonneoplastic lymphoproliferative diseases. 3,7 Most human LPDs occur sporadically, and familial predispositions to LPD in people are rare, usually occurring in association with inherited conditions such as ataxia-telangiectasia, X-linked lymphoproliferative disease, common variable or severe combined immunodeficiency, and autoimmune lymphoproliferative syndrome (ALPS). 22 Lymphoproliferative disease is common in cats due to the high incidence of lymphoma in this species. 12 However, other than an increased occurrence of mediastinal lymphoma in Oriental breeds, including the Siamese, 15 inherited predispositions to LPD have not been previously reported in cats.
In 2009, an unusual LPD was identified in multiple closely related British Shorthair (BSH) kittens in New Zealand. While a diagnosis of lymphoma was initially made, further investigations of affected kittens ultimately confirmed a nonneoplastic multicentric T-cell LPD with a likely inherited basis. The features of the disease in affected kittens differ from those previously reported with known causes of LPD in cats but have similarities to the human disease ALPS.
Herein is described the clinical presentation and pathology of this novel LPD in affected BSH kittens. To the authors’ knowledge, this is the first report of this disease presentation in kittens or cats.
Case Reports
Litter No. 1: Kitten Nos. 1–3
Litter No. 1 resulted from a mating between a BSH tom (T1) and a Manx-BSH queen (Q1) that produced 5 kittens. Between 6 and 7 weeks of age, 3 of 5 kittens in the litter (kitten Nos. 1, 2, and 3; 2 females and 1 male) developed multicentric lymphadenopathy involving all peripheral lymph nodes that rapidly progressed to marked but nonpainful enlargement of multiple nodes over a period of 1 to 2 weeks. Affected kittens also developed progressive abdominal distension and lethargy. Kitten No. 1 showed a moderate to severe regenerative anemia (packed cell volume [PCV] = 11%; reference interval, 24%–45%); PCV was within the reference interval for kitten No. 2. Peripheral leukocytosis (white blood cell [WBC] count = 34.7 × 109/L; reference interval, 5.5–19.5 × 109/L) with a lymphocyte count within the reference interval (1.5–7.0 × 109/L) was present in kitten No. 1 while leukocyte and lymphocyte counts were both within the reference intervals for kitten No. 2. Neither cat had detectable feline leukemia virus (FeLV) antigen or feline immunodeficiency virus (FIV) antibody (AGEN FeLV/FIV Simplify Test; AGEN Biomedical Ltd, Brisbane, Australia). Fine-needle aspirates of enlarged peripheral lymph nodes from 1 affected kitten (kitten No. 1) revealed many large lymphocytes with pleomorphism, macrokaryosis, macronucleoli, and many cells in mitosis, findings interpreted as most consistent with a diagnosis of lymphoma. Both kitten Nos. 1 and 2 developed progressive lethargy between 1 and 2 weeks after lymphadenopathy was first observed and, due to the poor prognosis associated with the presumptive diagnosis, were euthanized. The third affected kitten (kitten No. 3) died without veterinary intervention approximately 1 week after developing lymphadenopathy, and no further investigations were performed on this animal.
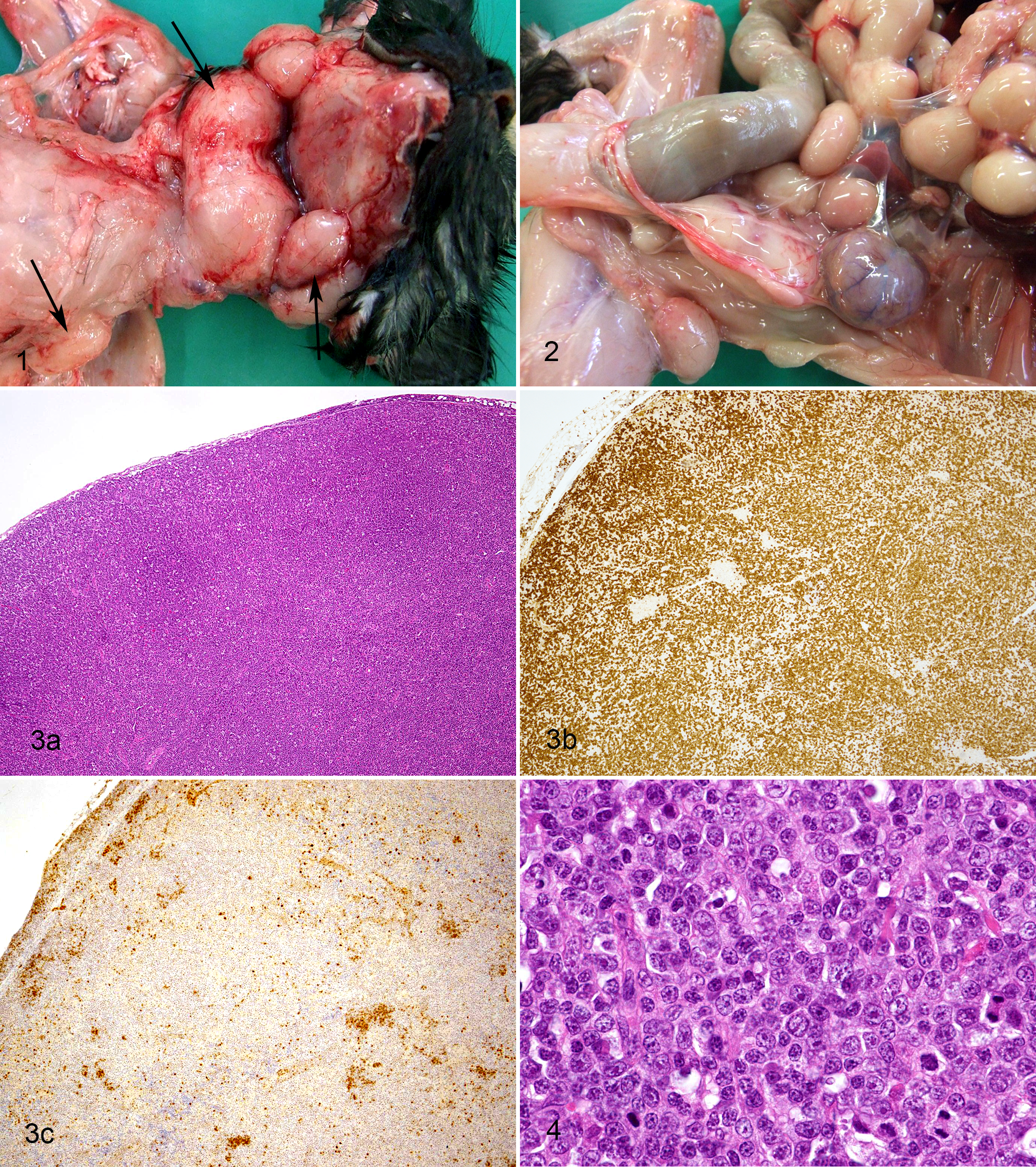
On postmortem examination of kitten Nos. 1 and 2, all identifiable peripheral and visceral lymph nodes had diffuse marked enlargement (Figs. 1, 2) that, on incision, showed effacement of corticomedullary architecture by soft and slightly bulging cream-colored tissue. Mild diffuse hepatic enlargement and moderate diffuse splenic enlargement were also present. Histologically, there was marked expansion of all identifiable lymph nodes by a population of intermediate to large lymphocytes that effaced or markedly distorted nodal architecture with frequent mitotic figures, findings interpreted as consistent with the presumptive cytologic diagnosis of lymphoma. There was also moderate expansion of the splenic white pulp, periportal regions of the liver, and hepatic sinusoids by a population of lymphocytes similar to those present within the nodes. Multifocal areas of scattered extramedullary hematopoiesis were present throughout both spleen and liver, and many splenic and hepatic macrophages contained variable numbers of intracytoplasmic erythrocytes and hemosiderin, indicative of erythrophagocytosis. The thymus of kitten No. 2 was examined and appeared grossly and histologically normal. Immunohistochemistry on sections of lymph node, liver, and spleen from kitten Nos. 1 and 2 using cross-reactive antibodies to human CD3∊ (LN10 mouse monoclonal; Novocastra, Leica Biosystems, Wetzlar, Germany) and human CD79a (HM57 mouse monoclonal; Dako, Carpinteria, CA) as previously described 5,18 revealed a predominant cell population within the lymph nodes exhibiting strong cellular membrane immunopositivity for CD3 and no cytoplasmic immunostaining for CD79a. Lymphocytes expanding the splenic white pulp, periportal regions of the liver, and hepatic sinusoids were also predominantly CD3+/CD79a–. Histological and immunohistochemical findings were interpreted as consistent with a T-cell proliferation within multiple lymph nodes, spleen, and liver, and a diagnosis of T-cell lymphoma was made.
Lymphoproliferative disease, British Shorthair kittens.
Due to the young age and unusual presentation of disease in affected kittens, an attempt to confirm the diagnosis of lymphoma was made by assessing clonality of the proliferating lymphocyte population within the lymph nodes by polymerase chain reaction (PCR) amplification of antigen receptor rearrangements of both the T-cell receptor γ (TCRG) and immunoglobulin heavy chain (IGH) loci on genomic DNA extracted from formalin-fixed, paraffin-embedded (FFPE) lymph node tissue from kitten Nos. 1 and 2 as previously described. 18,19,28 While cytology, postmortem, histology, and immunohistochemistry results had all indicated a diagnosis of T-cell lymphoma, PCR molecular clonality assays for both TCRG and IGH rearrangements revealed broad bands covering a range of product sizes on PCR, consistent with an unusual polyclonal T-cell proliferation and inconsistent with the initial diagnosis of lymphoma.
Litter No. 2: Kitten No. 4
Litter No. 2 resulted from a second mating of T1 and Q1 that produced 6 kittens. At 6 weeks of age, 1 male kitten (kitten No. 4) developed similar clinical signs to affected kittens in Litter No. 1 above (kitten Nos. 1–3) that rapidly progressed over a period of 2 weeks. Blood collected from this kitten had a moderate regenerative anemia (PCV = 18%; reference interval, 24%–45%). Mild peripheral leukocytosis (WBC count = 20.4 × 109/L, reference interval 5.5-19.5 × 109/L) and lymphocytosis (11.2 × 109/L; reference interval, 1.5–7.0 × 109/L) were present. Blood from kitten No. 4 was also negative for the presence of both FeLV antigen and FIV antibody (Snap Combo FeLV Ag/FIV Ab Test Kit; IDEXX Laboratories, Westbrook, ME). The kitten was euthanized at 8 weeks of age following the development of significant lethargy and weight loss.
Post mortem, cytological, histological, and immunohistochemical findings were similar to those described above for kitten No. 2 in Litter No.1 (Figs. 3, 4). Findings were again initially interpreted as consistent with a diagnosis of multicentric T-cell lymphoma. Bone marrow from kitten No. 4 was also examined cytologically and by routine histology and had a mild increase in overall cellularity due to increased erythroid precursors but was otherwise within normal limits; increased numbers of cells with lymphoid morphology were not present. Immunocytochemistry for CD3, CD4, CD8, and MHCII expression was also performed on direct smears made from multiple fine-needle aspirates from lymph nodes from kitten No. 4 using anti–feline CD3∊ (CD3-12; Serotec, Kidlington, UK), anti–feline CD4 (Fe1.7B11; Leukocyte Antigen Biology Laboratory [LABL], Peter F. Moore, University of California, Davis), anti–feline CD8α (Fe1.10E9; LABL), anti–feline CD8β (Fe5.4D2; LABL), or anti–feline MHCII (42.3; LABL) as tissue culture fluid supernatants diluted 1:10 as previously described. 1,26 All lymph nodes predominantly contained a lymphoid cell population that exhibited immunopositivity for CD3 and MHCII and immunonegativity for CD4, CD8α, and CD8β, consistent with a predominant CD3+/CD4–/CD8– T-cell (“double negative T-cell” or “DNT cell”) proliferation, findings again interpreted as consistent with an unusual T-cell lymphoma. However, subsequent molecular clonality PCR assays of DNA extracted from the lymph nodes of kitten No. 4 again revealed findings consistent with a polyclonal and nonneoplastic T-cell proliferation, inconsistent with the earlier diagnosis of lymphoma.
Litter No. 3: Kitten Nos. 5–7
Litter No. 3 resulted from a mating of T1’s son (T2) to the granddaughter of T1 (Q2) that produced 4 kittens. At 5 to 6 weeks of age, 3 of 4 kittens in this litter (kitten Nos. 5, 6, and 7; 2 females and 1 male) developed similar clinical signs to those seen in affected kittens in Litter Nos. 1 and 2 that again rapidly progressed over a period of 2 to 4 weeks. Blood collected from 1 kitten (kitten No. 5) revealed a severe regenerative anemia (PCV = 11%; reference interval, 24%–45%). Peripheral leukocyte and lymphocyte counts were both within reference intervals (WBC count = 5.5–19.5 × 109/L, 1.5–7.0 × 109/L), and blood was negative for the presence of FeLV antigen and FIV antibody (Snap Combo FeLV Ag/FIV Ab Test Kit). All 3 affected kittens were euthanized between 8 and 10 weeks of age following the development of significant lethargy.
Further diagnostics were performed on kitten No. 5; no further investigations were undertaken on kitten Nos. 6 and 7. Post mortem, cytological, histological, and immunohistochemical findings in kitten No. 5 were similar to those described above for kitten No. 4 in Litter No. 2, and subsequent molecular clonality PCR assays of DNA extracted from the lymph nodes of kitten No. 5 again revealed findings consistent with a polyclonal and nonneoplastic T-cell proliferation.
Litter No. 4: Kitten Nos. 8 and 9
Litter No. 4 resulted from a mating of T1’s grandson (T3) to a new BSH queen (Q3) that produced 4 kittens. At 6 weeks of age, 2 of 4 kittens in the litter (kitten Nos. 8 and 9; both female) developed similar clinical signs to those seen in affected kittens in the earlier litter Nos. 1 to 3. Blood collected revealed a mild to moderate regenerative anemia (PCV = 23% [kitten No. 8] and 19% [kitten No. 9]; reference interval, 24%–45%). Mild peripheral leukopenia (WBC count = 4.7 × 109/L; reference interval, 5.5–19.5 × 109/L) with a mild lymphopenia (lymphocytes = 1.4 × 109/L; reference interval, 1.5–7.0 × 109/L) was present in kitten No. 8; leukocyte and lymphocyte counts were within reference intervals in kitten No. 9. Evidence of gross autoagglutination potentially consistent with immune-mediated hemolytic anemia was present on blood smears from kitten No. 9, but blood samples from both this kitten and kitten No. 8 were negative on direct Coombs’ testing. Blood from both kittens was negative for the presence of both FeLV antigen and FIV antibody (Snap Combo FeLV Ag/FIV Ab Test Kit). Following the development of lymphadenopathy, both kittens received immunosuppressive doses of corticosteroids (2.2 mg/kg prednisone per os sid) for the 2 weeks prior to euthanasia, but the lymphadenopathy continued to progress, and kitten Nos. 8 and 9 were euthanized at 12 and 14 weeks, respectively, following the development of persistent lethargy and weight loss.
Postmortem and microscopic findings in kitten No. 9 were generally similar to those described above for kitten No. 4 in litter No. 2. However, in kitten No. 8, lymph nodes were less dramatically enlarged compared with earlier cases, and splenic enlargement was minimal. In contrast to earlier cases, lymph nodes from both kitten Nos. 8 and 9 typically had moderate to marked distortion of nodal architecture by a population of large lymphocytes rather than complete effacement. Several lymph nodes from these 2 kittens also contained moderate numbers of plasma cells, Mott cells, and macrophages scattered throughout both cortical and medullary regions. Lower numbers of lymphocytes were also present within the splenic white pulp and hepatic sinusoids of these kittens compared with earlier cases.
Immunohistochemistry for CD3 and CD20 (anti-human, L26, mouse monoclonal; Novocastra, Leica Biosystems) was performed on sections of lymph nodes, spleen, and liver as previously described. 5 Specific findings differed slightly from earlier cases since while nodes from both kittens had distortion and occasionally effacement of architecture by a predominantly CD3+/CD20–cell population consistent with T cells, variable numbers of CD3–/CD20+ B cells were also present within follicular remnants and subscapular sinuses of several nodes. Similar to kitten No. 4, immunocytochemistry to assess CD3, CD4, and CD8 expression was also done on direct smears of multiple fine-needle aspirates from lymph nodes of both kittens. Results indicated that the markedly expanded population of lymphocytes were CD3+/CD4–/CD8– DNT cells. As with the earlier cases, subsequent molecular clonality PCR assays of DNA extracted from the lymph nodes of kitten Nos. 8 and 9 again revealed findings consistent with a polyclonal and nonneoplastic T-cell proliferation.
Summary details of the cases included in this study are presented in Supplemental Table S1, and a partial pedigree chart showing the relationships between affected kittens is set out in Figure 5.
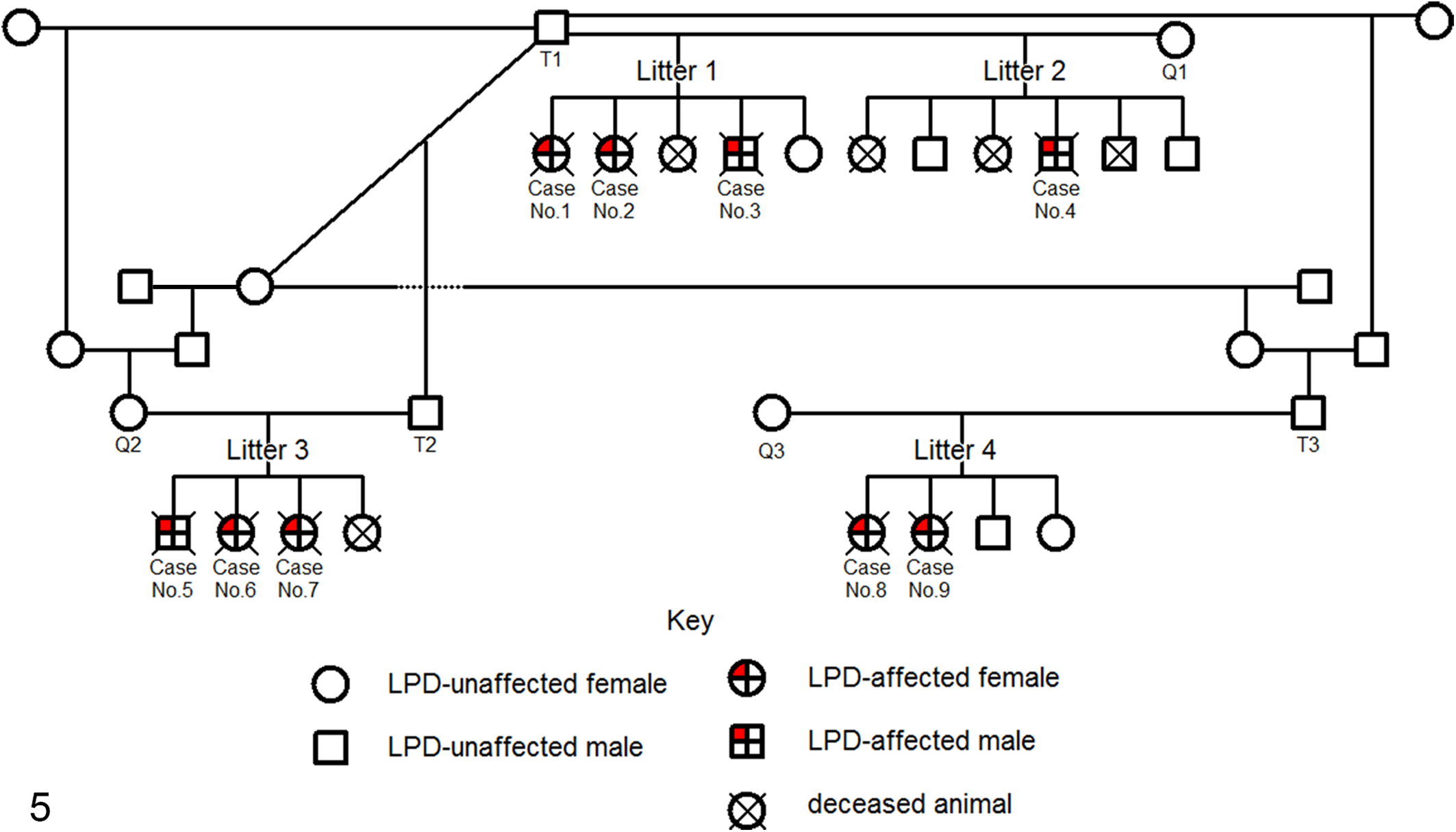
Partial pedigree of kittens affected by lymphoproliferative disease (LPD). All LPD-affected kittens are closely related and share at least one common ancestor (T1). None of the parents of any LPD-affected kittens are themselves affected by LPD.
Discussion
We describe a disease in BSH kittens that presented with multicentric nonpainful lymphadenopathy at 6 to 7 weeks of age. The disease rapidly progressed over several weeks to a dramatic lymphadenopathy affecting multiple lymph nodes. During this period, affected kittens also developed marked abdominal distension, variable regenerative and probable hemolytic anemia, progressive lethargy, and weight loss that ultimately resulted in euthanasia. Postmortem examination revealed marked diffuse enlargement of all identifiable lymph nodes and moderate splenomegaly. Histologically, most affected lymph nodes had effacement or marked distortion of architecture by a population of T cells consistent with DNT cells; infiltration of the spleen and liver also occurred but was more variable.
Prior to molecular clonality PCR testing, the results of cytology, histology, and immunohistochemistry all supported a diagnosis of T-cell lymphoma. However, the very young age of affected kittens, the pattern of disease affecting multiple closely related animals, and the presence of such rapidly progressive and marked generalized lymphadenopathy were not typical for feline lymphoma. Clonality assays using PCR to assess antigen receptor gene rearrangements are considered the most reliable basis on which to differentiate lymphoma from nonneoplastic lymphocyte proliferations 27 and have been validated for use in cats. 19,26,28 In all cases tested, molecular clonality assessment revealed a polyclonal proliferation of T cells inconsistent with lymphoma and indicative of an unusual nonneoplastic LPD.
The disease in these kittens appears to be inherited. Affected kittens were closely related with at least one common ancestor (T1). A disease with similar features to that reported here also appears to have been seen in related BSH kittens in Australia (Richard Malik, personal communication, 2014), providing further support for an inherited basis for disease. Its occurrence in both male (n = 3) and female (n = 6) kittens and the fact that all parents of affected kittens were unaffected by LPD both tend to support an autosomal recessive mode of inheritance, but other inheritance modes such as modified autosomal dominant inheritance are still possible, and further information is needed. However, although the mode of inheritance has yet to be confirmed, it is still recommended that the parents of any litter in which this disease is identified as well as any unaffected littermates of affected kittens are not used for breeding, as such animals are potential carriers of any causative genetic mutation. As the disease affects kittens early in life, identifying and excluding potential carrier animals from the BSH breeding population should ultimately reduce the frequency of disease occurrence. However, the BSH breed has a small gene pool in New Zealand, and stud animals are often used intensively by breeders. Consequently, any underlying genetic defect may already be widespread within the BSH breed both in New Zealand and other countries, and the exclusion of potential carrier animals and elimination of the disease may take some time.
Due to the presence of gross autoagglutination and histological evidence of erythrophagocytosis, probable immune-mediated hemolytic anemia was diagnosed, and treatment with immunosuppressive doses of corticosteroids was attempted in 2 affected kittens but was not successful. In both kittens, lymphadenopathy did not reduce and lethargy and weight loss worsened during the treatment course, with both animals ultimately requiring euthanasia. The implications of the failure to respond to treatment are presently uncertain. It is possible that immunosuppressive treatment would have been successful in managing the anemia and other clinical signs of disease had a longer treatment period than 2 weeks been possible, but unfortunately, the development of marked lethargy and weight loss necessitated euthanasia before any effects of treatment could be evaluated. It is also possible that the disease may not have responded to prednisone treatment because the dose administered was at the low end of that recommended in cats. 13 A higher prednisone dose rate or an alternative immunosuppressive drug, such as mycophenolate mofetil, 2 may have more successfully managed the clinical signs of disease in these kittens. However, it is also possible that treatment was unsuccessful due to the absence of any immune-mediated basis for disease development in these kittens. Suspicion of immune-mediated hemolytic anemia was based on the presence of regenerative anemia, evidence of gross autoagglutination, and erythrophagocytosis seen histologically and the absence of evidence of a hemorrhagic cause of the anemia. Additional testing to confirm a likely immune-mediated basis for the disease and immunosuppressive treatment of future cases are therefore needed to confirm the basis for immunosuppressive treatment in affected animals.
The clinical presentation and pathology of the disease in affected BSH kittens have several similarities to ALPS in people, a rare inherited disorder that causes persistent lymphoproliferation due to increased numbers of polyclonal DNT cells (CD3+/CD4–/CD8–) together with variable manifestations of autoimmunity. 20,23,24 Most (>70%) human patients with ALPS have inherited Fas gene mutations causing defective lymphocyte apoptosis, although in a proportion of people, the cause of disease is unknown. 21 Patients typically present in childhood with a chronic nonneoplastic but often dramatic lymphadenopathy, splenomegaly, and variable immune-mediated cytopenias, most commonly anemia. 23,25 Although most ALPS cases have an autosomal dominant pattern of inheritance, there is incomplete penetrance of the genotype and variable expression of the clinical signs. 10,11
Both ALPS in people and the disease in the kittens described here cause a nonneoplastic generalized marked lymphadenopathy and splenomegaly due to a proliferation of polyclonal DNT cells. 14,20,23 Cytopenias, including hemolytic anemia, are often present in ALPS; 10,24 evidence of a hemolytic anemia, including autoagglutination or erythrophagocytosis, was also present in several LPD-affected kittens. Thymic enlargement is not typically present in people with ALPS, 14 nor was it a feature of the disease in kittens, possibly supporting a similar mechanism of defective T-cell apoptosis in the feline disease. Both diseases typically have an early age of onset. The median age of presentation for patients with ALPS is approximately 24 months, 21 while all affected BSH kittens were less than 8 weeks of age at the first development of clinically detectable LPD. The disease in people is inherited, typically with an autosomal dominant mode of inheritance with variable expression of the clinical signs. 10 The feline disease also appears to have an inherited basis, and although the mode of inheritance is currently uncertain, autosomal recessive inheritance is considered most likely, and further studies to clarify this are in progress.
There are also features of the feline disease that appear to differ from ALPS in people or about which further information is needed. First, disease in patients with ALPS is typically chronic; a diagnostic criterion for ALPS is that the LPD is of more than 6 months’ duration. 20 In contrast, the disease in kittens is typically acute and rapidly progressive, with all affected kittens either dying or being euthanized early in the clinical course following the development of marked lethargy and weight loss. In addition, no evidence of significant immune-mediated neutropenia or thrombocytopenia was present in affected kittens; these cytopenias are frequently present in patients with ALPS. 24,25 Furthermore, people with ALPS typically show defective Fas-mediated lymphocyte apoptosis on in vitro assays, 20,23 tests that could not be performed on samples from any affected kitten described here. Finally, the typical microscopic changes within lymph nodes in ALPS are of marked paracortical T-cell expansion with retention of nodal architecture and variable numbers of plasma cells, 14 different from the more marked nodal distortion or complete effacement by T cells seen in the majority of affected kittens. However, it is of note that in some cases of ALPS, the T-cell proliferation is sufficiently florid to suggest a diagnosis of lymphoid neoplasia, and many early ALPS cases were initially misdiagnosed as lymphoma. 4,23 Interestingly, lymph nodes from kitten Nos. 8 and 9 showed incomplete effacement and contained significant numbers of plasma cells and macrophages within the proliferating T-cell population, features more similar to those described in ALPS. This may be because these 2 kittens were euthanized later in the clinical course of disease than the earlier cases, allowing more time for nodal infiltration of plasma cells and macrophages similar to histological findings seen in the more chronic disease in people. Alternatively, findings may reflect a partial response to immunosuppressive treatment in these 2 kittens.
There was no evidence to suggest that the LPD in affected kittens was due to any of the previously reported causes or syndromes of LPD in cats. While both FeLV and FIV infection reportedly cause LPD in cats, 8 affected BSH kittens repeatedly tested negative for evidence of either FeLV or FIV infection, including during the period when overt clinical signs of LPD were present. Although false-negative results occur with the tests used for both viruses here, reported sensitivities of both tests are excellent (>92%), 6,9 and the likelihood that multiple infected kittens tested falsely negative for evidence of either virus is extremely low. Accordingly, neither FeLV nor FIV is considered likely to have contributed to the development of LPD in these kittens. Similarly, the clinicopathological features of the disease in these kittens differ from those described in 2 previously reported but poorly defined diseases of cats causing lymphadenopathy: distinctive peripheral lymph node hyperplasia (DPLNH) 17 and generalized lymphadenopathy resembling lymphoma (GLRL). 16
The possibility that a novel infectious agent caused the development of disease in the kittens cannot be excluded but is considered unlikely as none of the parents of any affected kitten showed signs of disease at any stage. Furthermore, if a novel infectious agent was associated with the development of LPD in these kittens, it would be expected that this agent also would have affected kittens of breeds other than the BSH. To date, this has not been reported.
In conclusion, we report a disease that results in marked multicentric lymphadenopathy in young BSH cats with several similarities to the human disease ALPS. To the authors’ knowledge, this disease presentation has not been previously reported in cats. The development of the disease in multiple closely related BSH kittens suggests that the disease has an inherited basis. Evidence from the small number of cases to date suggests that the disease is uniformly fatal due to the development of marked lethargy and weight loss requiring euthanasia, typically within a period of 2 to 3 weeks of the onset of clinical signs. The clinical and microscopic features of the disease are suggestive of T-cell lymphoma, and molecular clonality PCR testing is required to identify the polyclonal and nonneoplastic nature of the lymphocyte proliferation. Observations of these kittens suggest that the development of marked multicentric lymphadenopathy with distortion or effacement of nodal architecture in a young cat should not automatically be assumed to be lymphoma, and molecular clonality PCR testing should be performed to exclude this unusual nonneoplastic disease. Recognizing and accurately diagnosing this disease is important given the apparently inherited basis and desirability of reducing future cases of disease by preventing potential gene carriers being used as breeding animals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the Palmerston North Medical Research Foundation and the Institute of Veterinary, Animal and Biomedical Sciences, Massey University.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.