
Abstract
Machupo virus, the causative agent of Bolivian hemorrhagic fever (BHF), is a highly lethal viral hemorrhagic fever of which little is known and for which no Food and Drug Administration–approved vaccines or therapeutics are available. This study evaluated the cynomolgus macaque as an animal model using the Machupo virus, Chicava strain, via intramuscular and aerosol challenge. The incubation period was 6 to 10 days with initial signs of depression, anorexia, diarrhea, mild fever, and a petechial skin rash. These were often followed by neurologic signs and death within an average of 18 days. Complete blood counts revealed leukopenia as well as marked thrombocytopenia. Serum chemistry values identified a decrease in total protein, marked increases in alanine aminotransferase and aspartate aminotransferase, and moderate increases in alkaline phosphatase. Gross pathology findings included a macular rash extending across the axillary and inguinal regions beginning at approximately 10 days postexposure as well as enlarged lymph nodes and spleen, enlarged and friable liver, and sporadic hemorrhages along the gastrointestinal mucosa and serosa. Histologic lesions consisted of foci of degeneration and necrosis/apoptosis in the haired skin, liver, pancreas, adrenal glands, lymph nodes, tongue, esophagus, salivary glands, stomach, small intestine, and large intestine. Lymphohistiocytic interstitial pneumonia was also present. Inflammation within the central nervous system (nonsuppurative encephalitis) was histologically apparent approximately 16 days postexposure and was generally progressive. This study provides insight into the course of Machupo virus infection in cynomolgus macaques and supports the usefulness of cynomolgus macaques as a viable model of human Machupo virus infection.
Machupo virus (MACV), an enveloped RNA virus of the Arenaviridae family, has a viral genetic code composed of 2 single-stranded RNA molecules known as the L (large) and S (small) segments. 19,35 MACV is the source agent of outbreaks of Bolivian hemorrhagic fever (BHF) in remote endemic regions of South America. BHF was first described during an outbreak of severe febrile disease in 1959 that occurred in a remote prairie region between Bolivia and Brazil. The causative agent was subsequently isolated in 1963 and named Machupo virus after the tributary of the Itenez River that flows through the area where the outbreak occurred. 5,16,30,32,35 After a thorough field investigation, the rodent vector, Calomys callosus, was identified. 11,19,35 Arenavirus infections are acquired by inhalation of aerosolized virus from rodent urine or excreta (eg, from sweeping floors), ingestion of virus via contaminated foodstuffs, or introduction of virus onto mucous membranes. 4,5,21 –24,27 –29,33,42 A major outbreak of BHF was controlled through the use of rodent traps in the summer of 1964. 12,19
Outbreaks of BHF in humans have been amplified or maintained by close contact between patients and either professional caregivers or attending family members. 4,33 Caregiver transmission is believed to be the result of accidental aerosolization during medical procedures or through contact with patient bodily fluids or materials contaminated with bodily fluids. Based on this observation, secondary cases can be reasonably expected during an intentional release of aerosolized MACV by a bioterrorist. First responders and medical personnel could be most at risk from such an exposure. Potential exposure to MACV in a laboratory or health care setting could occur through needle stick, direct contact, or aerosols. The ease of dissemination from rodent hosts to humans and human-to-human and a high fatality rate (5%–30%) 19,35 make MACV of premier importance that warrants inclusion on the National Institute of Allergy and Infectious Diseases Priority Pathogens List. 8,32 Thus, development of parenteral and aerosol exposure animal models for MACV infection is critical, and ultimately, testing of vaccines and therapeutics is a pressing priority.
Today, potential outbreaks or spread of this agent remain a great concern due to our lack of understanding of this disease and an effective treatment. 1,2,20 The dearth of scientific knowledge pertaining to MACV infection is due in part to the sporadic and remote nature of the outbreaks. Other major stumbling blocks to understanding this virus are the requirement for biosafety level 4 high-containment laboratory facilities, properly trained personnel to study MACV, and a general lack of funding for further studies. Studies documenting the natural history and pathogenesis of MACV are essential to facilitate our understanding of this virus. These investigations will ultimately form the foundation of scientific knowledge necessary for the development of vaccines and therapeutics to counteract the sporadic or intentional spread of BHF.
The cynomolgus macaque is a commonly used animal model in scientific research. As these nonhuman primates mount similar immunologic and physiologic responses to humans, cynomolgus macaques are effective animal models of disease. 9,11 In this study, we assessed whether the MACV Chicava strain would be lethal in macaques and whether the disease course and lesion development are analogous to that seen in humans. The Chicava strain was selected for this work as this strain was isolated without passage in animals and is currently used in guinea pig models.
Materials and Methods
Sixteen adult research naive male and female cynomolgus macaques of Chinese origin weighing between 4 and 9 kg were obtained from licensed and approved vendors. These macaques were determined to be free of preexisting immunity to MACV via the standard plaque reduction neutralization test. 18 Three studies consisting of 4 macaques in each dose group were performed. First, an intramuscular (IM) exposure study was performed using a standard challenge dose of 1000 plaque-forming units (PFU). Two subsequent studies were performed using the aerosol exposure method 7,17,37 , the first using a target dose of 1000 PFU and the second using target doses of 100 and 10 000 PFU. For each study, animals were randomly selected from the colony for enrollment. All animals either succumbed to disease or were euthanized at end of study between 30 and 42 days postexposure. The end of study for the IM-challenged macaques was 30 days postexposure; however, all macaques succumbed prior to or on day 21. For the aerosol studies, the study end point was extended to 35 or 42 days as some macaques survived beyond the hemorrhagic phase of disease.
This study was approved by the Institutional Animal Care and Use Committee, and research was conducted in compliance with the Animal Welfare Act and other federal statutes and regulations relating to animals. Experiments involving animals adhered to principles stated in the Guide for the Care and Use of Laboratory Animals from the National Research Council. The US Army Medical Research Institute of Infectious Diseases (USAMRIID) is fully accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International.
Virus Isolation, Preparation, Plaque Assay, Exposure, and Sampling Scheme
The MACV Chicava strain used in these studies was isolated from a fatal human case of BHF occurring in the Beni Province in 1994. The serum sample was sent to the Centers for Disease Control and Prevention (CDC), confirmed to contain the MACV Chicava strain, and designated as CDC#806786. The serum sample was passaged once (P1) on Vero E6 cells at the CDC by personnel of the Special Pathogens Branch. Then, cell culture supernatant from the infected flask was retrieved and used to infect a second Vero E6 monolayer (P2). A sample of supernatant from P2 was sent to USAMRIID. For a detailed description of how the virus was isolated and prepared as well as how animals were inoculated and samples were collected, please see the online supplemental material.
Clinical Chemistry and Hematology
Complete blood counts (CBCs) were performed using the HemaVet 950 FS Hematology Analyzer (Drew Scientific, Oxford, CT) in accordance with manufacturer’s guidelines. Serum chemistry analysis was obtained from whole-blood samples collected in sterile red-topped tubes. Serum was separated from whole blood by centrifugation at 1800 g. An aliquot of 100 μl was analyzed for glucose, creatinine, urea, serum urea nitrogen, calcium, albumin (ALB), total protein (TP), alanine transaminase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), total bilirubin, γ-glutamyl transferase, and amylase via the General Chemistry 13-panel rotor on a Piccolo Blood Chemistry Analyzer (Abaxis, Union City, CA). Results were compared with a panel of more than 100 institute historical control samples.
Histopathology and Immunohistochemistry
Complete necropsies were performed on each animal immediately following euthanasia in the USAMRIID biosafety level 4 laboratory. Tissues from all major organ systems were collected from each animal, immersion fixed in 10% neutral buffered formalin, and held in biocontainment for a minimum of 21 days. Histopathology samples were routinely processed, embedded in paraffin, sectioned, and stained with hematoxylin and eosin.
Immunohistochemistry (IHC) was used to identify cells containing MACV antigen via an immunoperoxidase assay using rabbit polyclonal antisera specific for MACV. This antibody was produced at USAMRIID by injecting rabbits with ultraviolet-inactivated MACV virus (Malale strain). Serum was collected and was determined to be cross-reactive to MACV strains Carvallo, Chicava, and Malale (unpublished data). Stained normal macaque liver sections served as the negative control. The positive control was stained liver sections from a macaque that had died from experimental MACV (Carvallo strain) infection at this institute. Normal mouse IgG was used as the negative serum control for the control slides. For a more comprehensive description of how these slides were prepared, please see the online supplemental materials.
Transmission Electron Microscopy
Select tissues were identified for transmission electron microscopy, cut into approximately 1-mm3 sections, rinsed in buffer, refixed in a mixed aldehyde fixative in 0.1 M of phosphate buffer, and postfixed in phosphate-buffered osmium tetroxide. Further sample processing and imaging were carried out as previously reported. 41 Samples were contrasted in ethanolic uranyl acetate, dehydrated through a series of graded ethanol and propylene oxide washes, and then embedded in EMbed-812 resin (Electron Microscopy Sciences, Hatfield, PA). Embedded tissues were cut with a Leica ultramicrotome Buffalo Grove, IL and mounted on copper grids. Thin sections were contrasted with uranyl and lead salts before examination on a 1011 transmission electron microscope (JEOL USA, Peabody, MA). Images were captured using a side-mounted DVC 1412AM-FW-TE camera (DVC, Austin, TX) or Hamamatsu digital camera with AMT v600 acquisition software (Advanced Microscopy Techniques, Woburn, MA).
Statistical Analysis
Using the change from baseline, pairwise comparisons between dose groups, adjusted for multiple testing by permutation, were made at each time point using dose, day, and the dose vs day interaction variables using a 2-sided t test. The means for each group were compared with 0 to determine significance for that group at each time point. Forest plots, which are figures that compare confidence intervals in a tabular format, were generated with SAS software, version 9.4 (SAS Institute, Cary, NC). The graphical portion of the forest plot represents the estimate of the mean using a box and the estimate of the 95% confidence interval using a line. A reference line indicates the expectation under the null hypothesis (no difference between the groups) of the test represented in the plot. Comparisons bearing confidence intervals overlapping this line were discarded as not statistically significant.
Results
Clinical Presentation of MACV Infection
Of the 4 macaques challenged IM with MACV Chicava strain, all appeared clinically normal until day 6. One macaque had decreased food consumption and blood-tinged urine on days 6 and 8, respectively. The rest of the macaques showed clinical signs of MACV infection on day 10 (weakness, depression, mild fever, dehydration, rash). A red, macular rash developed in the axillary and inguinal regions of several IM-challenged macaques and progressed to become more prominent in the affected areas with regional spread (Fig. 1). Hemorrhagic manifestations occurring on days 8 to 12 consisted of hematuria and epistaxis. One macaque experienced a tremor on day 10 and had ataxia by day 15, with death occurring on day 16. By day 17, the 3 remaining IM-challenged macaques had facial edema, darkened hard palate, and a blackish/purple discoloration of the lips. These macaques met end-point euthanasia criteria on days 18, 18, and 21 (Suppl. Table S1).
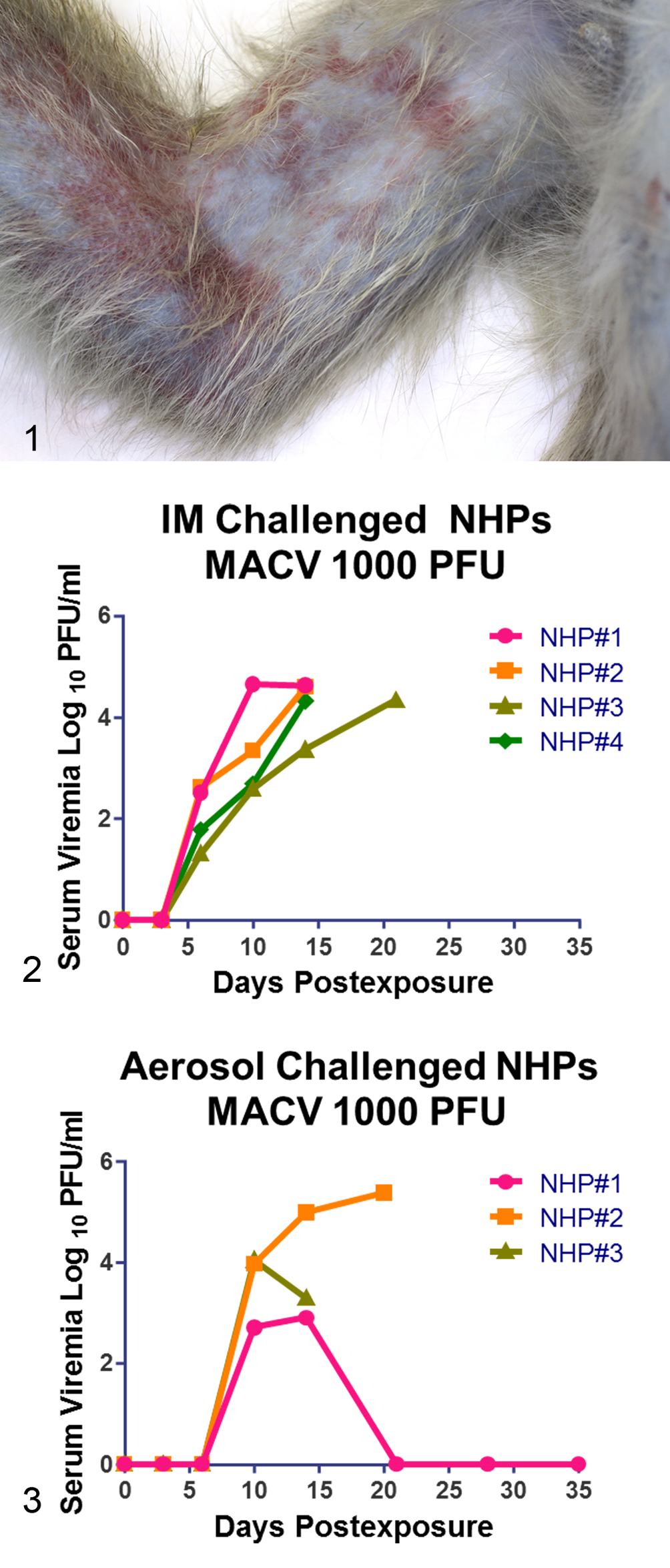
Following the initial IM challenge study, we used the same target challenge dose (1000 PFU) to expose 4 additional macaques to aerosolized virus. In this first aerosol study, 2 macaques survived. In an attempt to identify a more appropriate target challenge dose to ensure uniform lethality, we conducted a third study in which 8 macaques were exposed to either 100 or 10 000 PFU of aerosolized MACV (4 macaques in each dose group). Clinical signs were similar in all challenge groups. The 1000 PFU IM group had a slightly faster clinical progression of disease, with clinical signs and serum viremia noted 3 days earlier compared with the 3 aerosol groups (Figs. 2, 3). In general, macaques became lethargic, anorexic, and febrile, with loose stools or overt diarrhea occurring around day 8 in the IM-challenged group and around day 10 in the aerosol-challenged groups.
Some aerosol-exposed macaques experienced labored breathing and respiratory difficulty not seen in the IM group. Interestingly, at approximately day 21 postexposure, 1 macaque in the highest dose aerosol exposure group (10 000 PFU) displayed behaviors suggestive of photophobia. Photophobia is a reported observation in human cases of BHF. 26
By day 21, all macaques in all groups had either succumbed to infection (all 4 IM-challenged macaques) or had begun to clinically improve (Suppl. Table S1). One macaque in the 10 000 PFU aerosol group initially became ill and appeared to begin to recover around day 14 postexposure; however, by day 23, this animal developed severe neurologic signs and met euthanasia criteria on day 34 postexposure.
Clinical Chemistry and Hematology
IM Challenge
CBCs revealed that the number of leukocytes decreased initially. Lymphocytes, monocytes, and neutrophils were consistently affected. Total leukocyte numbers as well as individual measurements of lymphocytes, monocytes, and neutrophils began to decrease on day 3 and continued to decrease until day 10, with a majority of animals having a reversal and slight recovery in overall leukocyte numbers as well as increases in lymphocytes, monocytes, and neutrophils by day 14. Platelets decreased steeply over the course of the disease. On day 14, the 4 IM-challenged macaques had significantly decreased (P < .0001) platelet concentrations ranging from 30–153 × 103/μl (normal reference range for cynomolgus macaques at this institute ranging from 281–457 × 103/μl).
Chemistry panel screening revealed changes in TP, ALB, ALT, AST, and ALP by day 14 in the majority of macaques. Serum TP concentrations dropped significantly (P < .0001); ALB was the major contributing factor (1.3–2.2 g/dl; normal reference range from institute archives of 2.8–4 g/dl, P = .0012). Liver aminotransferases were increased in all 4 macaques with ALT concentrations ranging from 105 to 1599 U/l (reference range of 23–61 U/l, P = .0412) and AST concentrations ranging from 173 to 2000 U/l (reference range of 25–63 U/l, P = .0133). In 3 of 4 macaques, ALP concentrations were increased with concentrations ranging from 399 to 706 U/l (reference range of 67–330 U/l, P = .0001).
Aerosol Challenge
Aerosol-challenged macaques had similar CBC findings to the IM-challenged macaques. As with the IM-challenged macaques, platelets also decreased steeply over the course of the disease. The only statistically significant differences between MACV dose groups were noted for eosinophil and monocyte populations. For both these cell types, the 10 000 PFU aerosol dose group had significantly higher cell counts in macaques surviving at day 21 than the 1000 PFU and 100 PFU groups (P < .0001 for all comparisons). TP concentrations dropped near the end of the disease course for macaques succumbing during the acute phase (beginning at 7–10 days through day 21 postexposure), and a major contributing factor to this decrease in TP was a decrease in ALB.
Serum chemistry results of liver and renal function support the diagnosis of hepatic necrosis with declining liver function and azotemia. Concentrations of ALT and AST increased dramatically in the days preceding death in those that succumbed on or before day 21 postexposure (P = .0054, P < .0001). ALP concentrations increased prior to death in fewer macaques compared with those with increased AST and ALT (data not shown). In addition, serum urea nitrogen and creatinine increased markedly during the last few days prior to death in 3 of the 12 aerosol-challenged macaques (P < .0001 for all). Although prerenal azotemia was presumed (likely due to decreased glomerular filtration rate secondary to renal hypoperfusion occurring with metabolic shock), urine was not available for concentration analysis to confirm cause.
Pathology
Gross Pathology
Gross pathology observations in the IM group included a macular rash (Fig. 1); hemorrhages covering the serosal and mucosal surfaces of the small and large intestine (Fig. 4); enlarged spleen; irregularly pale, friable, and mildly enlarged liver; enlarged peripheral lymph nodes; and diffusely congested meninges (Suppl. Table S1).
Reflecting the route of exposure, appreciable gross pathologic and histopathologic changes unique to the aerosol-challenged macaques were in the lung (Fig. 5). Grossly, in 5 of 12 macaques, lung lobes did not completely collapse and were red and mottled. Serous fluid exuded from serosal surfaces (Suppl. Table S1 and Fig. 5). All other gross pathologic changes were similar between the aerosol- and IM- exposed macaques.
Histology and Immunohistochemistry
IM challenge
Histologically, widespread organ involvement was noted that mainly affected the haired skin, liver, spleen, lung, esophagus, small intestine, large intestine, adrenal gland, pancreas, submandibular salivary gland, lymph nodes, urinary tract, bone marrow, and central nervous system (Figs. 6a–12a and Suppl. Table S2). Some of the IM-challenged macaques had minimal-to-mild interstitial pneumonia; however, this pneumonia was much less severe and found in fewer areas compared with that observed in the aerosol-exposed groups.
In the liver, mild-to-moderate multifocal hepatocellular cell death was noted, with mild mixed cellular inflammation scattered throughout sinusoids and/or surrounding portal areas. Basophilic cytoplasmic inclusion bodies in hepatocytes were strongly immunoreactive for MACV antigen (Fig. 7a,b). Transmission electron micrographs of liver sections demonstrated multiple, prominent electron-dense inclusions measuring at least 1 μm2 and often as large as 6 to 8 μm2 (Fig. 14a,b). Higher magnification revealed these inclusions to be composed of tightly packed, electron-dense spheres approximately 25 nm in diameter (Fig. 14b). Similar cytoplasmic basophilic inclusion bodies were noted in pancreatic islets and adrenal glands along with degeneration of the adrenal cortical cells (Fig. 11a).
(a) Hepatic inclusions, liver; cynomolgus macaque No. 2, intramuscular challenge. Multiple, prominent electron-dense inclusions (arrows) are ≥1 μm2 and are often as large as 6 to 8 μm2. Bar = 1 μm. (b) Inclusions, composed of tightly packed electron-dense spheres, ˜25-nm diameter spheres, are most likely ribosomes. Bar = 50 nm. Transmission electron microscopy.
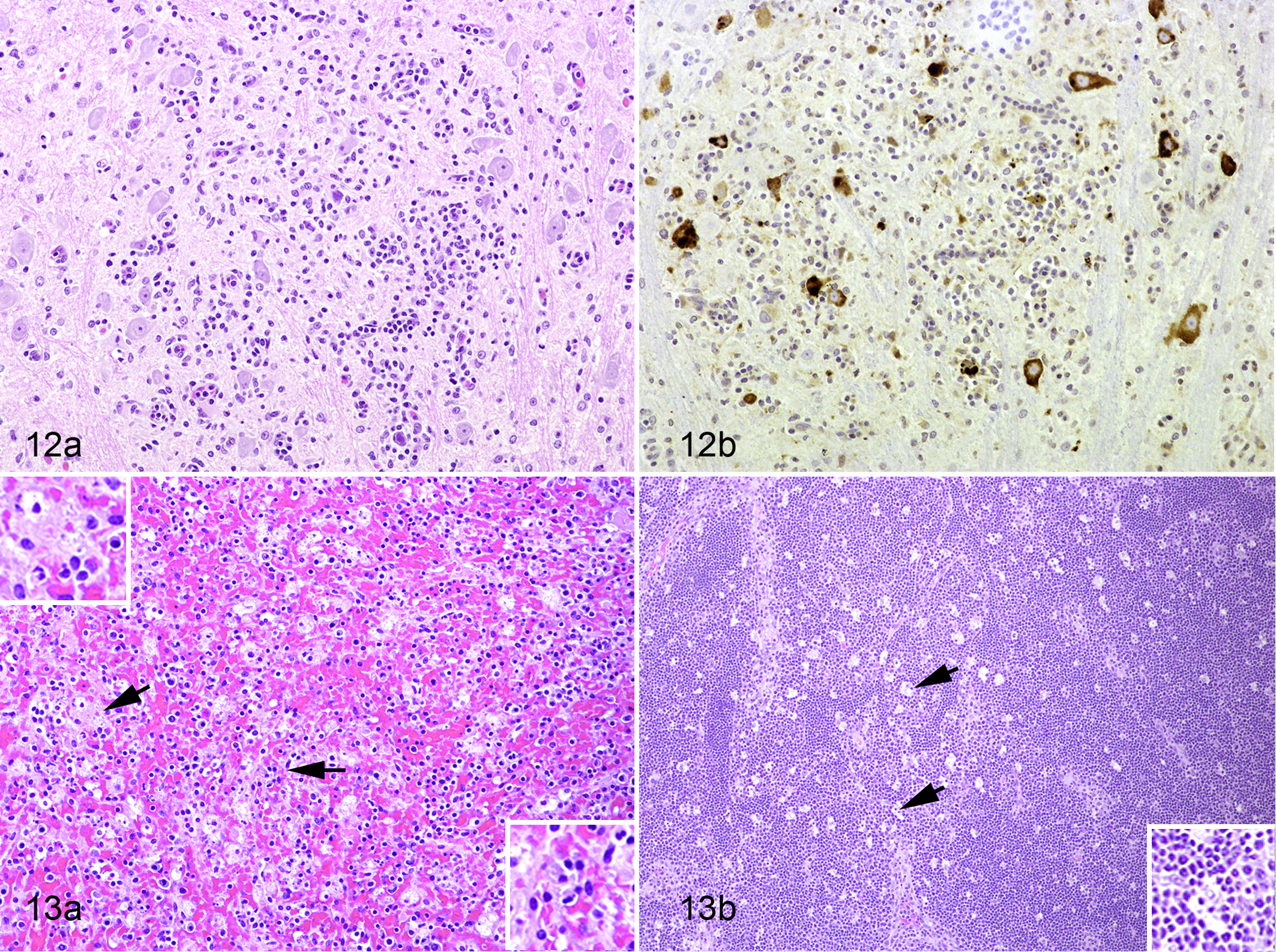
In the spleen, lymph nodes, and tonsils, lymphocytolysis and lymphoid depletion were noted. Splenic lymphoid cell death, mild-to-moderate hypocellularity of the red and white pulp, and mild mixed cell death of macrophages were accompanied by moderate congestion/hemorrhage and fibrin deposition (Fig. 13a). Moderate numbers of tingible body macrophages (arrows) were present in all lymph nodes (Fig. 13b) and tonsils.
Degeneration and cell death were noted in epithelial cells within the tongue, esophagus, haired skin (Fig. 6a), urinary tract, renal tubules (rarely noted), adrenal glands (Fig. 11a), submandibular salivary glands, and pancreas. Epithelial cells in the skin (Fig. 6b) and in areas of degeneration within the adrenal cortex (Fig. 11b) displayed strong immunoreactivity to MACV antigen. In areas of epithelial compromise in the tongue, esophagus, and larynx, bacterial colonies were commonly associated with localized ulcerative and inflammatory lesions.
In the small and large intestine, and to a much lesser degree in the stomach, cell death of cells believed to be macrophages within the lamina propria was immunoreactive to MACV antigen (Figs. 9–10a,b). Multifocal degeneration and cell death of the glandular epithelial cells that were immunoreactive to MACV antigen resulted in glandular or villous atrophy.
In all IM-challenged macaques, minimal-to-mild mononuclear perivascular inflammation was noted within the cerebrum, choroid plexus, or brainstem of all animals, and rare glial nodules were present within the gray matter.
Bone marrow changes included multifocal cell death with fibrin accumulation; a few progenitor cells and megakaryocytes showed strong, specific, intracytoplasmic positive immunoreactivity to MACV antigen (Suppl. Table S3).
Aerosol challenge
Histologically, lesions in the aerosol-challenged group consisted of a more pronounced interstitial pneumonia than that observed in the IM group (Suppl. Table S2). Lesions were characterized by mononuclear (lymphohistiocytic) interstitial inflammation, alveolar histiocytosis, type II pneumocyte hyperplasia, and fibrin deposition within alveolar septa and lumina (Fig. 8a). Alveolar macrophages and pneumocytes were strongly immunoreactive to MACV antigen (Fig. 8b).
In the aerosol-challenged macaques, neurologic lesions were similar to the IM group in those animals that died 21 days postexposure or before. In the macaque that succumbed on day 13, no observable neurologic lesions were noted. In 5 macaques (aerosol challenged) that either died close to the end of study extension (34 days postexposure) or survived, mild-to-moderate nonsuppurative encephalitis or gliosis was observed (Fig. 12a). Of the 4 survivors, 1 had strong IHC staining in neurons and a small number of glial cells that were collocated with inflammatory cells (Fig. 12b). In the macaque that succumbed on day 34, abundant IHC staining was also noted within neurons and rare glial cells that were amid inflammatory cells within the brain. In the 3 other remaining end-of-study survivors, weak or very rare positive IHC staining was observed within glial cells, within glial nodules, or within endothelial cells or cells of the choroid plexus. The 4 survivors appeared clinically normal, but dominant residual lesions were present within the cerebrum and cerebellum.
Signs of lymphoid replenishment and repopulation in the spleen and lymph nodes indicated immunologic convalescence in aerosol-challenged survivors. Interestingly, macaque 16F (aerosol challenged), which died at 34 days postexposure, displayed a wide range of lesions, including signs of ongoing cell death, lymphoid recovery, and neurologic lesions, in a pattern somewhere between those that died at or before 21 days postexposure and those that survived to the end of the study extension (all aerosol challenged).
Discussion
Viral hemorrhagic fevers, including BHF, are devastating diseases that we know little about and for which there are no Food and Drug Administration (FDA)–approved treatments. Because efficacy studies involving treatments and vaccines for a number of severe and/or rare diseases, including viral hemorrhagic fevers, are neither ethical nor feasible using human subjects, the FDA adopted a regulation referred to as the “Animal Rule.” 10 This rule permits approval of countermeasures for infectious diseases or diseases caused by chemical or radiological agents based on animal studies when human efficacy studies are not possible. 38 The results of this study are meant to serve as a baseline for further development of a macaque model of MACV infection to evaluate life-saving medical countermeasures against BHF resulting from outbreaks or accidental or intentional exposure.
Previous MACV studies in nonhuman primates (NHPs) performed at USAMRIID and elsewhere used the Carvallo strain. In our hands, the Carvallo strain was not lethal in Hartley guinea pigs without adaption by serial passage of the virus through guinea pig spleen, but the Chicava strain was lethal without adaption to guinea pigs or serial passage through mouse suckling brain. Our aim for development of animal models of arenavirus infection is to use, when possible, the same virus strain for rodents and NHPs to enable more direct comparisons between these models. Thus, the Chicava strain is the MACV virus strain that is closest to human clinical specimens currently available at this institute.
The clinical picture of MACV disease in macaques mimics that seen in human cases of MACV infection in South America. 5,6 In humans, the incubation period is 7 to 14 days and can be as disparate as 5 to 21 days, with onset of disease beginning with the nonspecific symptoms of malaise, myalgia, fever, headaches and dizziness, and skin sensitivity. 5,6 The macular rash of the skin and petechiae within the gastrointestinal tract, including the oral cavity, begins to appear after a few days of clinical illness, and disease progresses, leading to loss of intravascular fluid and hypovolemic shock. In patients with MACV infection, systemic inflammation leads to vascular leakage and coagulation throughout the body without large-scale destruction or loss of erythrocytes. 5,20 Blood loss is not a major factor in human cases of MACV infection, but loss of clotting factors and increased bleeding times are major factors. Leukopenia and thrombocytopenia commonly occur in patients with MACV infections. 5,6,29,39 Renal function in patients infected with MACV normally remains intact until end-stage disease with renal failure attributed to hypovolemia. 5,6 The combination of thrombocytopenia and hypovolemia is a common finding in other viral hemorrhagic fevers. 3,5,20
In the our studies, the incubation period of MACV infection in macaques ranged from 6 days in the IM-challenged macaques to 10 days in the aerosol-challenged macaques (6- to 10-day incubation period overall) . In all challenge groups of this study, signs of MACV infection (eg, macular rash of the skin and petechiae in the gastrointestinal tract, hypovolemic shock) and disease progression were similar to patients with BHF.
In select macaques infected with MACV in this study, the loss of platelets that compromised clotting, vascular leakage, and renal failure were similar to that seen in MACV-infected patients. Platelet counts decreased markedly in those macaques that succumbed to disease, and in general, platelet counts decreased in all macaques to a modest extent. CBCs from all macaques revealed an initial leukopenia (at least a moderate decrease in monocytes, neutrophils, and lymphocytes) until approximately day 14 postchallenge. At this point, some macaques had a rebound in all cell lines. Nonsurvivors generally had minimal leukocyte rebound and often succumbed to MACV disease by days 20 to 21 (data not shown). The time from disease onset to death in human cases is between 7 and 12 days, 6 and the disease course in these macaques was similar. MACV was also present within the bone marrow progenitor cells and megakaryocytes as noted by IHC immunoreactivity. Viral tropism for these progenitor cells in the bone marrow helps to explain decline of these cells and subsequent thrombocytopenia and leukopenia.
Clinical chemistry data revealed marked increases in AST and ALT and moderate increases in ALP in macaques that succumbed to infection, which correlates with the multifocal areas of cell death seen histologically within the liver. TP also decreased in all macaques, and decreases in ALB were a major contributing factor. These findings resemble the vascular leakage and protein loss seen with other viral hemorrhagic fevers, 3,20 with the hepatic damage most likely limiting ALB and possibly clotting factor production and contributing to the overall decrease in TP. Through the help of electron microscopy, cytoplasmic basophilic spheres in areas of hepatic damage were examined and consisted of prominent inclusions comprising masses of tightly packed ribosomes that are consistent with previously reported inclusions for arenaviruses. 31 Although individual virions were not observed, the presence of inclusions strongly supports viral activity. Histologically, similar viral inclusions were noted in the cytoplasm of cells both within the adrenal cortex and pancreatic islets.
In addition, neurologic manifestations after a few days of clinical illness are common findings in patients infected with MACV. 5,6 Progressive and debilitating neurologic signs often begin with headaches, dizziness, and photophobia and can progress to tremors. These neurologic signs often culminate in seizures, coma, and death. 5 In patients, MACV infection can manifest with neurologic symptoms, hemorrhage, or both, and the macaques in this study demonstrated these same clinical manifestations of disease. 5
Our survivors were reported to be clinically normal even though several macaques had appreciable inflammation and MACV antigen within the cerebrum and cerebellum. In previous studies, a “2-phase” disease was observed in rhesus and cynomolgus macaques challenged subcutaneously with hamster-adapted Caravallo strain of Machupo virus. 9,25,30,40 These studies characterized MACV disease progression in macaques by an initial acute phase beginning at 7 to 10 days postexposure with death occurring generally by the end of week 3. Clinical improvement in survivors of the acute phase occurred around day 21 and progressed for a subsequent 7 to 10 days. Beginning as early as day 26 and as late as day 40, most of the macaques surviving the first phase developed severe neurologic disease and succumbed to this “second phase” of disease. 9,25,30,40 In our experience with the Chicava strain, 1 macaque surviving the first phase of disease succumbed on day 34, during the second phase. The other 4 surviving macaques appeared clinically normal at the study end points, but some had immunohistochemical evidence of strong, specific, intracytoplasmic staining of neurons for MACV antigen in combination with chronic inflammation. Due to study end-point restrictions, data are not available on disease progression in survivors, so it is unknown if recrudescence mimicking the “second phase of disease” would have occurred. Future studies with longer study intervals may be needed to answer this question. In contrast to macaques, recovery from BHF in humans is often complete with a lack of long-term neurologic sequelae. 5
Based on immunohistochemical staining in combination with histomorphologic analysis, monocytes, macrophages, and dendritic cells appear to be a primary site of MACV infection. Infection in this case does not necessarily denote viral replication in these cells as antigen may have been taken up as part of the immune response. These cells demonstrate strong immunoreactivity in lymph nodes, in the spleen, within the vasculature of almost all organs (monocytes), within occasional Kupffer cells, and within the lung (alveolar macrophages). Other viruses that cause viral hemorrhagic fevers, such as Ebola and Marburg viruses, display similar cellular tropism for monocytes, macrophages, and dendritic cells. 13 –15
In addition, lymphocytes undergo cell death in all lymphoid organs but do not appear to be actively infected based on immunohistochemistry. Again, as with Ebola and Marburg hemorrhagic fevers, lymphocyte death is suggested to be a bystander event resulting from the release of apoptosis-inducing cytokines by actively infected macrophages and dendritic cells. 3,14
Epithelial cells also appear to be a prominent target of the virus. Such cells within the tongue, submandibular salivary gland, esophagus, lung, stomach, small intestine, large intestine, liver, adrenal gland, pancreas, and skin demonstrated histologic evidence of degeneration and cell death with concomitant strong positive MACV immunohistoreactivity indicating virus causality. The propensity for MACV to infect epithelial cells, especially those of the gastrointestinal tract and the bone marrow, may be due to the virus entry receptor, the transferrin receptor, expressed on these cells. 34,36 Interestingly, the transferrin receptor is expressed at much higher levels on cells that are rapidly dividing, and this may help to explain the previously mentioned viral antigen localization. 34
Our findings indicate that MACV infection causes a cascade of events during aerosol and IM exposures, and this cascade appears to follow the course of disease seen in human patients. Current evidence suggests that aerosol MACV exposure in macaques leads to infection of epithelial cells within the oral cavity and respiratory tract via the transferrin 1 receptor. In addition, MACV infection of resident macrophages and dendritic cells leads to systemic dissemination of the virus via the lymphatic systems followed by vascular dissemination, seeding of organs, and infection of parenchymal cells. MACV replication in mononuclear cells heralds the release of chemokines/cytokines, and this release leads to immune dysregulation, death of lymphocytes via apoptosis, and subsequent cell death of macrophages and dendritic cells. Virus replicates within epithelial cells, leading to loss of mucosal integrity. Within the bone marrow, viral replication with loss of progenitor cells contributes to leukopenia and thrombocytopenia. Systemic infection and inflammation promote vascular leakage and subsequent hypoproteinemia.
In advancing disease, diarrhea, dehydration, and mucosal ulceration of gastrointestinal and respiratory system as well as ulceration of the haired skin become evident. A combination of systemic inflammation, immune dysregulation, multiorgan infection and cell death, thrombocytopenia, dehydration, and secondary bacterial infection culminates in death in the acute phase of MACV infection. Encephalitis and death occur later in a subset of initial survivors of the acute phase. Renal function normally remains viable until end-stage disease, with renal failure attributed to hypovolemia.
Conclusion
Currently, there are no FDA-approved treatments or vaccines for Bolivian hemorrhagic fever, a highly lethal hemorrhagic fever that is a risk to national security and public health as denoted by the NIAID Category A designator. Because of this, development of an appropriate animal model is the crucial first step in developing an effective vaccine or treatment. This study demonstrates that the cynomolgus macaque is an excellent model of the human MACV disease as the incubation period, clinical signs, disease progression, and clinical pathology findings closely mimic those seen in humans We recommend further development of this model so it can act as a crucial bridge to test and evaluate vaccines, therapeutics, and diagnostics for human use under the FDA’s Animal Rule. We also advocate pathogenesis studies in this model and other models to clearly define the progression and nature of disease caused by MACV to further our understanding of this highly lethal virus. Such studies could include IHC staining for both MACV and an apoptosis marker to clearly delineate tissue and cellular tropism and mechanism of cell death, or studies of MACV viral entry via the transferrin receptor 1.
Footnotes
Acknowledgements
We gratefully acknowledge the numerous contributions of USAMRIID’s pathology personnel, including William Aguilar, Alejandro Barajas, Taylor Chance, Neil Davis, Paul Facemire, Phil Fogle, Angela Grove, Shelley Honnold, Gale Krietz, Kathleen Kuehl, Bridget Lewis, Christine Mech, Brandon Meng, Don Nichols, Jo Lynne Raymond, Nancy Twenhafel, and Brandon Wilke. We also thank members of USAMRIID’s Virology Division—Anna Honko, Heather Esham, Joshua Shamblin, Ginger Donnelly, and Joshua Johnson—for help with phlebotomy and/or animal observations; Chris Reed for helpful discussions regarding transmission electron microscopy; and members of the Center for Aerobiological Sciences at USAMRIID for assistance with the aerosol exposures. We thank Laura Bollinger for providing technical writing services and William Discher for assistance with the generation of figures. Cindy Rossi of Diagnostic Systems Division, USAMRIID, kindly provided the polyclonal rabbit serum for immunohistochemistry. We are grateful for the contributions of Samuel Dickson from USAMRIID who performed the statistical analysis. Finally, we acknowledge the Special Pathogens Branch of the CDC for providing USAMRIID with the original sample containing the MACV Chicava strain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The views, opinions, and/or findings contained herein are those of the authors and should not be construed as an official Department of Army position, policy, or decision unless so designated by other documentation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research was performed under USAMRIID project number 195743 and was funded by a Defense Threat Reduction Agency, Joint Science and Technology Office (DTRA/JSTO) Translational Medical Technologies (TMT) grant TMTI_0045_09_RD_T.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.