
Abstract
The common marmoset (Callithrix jacchus) is a New World primate that is used in biomedical research due to its small size and relative ease of handling compared with larger primates. Although bone disease in common marmosets is well recognized, there are very few detailed descriptions in the literature that cover the range of lesions seen in these animals. For all animals used to model human disease, it is important to be aware of background lesions that may affect the interpretation of study findings. This retrospective study details bone diseases encountered in marmoset breeding colonies at 2 different institutions. Affected marmosets at Johns Hopkins University had lesions compatible with diagnoses of rickets, fibrous osteodystrophy and osteopenia. Affected marmosets at the Wisconsin National Primate Research Center exhibited severe lesions of osteoclastic bone resorption and remodeling that had an unusual distribution and were not easily categorized into a known disease entity. The purpose of this report is to document these naturally occurring skeletal lesions of common marmosets and suggest an approach to evaluating skeletal disease in prospective studies of these animals that will allow the most accurate diagnoses.
Keywords
The common marmoset (Callithrix jacchus) is a New World primate indigenous to Brazil that achieves an adult weight of only 350 to 450 g, making it the smallest nonhuman primate commonly used in biomedical research. 1,10,16 The success of captive breeding programs, coupled with short generational times and the ease and safety of handling, makes common marmosets particularly desirable for research studies. Sexual maturity typically occurs between the ages of 16 and 25 months. 14 Epiphyseal closure in the distal humerus occurs at approximately 6.6 months of age, and termination of bone growth is complete with the closure of the ischial tuberosity at an average age of 22.6 months. 15 Common marmosets are used to model bone diseases, including osteoporosis. However, the results of these studies may be influenced by naturally and commonly occurring bone disease and by peculiarities of bone metabolism, including target-organ receptor resistance to the active form of vitamin D3, 1α,25-dihydroxyvitamin D3 (1α,25(OH)2D3). 20,25,31 In addition, our group and another have recently demonstrated a link between bone disease and gastrointestinal disease and weight loss, suggestive of marmoset wasting syndrome (MWS), 3,12 which is highly prevalent in marmosets at Johns Hopkins University (JHU).
Perhaps the most common bone disease reported in marmosets is vitamin D–dependent rickets type II. 31 Reported radiographic lesions included kyphosis, decreased bone density, bone fractures, subperiosteal bone resorption in the bones of the hand, and a lack of lamina dura (alveolus) of the tooth sockets. The reported histological features included increased amount of osteoid, an increased number of osteoclasts, subperiosteal osteoclastic bone resorption, and, in 1 animal, myelofibrosis involving trabecular bone. 31 Other reports describe a marmoset with idiopathic myelofibrosis associated with trabecular and cortical bone remodeling accompanied by prominent osteoclasts and woven bone 13 and another with osteomalacia and metabolic bone disease. 11 Spontaneous bone diseases reported in surveys of marmoset colonies include osteodystrophy, fibrous osteodystrophy, osteoporosis, osteopenia and myelofibrosis, and osteopathy. 5,7,19,23,28 Unfortunately, few of these reports include descriptions of the lesions or the criteria used for diagnosis. Whether or not the various bone lesions observed in common marmosets represent separate and distinct disease entities or a disease complex with multiple causes that differ among cases is unclear.
Necropsy examinations of animals from the longstanding marmoset colonies at JHU and the Wisconsin National Primate Research Center (WNPRC) have produced an archive of marmoset disease cases. Our aims were to (1) determine if bone disease in common marmosets can be categorized into separate disease entities that can be distinguished based on the type, severity, and distribution of lesions present and (2) suggest an approach to evaluate bone disease in common marmosets.
Materials and Methods
Study Animals, Housing, and Diet
WNPRC and JHU are accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International (AAALACi). All animals were members of biomedical research colonies and were housed in family units, in pairs, or individually. The colony at WNPRC was closed (no introductions of new marmosets from the outside either previous to or during the 9-year period in which the animals were studied), but new animals were periodically introduced to the JHU colony.
WNPRC marmosets were fed a component diet consisting of 38 g/d of a commercial marmoset diet (ZuPreem 9920 CS canned marmoset diet; ZuPreem, Shawnee, KS), containing approximately 4770 IU vitamin D3/kg dry matter (DM) basis. The canned marmoset diet was top-dressed with yogurt containing added Provim and Nutra-Plus vitamin/mineral/protein supplements (Nutra-Vet Research Corporation, Poughkeepsie, NY); however, dominant animals likely received more of the yogurt. JHU marmosets were fed approximately 25 g per 350 g of body weight of a complete and balanced diet consisting of a custom homogenized blend of Teklad 8794 N New World Primate Diet (Harlan Laboratories, Indianapolis, IN), ZuPreem 9920 CS canned marmoset diet (ZuPreem), and Bio-Serv Newberne Hayes Vitamin Mix (Bio-Serv, San Diego, CA) (estimated to contain 8200 IU vitamin D3/kg DM). Diets at both institutions were supplemented with fruit, yogurt, and other enrichment items, and water was provided ad libitum. Animal care and experimentation were conducted in accordance with all relevant local, state, and national regulations, using protocols approved by the appropriate Institutional Animal Care and Use Committees.
Historical Information
The bone lesions were first recognized in individual animals as an incidental finding during survey radiography prior to enrollment in a clinical study (WNPRC) or as a femoral fracture of unknown etiology (JHU). This resulted in periodic radiographic evaluation of all marmosets in both colonies. Over a period of 9 years, 24 animals were identified with bone disease at WNPRC from a colony of approximately 280 (8.6% prevalence over 9 years), whereas, over a similar time period, 38 animals from a colony of approximately 296 were identified at JHU (12.8% prevalence over 9 years). Study of the marmoset colony at JHU led to the discovery of a strong correlation between lesions of gastrointestinal disease considered typical of marmoset wasting syndrome (MWS), the hallmark of which is chronic lymphocytic enteritis, and bone lesions in the JHU colony. 3 As discussed in more detail in Baxter et al, 3 the combination of bony lesions and gastrointestinal disease was most closely associated with antemortem findings of low albumin and decreased body weight (<325 g), although increased parathyroid hormone (PTH) levels also were associated with bone disease. Specifically, serum levels of PTH were higher in animals with a histologic diagnosis of fibrous osteodystrophy (FOD) (mean ± standard error of 2176 ± 936.2 pg/ml, Kruskal-Wallis P < .05) or osteopenia (1777 ± 650.5 pg/ml, P < .05) than animals with no bone disease (254.2 ± 70.21 pg/ml), but these groups (FOD and osteopenia) did not significantly differ from one another. 3 Levels of serum vitamin D were measured in several animals in an attempt to compare clinically normal with affected animals. Unfortunately, histopathologic analysis later identified lesions consistent with FOD in several of the clinically normal animals. Thus, there were insufficient data from unaffected animals to allow useful comparisons (results not published).
Necropsy Methods
Complete necropsy examinations, including histological evaluation of the major organs, were done on 12 of the 24 affected WNPRC animals and on 65 JHU animals (both affected and unaffected). 3 The animals were humanely euthanized due to disease or at the termination of an experimental study with either an injection of intravenous sodium pentobarbital solution (Beuthanasia-D Special; Schering-Plough Animal Health Corp., Kenilworth, NJ) or an intraperitoneal injection of Euthasol (Virbac Corporation, Fort Worth, TX) after being anesthetized with 40 mg/kg ketamine administered intramuscularly.
Specimens of bone (long bones in all cases; scapulae, vertebrae, and metatarsals in some cases) were saved from 7 of the 12 WNPRC cases (6 females and 1 male) and included affected and contralateral unaffected sites for most cases but were not collected according to a standardized protocol. These were fixed in 10% neutral buffered formalin and sent to the University of Minnesota College of Veterinary Medicine where dorsoventral (DV) and lateral radiographs were taken of all fixed bone specimens using a cabinet radiography unit (Faxitron series; Hewlett Packard, McMinnville, OR) and high-detail film (X-Omat TL; Eastman Kodak Company, Rochester, NY). After radiography, the bone specimens were decalcified in 10% EDTA and processed for histological evaluation. Representative longitudinal and cross sections of bone were prepared from each site containing a radiographic lesion and, when available, matching sites from the contralateral unaffected extremity. Routine paraffin-embedded histological sections (Tissue-Tek; Sakura Finetek U.S.A. Inc., Torrance, CA) were cut at 5 μm and stained with hematoxylin and eosin (HE). Selected histological sections were stained with tartrate-resistant acid phosphatase (TRAP) (Sigma Chemical Company, St Louis, MO; Aldrich Chemical Company, Milwaukee, WI) for the identification of osteoclasts or Gomori’s One-Step with Aniline Blue Trichrome stain kit (Newcomer Supply, Middleton, WI) for the identification of fibrous connective tissue.
For the JHU studies, selected bones from variable anatomic locations were stripped of soft tissue, decalcified in formic acid, and processed routinely for paraffin embedding. Tissues were sectioned at 5 μm and stained routinely with HE.
Blood was collected from 16 of 24 affected WNPRC marmosets for complete blood count, serum chemistry panels, and other analytes, including ionized calcium, vitamin D, and free PTH. Complete blood counts were analyzed in-house while serum chemistry panel and other analyte results were obtained through contract reference laboratories (General Medical Laboratories, Meriter Hospital, Madison, WI, and Animal Health Diagnostic Laboratory, Michigan State University). Serum chemistry results for the JHU marmosets were published previously 3 and are summarized in the Results.
Results
Marmosets at WNPRC
Sixteen of the affected animals were females and 8 were males. The mean age at which clinical signs first became apparent, or at which the disease was first diagnosed radiographically, was 24.4 months (range, 8–79.2 months). All but 4 (20/24) of these animals had a body weight ≥325 g at the time of death (mean body weight 382 g; range, 294–545 g). Five of the 16 affected females first exhibited signs of disease during pregnancy, but each of these animals had prior and/or subsequent pregnancies during which they were free of radiographic lesions. In other affected animals, the lesions were observed to wax and wane over time. Seventeen of the 24 affected animals were from multiple offspring within a single-family unit, including 1 pair of twins and 2 siblings from a single group of triplets. In 1 family, 5 of the 26 offspring of the same parents developed bone lesions during the 9 years of the study. Another family had 4 affected offspring from the same father, with 2 affected animals from each of 2 different mothers. There was also 1 case of an affected mother-daughter pair as well as several isolated offspring from different families with no affected siblings.
A review of the necropsy reports from the 12 animals that received a complete necropsy examination revealed that the most common soft tissue findings included lymphocytic enteritis (62% of the cases) and lymphoplasmacytic interstitial nephritis (31% of the cases). Extramedullary hematopoiesis was also commonly observed in the adrenal gland, liver, kidney, and spleen (27% of the cases). None of the necropsy records mentioned lesions involving the parathyroid gland, but 4 animals had lymphocytic thyroiditis and 1 had adenomatous hyperplasia of a thyroid gland. Clinical chemistry results in affected animals were similar to those from animals with no radiographic lesions or clinical signs detected and were determined to be within normal limits for marmosets. 33 Briefly, these included the following (mean [range]): intact PTH = 14.57 pmol/L [3.1–54.7]; vitamin D, all >250 nmol/L; ionized calcium = 1.34 mmol/L [1.03–1.49]; alkaline phosphatase = 156 mU/ml [66–312]; calcium = 10.5 mg/dL [8.6–11.9]; phosphorus = 5.8 mg/dL [3.3–6.8]; and Ca to P ratio = 2.2 [0.8–3.6].
The extent and location of the radiographic lesions varied markedly. Most commonly, lesions were seen in long bones, including the humerus, radius, ulna, femur, tibia, and fibula. Less commonly, lesions were present in the vertebrae, cranium, scapulae, pelvis, and tarsal bones. The radiographic lesions were most often unilateral but occurred bilaterally in about 20% of the cases and were of 2 different morphological types. One type was characterized by severe, localized, or locally extensive areas of radiolucency that tended to be well demarcated and often were present throughout an entire bone or several contiguous bones. These were accompanied by marked cortical thinning and focal or multifocal full thickness loss of cortical bone (Figs. 1, 2). The second type was characterized by locally extensive to widely disseminated multilocular expansion of either a portion of a bone or an entire bone, resulting in an increase in the diameter that was sometimes greater than twice the diameter of the corresponding unaffected contralateral site (Figs. 3, 4). Clinical reports and radiographs from these animals clearly indicated that lytic lesions could develop into expansile lesions over time in individual animals.
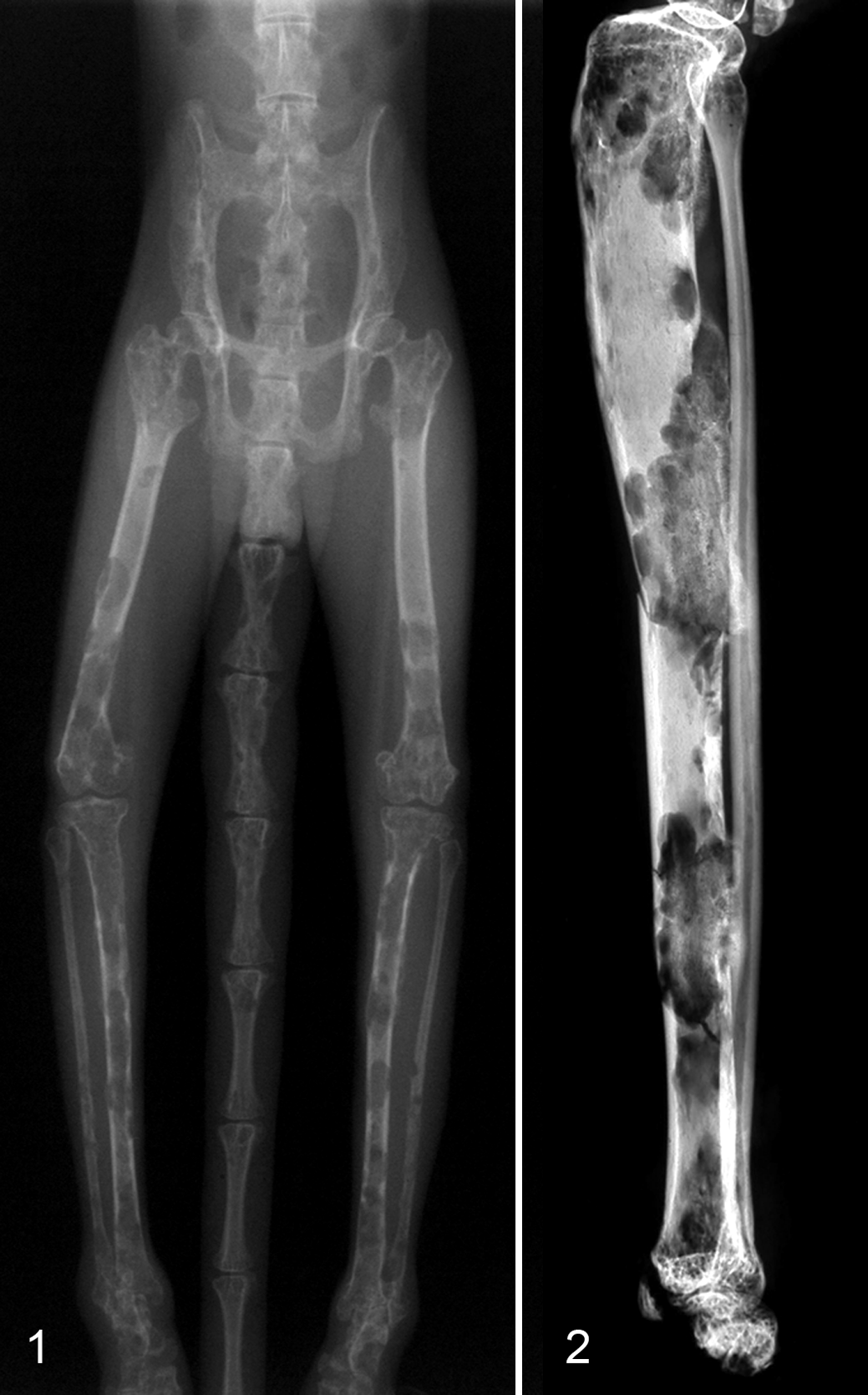
Bone, common marmosets. Wisconsin National Primate Research Center colony.

Bone, common marmosets. Wisconsin National Primate Research Center colony. Same animal.
Interestingly, some of the animals had severe lesions that were restricted to 1 or 2 bones, with an immediately adjacent bone having no lesions (e.g., radius and ulna affected but humerus normal) on routine clinical radiography. However, ex vivo radiographs revealed involvement of bones that appeared normal on routine clinical radiographs (Figs. 3, 4).
Similar to the radiographic lesions, the histological lesions also were of 2 distinct morphological types. The histologic changes in bones containing areas of radiolucency (Figs. 1, 2) were characterized by areas of marked osteoclastic bone resorption, primarily involving endocortical bone. The lesions in some sections were strikingly severe (Figs. 5, 6), containing myriads of osteoclasts (up to 20 per 40× field) that were closely associated with resorption lacunae in cortical, trabecular, and subchondral bone. Sites of endocortical osteoclastic resorption often contained corresponding areas of periosteal new bone (Fig. 6). In some areas, presumably representing a more chronic process, areas of cortical lamellar bone were replaced by woven bone. TRAP-stained sections revealed positive staining of multinucleated osteoclasts adjacent to bone surfaces, as well as large numbers of uninucleate cells within the marrow cavity that were presumed to be osteoclast precursors (Fig. 7). In general, the marrow spaces in sites containing lytic lesions were highly cellular (Fig. 8). In some of these sites, the cells were composed entirely of hematopoietic cells exhibiting normal maturation, while in others, the cells were composed primarily of mature granulocytes accompanied by large numbers of megakaryocytes and small numbers of erythroid precursor cells (Fig. 8). Although minimal collagenous connective tissue appeared to be present in marrow spaces in the lytic lesions based on the HE sections, myelofibrosis was not confirmed in trichrome-stained sections (no or minimal trichrome positivity in these areas) (Fig. 9). No bacteria or viral inclusions were observed in any of the sections examined.
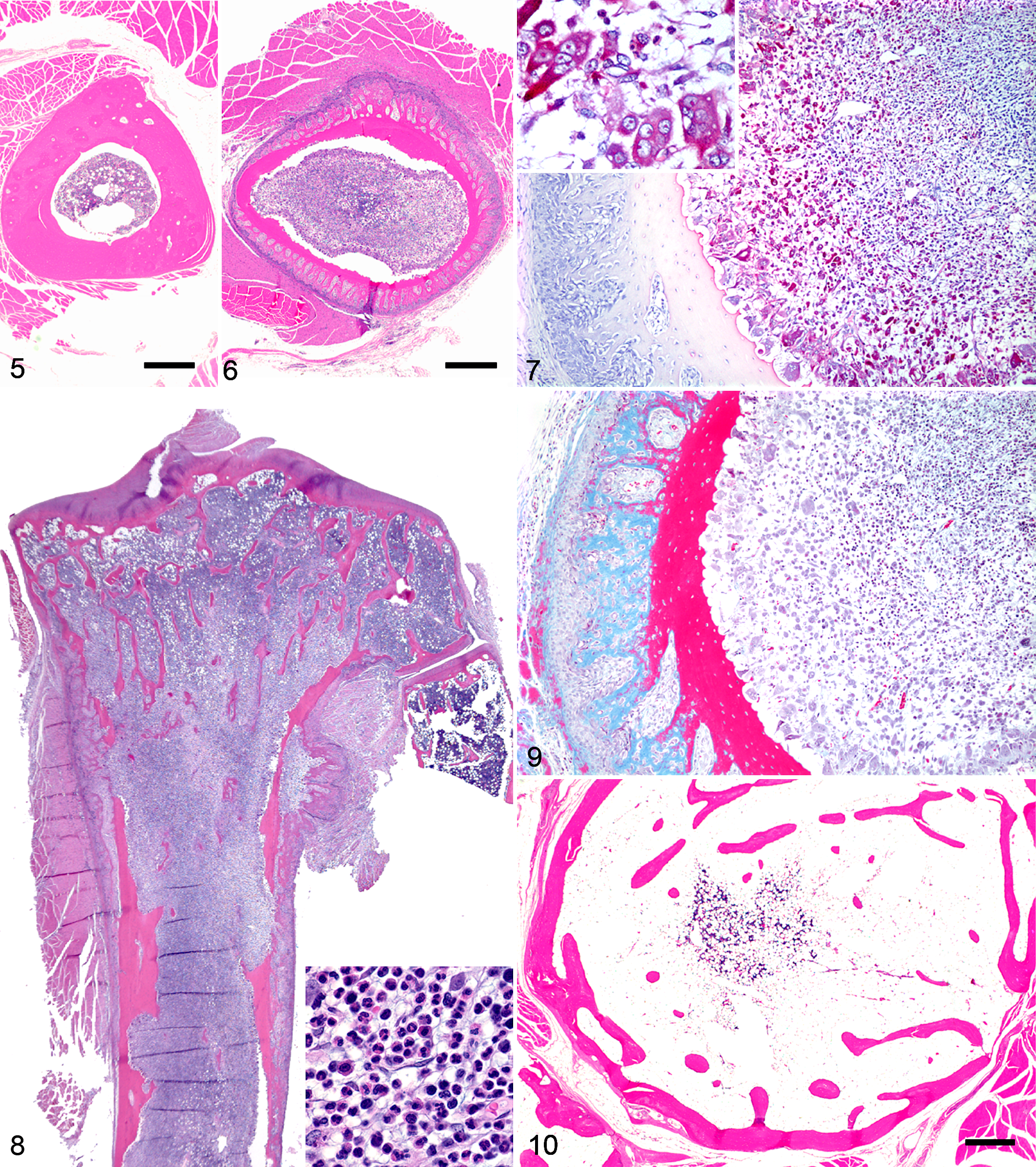
Bone, common marmoset. Wisconsin National Primate Research Center colony.
The histological changes in bones from sites characterized radiographically by multilocular expansion of cortical bone had histological changes that were characterized by marked replacement of cortical lamellar bone by trabecular woven bone and a marked increase in bone diameter (Fig. 10). Osteoclastic bone resorption was not a prominent feature of these lesions and often was completely absent. In general, the bone marrow in these sites was hypocellular and contained low numbers of hematopoietic cells with normal maturation and a moderate to large amount of adipose tissue and, in some cases, a minimal amount of fibrillar connective tissue. Marrow spaces in trichrome-stained sections of these expansile lesions were negative or weakly positive.
Lytic lesions and proliferative/expansile lesions were sometimes observed in the same histological section, and some sections that were taken from radiographically normal sites contained mild histological lesions of either type.
Marmosets at JHU
Bones were examined histologically from 65 animals, ranging in age from 6 months to 15 years. Thirty-eight animals had histological evidence of bone disease (20 females, 17 males, and 1 of unrecorded sex) and 27 did not (11 females, 15 males, and 1 of unrecorded sex). Chi-square analysis revealed no association between sex and disease status (P = .45). The number of affected animals (38 of 296 animals in the colony) is likely an underestimate because bones were not evaluated from all animals necropsied. Animals with evidence of bone disease ranged in age from 6 months to 16 years (mean age, 4.0 years) and animals with no evidence of bone disease ranged in age from 6 months to 7 years (mean age, 3.9 years). With the exception of the index case, all animals diagnosed with bone disease antemortem were discovered during routine radiography or during clinical workup for MWS.
The bone lesions identified in the JHU colony could be divided into 3 disease categories that included rickets, FOD, and osteopenia (radiographic lesions shown in Figs. 11–15), albeit with some degree of overlap among these. Rickets was diagnosed in 6 of the 12 marmosets that had open growth plates (mean age, 7.8 months). Radiographic lesions of rickets, identified in 3 cases, were characterized by physes that were 2 times or greater thickness than those of age-matched controls and a variable degree of metaphyseal flaring in some cases (Figs. 11, 12). Histologically, these 3 cases had a markedly widened zone of hypertrophic chondrocytes within the growth plates (Fig. 16). Three additional animals that did not have radiographic lesions of rickets had histological changes that included a disorganized cellular arrangement in the growth plates, with increased numbers of hypertrophic chondrocytes, that resulted in a focal or diffuse increase in thickness of the affected growth plates. In most cases (n = 5/6), there was also locally extensive retention of hypertrophic chondrocytes within the primary spongiosa with failure of endochondral ossification at the affected site.
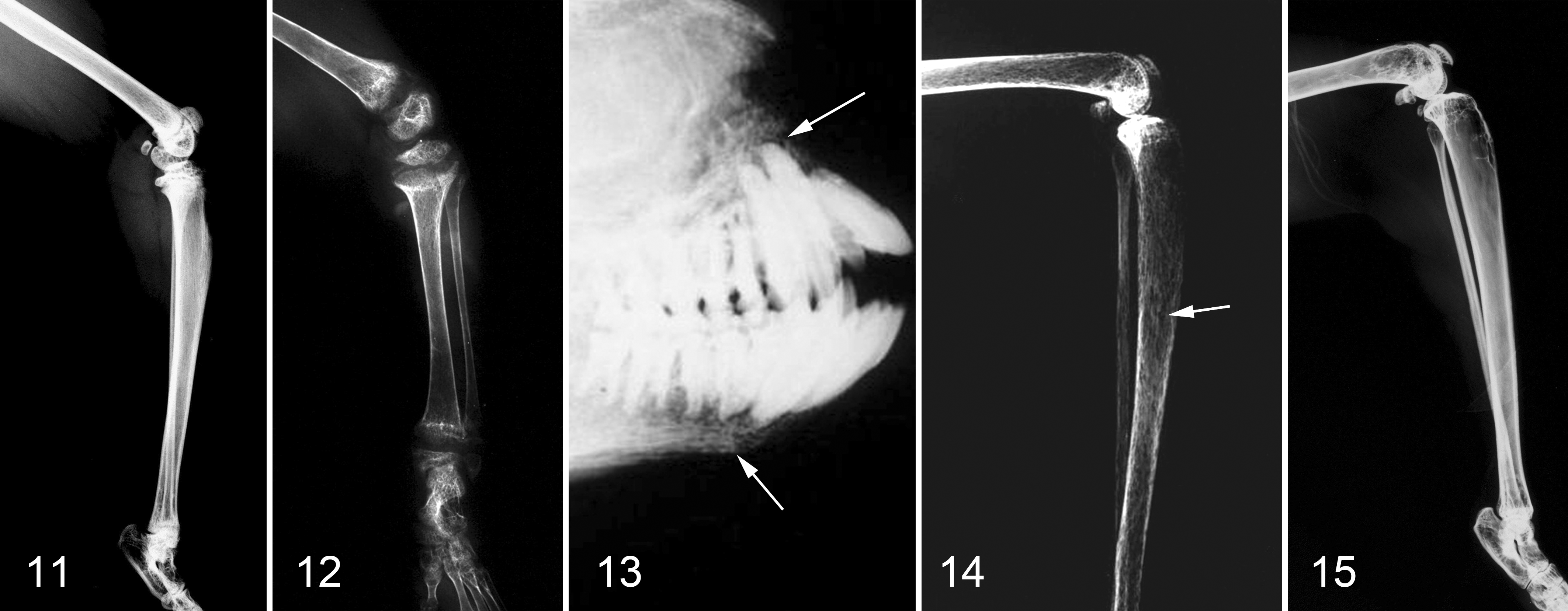
Common marmosets. Johns Hopkins University colony. Radiographs depicting features associated with postmortem histologic diagnoses.
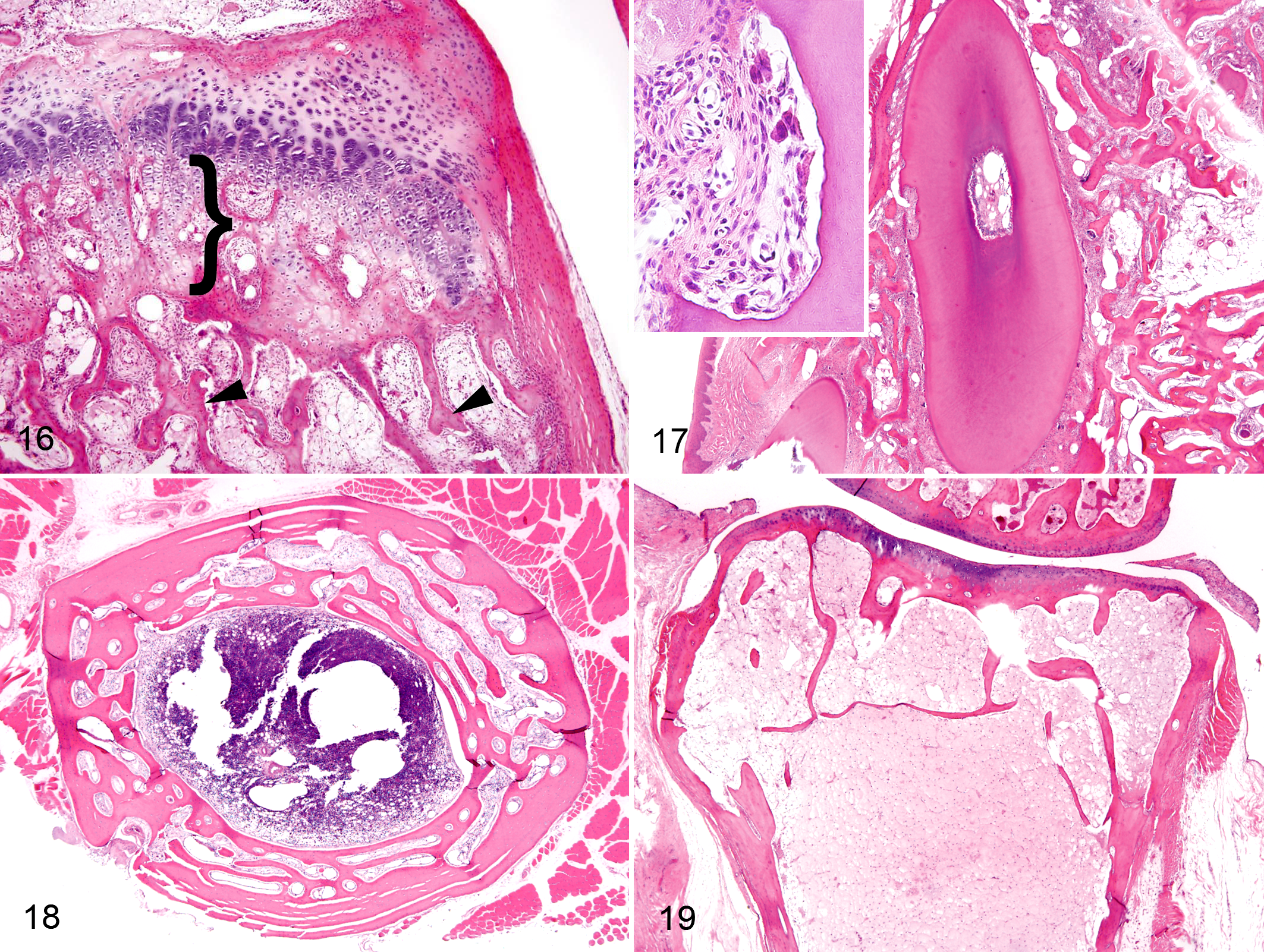
Bone, common marmosets. Johns Hopkins University colony. Hematoxylin and eosin (HE).
Animals assigned a radiographic diagnosis of FOD (n = 5, mean age 72 months) exhibited multifocal areas of radiolucency or “moth-eaten” appearance in the cortex and medulla involving multiple bony sites. This lesion was most obvious in long bones, extending from metaphyses through diaphyses, but also included mandible, maxilla, and vertebrae in some cases (Figs. 13, 14). All animals having this radiographic pattern, as well as 13 additional animals in which this diagnosis was based on histological changes alone, had histological lesions characterized by increased numbers of osteoclasts within erosion lacunae (osteoclastic osteolysis, 100% of cases), peritrabecular fibrosis (72% of cases), cortical trabeculation (83% of cases), incomplete dental alveoli/tooth sockets (33% of cases), endosteal resorption (67% of cases), and periosteal new bone formation (56% of cases). Increased osteoclast numbers were evidenced by the presence of 3 to 5 osteoclasts lining erosion lacunae per high-power field in 2 or more locations in the section.
Peritrabecular fibrosis was defined as increased amounts of finely fibrillar to more densely collagenous connective tissue surrounding trabeculae and occasionally extending into marrow cavities. These areas were present in sites of bone resorption and usually were accompanied by foci of cuboidal (presumably active) osteoblasts. The most severely affected sites tended to be located in sections of skull, in which bone was often extensively replaced by primitive fibro-osseous tissue (Fig. 17). Cortical trabeculation was characterized by increased porosity of cortical bone due to replacement by trabecular woven bone (Fig. 18).
The absence of complete dental alveoli (tooth sockets) in the mandible or maxilla due to multifocal or diffuse absence of alveolar bone was a less common feature but tended to be quite striking when present. These sites were characterized by the presence of isolated spicules of bone that were surrounded by fibrous tissue and plump fibroblasts (Fig. 17). Increased numbers of osteoclasts were sometimes present in these areas and included odontoclasts in the most severely affected cases (Fig. 17 inset). Endosteal resorption was characterized by an undulating or scalloped endosteal surface with or without the presence of osteoclasts. This was often associated with decreased cortical thickness and/or overall reduced amount of bone (osteopenia). Periosteal new bone formation was characterized by a focal or diffuse increase in periosteal osteoblast numbers accompanied by foci of new bone, often resulting in an irregular cortical surface.
The third disease category that was identified in these animals was osteopenia, which was characterized radiographically in 4 animals (mean age 43.4 months) by a generalized, diffuse decrease in radiodensity involving the cortex and medulla of all bones (Fig. 15). In all cases identified radiographically, histological examination revealed a diffuse decrease in cortical thickness. An additional 27 animals were diagnosed histologically with osteopenia (n = 31) based on agreement among 3 pathologists with experience evaluating bone tissue from marmosets (C.S.C., E.J.O., and G.C.S.) that the amount of cortical or trabecular bone present in the section was reduced relative to what would normally be expected (Fig. 19). This was often accompanied by endosteal resorption and was sometimes accompanied by cortical trabeculation. The diagnosis of osteopenia was made subjectively, as bone densitometry was not done on live animals or on bone samples, and standardized tissue sections were not evaluated using histomorphometry to quantitate bone area.
Importantly, the 3 categories of bone disease that were noted in the JHU animals were not mutually exclusive. In fact, although the diagnosis of rickets was reserved for young animals with open growth plates, all cases of rickets also exhibited histological lesions of FOD and osteopenia. FOD and osteopenia were present concomitantly in adult animals as well, with nearly all animals with FOD also exhibiting osteopenia and approximately half of the osteopenic animals also exhibiting lesions of FOD.
A review of the 65 necropsy reports revealed an association between bone and gastrointestinal disease, which was previously reported. 3 Of the 38 animals with bone lesions, 35 had suspected or confirmed gastrointestinal disease considered typical of MWS. In addition, renal disease was diagnosed in 23 of 38 (60.5%) animals that had bone disease and 19 of 27 (70.4%) animals that did not have bone disease. Lymphoplasmacytic interstitial nephritis was the most common kidney lesion in both groups.
Discussion
Bone lesions were present in both marmoset colonies examined in the present study but appeared to differ between the 2 colonies in severity, distribution, frequency, and natural history. In the JHU colony, 3 different categories of bone disease were present, although these occurred concurrently in many animals. Importantly, the prevalence was lower, the lesions were observed to wax and wane, and the lesions tended to be unilateral in the WNPRC compared with the JHU animals.
FOD only existed in animals that had gastrointestinal disease as defined in Baxter et al. 3 Marmosets (and other New World primates) have unique vitamin D requirements to maintain serum calcium levels and are thus exquisitely sensitive to calcium and vitamin D deficiencies. 11,20,25,27,31 Although it is known that callitrichids require large amounts of vitamin D in their diets, the exact amount required to prevent disease has not been established. The conclusions of several studies vary considerably but, taken together, indicate that a diet that provides 1000 to 3000 IU vitamin D3/kg DM to animals that rely solely on diet for their vitamin D appears to be adequate. 6 The diet fed at JHU included approximately 7800 IU vitamin D3/kg DM, which should have been more than adequate. Although meaningful comparisons between serum vitamin D3 levels in diseased and unaffected animals were not done, it has previously been established that levels of PTH in the JHU marmosets were higher in animals with FOD or osteopenia than in control animals. 3 This finding supports a diagnosis of secondary hyperparathyroidism in the JHU animals, which may be a response to low circulating levels of calcium or vitamin D3 due to impaired gut absorption caused by inflammatory gastrointestinal disease. 3,12 Thus, it is possible that gastrointestinal disease, which is common in captive marmosets, contributes to the development of bone diseases that are frequently encountered in these animals.
In addition to rickets and FOD, which have characteristic radiographic and histological lesions, the JHU marmoset colony included a number of cases that had histological evidence of osteopenia in the absence of other lesions. The subjective nature of this lesion, combined with the difficulty in detecting it via static 2-dimensional radiographs, 17 makes osteopenia a potentially insidious confounding lesion in experimental bone disease. Indeed, there have been many recent studies using the marmoset as a model of skeletal disease and biology, 2,24,29 which clearly could be affected by this background lesion, which appeared to be quite prevalent in the JHU colony. To better address this issue, our group has developed a technique to remove some of the subjectivity from the interpretation of digital radiographs. This technique uses digital image analysis to quantify the radio-opacity of the femur to distinguish animals having evidence of osteopenia from those which do not, 3 allowing the identification and exclusion of animals with radiographically evident, but subtle, bone disease from studies. For a definitive diagnosis of osteopenia, standardized dual-energy X-ray absorptiometry (DEXA) scans would be highly desirable and would detect this lesion much earlier than would static 2-dimensional radiographs, which do not typically reveal osteopenia until there is a reduction of approximately 30% in bone tissue. 9,17
While it was relatively straightforward to diagnose rickets in the JHU animals, osteomalacia (the equivalent of rickets in adult animals) is more difficult to recognize in routine (decalcified) sections of paraffin-embedded bone. Osteomalacia is characterized by an increase in unmineralized osteoid and requires that the tissues be processed without decalcification (usually in plastic) to allow differentiation of mineralized from unmineralized osteoid. In prospective studies in marmosets, undecalcified bone specimens should be collected and used to evaluate the amount of osteoid present in histological sections.
The bone lesions in the WNPRC colony appeared to be different from those occurring in the JHU colony and from other previously described bone lesions in common marmosets. In fact, we were not able to identify a known bone disease in any species, including humans, that closely matched the features seen in these animals. Some considerations included Paget disease, FOD, fibrous dysplasia, and metabolic bone disease secondary to vitamin D deficiency, although each of these is considered unlikely.
Paget’s disease of bone, or osteitis deformans, is a chronic condition of the adult skeleton characterized by localized areas of excessive bone remodeling. The lesion is characterized histologically by large numbers of activated osteoclasts, osteoblasts, and loss of normal lamellar architecture. 18,26,30 Genetic, viral, and environmental etiologies have been suggested, but the cause remains unknown. Although increased numbers of osteoclasts were observed in the WNPRC cases, these cells were not larger than usual (described in Paget disease to contain more than 100 nuclei), 22,30,32 and other characteristics of Paget disease (abnormal osteoclast precursors, distribution of lesions, age of affected individuals, and a slight predominance in males) were not observed in the WNPRC animals. 8,18,22
Fibrous dysplasia (FD) is a common, crippling hereditary skeletal condition that may involve 1 bone (monostotic FD) or multiple bones (polyostotic FD) and usually appears in childhood or adolescence. 4,21 While some of the clinical and radiographic features of FD were compatible with those present in the WNPRC marmosets, the histological features of FD (replacement of normal bone and marrow by an abnormal fibrous tissue within which irregular trabeculae of woven bone are haphazardly distributed) were not. 21
FOD was also considered but was excluded based on necropsy findings (lack of lesions involving parathyroid glands and lack of significant renal disease), the striking severity of the lesions and their tendency to occur unilaterally, evidence for a familial distribution, the fact that the lesions waxed and waned despite a constant diet, the lack of myelofibrosis, and the fact that PTH levels in these animals appeared to be within normal limits. In addition, the lytic lesions in these animals were endocortical and often resulted in full-thickness osteoclastic osteolysis of cortical bone, while the new bone formation was entirely periosteal. An admixture of the 2 processes in the same location (ie, osteoclastic bone resorption accompanied by primitive fibro-osseous tissue), as is seen in typical lesions of FOD, was not appreciated. This topographical separation of bone removal and formation may explain the marked increase in diameter of affected bones in the multilocular expansile stage of the disease, as it appeared that the original cortex was completely removed in the lytic stage of the disease and the new bone in the multilocular expansile stage originated entirely from the periosteal surface.
An influence of gastrointestinal disease on calcium absorption, as has been hypothesized for the JHU marmosets, was considered for the WNPRC marmosets, but this also appears to be unlikely. Although necropsy results revealed the presence of lymphocytic enteritis in 62% of the affected animals, only 4 of 24 (17%) of the animals had a body weight of less than 325 g, failing to support gastrointestinal disease as an important clinical factor in these animals and also differentiating the disease in the WNPRC animals from that affecting the JHU animals, in which a body weight of <325 g was highly predictive of gastrointestinal and bone disease. 3
Finally, due to the unique metabolism of vitamin D in this species, a diagnosis of “metabolic bone disease” as a result of vitamin D deficiency was considered. However, accumulation of excess unmineralized osteoid was not observed in any of the cases (albeit only decalcified sections were examined), and serum 25-hydroxy vitamin D3 levels were similar between affected and unaffected animals. Other factors that were previously discussed also failed to implicate a dietary cause for the disease in these animals, although the combination of diet and genetic factors could not be ruled out.
Conclusion
While the prevalence of skeletal disease likely varies from colony to colony, our findings and those of previous reports 3,11,13,27,31 suggest that thorough musculoskeletal examinations should be included in the management of marmosets. Prompted by these findings, JHU instituted survey radiography as part of a once-yearly wellness check for all marmosets. While this may not be feasible or necessary for other institutions, a full baseline workup, including bone densitometry, should be considered in any study where bony lesions may interfere with experimental results. In addition, care should be taken to ensure that appropriate bone specimens are collected during a complete necropsy examination, including maxilla, mandible, and representative long bones, including associated epiphyses. At least 1 bone sample should be processed without decalcification for the evaluation of osteoid. A serum chemistry panel and serum PTH levels should be assessed to support or rule out a diagnosis of hyperparathyroidism. Clearly, a complete necropsy examination, including histological evaluation of thyroid and parathyroid glands, kidneys, and large and small intestine, should be done to determine if bone disease may be occurring secondary to lesions in these tissues. Finally, but importantly, future prospective studies should take careful note of effects of pregnancy and lactation, housing, diet (particularly changes in diet), lighting, and other environmental factors that may play a role in bone disease in these animals.
Footnotes
Acknowledgements
We gratefully acknowledge the following individuals for their contributions to this project: Ms Anne Undersander and Drs Aric Frantz, Dori Borjesson, and Kari Anderson (University of Minnesota); Drs Amy Usborne, Lisa Forrest, Jan Ramer, James Thomson, and Amanda Goudy-Trainor, as well as Jill Bodden (WNPRC); and Ms Pat Wilcox (JHU).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American College of Laboratory Animal Medicine Foundation and the US Department of Health and Human Services, National Institutes of Health, NIH Office of the Director (grant numbers 2T32OD010993-11 and 5T32OD011089-38).