
Abstract
Canine perivascular wall tumors (cPWTs) arise from vascular mural cells and are included among soft tissue sarcomas (STSs). Most prognostic studies are performed on canine STSs as a general group and regardless of their specific histotype. The aim of this study was to identify pathological parameters and profiles with prognostic impact for cutaneous/subcutaneous cPWTs. Anatomical location, type of growth, surgical margins, and size and depth of the tumor were collected in 56 cPWTs. The association between each pair of variables was evaluated by χ2 test. Multiple correspondence analysis (MCA) was performed to describe the multivariate association of variables and was followed by cluster analysis to identify specific pathological profiles. The prognostic impact of variables and profiles was assessed by Cox regression model. Size and depth were significantly associated with increased relapse probability. Cases with complete surgical margins did not recur. Other single variables were not significantly associated with relapse. Cluster analysis on MCA considering site, depth, margins, and type of growth identified 3 pathological profiles associated with PWT relapse and having a high prognostic impact. Major prognostic factors for cPWTs were tumor size, depth of growth, and pathological profiles.
Canine soft tissue sarcomas (STSs) are a heterogeneous group of tumors that comprise several neoplastic entities characterized by low metastatic potential and a variable recurrence rate after marginal surgical excision. 14,16,24,25,27,33
Perivascular wall tumors (PWTs) are mesenchymal neoplasms in the group of STSs and previously were included under the term hemangiopericytoma (HPC). 1 A previous study, including cases diagnosed as HPC and selected on the basis of specific histological and cytological features, demonstrated the perivascular origin of most tumors, excluding a diagnosis of peripheral nerve sheath tumors (PNSTs) and other types of spindle cell tumors according to phenotype and morphology. 1 This study identified morphological patterns consistent with PWT diagnosis. The general name of PWTs for this category of neoplasm was also proposed. 1 Furthermore, a subclassification was performed by the application of a wide panel of antibodies, identifying several subcategories of PWTs. 1 An ultrastructural study evaluating the features of STSs histologically consistent with PWTs but immunohistochemically not clearly classifiable confirmed the perivascular origin for all cases with perivascular patterns and excluded other types of STS, corroborating the specificity of these histological patterns. 26 Considering the overlap with the old category of canine HPC, PWTs seem to represent a significant proportion of STSs, 13 even if epidemiological studies of this newly described group of tumors are missing. In a recent study, the most important prognostic factors identified for canine PWTs (cPWTs) were tumor size and completeness of surgical margins. 32
Prognostic impact of single variables (univariate) is usually evaluated by their statistical significance: an in-depth evaluation should also account for the ability of the single variable to discriminate patients with different risks, as measured by Harrel’s C statistic. 19
For large case series, when several cases of tumor progression are observed, the appropriate evaluation of the joint prognostic role of the variables is evidenced by multivariate Cox regression analysis, providing estimates adjusted for the association among variables. Unfortunately, this analysis is not feasible for diseases with a low rate of relapses, metastases, or deaths. 18,31,34 A possible approach in these instances (low number of events) is to summarize the information provided by the variables by the application of profiles that account for their association and to use these profiles as categories in a univariate analysis. 17
Preliminary to the identification of profiles, study of the multivariate association pattern is necessary. When categorical variables are of concern, multiple correspondence analysis (MCA) is an useful tool. 22 This approach has the advantage of providing a simple graphical interpretation of the association patterns since a forthright inspection of the graphs may allow the identification of cases with similar features (profiles). To identify more consistently a limited number of profiles, cluster analysis can be applied to the results of MCA. The profiles can be described by the main characteristics of the cases incorporated by the cluster analysis into the same profile. 22 Moreover, the identification of profile characteristics is relevant for the interpretation of their prognostic role. 22
The aims of this study were to evaluate (1) the prognostic impact of histological parameters not previously evaluated in cPWT, (2) the association among the newly evaluated variables to identify potential pathological profiles, and (3) the prognostic impact of the identified profiles.
Materials and Methods
Selection Criteria, Tissue Handling, Trimming Protocol, and Diagnosis
In the study, we included cases of canine subcutaneous PWTs diagnosed at the histopathological diagnostic service of the Veterinary School of Milan, Italy, between 2001 and 2009, that fulfilled the following criteria:
Dogs undergoing treatment with the widest feasible excision until there was a maximum of 3 cm of normal tissue around the grossly visible mass, with at least 1 fascial plane removed that was macroscopically not infiltrated by the tumor.
Uniformity in the trimming protocol for evaluation of margins: evaluation of a complete longitudinal section and of multiple transversal sections placed at a maximum distance of 1 cm from each other. Additional sections were made in the areas where neoplastic infiltration was suspected by macroscopic evaluation of the sample.
Presence of prevalent growth patterns consistent with PWT, 1 including perivascular whorls, bundles radiating from the vascular wall, staghorn vessels (thin-walled branching vessels), and placentoid (multiple lobules with a central capillary) as previously reported. 1
When fresh tissue was available, 1 part of the tumor was snap-frozen in isopentane cooled at the freezing temperature in liquid nitrogen. Then, 5-μm cryosections were air dried, fixed in acetone (3 minutes), and stored at –70°C for immunohistochemistry to attain the specific diagnosis of a PWT subtype, applying a previously reported diagnostic algorithm. 1 When fresh tissue was not available, a generic diagnosis of PWT was granted based on the detection of the typical perivascular morphological patterns associated with expression of myoid markers (smooth muscle actin and/or desmin). 1
Pathological Parameters
The pathological parameters were recorded as follows:
Size: defined as the maximum diameter measured in centimeters with a caliper
Site: defined as extremities or acral (knee and distal, elbow and distal) and “other site” (eg, neck, thorax)
Depth: defined as the deepest tissue layer infiltrated by the tumor (dermis, subcutis, and muscular layer)
Type of growth: defined as expansile, satellite neoplastic nodular growth and infiltrative
Margins: defined as complete (distance between surgically created tissue edge and neoplastic cells was at least 3 mm), close (distance between surgically created tissue edge and neoplastic cells was less than 3 mm in thickness or surgical margins did not contain normal tissue outside the pseudo-capsule), and incomplete (neoplastic cells were continuous with at least 1 surgical margin in any plane), as indicated in the literature 7
Mitotic index (MI): absolute number of mitoses counted in 10 continuous high-power fields (400×) from the most cellular part of the tumor, categorized in 3 classes: 0 to 9, 10 to 19, and ≥20
For each case, the grade was calculated according to the guidelines reported in the literature and based on the degree of differentiation, mitotic index, and percentage of necrosis within the tumor. 7
Immunohistochemistry
For diagnostic purposes, when fresh tissue was available, immunohistochemical subtyping of PWTs was performed on frozen sections or cytological smears, applying the techniques and the antibody panel previously reported. 1 When fresh tissue was not available, immunohistochemical stains with monoclonal antibodies anti-desmin (clone DER-II, dilution 1:200, enzyme-induced antigen retrieval; Novocastra Laboratories Ltd, Newcastle UK) and anti–α smooth muscle actin (clone 1A4, dilution 1:2000; Dako, Glostrup, Denmark) were performed. Negative controls consisted of substitution of specific antibodies with an isotype-matched, irrelevant monoclonal antibody or omission of the primary antibody.
Follow-up Collection
Follow-up was performed by the oncologists using a standardized procedure that consisted of clinical examination at monthly intervals for the first 3 months after surgery, every 3 months for the first year, and every 6 months for the second year. After the first 2 years, follow-up consisted of a telephone conversation with the owner or the referring veterinarian. Thoracic radiographs and abdominal ultrasound were performed 6, 12, 18, and 24 months after surgery.
Relapses were confirmed by histology in all cases with the exception of the single metastatic case, in which metastases were diagnosed by cytology. Although cytological diagnosis of STS can be difficult to differentiate from reactive fibroplasia, the presence of the typical cytological features described in canine HEP 5,11 was considered sufficient for the diagnosis.
Statistical Analysis
Disease-free interval was calculated as the time elapsed from surgery to the date of the first evidence of tumor progression (local relapses and distant metastases). For cases without tumor progression, the disease-free interval was calculated as the time elapsed from the date of surgery to the date of the last follow-up information (right censored). The distribution of follow-up time was obtained by the reverse Kaplan-Meier method. 29
The collected data were analyzed following several consecutive steps:
The prognostic role of each variable was evaluated by the Cox regression model, which allowed estimation of the relationship between the logarithm of hazard ratios and variable values. For categorical variables, results were reported as the ratio of the hazard of relapse between a given category and the reference one. For the variables measured on a continuous scale, the relationship was investigated by cubic regression splines, allowing analysis of possible nonlinear behavior. 19 Linear behavior results were reported as the hazard ratio for a unit increase of the variable. Nonlinear behavior regression model estimates were not directly interpretable, and a graphical representation of relative hazard as a function of variable values was needed. The hypothesis of regression coefficients equal to 0 was tested by the 2-tailed Wald test.
The discriminant capability of each variable was measured by Harrel’s C index, which is an extension of the area under the receiver operating characteristic (ROC) curve for survival analysis. This index ranges between 0.5 (absence of discriminate ability) and 1.00 (perfect discrimination). 19
To study the association among variables, a preliminary analysis of each pair of variables was performed by χ2 statistics, after categorizing variables measured on a continuous scale. In this first step, a conservative P value of .20 was used as suggestive of a putative association between variables.
The joint association among variables was evaluated by MCA. This descriptive technique allows one to represent the association structure as a plot on a low-dimension subspace (possibly a plane), characterized by a high percentage of explained variability. On the plot, it is possible to report both the categories of the variables and the subjects. The distance among categories and among subjects is based on the χ2 metric. The proximity among categories can be interpreted as an association among them, and the proximity among subjects can be interpreted as subjects having variables with similar patterns. 22 Hierarchical cluster analysis was then applied to the coordinates of subjects on the MCA plane to identify profiles of clinical/pathological variables. Due to the limited size of the case series, a maximum of 3 clusters were allowed.
The joint prognostic role of the variables was summarized comparing the disease-free interval curves by the log-rank test.
Results
Cases, Diagnosis, and Outcome
A total of 56 cPWTs in 55 dogs were collected, 14 of which were included in a previous classification study 1 and 51 in a clinical and prognostic study. 32 Results regarding site, depth, type of growth, completeness of the margins, and outcome are summarized in Table 1. Of the 56 cases, 21 tumors were myopericytomas, 4 were angioleiomyomas, 2 were angioleiomyosarcomas, 2 were hemangiopericytomas, 2 were angiofibromas, and 2 were adventitial tumors. In 23 cases, fresh tissue was not available, and a generic diagnosis of PWT was made based on the detection of 1 or more diagnostic perivascular growth patterns together with the expression of smooth muscle actin and/or desmin. One of 23 cases expressed smooth muscle actin only, 10 cases expressed desmin only, and the remaining 12 cases expressed both actin and desmin.
Summary of Pathological Parameters and Outcome of Canine Perivascular Wall Tumors.
Twenty-eight cases were located at the extremities distal to the elbow and knee (acral), and 28 were located in “other sites” (proximal limbs, thorax, neck/head, perineal, abdominal, tail base). Size ranged from 0.5 to 15 cm (mean, 6.23 cm; median, 5 cm). In 4 cases, tumor size was not available. In 51 cases, the neoplasm was limited to the subcutaneous tissues, while in 5, tumor infiltration of the underlying muscular layers was detected microscopically (Fig. 1). At the histological examination, the type of growth was expansile in 28 cases, satellite nodules were present in 11 cases (Fig. 2), and infiltrative growth was evident in 17 cases (Fig. 1). Margins were complete in 6 cases, close in 15 cases, and incomplete in 35 cases. MI ranged from 0 to 48 (mean, 8; median, 4). Twenty-five cases were grade I, 27 were grade II, and 4 were grade III. Ten cases recurred, 1 case metastasized, and 5 were lost to follow-up. Follow-up was ≥330 days in 75% and ≥1140 days in 25%, and median follow-up was 735 days.
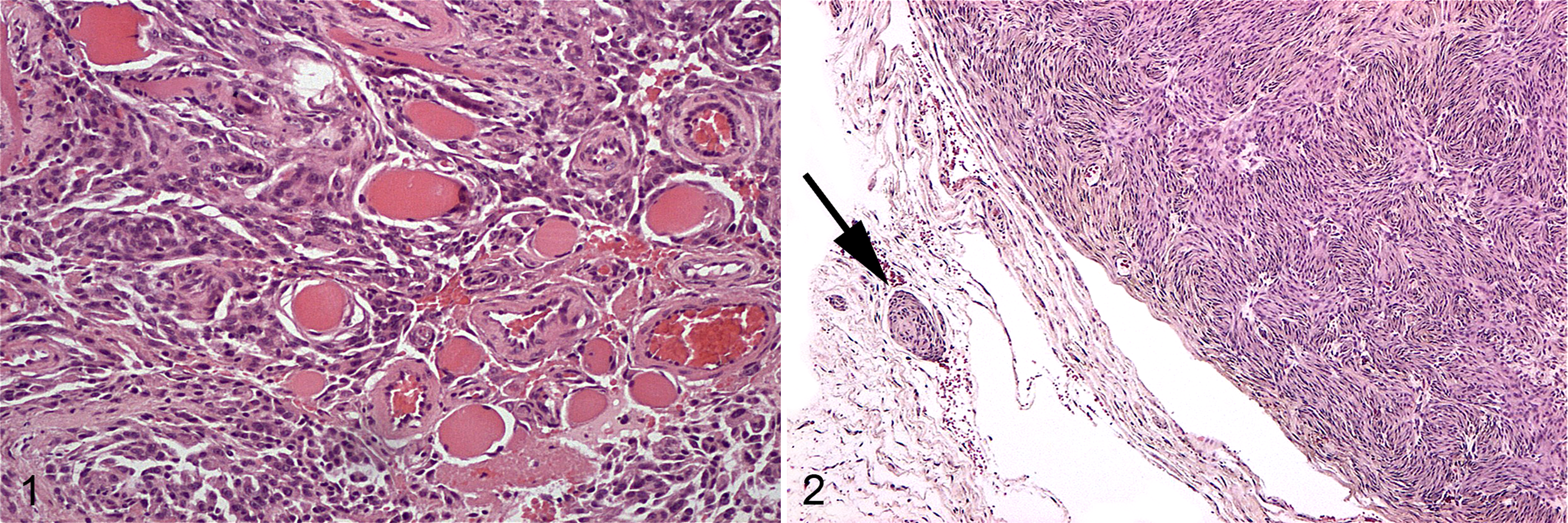
Subcutis; canine perivascular wall tumor; dog No. 8. Neoplasm reaching the muscular layer and characterized by infiltrative growth. Hematoxylin and eosin (HE).
Analysis of the Disease-Free Interval
Only tumor size and depth of the lesion had a significant prognostic role. The hazard of relapse of dogs with tumors >5 cm was about 6 times greater than dogs with tumors ≤5 cm. A better estimation was obtained when tumor size was analyzed as a continuous variable: a log-linear prognostic relationship was found, and a ratio of 1.23 of the hazard of relapse was estimated for each centimeter increase in tumor size. The discriminant capability (Harrel’s C index) was 0.698, which is significantly greater than 0.5. Depth of the lesion had a relevant prognostic impact: the hazard of relapse of tumors with muscular invasion was about 8 times greater than that of subcutaneous ones (Fig. 3). Results of the analysis are listed in Table 2.
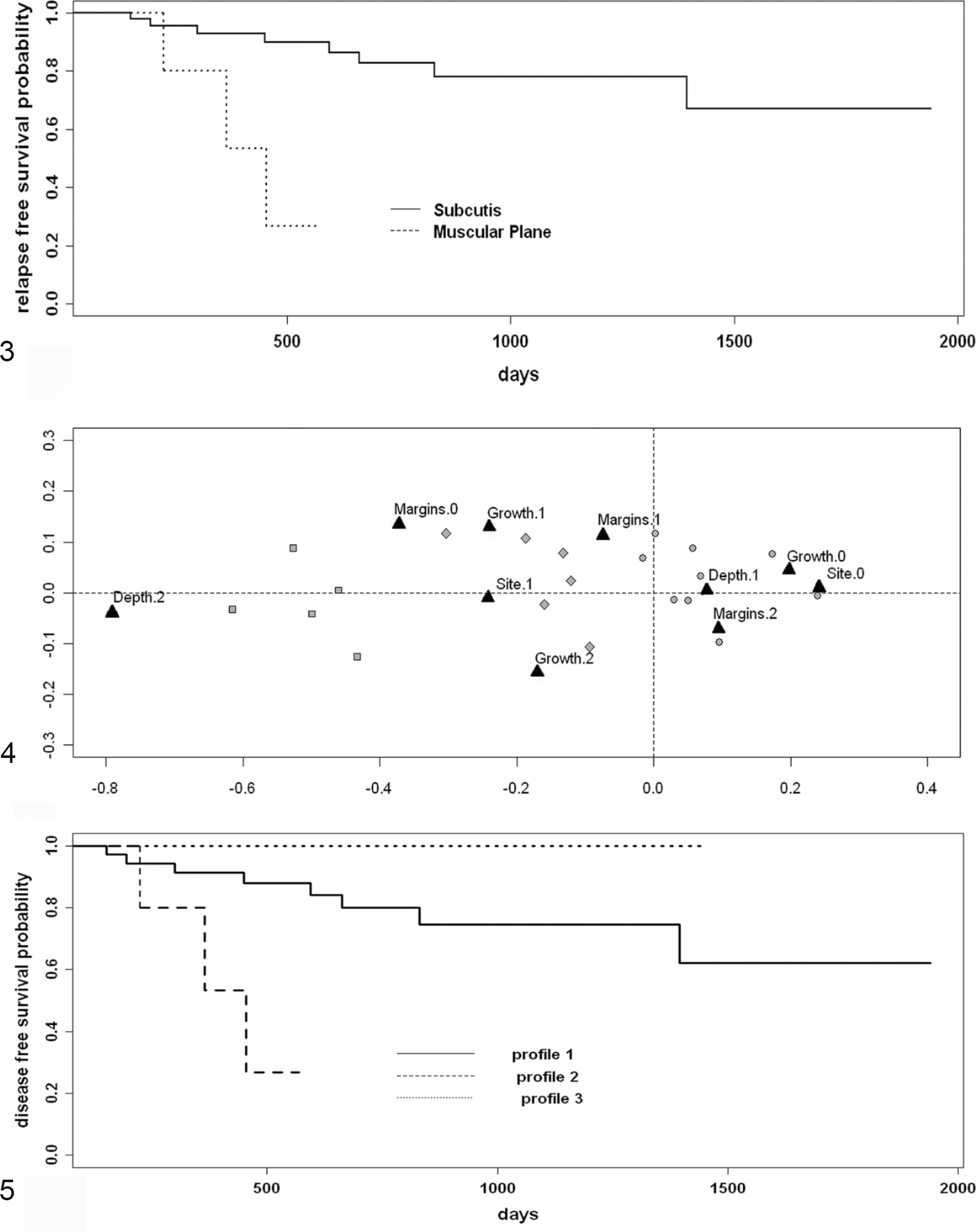
Prognostic impact of the depth of the lesion. Kaplan-Meier disease-free interval curve for cases located in the subcutis compared with cases reaching the muscular plane.
Analysis of Disease-Free Interval (Univariate Analysis): Cox Model Results.
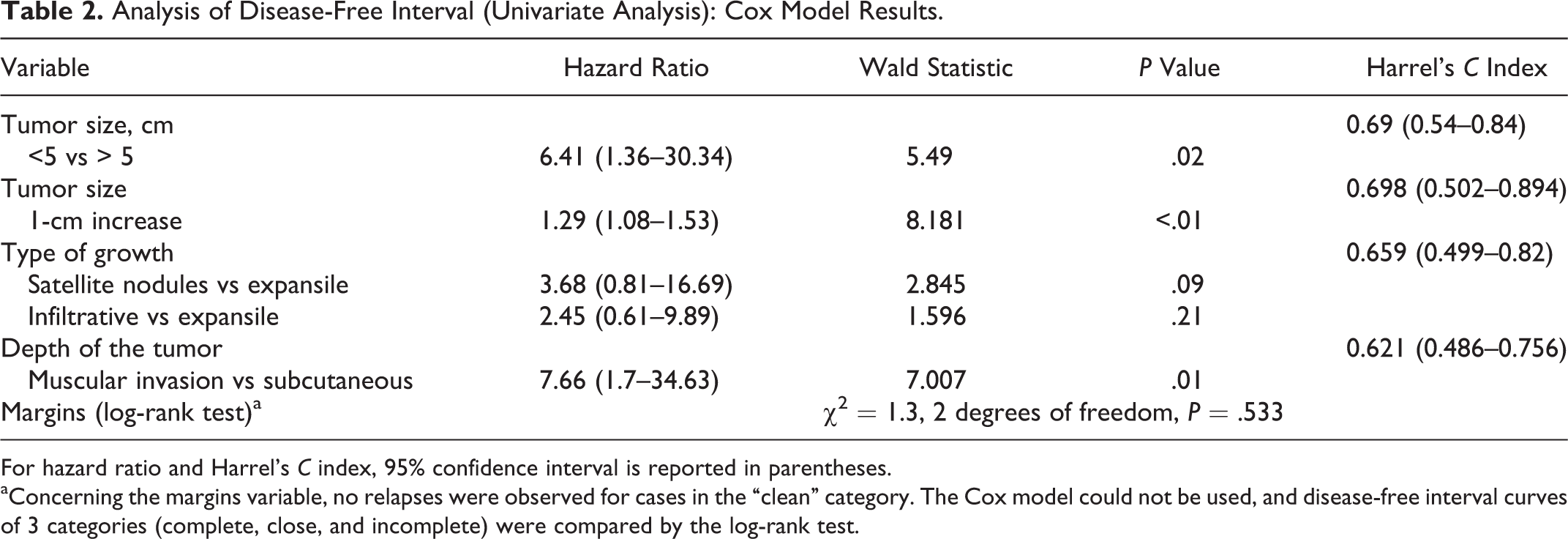
For hazard ratio and Harrel’s C index, 95% confidence interval is reported in parentheses.
aConcerning the margins variable, no relapses were observed for cases in the “clean” category. The Cox model could not be used, and disease-free interval curves of 3 categories (complete, close, and incomplete) were compared by the log-rank test.
Analysis of the Association Among Variables
Site was correlated with type of growth (P = .115). Cases developing in distal limbs were more commonly characterized by expansile growth. Development of tumors in “other sites” correlated with infiltrative growth and satellite nodules. Site was also correlated with depth of the lesion (P = .051), with muscular invasion evident only in cases in other sites. Depth of tumor location correlated with the type of tumor growth (P = .022), with infiltrative growth and satellite nodules the most common growth types in cases infiltrating the musculature. No association was found between size and any of the other variables.
MCA
Size was not included in MCA since an association with other variables was not found in preliminary the χ2 analysis. The plane accounted for 79.2% of the total variability (inertia), so the profiles, identified by position of the modalities in the plane, were well represented (Fig. 4).
Tumors located in the subcutis of the distal limbs were characterized more frequently by expansile growth and incomplete margins, while tumors in other sites showed more frequently complete or close margins and satellite nodules or infiltrative growth.
When hierarchical clustering was applied to the subject coordinates of MCA, 3 profiles were identified and were mainly characterized as follows:
Profile 1 (37 cases) included all tumors in the extremities and tumors in other sites with expansile growth and close or incomplete margins.
Profile 2 (5 cases) comprised tumors in other sites with infiltrative growth or satellite nodules and reaching the muscular plane.
Profile 3 (14 cases) included subcutaneous tumors in other sites characterized by expansile growth and complete margins or by infiltrative growth/satellite nodules.
Main features of the profiles are summarized in Table 3.
Features Describing Most Canine Perivascular Wall Tumors Included in Each Profile.

For the analysis of disease-free interval, 5 cases were lost to follow-up (1 case of profile 1 and 4 cases of profile 3). The estimated disease-free interval curves of the 3 profiles are shown in Fig. 5: no relapses were observed in profile 3 (10 cases), 3 relapses were observed in profile 2 (5 cases), and 8 relapses were observed in profile 1 (36 cases). A statistical significance was obtained for the comparison of the disease-free interval of the 3 profiles (log rank test = 10.7, 2 degrees of freedom, P = .005).
In summary, cluster analysis identified 3 clusters representing pathological profiles with different risks of relapse.
Discussion
Heterogeneity of canine STSs often hampers their specific differential diagnosis and has led to the application, for a subgroup of STSs, of the generic term spindle cell tumor of canine soft tissue, encompassing schwannoma, fibrosarcoma, and the so-called HPC. 35 Following this path, a more generic nomenclature for schwannoma and HPC has been suggested: PNST, representing neoplasms arising from peripheral nerve sheath, 12,15,20 and PWTs, indicating neoplasms arising from vascular mural cells. 1 Several studies have attempted to clarify the cellular differentiation and the hallmarks for the diagnosis of these 2 groups of tumors. 1,10,26,30 Histological features described in canine PNSTs have included whorls around collagen fibers, 10,12 interlacing bundles, 10,15 Verocay bodies, 10,15 and tactile-like structures. 30 Histological features described for cPWTs include perivascular whorls, interlacing bundles, placentoid growth, and thin-walled branching vessels (staghorn vessels). 1 Immunohistochemical and ultrastructural studies of PNSTs and cPWTs have respectively confirmed the perineural and perivascular origin of tumors indentified by the aforementioned growth models and have allowed their specific subtyping. 1,10,26,30 Hence, cPWTs have been subclassified into hemangiopericytomas, myopericytomas, angioleiomyomas/sarcomas, angiofibromas, and adventitial tumors, 1 while PNSTs have been subtyped into schwannomas and neurofibromas. 10,15,30 Of the latter, several histological variants have been described. 30 Despite all these efforts, the generic diagnosis of STS is still commonly applied and, as a consequence, prognostic parameters most commonly evaluated for cPWTs have been completeness of surgical margins and tumor grade that are regarded as the most important prognostic factors for canine STS. 6,21,25 To verify the role of these factors, this study focused on the study of the prognostic impact of pathological parameters for cPWTs only. To provide a practical approach to cPWT prognostication in daily diagnostic activity, their identification was based on the typical histomorphological patterns and confirmed by immunohistochemistry (IHC) for desmin and actin. 1
In prognostic studies, the statistical assessment of the significance of the prognostic impact of each variable examined should be evaluated by multivariable regression models that can be applied only if the ratio between the number of events and the number of variables in the regression model is adequate. The adequate ratio was suggested to be 1018,31 or, more recently, 5. 34 When the incidence of the events does not allow the investigation of the joint prognostic role of several variables, as occurred for this caseload, a suggested strategy is to reduce the number of variables in the regression model by data reduction techniques. 17 This method consists of the application of multivariate analysis techniques (eg, principal components or cluster) to build a limited number of derived variables accounting for the association structure of the original ones and to include the derived variables in the regression model. 17 This strategy has the advantage of evaluating the joint prognostic role of the original variables. 17 In the current study, a limited number of events were recorded for statistical evaluation. Specifically, 10 cases recurred and 1 case metastasized, for a total of 11 events. Our approach was therefore to evaluate the prognostic impact of each variable by univariate analysis, define derived variables (pathological profiles) by means of MCA and cluster analysis, and evaluate the joint prognostic role of the parameters, allowing an adequate ratio to be reached between the number of events and the number of variables. According to the univariate analysis by the Cox regression model and corresponding Harrel’s C index, tumor size proved to have the highest prognostic impact, being strongly associated with recurrence, as previously reported. 32 In this work, the association between tumor size and other variables was not observed.
In this study, all cases with complete margins did not recur, paralleling previously reported data. 25,32 Unexpectedly, an association between incomplete or close margins and acral location was not identified, even if this result was expected as a consequence of the paucity of nonneoplastic tissue that can be generally excised when the tumors develop in distal limbs. However, this result can be explained by the association identified between type of growth and site of the lesions. Indeed, acral PWTs were more commonly characterized by expansile growth, while infiltrative growth and satellite nodules were more frequently found in cases developing in other sites. A likely hypothesis is that the presence of an expansile growth pattern in acral tumors allows for a complete excision, compensating for the negative role of a distal limb origin.
Depth of tumor had a relevant prognostic impact, with tumors developing or extending into skeletal muscles approximately at an 8 times greater hazard of relapse compared with sole subcutaneous involvement. To our knowledge, the prognostic impact of depth of tissue invasion has not been assessed for canine STSs, with the exception of 1 study evaluating clinically, but not histologically, the tumor adhesion to underlying tissues. 6 On the contrary, depth is routinely included in the evaluation protocols of human STSs, at least by macroscopic examination. 28 The correlation of depth of tumor invasion with relapse but not with type of surgical margins suggests that PWTs reaching the muscular layer may have a more aggressive behavior independent of a more or less feasible excision.
MCA and cluster analysis defined 3 major pathological profiles with high prognostic impact. Profile 1, characterized by an intermediate rate of relapse, was composed mainly of cases located in the extremities, limited to the subcutis and characterized by expansile growth. The intermediate rate of relapse can be explained by the combination of expansile growth and distal acral location. The first can assist the surgeon in performing a complete excision, while the second can have an opposite influence. Profile 2 included all cases not located in the extremities with nonexpansile growth (infiltrative or satellite nodules) that reached muscular layers. This group of cPWTs was characterized by the highest relapse rate and included also the single case that metastasized. The association between muscle infiltration and relapse supports the hypothesis that deep tumor growth indicates a more aggressive biological behavior. Profile 3, characterized by the lowest relapse rate, included mainly tumors not located in the extremities, limited to the subcutis, and, surprisingly, with nonexpansile growth. The unexpected inclusion of nonexpansile growth in the profile with the lowest rate of relapse can be explained considering that all cases in profile 3 were located in sites other than extremities, allowing for a complete excision.
Even if several studies have evaluated the prognostic impact of at least 1 parameter that delineates the profiles, the joint prognostic role of these parameters has not been previously investigated. 2 –4,6,25 The prognostic impact of the completeness of surgical margins already has been demonstrated, 6,21,25 while the evaluation of the prognostic impact of tumor location has produced discordant results. 2 –4,6,21 Last but not least, even if the histological evaluation of type of growth and depth of the lesion seems to have never been reported, a study showed the association between manual assessment (by palpation of lesions prior to excision) of tumor invasion into underlying tissues and a decreased disease-free interval. 6 This evidence can presumably be the consequence of the nonexpansile growth and infiltration of the muscular layer with subsequent tumor adhesions to deep tissue components.
As a conclusion, the statistical approach applied in this work identified 3 tumor groups with a different risk of recurrence and a high prognostic impact that likely depends on the effect of the interaction of different pathological parameters. Some of these, such as site and type of growth, can influence the completeness of the excision, while others, such as depth of the lesion, seem to be associated with a more aggressive biological potential. These profiles can therefore have an important role in the prognostication of recurrence, considering that the parameters on which they are built include factors that may influence the completeness of the surgical margins and the surgical margins themselves. This is in accordance to what has been described in the World Health Organization (WHO) classification of tumors in humans, which states that “grade particularly indicates the probability of distant metastasis and overall survival, but is of poor value for predicting local recurrence which is mainly related to the quality of surgical margins.” 9
Of note, the homogeneity of our caseload allowed us to identify a metastatic rate (2%) that is lower than the range of 8% to 17% reported in studies evaluating a heterogeneous group of STSs. 2,6,8,21,23 This observation further supports that cPWTs have a distinctive and less aggressive behavior compared with canine STSs in general.
In conclusion, by the evaluation of the sole group of cPWTs, we were able to identify pathological profiles based on straightforward pathological parameters that were significantly associated with recurrence. In this study, the number of profiles identified by MCA and cluster analysis was limited because of the number of cases evaluated. It is worth mentioning that with a larger caseload, the number of profiles may increase, providing a better characterization of profiles and of cPWTs. As a consequence, we suggest that further studies of independent case series should be performed to validate the stability of the pathological association structure. This strategy of analyzing prognostic factors is not commonly applied in veterinary oncology, but given our results, we believe this approach can be a useful and resourceful tool for future prognostic studies, especially those focusing on neoplasms characterized by low recurrence and metastatic rate. Indeed, these behavioral features can limit the evaluation of prognostic parameters as a consequence of the low number of events, a problem that can be circumvented by the data reduction technique illustrated and applied in this work. In our opinion, the major problem of the sample size is one of the main reasons for prognostic studies on heterogeneous, even if larger, caseloads. This, however, prevents the recognition of distinctive features of different canine STS types. Furthermore, this approach has the advantage of providing useful information on the association structure among variables and their interaction.
Our results revealed the existence of pathologic profiles with significant prognostic impact for cPWTs, supporting the efficacy of the evaluation of homogeneous STS caseloads. In conclusion, we suggest routinely evaluating the size and depth of the tumors, as well as pathological profiles based on site, margins, depth, and type of growth to predict recurrence of cPWTs. This approach can be useful during routine diagnostic activity, when the pathologist is required to provide the clinicians with information on the probability of local recurrence rather than the unlikely event of metastasis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.