
Abstract
The white-tailed deer (Odocoileus virginianus) is a common and widespread North American game species. To evaluate the incidence, clinical manifestations, demography, and pathology of bacterial and parasitic dermatologic diseases in white-tailed deer in the southeastern United States, we retrospectively evaluated white-tailed deer cases submitted to the Southeastern Cooperative Wildlife Disease Study from 1975 to 2012. Among 2569 deer examined, bacterial or parasitic dermatologic disease was diagnosed in 88 (3.4%) individuals, with Demodex spp (n = 37; 42.0%) and Dermatophilus congolensis (n = 19; 21.6%) as the most common causes. Demodicosis was significantly more common in deer older than 2 years and was most often detected in the fall; no statistically significant sex predilection was identified. Affected animals had patchy to generalized alopecia, often distributed over the head, neck, limbs, and trunk; microscopic lesions included epidermal crusts and cutaneous nodules with mild perifollicular, lymphoplasmacytic inflammation. Dermatophilosis was most common in males younger than 1 year that were often found dead. Crusting, erythema, and alopecia occurred on the face, ears, and distal extremities. Less commonly, infectious dermatologic diseases were associated with other bacteria (n = 13; 14.8%), fungi (n = 5; 5.7%), ectoparasites (chiggers, lice, mites, and ticks; n = 11; 12.5%), and larval nematodes (n = 7; 8.0%). Population-level effects of these diseases in white-tailed deer are likely minimal; however, due to their dramatic presentation, demodicosis, dermatophilosis, and other infectious skin diseases can be of concern to hunters and, in some cases, may have zoonotic potential.
Free-ranging white-tailed deer (Odocoileus virginianus) are susceptible to a variety of infectious agents that can cause dermatologic diseases with variable sequelae ranging from subclinical to fatal. These diseases are often externally evident on the deer and therefore can be visible to the general public, hunters, and wildlife biologists; in addition, some of these disease agents have potential public health implications for those in direct contact with the deer. Documentation of diseases such as demodicosis and dermatophilosis among free-ranging wildlife is often limited to single or small numbers of individuals. 5,20,23 Therefore, it is difficult to assess disease prevalence, geographic distribution, demographic and temporal patterns, and potential population-level impacts. Factors that may contribute to the incidence and severity of dermatologic diseases in wildlife may include environmental (eg, seasonal adverse weather, poor habitat quality, scarce nutritional resources) or physiologic stressors (eg, seasonal hormonal cycles associated with breeding), host immunologic and genetic factors, and concurrent disease.
To better determine the frequency and extent of dermatologic diseases and assess patterns of gross and microscopic lesions in white-tailed deer, we reviewed all white-tailed deer sample submissions to the Southeastern Cooperative Wildlife Disease Study (SCWDS) from 1975 to 2012 for dermatologic diseases for which a bacterial, fungal, or parasitic etiology was identified. For the most commonly diagnosed diseases, demographic trends, geographic distribution, and seasonal patterns were examined. In addition, nutritional condition, gross and microscopic lesion patterns, and concurrent diseases among deer with demodectic mange and dermatophilosis were examined. Agents associated with skin disease in white-tailed deer, including bacteria, fungi, nematodes, and ectoparasites, were included. Cutaneous fibromas and spontaneous neoplasms were not included in this study.
Materials and Methods
The records of white-tailed deer clinical cases submitted to SCWDS from January 1975 to April 2012 were reviewed for individuals diagnosed with demodectic mange and dermatophilosis, as well as those that had dermatologic lesions associated with other micro- or macro-organisms. Cases of demodectic mange were defined as those in which animals had gross lesions suggestive of demodicosis (ie, variable alopecia, thickened skin, crusting, scaling, lichenification, or seborrhea) along with identification of Demodex sp (size was most consistent with, but not confirmed as, Demodex odocoilei) 6 either by microscopic examination of skin scrapings or within hair follicles upon histologic evaluation. Demodicosis was considered generalized when 3 50% of the surface of the skin was grossly affected. Deer were diagnosed with dermatophilosis when they had grossly visible dermal encrustations with intralesional Dermatophilus congolensis, as determined by microscopic examination of skin smears or histologic examination, and, in some cases, confirmed by bacterial culture. For other cases in which infectious organisms were observed during routine histopathology, additional histochemical stains and bacterial cultures were performed to determine the etiology. Ectoparasites and larval nematodes were identified by distinguishing morphological characteristics (eg, size) as well as location.
Samples submitted for diagnostic evaluation varied from formalin-fixed skin sections over a localized area to the entire carcass. Therefore, full postmortem examinations were limited to a subset of deer in this study. For cases in which submitted samples consisted only of formalin-fixed skin sections, documentation of the gross lesion distribution on the skin was made in the field by wildlife biologists. In cases in which carcasses were submitted, full gross and microscopic evaluations were performed by veterinary diagnosticians at SCWDS.
Tissues were fixed in 10% neutral-buffered formalin, routinely processed, embedded in paraffin, sectioned at approximately 5 μm, mounted on glass slides, and stained with hematoxylin and eosin. Additional histochemical stains performed on select case slides included Lillie Twort Gram, periodic acid–Schiff, Giemsa, Grocott’s methenamine silver, and Ziehl-Neelsen and modified acid fast stains. When fresh samples were available, standard aerobic and, less often, anaerobic bacterial culture was performed. Multiple organisms were identified in the skin of some deer. When an organism was identified histologically as being numerous, widespread, and associated with lesions, it was considered a primary etiology; however, deer with multiple organisms in the skin in which the primary infectious organism could not be distinguished were considered coinfected.
Data compiled for each animal with demodicosis and dermatophilosis included county and state of origin, date when found, sex and age, gross lesion distribution and characteristics, microscopic lesions, and additional observations from gross examination and, when possible, full necropsy. In some cases, sex, age, and gross lesion distribution were not reported. Sex, age (juvenile, subadult, adult), and seasonal distribution were analyzed with a χ2 test using SAS 9.2 software (SAS Institute, Cary, NC). The age classes were defined as juvenile (≤1 year), subadult (1–2 years), and adult (>2 years). Seasons consisted of spring (March 22 to June 21), summer (June 22 to September 21), fall (September 22 to December 21), and winter (December 22 to March 21).
Results
A total of 2569 white-tailed deer were received for diagnostic evaluation at SCWDS between January 1975 and April 2012. During this time, 88 (3.4%) white-tailed deer were diagnosed with a variety of infectious skin diseases (cases with viral or noninfectious causes of skin disease, including cutaneous fibroma, and those with undetermined etiology were excluded). Infectious skin diseases were associated with a variety of etiologic agents, including bacteria, fungi, nematode larvae, mites, and other ectoparasites, and the skin of some individuals was infected with multiple agents.
Demodectic Mange
Demodectic mange was diagnosed in 37 white-tailed deer; half of these cases were from the last 5 years of the study period. Most of these deer were hunter harvested or killed by wildlife biologists for necropsy (32/37; 86.5%); in addition, 1 deer was killed by vehicular collision, 2 were found dead, and the cause of death was unknown in 2 deer. Deer diagnosed with demodectic mange were from 12 states (31 counties), the majority of which were in the southeastern United States, although cases were observed in Delaware, Maryland, and as far west as Kansas (Fig. 1).
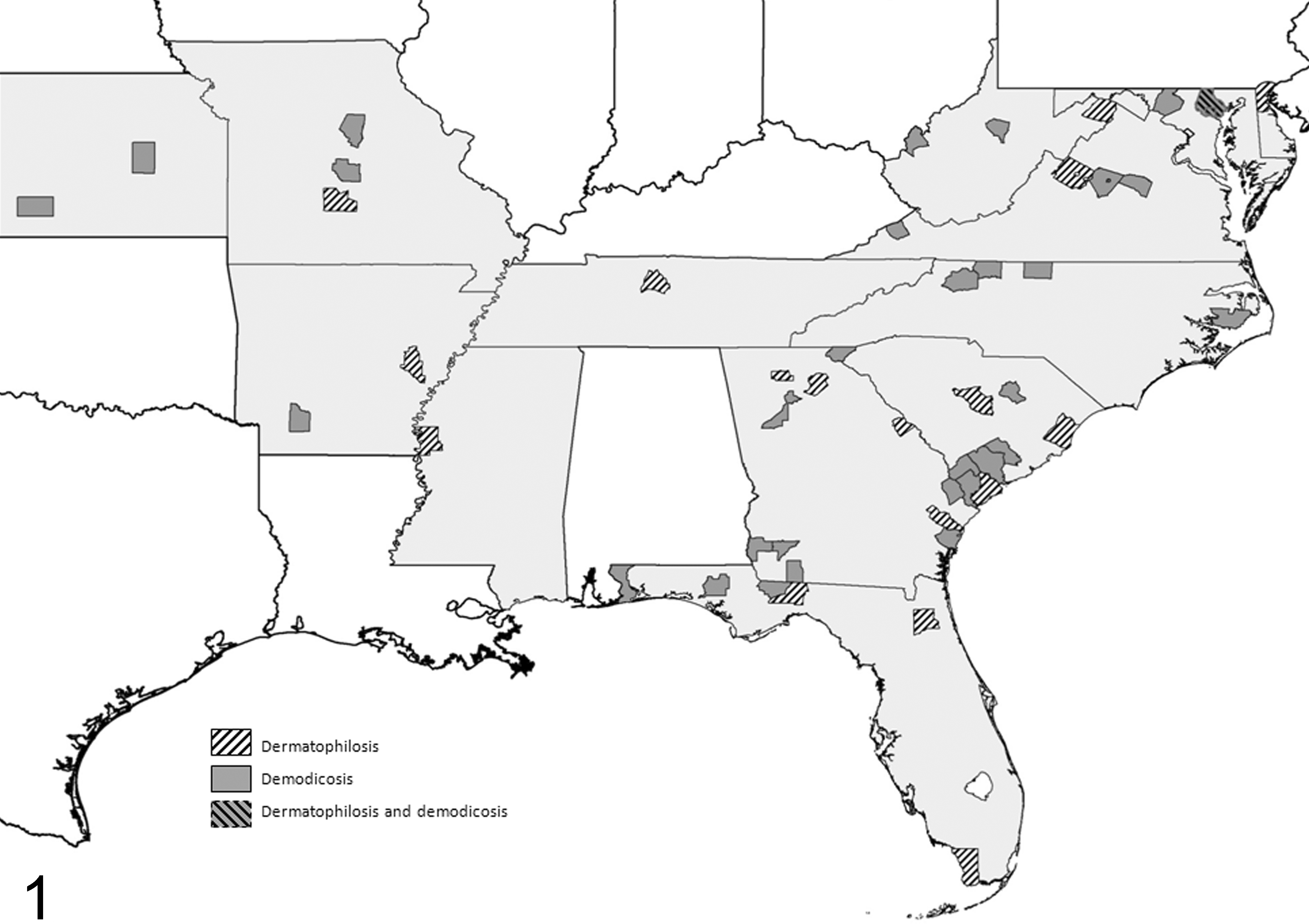
Geographic distribution by state (light gray) and county for cases of demodicosis (Demodex spp) and dermatophilosis (Dermatophilus congolensis) in white-tailed deer (Odocoileus virginianus) submitted to the Southeastern Cooperative Wildlife Disease Study from 1975 to 2012.
Most (63.9%) deer with demodicosis were male (n = 36; sex was unreported in 1 deer), but there was no significant difference between the proportions of sexes with demodectic mange (P = .182, χ2 = 1.778). The proportion of deer in various age classes differed significantly (P < .001, χ2 = 31.771), with 25 adult deer, 7 subadults, and 1 juvenile (n = 35; age was unreported in 2 deer). The proportion of deer with demodicosis was also significantly different by season (P < .001, χ2 = 17.570). Nearly half of the deer with demodectic mange were observed during the fall (18/37), with the remainder during summer (9/37) and winter (10/37).
Full necropsies and microscopic evaluations were performed on 15 deer with demodectic mange. Seven (47%) of these deer were in good to excellent nutritional condition, 2 were in fair condition (13%), and 6 (40%) were in poor condition. Eight (53%) deer had pulmonary larval nematodiasis. Concurrent infestations with biting lice morphologically consistent with Tricholipeurus parallelus were noted on the skin of 3 deer with demodicosis, and one yearling had concurrent dermatophilosis.
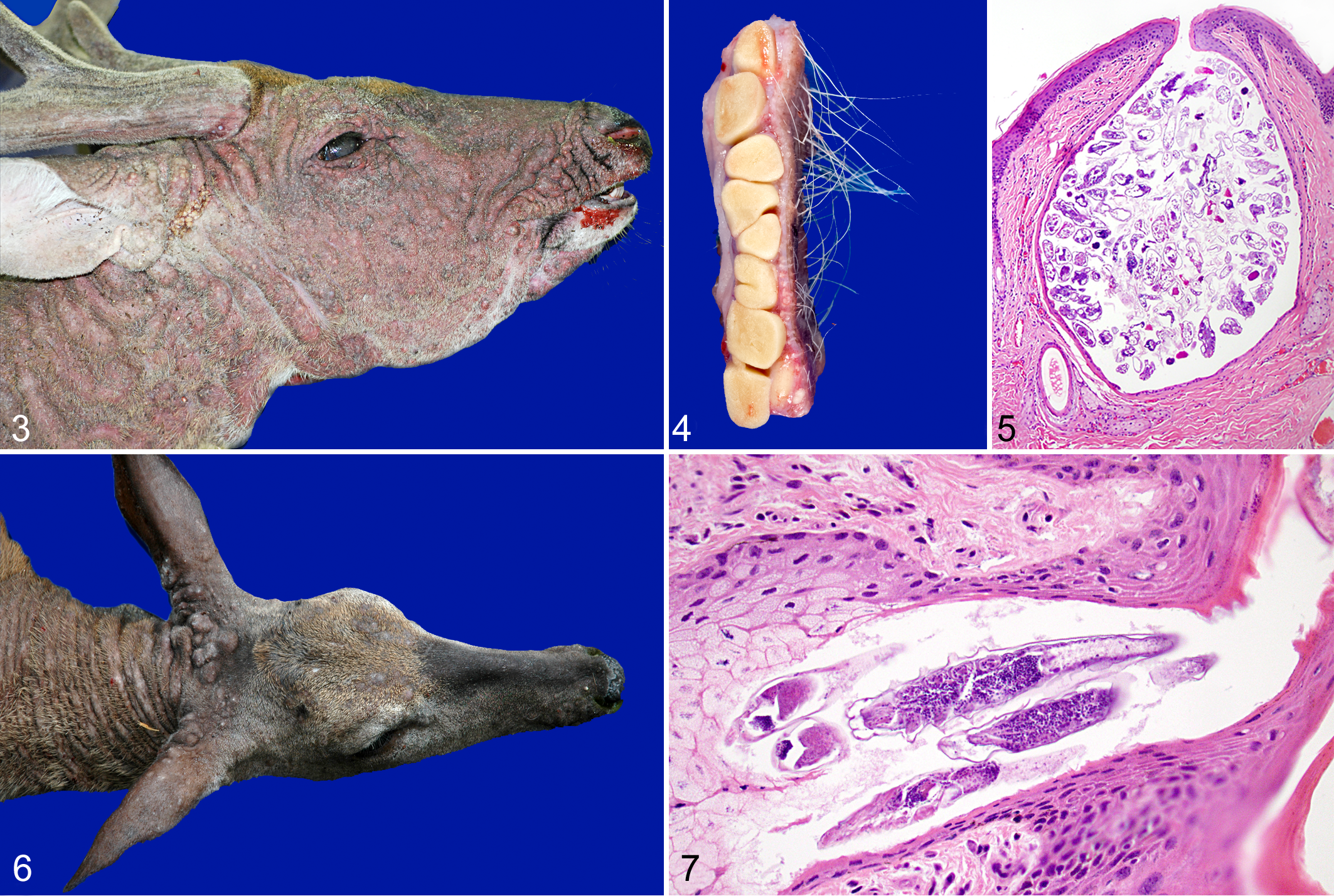
Gross lesions and anatomic distribution of lesions in deer with demodicosis are provided in Fig. 2. Among the 30 deer in which lesion distribution was reported or observed at necropsy, generalized alopecia (ie, covering more than 50% of body) was most often observed in females (8/13; 62%) vs males (7/16; 44%) and was most commonly seen during the fall (50%). The distribution of alopecia was unreported in 7 deer. Localized alopecia had a patchy, multifocal distribution that most often involved the head (base of the pinnae, muzzle, and face), neck, and limbs but also variably affected the ventral neck, shoulders, axillae, dorsum, ventrum, and flanks in some deer. Alopecia was the most common finding in deer with demodectic mange, followed by numerous, 1- to 3-mm-diameter dermal nodules (No. 1; Figs. 2, 3, 6). These nodules consisted of cutaneous glands and hair follicles distended up to 4-mm in diameter and impacted with yellow-white caseous material that consisted of countless mites (No. 2; Fig. 4). The distribution of dermal nodules was unknown in 5 animals. Microscopically, hair follicles were distended with variable numbers of mites (No. 2; Figs. 5, 7). Inflammation in the surrounding dermis (lymphocytes and plasma cells, with fewer neutrophils and rare eosinophils) was minimal except when associated with furunculosis, which was observed in 4 cases.
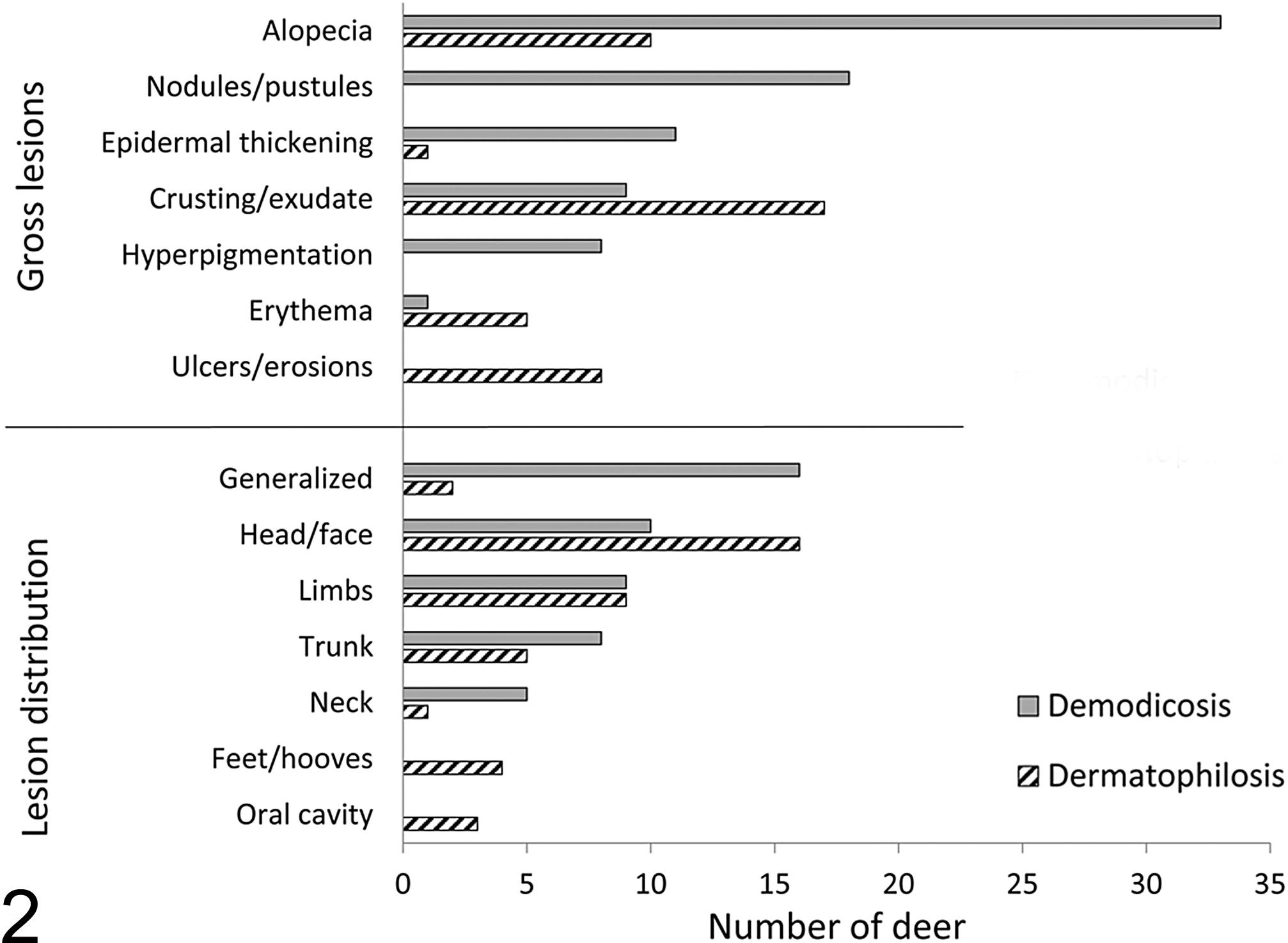
Gross lesions and anatomical distribution associated with Demodex spp infestation and Dermatophilosis congolensis infection in white-tailed deer (Odocoileus virginianus) in parts of the midwestern and southeastern United States.
Dermatophilosis
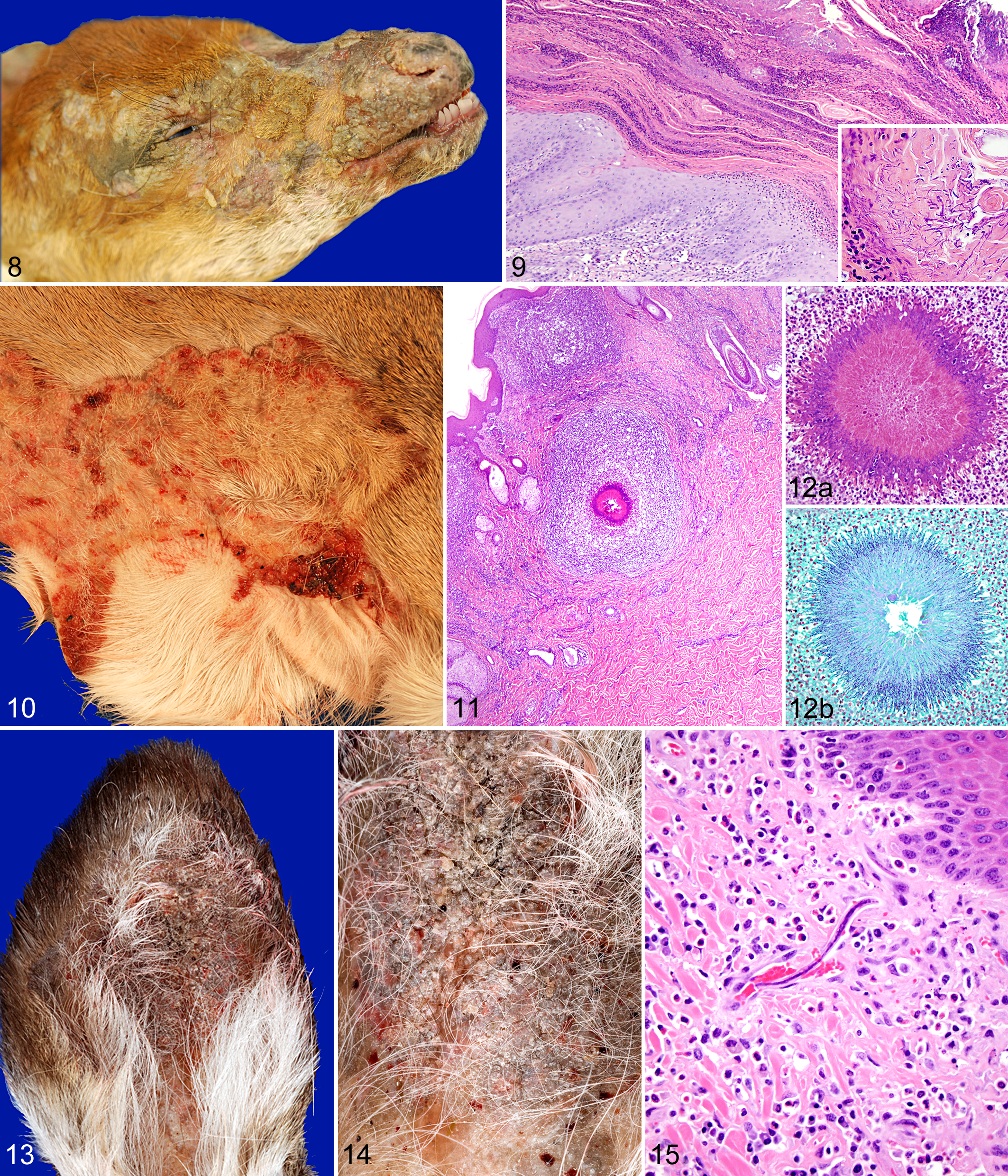
D. congolensis was detected in 19 white-tailed deer submitted to SCWDS during the study period. Most of the cases consisted of carcasses that were recovered year-round in 18 southeastern and mid-Atlantic states, as well as Missouri (Fig. 1). Affected deer were often emaciated, and several had concurrent fractures or arthritis. There was a significant difference between age classes; 63% (12/19; P = .008, χ2 = 9.579) of the deer were juveniles. Seventy-three percent (11/15) of deer with known sex were male; however, the difference between affected males and females was not significant (P = .07, χ2 = 3.267). Deer with dermatophilosis were observed in all seasons, and there were no significant differences in the seasonal distribution of cases (P = .376, χ2 = 3.105). Gross lesions usually consisted of alopecia with crusting and erythema on the face and ears (No. 3; Figs. 2, 8), as well as the distal limbs. Cytologic examination of direct smears revealed parallel chains of cocci in “railroad track” configurations characteristic of D. congolensis. Histologic lesions were characterized by extensive serocellular crusts composed of many degenerate neutrophils, keratin, and necrotic cell debris containing multiple filamentous chains of bacteria characteristic of D. congolensis (No. 3; Fig. 9). Five deer with dermatophilosis also had verminous or bacterial pneumonia.
Other Dermatopathies
Thirteen white-tailed deer had dermatitis associated with other bacteria, most commonly Staphylococcus and Streptococcus spp, and 2 of these had concurrent fungal infections. A 1.5-year-old doe from Georgia had Streptomyces sp infection affecting the skin over the muzzle and proximal limbs (No. 4, Fig. 10), associated with severe, chronic, ulcerative, pyogranulomatous dermatitis with Splendore-Hoeppli material (No. 4; Fig. 11). Occasionally embedded within the Splendore-Hoeppli material were mats or loose aggregates of acid fast–negative, Gram-positive, filamentous, rod-shaped bacteria (Fig. 12a,b). An 8-year-old doe from Georgia had severe crusting over the axillae, inguinal region, face, neck, and flank associated with Arcanobacterium haemolyticum, which also caused severe inflammation in adjacent lymph nodes. Five individuals from Georgia, Delaware, Missouri, and West Virginia had fungal dermatitis, 2 of which had concurrent bacterial dermatitis, and 1 had concurrent deer ked (Lipoptena cervi) infestation. Nine white-tailed deer from Georgia, Louisiana, South Carolina, Tennessee, Virginia, and Maryland had ectoparasite-associated dermatitis associated with large numbers of a variety of arthropods consistent with chiggers (larval Trombiculidae), Texas itch mites (Chorioptes texanus), chewing lice (Tricholipeurus spp), and deer keds (L. cervi). Also among these, 2 deer had multifocal alopecia and eosinophilic dermatitis associated with massive burdens of Amblyomma maculatum and Amblyomma americanum ticks. Seven deer, all found in Hampshire County, West Virginia, in the spring (March–April 2009, 2010, and 2012), had severe aural dermatitis of the inner and, less commonly, outer ear pinnae with infestation of nematode microfilariae (No. 5; Figs. 13–15). Deer with aural nematodiasis ranged in age from 1.5 to 4.5 years of age.
Discussion
Free-ranging white-tailed deer are intermittently or seasonally exposed to potentially infectious organisms of the skin, either directly through intra- or interspecific contact, indirectly through contact with contaminated environments, or via arthropod vectors. Although speculative, stress-associated immunosuppression from a variety of natural or anthropogenic sources may further increase the likelihood and severity of colonization of the skin by potential pathogens. In the present study, Demodex spp and D. congolensis were the most common causes of infectious dermatologic disease in white-tailed deer in a geographic region that comprised much of the southeastern and parts of the mid-Atlantic and midwestern United States. Additional bacteria such as Staphylococcus spp; ectoparasites such as mites, chiggers, lice, and ticks; and nematode larvae and fungi were less common causes of skin disease. Although free-ranging white-tailed deer are common throughout North and South America, 13 information on their dermatopathies across this wide geographic region is limited.
Demodicosis (Demodex spp; family Demodicidae) has been documented in a variety of free-ranging mammals worldwide, 6,9,14 –16,18,25 –27 including white-tailed deer and other cervids such as mule deer (Odocoileus hemionus) and Rocky Mountain elk (Cervus elaphus nelsoni). 1,2,4,5,10 Demodex spp are symbiotic with their hosts; however, under certain circumstances, proliferation of mites can lead to localized or generalized disease. Skin lesions attributed to Demodex spp in white-tailed deer in the present study varied in distribution and severity and most commonly included alopecia and nodular epidermal thickening on the head, neck, trunk, and medial aspect of the limbs. Microscopic examination of grossly affected skin revealed varied numbers of mites within hair follicles and minimal inflammation, consistent with past observations, 6 except when associated with furunculosis. Although D. odocoilei has been documented in white-tailed deer, 5,6 the species of mites in the present study were not confirmed. Although Demodex spp are generally species specific, several species have been identified in white-tailed deer, including D. odocoilei and Demodex kutzeri. 5 Conversely, D. odocoilei has been documented in mule deer and black-tailed deer (Odocoileus hemionus columbianus); however, DNA analyses were not performed in these studies. 1,10
White-tailed deer with demodectic mange were most commonly observed during the fall months, which coincide with the breeding season and decreasing availability of food resources. Increased circulating sex and stress hormones, such as testosterone and cortisol, could contribute to immunosuppression, which may predispose or exacerbate existing infections. 4,5 Deer in the present study were often collected opportunistically, and the demographics of the deer (ie, adult males) may have been affected by increased visibility to hunters. In addition, adult animals may be better able to withstand long-term, ongoing infections or infestations and would therefore be more likely to be detected. Increased detections within the past 5 years could also reflect increased awareness or higher densities of deer in suburban areas.
While most observed demodectic mange cases among white-tailed deer manifested as localized infestations, generalized cases occasionally occur. The underlying reasons for the generalized manifestation of demodectic mange in deer are unknown but could reflect host immunologic or genetic factors or concurrent endocrine disorders, as has been suggested in domestic canids (Canis familiaris). 17,21,22 The effects of demodectic mange on the host are usually subclinical, and most white-tailed deer in the present study were in good nutritional condition and exhibited normal behavior. However, clinical disease in the host can result from parasite expansion, which is thought to be secondary to immunosuppression from transient or prolonged stress, poor nutrition, or concurrent infections. 2,4 –6,10,17 For example, crowding, seasonal food shortages, and concurrent lungworm infections were associated with severe demodicosis characterized by multifocal to generalized alopecia in roe deer (Capreolus capreolus) in Belgium. 4 Immune function is suspected to play a role in the manifestation of clinical demodicosis in numerous species. For instance, the occurrence of this disease in young dogs has been attributed to incomplete immune system development, 8 while Demodex folliculitis infestations occur in older, immunosuppressed humans. 7 Unlike some species, such as domestic dogs and African buffalo (Syncerus caffer), in which clinical demodicosis is thought to be more common in young animals, 12,29 demodectic mange was more commonly observed in adult white-tailed deer in the present study. The demographics of demodicosis cases in the present study may have been biased by the greater visibility of adult deer to biologists and hunters. Transfer of mites likely occurs during direct physical contact between suitable hosts, such as during mating, nursing, allo-grooming, and sparring between males. 12,29 While the initial onset and frequency of disease could not be determined among deer in the present study, demodectic mange appears to be established and widespread among white-tailed deer throughout much of the United States, based on the present as well as previous studies.
D. congolensis (family Dermatophilaceae) can cause skin disease in a variety of mammalian species, including humans and numerous domestic animal species, and is geographically widespread but more common in nontemperate regions. 3,19,30 In the present study, this bacterium caused disease of varying severity among white-tailed deer. Dermatophilosis was most common and often more severe in male deer ≤1 year of age. Consistent with past studies, 11,19 exudative crusts were often confined to the face, muzzle, and ear pinnae of fawns in the present study, although skin of the distal limbs adjacent to the coronary band was also commonly affected. These lesions were often concurrent with multifocal to generalized alopecia. 11,19,20 Adults often recover without complication; however, lesions in fawns may contribute to weakness, emaciation, shock, and death, as was the apparent outcome for the fawns with dermatophilosis in the present study. Transmission may be facilitated by contact between the fawn’s muzzle and the doe’s wet skin while nursing. 19
Additional skin pathogens observed in hunter-harvested white-tailed deer in the present study included bacteria such as Staphylococcus and Streptomyces spp; numerous ectoparasites such as mites, chiggers, lice, and ticks; and nematode larvae. Staphylococcus spp are common commensal bacteria of the skin that can cause disease when the skin’s barrier function is compromised or with immunosuppression. Streptomyces spp are ubiquitous, saprophytic, actinomycete bacteria that most likely cause opportunistic infections with traumatic implantation. A variety of ectoparasites have been observed on white-tailed deer in the United States, 3,6,16,24,28 and infestations may have been underreported in the present study, as the presence of mites and other ectoparasites in the field was likely often considered incidental. Microfilariae of the nematode Onchocerca cervipedis within the skin have been more commonly reported in mule deer and black-tailed deer vs white-tailed deer, and this parasite is rarely reported in white-tailed deer in the southeastern United States vs northeastern and western states. 3 Although the identity of the nematode larvae in the ear pinnae of white-tailed deer in the present study was most likely O. cervipedis based on previous observations, Elaeophora schneideri remains a possibility. The identities of parasites reported in white-tailed deer in the present study should be interpreted with caution because molecular confirmation was not performed.
Free-ranging deer and other wildlife have evolved with the ongoing and cyclic stresses associated with food scarcity and breeding activities. As habitat fragmentation and interactions between deer and humans increase, baseline stress levels may concurrently rise. The significance of the increased detections of generalized demodectic mange and the occurrence of dermatophilosis and other skin diseases of white-tailed deer in the southeastern United States are unknown. However, these detections underscore the need for monitoring diseases among white-tailed deer and other wildlife. Although the prevalence and overall impacts of dermatologic diseases in white-tailed deer are unknown, generalized demodectic mange appears to be non–population limiting and to occur as isolated cases. Similarly, reports of fatal dermatophilosis in deer are rare and more common in young animals. 3 However, these and many other infectious diseases appear to have few geographical limitations, and monitoring of wildlife diseases in light of changing climatic conditions and land use patterns is increasingly important.
Footnotes
Acknowledgements
The expertise of numerous SCWDS diagnosticians and technical staff made this work possible. We thank the field biologists and hunters, as well as all SCWDS member states, that contributed case material. Histology and bacterial and fungal cultures were performed at the Athens Diagnostic Laboratory at the University of Georgia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.