
Abstract
Canine nonangiogenic, nonlymphogenic, gastrointestinal sarcomas have been previously diagnosed as gastrointestinal stromal tumors (GIST), leiomyosarcomas, or nonspecified spindle cell sarcomas, but diagnostic criteria for each entity are poorly defined. We propose a classification for canine nonangiogenic, nonlymphogenic, gastrointestinal sarcomas based on microscopic, immunohistochemical, and molecular characteristics. Applying the classification to 40 canine nonangiogenic, nonlymphogenic, gastrointestinal sarcomas documented its diagnostic and prognostic value. Eighteen (45%) sarcomas were classified as GIST based on positive KIT immunoreactivity. All GISTs were positive for vimentin, 14 (78%) were positive for S-100, and 6 (33%) were positive for smooth muscle actin (SMA). In contrast to their human counterparts, canine GISTs occurred mainly in the small intestine (67%) but commonly metastasized (5/18) to liver, lymph nodes, and omentum. Six GISTs had an activated KIT mutation in exon 11 of c-Kit, but no mutations were detected in exons 8, 9, 13, and 17. Twelve (30%) sarcomas were classified as leiomyosarcomas based on positive labeling for SMA and negative labeling for KIT. Four of these neoplasms were well differentiated leiomyosarcomas characterized by weak to no labeling for vimentin, and 8 were poorly differentiated leiomyosarcomas characterized by strong labeling for vimentin. None of the leiomyosarcomas metastasized, but poorly differentiated leiomyosarcomas had a higher risk of local invasion. Ten (25%) sarcomas were classified as non-GIST/nonleiomyosarcomas that were negative for KIT and SMA but positive for vimentin and either S-100 and/or PGP 9.5. These neoplasms most likely represent sarcomas of neurogenic differentiation resembling Schwann cells or perineurial or endoneurial fibroblasts, respectively.
Primary canine mesenchymal gastrointestinal sarcomas that are not of angiogenic or lymphomatous origin (nonangiogenic, nonlymphogenic intestinal sarcomas) include leiomyosarcomas, neurofibrosarcomas, fibrosarcomas, and sarcomas of neurogenic origin. In the veterinary literature, these tumor entities are often identified as gastrointestinal stromal tumors (GISTs).18,26 In contrast to the case in human medicine, criteria to diagnose canine GISTs are not defined and the biological behavior of tumors classified as canine GISTs based on light microscopic features is highly variable.18,26 In fact, the terms GIST and leiomyosarcoma are commonly used interchangeably.18,26 Recent studies to more accurately diagnose and prognosticate nonangiogenic, nonlymphogenic intestinal sarcomas have attempted to better define canine GISTs.3,11,24,25,32
Human GISTs are recognized as a distinct tumor entity with neoplastic cells originating from the interstitial cells of Cajal and expressing CD117 (KIT protein). 45 GISTs are the most common mesenchymal gastrointestinal neoplasms in humans and can occur anywhere throughout the gastrointestinal tract, with a higher prevalence in the stomach followed by the small intestine.6,9 These neoplasms are characterized by a highly variable clinical behavior ranging from benign, indolent nodules to those that act like sarcomas and metastasize. 9 Human GISTs have a diverse microscopic appearance and have been classified into 4 basic morphologic patterns: spindle shaped (storiform), myxoid, fascicular, and epithelioid. 43 Positive labeling for KIT is necessary to make a diagnosis of GIST. The existence of GISTs that lack KIT expression is speculative. 11 Activating KIT mutations in exon 11 that lead to ligand-independent constitutive phosphorylation and activation of KIT are often implicated in the pathogenesis of GISTs.20,30,35
KIT-positive gastrointestinal sarcomas have been reported in dogs, horses, nonhuman primates, and a Fisher 344 rat.3,8,9,11,12,16,25,32,39,46 Unlike their human counterparts, canine GISTs have been primarily reported in the large and small intestine with few reports of occurrence in the stomach. 4 As in humans, the biological behavior of canine GISTs seems highly variable, ranging from a benign clinical presentation to aggressive neoplasms that have a propensity to metastasize.3,11,32,44 KIT mutations have only been reported in exon 11 of canine GISTs.11,15
Human leiomyosarcomas are rare, slow-growing, malignant tumors of smooth muscle origin that occur in all parts of the gastrointestinal tract but are most common in the colorectum.37,43 They vary from small intraluminal polypoid lesions to large transmural masses.37,43 They are composed of homogenous spindle cells that closely resemble normal smooth muscle cells to pleomorphic spindle cell sarcomas.34,35,43 However, even a high mitotic index rarely indicates a poor prognosis as long as complete excision can be achieved. 37 Leiomyosarcomas are positive for smooth muscle actin and desmin and negative for KIT.1,11,26 Canine leiomyosarcomas are most commonly found in older dogs in the jejunum and cecum, but their true prevalence is uncertain as a result of the recent definition of GISTs.1,4,6,7,22
Intestinal neurogenic sarcomas are uncommon in humans and animals and are diagnosed on their microscopic features as neurofibrosarcomas or malignant schwannomas.18,23,43,47,48 The World Health Organization (WHO) recently grouped these heterogenous neoplasms that originate from Schwann cells or modified Schwann cells, fibroblasts, or perineurial cells as peripheral nerve sheath tumors.17,23,47,48 They consist of spindle cells in a primarily storiform pattern with areas of whorling and palisading, Antoni A pattern.48,49 In contrast, Antoni B pattern is much less common and is characterized by cells in a loose network of fibers. Neoplastic cells are positive for S-100 protein, glial fibrillary acidic protein (GFAP), PGP 9.5, and vimentin and negative for smooth muscle actin and KIT. 17
There have been few comprehensive studies that attempt to classify canine nonangiogenic, nonlymphogenic intestinal mesenchymal tumors (NIMTs) other than as gastrointestinal stromal tumors. Canine NIMTs have variable histologic patterns, and therefore the diagnoses are often erroneous when based solely on morphologic characteristics. The present study proposes a classification of canine NIMTs based on morphologic, immunohistochemical, and molecular characteristics of this heterogenous group of neoplasms for more accurate diagnosis and better prognostication.
Material and Methods
Case Selection
A total of 40 formalin-fixed, paraffin-embedded (FFPE) tissue blocks of canine nonangiogenic, nonlymphogenic gastrointestinal sarcomas that had been submitted for routine biopsy between 1991 and 2006 to the Michigan State University Diagnostic Center for Population and Animal Health were included in this study. Neoplasms of the stomach and the small and large intestine were included as well as all cases with previous diagnoses of GIST, leiomyosarcoma, fibrosarcoma, spindle cell sarcoma, undifferentiated sarcoma, and anaplastic sarcoma. All cases had sufficient amounts of FFPE tissues for routine 5-μm hematoxylin and eosin staining, immunohistochemistry, and DNA extraction.
Immunohistochemistry
Antibodies to the following antigens were used to label all 40 neoplasms: KIT (CD117), smooth muscle actin (SMA), desmin, vimentin, S-100, and PGP 9.5. Other antibodies used for selected neoplasms included factor VIII related antigen, pancytokeratin, and CD18. Antibodies against S-100 (1:800), desmin (1:400), KIT (1:300), and SMA (1:50, all Dako North America, Inc, Carpinteria, CA) were run on the Bond maX autostainer using the Bond Polymer Detection System (Leica Microsystems GmbH, Wetzlar, Germany), whereas the antibody against vimentin (RTU, Ventana Medical Systems, Inc, Phoenix, AZ) was run on the Bench Mark autostainer using an Enhanced V Red Detection System (Alk. Phos. Red) System (Ventana Medical Systems, Inc). For both systems, slides were counterstained with hematoxylin. Positive controls included normal canine skeletal muscle, brain, small intestine, and a mast cell tumor. For negative controls, the primary antibodies were replaced with homologous nonimmune sera.
Morphologic and Immunohistochemical Evaluation
Mesenchymal neoplasms (40) that originated from the gastrointestinal tract with histologic criteria of malignancy were classified as nonangiogenic, nonlymphogenic gastrointestinal sarcomas. Vascular and hematopoietic sarcomas were excluded. Criteria of malignancy included metastasis, local invasion of surrounding tissue, increased cellularity, anisokaryosis and anisocytosis, and numerous or abnormal mitotic figures. The nonangiogenic, nonlymphogenic gastrointestinal sarcomas were further classified as GISTs, leiomyosarcomas, and non-GIST/non–smooth muscle sarcomas. A diagnosis of GIST was based on positive expression of KIT regardless of the coexpression of SMA, vimentin, desmin, S-100, or PGP 9.5. GISTs were subdivided into 4 distinct morphologic patterns based on the WHO’s Histologic Classification of Tumors of the Alimentary System (AFIP fascicle): spindle shaped (storiform), epithelioid, myxoid, and fascicular. Nonangiogenic, nonlymphogenic gastrointestinal sarcomas were classified as leiomyosarcomas when they were negative for KIT and positive for SMA regardless of their immunoreactivity for vimentin, desmin, S-100, or PGP 9.5. Leiomyosarcomas were further subdivided into well differentiated and poorly differentiated based on the lack of or intensity of vimentin expression, respectively. Nonangiogenic, nonlymphogenic gastrointestinal sarcomas were classified as non-GIST/nonleiomyosarcomas when negative for KIT and SMA.
Molecular Evaluation of FFPE Sections
Neoplastic tissue from all 18 GISTs (KIT positive sarcomas), less than 1 mm3, was excised from each FFPE block to retrieve sections corresponding to immunohistochemistry (IHC) positive KIT areas. Similarly, sections of histologically normal tissue, negative for KIT immunolabeling, were also collected from each case. DNA was isolated as previously described.2,15,54
Exons 8, 9, and 11, coding for the juxtamembrane domain of KIT, and exons 13 and 17, coding for the kinase domain of KIT, were amplified from tissue sections via PCR using primers and conditions optimized in earlier studies.15,21,51,52 Amplified fragments from all tissue sections were submitted for automated sequencing as previously described. 15
Results
The dogs ranged in age from 1 to 15 years. A variety of small, medium, and large-sized breeds were represented in the study population. Most neoplasms presented as single, nodular masses arising in the wall of the small or large intestine (Fig. 1). Metastases to liver (n = 1), mesenteric lymph nodes (n = 2), or omentum (n = 4) were present in 7 cases and transmural invasion in 24 cases (Table 1).
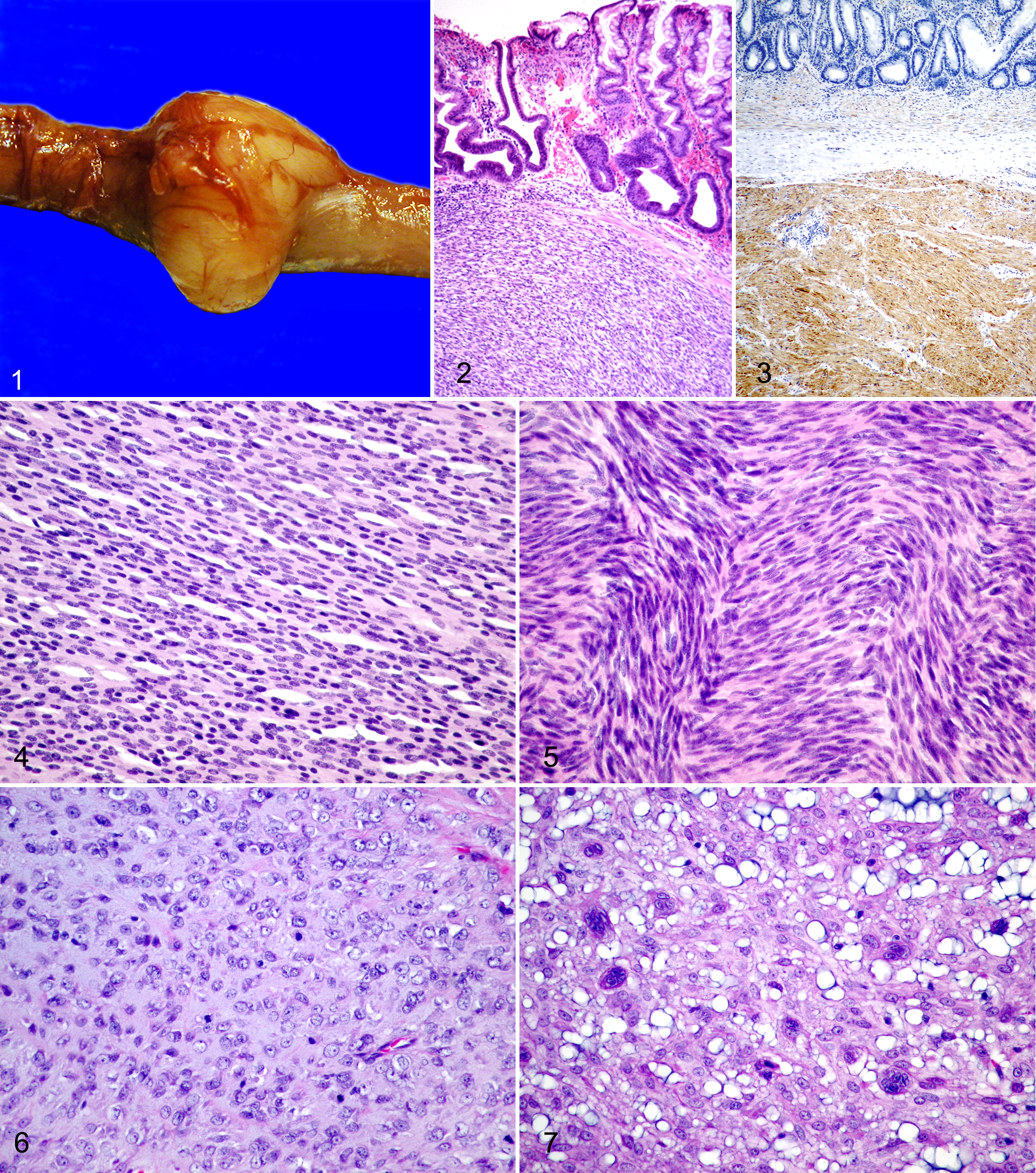
Small intestine, GIST; dog No. 1. Single, nodular mass arises in the wall of the small intestine.
Summary of Signalment, Diagnoses, and Occurring Metastases for 40 Dogs With Nonangiogenic, Nonlymphogenic Intestinal Sarcomas.
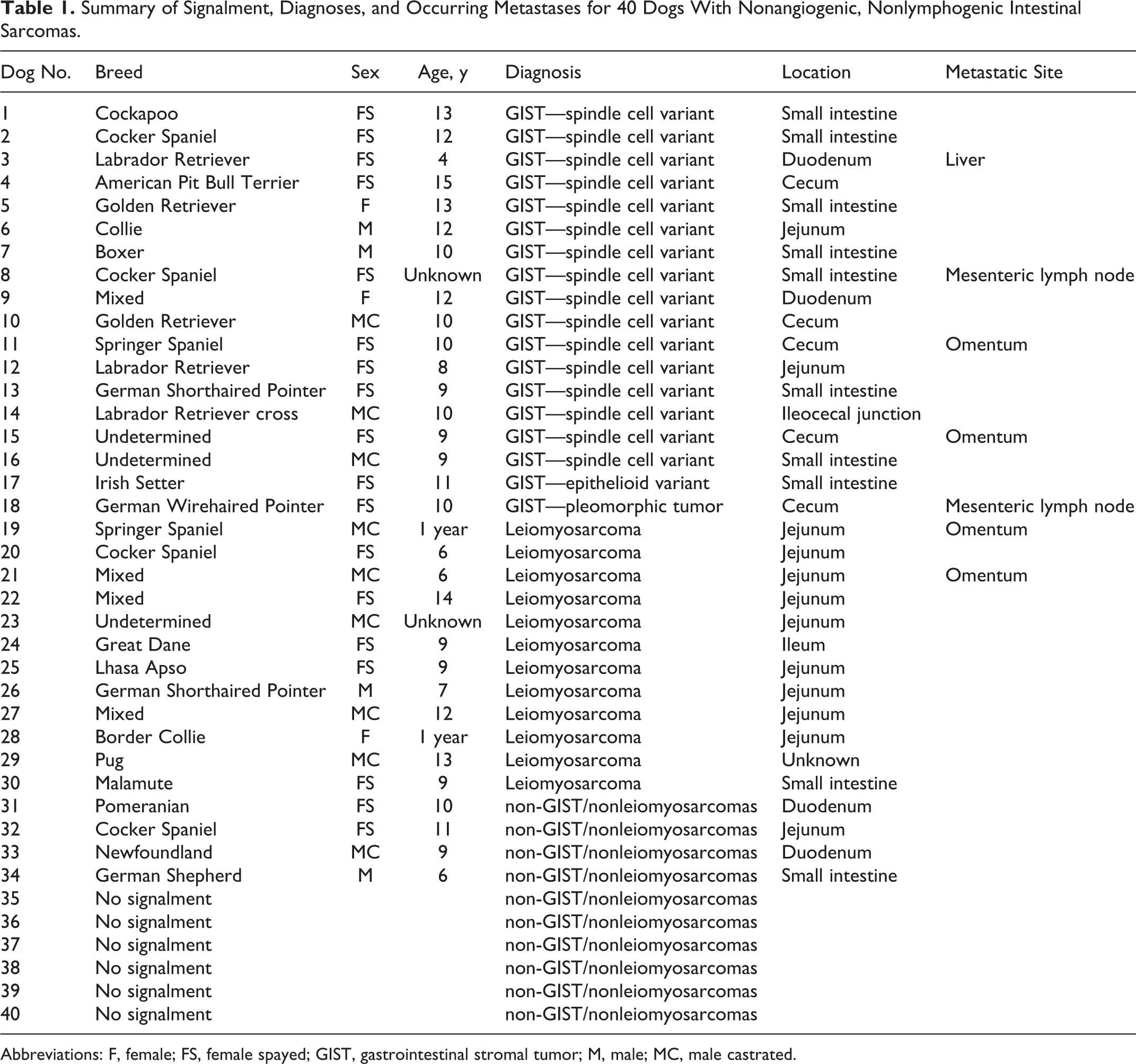
Abbreviations: F, female; FS, female spayed; GIST, gastrointestinal stromal tumor; M, male; MC, male castrated.
Gastrointestinal Stromal Tumors
Eighteen (45%) nonangiogenic, nonlymphogenic, gastrointestinal sarcomas were classified as GISTs (Fig. 2) based on at least 70% positive immunohistochemical labeling for KIT. All 18 GISTs were positive for vimentin (Fig. 3). Fourteen (78%) GISTs were also positive for S-100 and 6 (33%) were positive for α-SMA. One GIST labeled positive for PGP 9.5. All GISTs were negative for desmin.
GISTs were detected in 13 female and 5 male dogs ranging from 4 to 15 years of age (with the exclusion of 1 Cocker Spaniel of unknown age) with an average age of 9.9 years. Twelve (67%) GISTs were located within the duodenum, jejunum, or ileum. Five (27%) were located within the cecum. One GIST was located at the ileocecal junction. There were no gastric GISTs. All GISTs were primarily localized in the submucosa and muscularis but expanded transmurally and invaded at least focally into the propria mucosa. Five GISTs had metastatic foci within the liver (dog No. 3), mesenteric lymph nodes (dog Nos. 8 and 18), or omentum (dog Nos. 11 and 15).
Two distinct morphologic cell patterns were observed: spindloid (storiform or palisading) and epithelioid (Figs. 4 –6). Sixteen GISTs spindloid characterized by a population of loose to dense spindle cells arranged in a storiform pattern resembling leiomyosarcomas (Fig. 4) or were palisading, resembling Schwannomas (Fig. 5). The spindloid pattern was often accompanied by smaller clusters of epithelioid cells. In general, neoplastic cells were supported by a dense fibrous stroma; contained moderate to abundant, lightly eosinophilic, wispy cytoplasm; and had indistinct cell borders. In most GISTs, neoplastic cells contained round to ovoid, spindle- to cigar-shaped, hyperchromatic nuclei with mild anisokaryosis and an indistinct, single nucleolus. The mitotic index was variable and ranged from 0 to 3 mitotic figures per 5, 400× fields. The majority of GISTs had multiple regions of hemorrhage and necrosis surrounded by variable numbers of hemosiderin-laden macrophages and neutrophils. One GIST was highly vascular with dilated vessels and neoplastic cells multifocally surrounded by large, cavernous, blood-filled spaces with variable numbers of siderophages. The neoplastic cells were negative for factor VIII related-antigen (endothelial marker) and positive for KIT.
Only one GIST exhibited an epithelioid pattern (Fig. 6). Neoplastic cells were arranged in sheets separated by dense fibrous tissue. There were moderate anisokaryosis and anisocytosis. Neoplastic cells were round to polygonal with abundant, slightly basophilic, stippled cytoplasm and indistinct cell borders. Nuclei were round to polyhedral with a stippled to open chromatin pattern and 1 to 4 nucleoli. The mitotic index was 0 to 1 per 400× field.
One GIST was highly pleomorphic (Fig. 7) and was composed of sheets of round to polyhedral, mesenchymal cells that were supported by abundant, fibrous to slightly basophilic, myxoid to fatty connective tissue stroma. Neoplastic cells had abundant, slightly basophilic cytoplasm and indistinct cell borders. Throughout the neoplasm, large numbers of neoplastic cells contained 3 to 10 nuclei and had abundant eosinophilic cytoplasm (multinucleate cells). Nuclei were round to polyhedral with marked anisokaryosis. Nuclei had stippled chromatin and an indistinct or single nucleolus. Mitotic figures were not present in the examined sections. The GIST was infiltrated by large numbers of lymphocytes and plasma cells. There were multifocal regions of hemorrhage and necrosis surrounded by moderate numbers of neutrophils. The neoplasm was negative for CD18 and positive for KIT. The marked pleomorphism of this particular GIST did not allow simple classification into 1 of the 4 patterns but may be best characterized as an epithelioid pattern.
KIT Mutation Status
Of the 18 KIT immunopositive cases, 17 cases yielded amplification products. Mutations were identified in 6 dogs (dog Nos. 1, 4, 11, 14, 15, and 18). 15 The mutation in 2 cases consisted of a 6–base pair deletion eliminating 2 amino acids, tryptophan and lysine at codon 556 and 557 respectively. 15 Another mutation in 4 cases resulted in a 6–base pair deletion eliminating lysine and valine at codons 557 and 558. 15 The deletion of the last 2 guanines of codon 556 in this mutation combined with deletion of the next 4 nucleotides resulted in an amino acid change from tryptophan to phenylalanine. 15
Leiomyosarcoma
Twelve (32%) of the nonangiogenic, nonlymphogenic gastrointestinal sarcomas were classified as leiomyosarcomas based on negative labeling for KIT and positive labeling for SMA (Figs. 8 –13). Four neoplasms that had strong labeling for desmin (Fig. 9) and no to minimal labeling for vimentin (Fig. 10) were classified as well-differentiated leiomyosarcomas, and 8 leiomyosarcomas that had weak labeling for desmin (Fig. 12) and strong immunohistochemical labeling for vimentin (Fig. 13) were classified as poorly differentiated leiomyosarcomas. Seven (58%) leiomyosarcomas were positive for desmin. Two neoplasms were positive and 2 were focally positive for PGP 9.5. Four neoplasms were diffusely positive, and 2 were focally positive for S100.
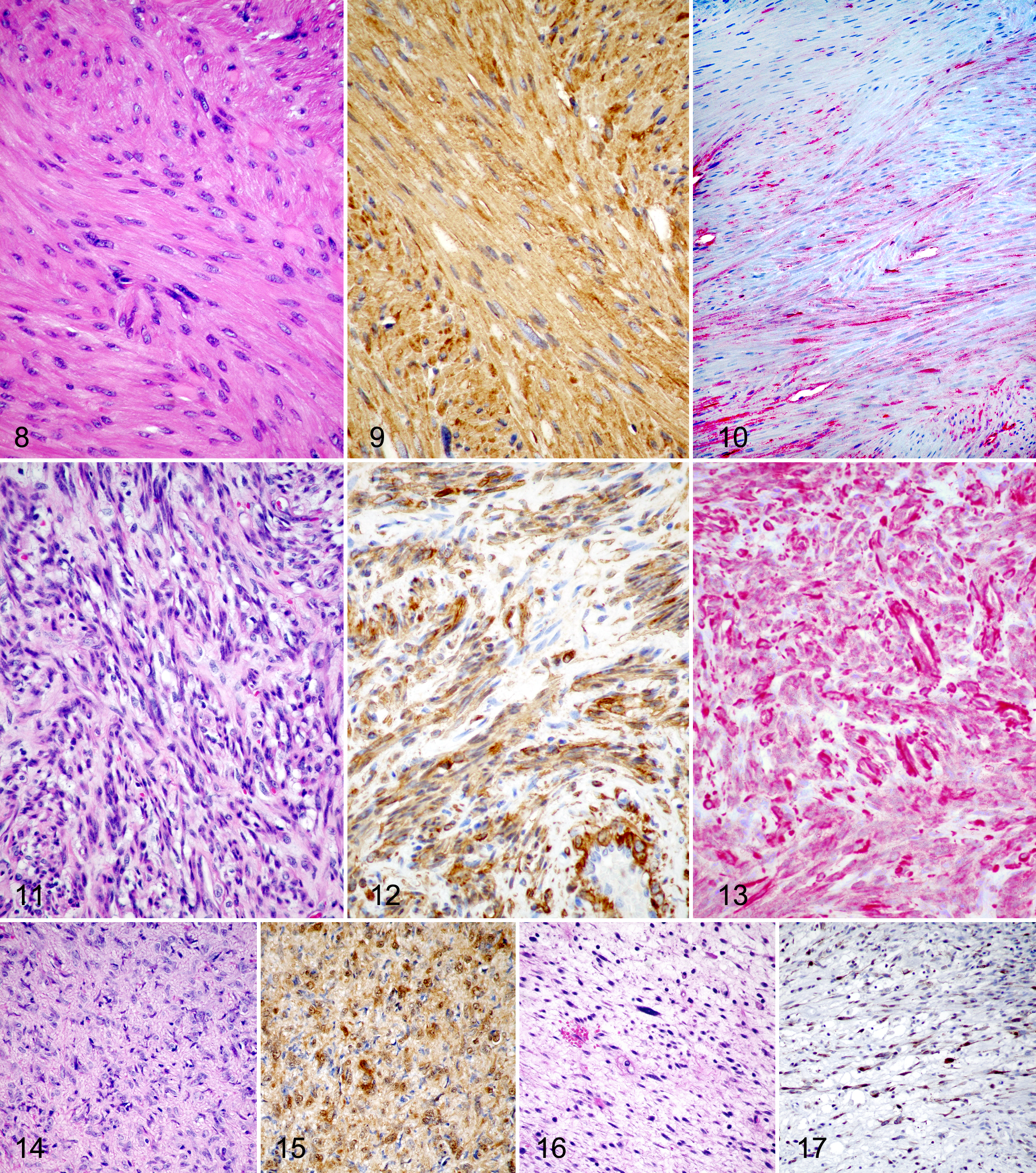
Ileum, well-differentiated leiomyosarcoma; dog No. 30. Spindle cell neoplasm with low cellular density composed of bundles and streams of well-differentiated smooth muscle cells that are cigar shaped with abundant deeply eosinophilic cytoplasm and indistinct cell borders. HE.
Leiomyosarcomas were detected in 12 dogs ranging from 1 to 14 years of age with an average of 7.5 years. There was no breed or sex predilection. Eleven (92%) leiomyosarcomas were located within the duodenum, jejunum, or ileum. One was located in the cecum. Two tumors had metastasized to the omentum (dog Nos. 19 and 21).
The 4 well-differentiated leiomyosarcomas had low cellular density and were composed of bundles and streams of well-differentiated leiomyocytes. Neoplastic cells were spindle to cigar shaped and had abundant, deeply eosinophilic, wispy cytoplasm and indistinct cell borders (Fig. 8). Nuclei were spindloid, and there was mild anisokaryosis. Nuclei were hyperchromatic with indistinct nucleoli. Mitotic figures were not present in sections examined. The 8 poorly differentiated leiomyosarcomas were markedly cellular and composed of poorly organized bundles and streams of mesenchymal cells supported by a loose, fibrous, often edematous stroma (Fig. 11). Neoplastic cells were spindle to cigar shaped and had abundant, slightly eosinophilic cytoplasm and indistinct cell borders. Nuclei were hyperchromatic and spindloid with indistinct nucleoli, moderate anisokaryosis, and anisocytosis. Six of the poorly differentiated leiomyosarcomas were transmurally invasive, and 2 neoplasms invaded the adjacent omentum.
Non-GIST/Nonleiomyosarcomas
Ten (26%) of the nonangiogenic, nonlymphogenic gastrointestinal sarcomas were classified as non-GIST/nonleiomyosarcomas based on negative labeling for KIT and SMA. All non-GIST/nonleiomyosarcomas labeled positive for vimentin. Neoplasms in this category had variable cellular and immunohistochemical patterns, with 2 additional entities being noticed in particular (Figs. 14 –17). Four non-GIST/nonleiomyosarcomas (40%) were positive for S-100 (Fig. 15) but negative for PGP 9.5, and 4 (40%) non-GIST/nonleiomyosarcomas were positive for PGP 9.5 (Fig. 17) but negative for S-100. The other 2 sarcomas were positive for S-100 and PGP 9.5.
Non-GIST/nonleiomyosarcomas were present in 4 dogs ranging from 6 to 11 years of age with an average of 9 years. Signalment (age, breed, sex) and tumor location were not available for 6 animals. Based on the available signalment, these 4 neoplasms were located within the small intestine. All non-GIST/nonleiomyosarcomas were primary localized in the submucosa and muscularis with no evidence of mucosal or omental invasion.
The S-100 positive sarcomas were composed of densely arranged clusters, whorls, and bundles of neoplastic mesenchymal cells supported by fibrous stroma. These neoplasms lacked an Antoni type A pattern and were composed entirely of wispy cells separated by basophilic mucin, often described as an Antoni type B pattern in peripheral nerve sheath tumors.5,48,49 Neoplastic cells were spindloid to stellate and had scant to moderate eosinophilic cytoplasm and indistinct cell borders. Nuclei were mildly pleomorphic (Fig. 14) and hyperchromatic with 1 distinct basophilic nucleolus. The mitotic index was low. The PGP 9.5 positive sarcomas were composed of loosely arranged sheets of mesenchymal cells supported by a scant, slightly eosinophilic, fibrous stroma. Neoplastic cells were stellate to spindloid and had scant, wispy eosinophilic cytoplasm and indistinct cell borders (Fig. 17). Nuclei were round to stellate with moderate anisokaryosis. Nuclei were hyperchromatic with indistinct nucleoli and a low mitotic index.
Discussion
Using immunohistochemistry to more accurately diagnose canine nonangiogenic, nonlymphogenic gastrointestinal sarcomas, we classified 45% of the examined sarcomas as GISTs based on at least 70% positive labeling for KIT. Coexpression of KIT with immunohistochemical markers specific for smooth muscle (SMA and desmin) or a neuronal origin (neuron specific enolase, PGP 9.5 and S-100) has been previously documented in human GISTs and has been confirmed in dogs in this study and others.3,11,25,32,35,38,44 Furthermore, these coexpression studies have long suggested that canine GISTs are capable of multidirectional differentiation, which can be explained by the distribution of interstitial cells of Cajal (ICC) or that GISTs arise from a primitive mesenchymal cell that is capable of differentiation into muscle or ICC.3,11,17,26,33,35,36,44,45
The current study investigated the morphologic characteristics of these multidirectional tumors and divided them into 2 basic morphologic patterns: spindloid/storiform and epithelioid. The most common histologic variant among human GISTs is the spindloid/storiform pattern followed by the epithelioid variant.35,43 A mixture of these patterns is often present. Similar to human studies, the vast majority of the GISTs in the current study had a spindle cell pattern. Mixed spindle and epithelioid (usually focal) patterns were observed in a few neoplasms.
The proto-oncogene c-Kit encodes a receptor tyrosine kinase (KIT) that plays an important role in proliferation and differentiation of a number of different cell types, including ICC.40,50,51 Activation of c-Kit mutations has been implicated in the carcinogenesis of multiple human and canine neoplastic diseases, including canine mast cell tumors and canine GISTs.11,30,38,51 Activating c-Kit mutations are present in approximately half of human GISTs and occur most commonly in exon 11 of the juxtamembrane domain.20,31 Similar mutations have been described in canine cutaneous mast cell tumors, leading to the licensing of the first FDA-approved dog-specific anticancer drugs, tyrosine kinase inhibitors (TKIs), to specifically treat these neoplasms.29,52 In the study described herein, 17 of 18 GISTs yielded amplification products, and 6 GISTs were found to have deletion mutations in exon 11 of c-Kit similar to previously described mutations in canine and human GISTs and canine mast cell tumors.11,35,51 No mutations were detected in exons 8, 9, 13, and 17 of c-Kit. Whether canine GISTs represent a therapeutic target for TKIs remains unclear. However, the central role of KIT in GIST tumorigenesis as evidenced by the expression of KIT and the identification of these activating mutations in c-Kit are strong indicators for the potential benefit of TKIs for the treatment of canine GISTs.
A small subset of GISTs may lack detectable KIT protein overexpression. When compared with KIT positive GISTs, these KIT immunonegative tumors in humans have been reported to likely be of epithelioid morphology, contain platelet-derived growth factor receptor alpha (PDGFRA) oncogenic mutations, and arise in the omentum/peritoneal surface, whereas the majority of KIT positive neoplasms arise in the stomach. 33 PDGFRA mutations account for 5% to 10% of known mutations in human GISTs. 55 Approximately 9% to 15% of human GISTs do not exhibit mutations in either KIT or PDGRA and are termed wild-type. 55 In rare cases, these lesions may have typical morphologic characteristics of GISTs and appear to be immunohistochemically inert due to fixation or processing artifact and, in limited cases, due to sampling error. 10 Recent studies have shown that antibodies against DOG1.1 have superior sensitivity and specificity compared with KIT and CD34 in diagnosing human GISTs and that these antibodies can detect KIT negative tumors irrespective of the underlying mutation or KIT expression by IHC. 28 At the time of manuscript preparation, this study was one of the few canine classification studies in which GISTs have been categorized into distinct histologic variants (epithelioid and spindloid), and the rare occurrence of epithelioid GISTs in our study suggests that potentially occurring KIT negative GISTs are exceedingly rare in dogs. To date, PDGFRA mutations and DOG1.1 immunohistochemical labeling have not been investigated in canine GISTs.
Aside from immunophenotyping and comparable origins to human GISTs, very little is known about the sex, breed, and anatomic site predilection or prognostic indicators for canine GISTs. Similar to humans and previous canine reports, GISTs in the current study occurred in dogs with a median age of approximately 10 years. Although a sex predilection has not been reported in previous studies, female dogs were overrepresented in the current study.3,11,44 In humans, many parameters have been proposed to distinguish benign from malignant GISTs and to determine the metastatic potential of these neoplasms.10,27 The proposed risk assessment for human GISTs is based on tumor size and mitotic activity, with the most important cutoffs being tumor size. 10 There is strong evidence that gastric GISTs have a much lower rate of aggressive behavior than jejunal and ileal GISTs of similar size and mitotic activity.36,37 Thus, location is an additional parameter in risk assessment in human GISTs. Parameters for risk assessment have only recently been investigated in dogs. 14 A significant difference exists among mitotic index, AgNOR, and Ki67 scores depending on location of the tumors, with small intestinal GISTs having greater values than large intestinal GISTs. 14 The results of the current study indicate a higher degree of malignancy and metastatic potential of small intestinal GISTs compared with other nonangiogenic, nonlymphogenic gastrointestinal sarcomas, similar to the results of a previous study. 11 A prospective study assessing disease-free survival times following surgical excision and metastases is needed to further characterize the malignant potential of canine GISTs.
Among the 40 nonangiogenic, nonlymphogenic, gastrointestinal sarcomas in the current study, only 12 of 40 (30%) were classified as leiomyosarcomas based on negative labeling for KIT and positive labeling for SMA. Akin to leiomyosarcomas in humans, previous reports describing the morphologic characteristics, incidence, and biological behavior of canine leiomyosarcomas predate the use of IHC to detect KIT. Therefore, the clinical behavior of true canine leiomyosarcomas is confounded by the presence of a large proportion of GISTs.8,18,26 Canine leiomyosarcomas in our study were found throughout the small intestinal tract with no site predilection. More important, whereas earlier studies reported metastatic rates for gastrointestinal leiomyosarcomas between 16% and 50%, including metastases to liver and spleen, only 2 (16%) leiomyosarcomas in our study invaded into the adjacent mesentery and there was no evidence of distant metastases.6–8,22 In contrast, canine GISTs had a much higher metastatic rate of 28% (5/18), including liver metastases.
In addition to accurately distinguishing GISTs from leiomyosarcomas, we observed strong expression of vimentin and weak SMA and desmin expression in highly cellular, poorly differentiated leiomyosarcomas with microscopic features of malignancy. Similarly, well-differentiated leiomyosarcomas had negative to minimal expression of vimentin and strong labeling for SMA and desmin. Similar findings were reported in another canine GIST classification study. 26 Several investigators propose that the differentiation or dedifferentiation of malignant smooth muscle tumors is comparable to that of primitive myoblasts, which express primarily vimentin and little desmin, but as maturation progresses, desmin becomes the predominant intermediate filament.1,13,26 Thus, strong vimentin and weak desmin expression may predict malignant behavior in leiomyosarcomas. In humans, prognostic indicators for leiomyosarcomas include immunohistochemical detection of MDR-1 gene product P-glycoprotein (P-gp) and multidrug resistance protein-1 (MRP-1). 41 Overexpression of these proteins is associated with multidrug resistance to numerous natural product drugs such as anthracyclines that are widely applied chemotherapeutics. Expression of multidrug resistant proteins are less pronounced in leiomyosarcomas when compared with GISTs, suggesting that these neoplasms may be more sensitive to conventional chemotherapeutic agents than GISTs. 41 Prognostic indicators for canine gastrointestinal leiomyosarcomas have not been investigated. Consequently, our findings provide a novel approach for the prognosis of leiomyosarcomas using IHC for vimentin, SMA, and desmin and extend previously suggested classification schemes. Our data also suggest a more aggressive behavior of poorly differentiated leiomyosarcomas.3,11,32,44
We observed 2 distinct cellular/immunohistochemical patterns in non-GIST/nonleiomyosarcomas. Although S-100 and PGP 9.5 are expressed in a wide variety of tissues and mesenchymal neoplasms, both have been described as useful markers to identify neurogenic differentiation, and considering morphologic characteristics and IHC phenotype, we speculate that these neoplasms may represent malignant peripheral nerve sheath tumors.4,5,17,42 Malignant peripheral nerve sheath tumors are possibly composed of several cell types: Schwann cells, perineurial cells, or perineurial or endoneurial fibroblasts.5,19,49 The sarcomas that were positive for vimentin and S-100 commonly exhibited an Antoni type B pattern similar to that reported for canine peripheral nerve sheath tumors but lacked an Antoni type A pattern and Verocay bodies. 48 Sarcomas that were PGP 9.5 positive and S-100 negative may arise from a different cell type. One possibility for the lack of S-100 immunostaining is that the predominant neoplastic cell type is derived from cells other than Schwann cells. 5 Another possibility is suboptimal S-100 antigen preservation in Antoni B regions. Some researchers now contend that these are degenerated Antoni A regions. 53
Recent studies of canine nonangiogenic, nonlymphogenic, gastrointestinal sarcomas have primarily focused on the clinicopathologic features of GISTs.18,26 With the recent recognition of canine GISTs as a specific neoplastic entity, it has become increasingly important to differentiate GISTs from leiomyosarcomas and other nonangiogenic, nonlymphogenic, gastrointestinal sarcomas. Following our proposal, IHC for KIT, SMA, vimentin, S-100, and PGP 9.5 will allow a more accurate diagnose of these neoplasms and provide more accurate information about their biological behavior. Little light has been shed on the molecular aspects of canine GISTs, and in this study, activated c-Kit mutations were identified in 6 GISTs. Although we were unable to identify activated mutations in all GISTs, the successful use of TKIs in the treatment of canine mast cell tumors that contain similar c-Kit mutations suggests that a similar therapeutic approach should be investigated for canine GISTs. Despite the advances in accurately distinguishing gastrointestinal leiomyosarcomas from GISTs, further prospective studies are necessary to clarify the behavior of these and other canine nonangiogenic, nonlymphogenic, gastrointestinal sarcomas and to more accurately determine their response to various therapeutic approaches.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.