
Abstract
The clinical, clinicopathologic, and pathological findings of 9 dogs with T-cell lymphoma that involved the liver in the absence of peripheral lymphadenopathy were assessed. Seven dogs had hepatosplenic T-cell lymphoma (HS-TCL). Dogs with HS-TCL presented with hepato- and/or splenomegaly, regenerative anemia, thrombocytopenia, and hypoproteinemia. The clinical course was rapidly progressive with all dogs but 1 dead within 24 days of initial presentation. Neoplastic lymphocytes were centered on hepatic and splenic sinusoids and had a CD3+ (5/7), TCRαβ– (5/5), TCRγδ+ (3/5), CD11d+ (6/7), granzyme B+ (5/7) immunophenotype. Bone marrow and lungs were consistently but variably involved. These findings closely resemble the human disease and support the classification of HS-TCL as a distinct World Health Organization entity in dogs. The remaining 2 dogs markedly differed in the pattern of hepatic involvement by neoplastic lymphocytes, which were not confined to hepatic sinusoids but invaded hepatic cords. In addition, neoplastic cells had a CD11d– immunophenotype, and clinicopathologic data indicated marked cholestasis and mild to absent anemia. Based on the distinct tropism of neoplastic lymphocytes for hepatocytes, the name hepatocytotropic T-cell lymphoma (HC-TCL) is proposed. Given the histomorphologic, clinicopathologic, and immunophenotypic differences, HC-TCL likely represents a separate biological entity rather than a histomorphologic variant of HS-TCL.
Keywords
Considerable effort has been directed toward a generally accepted classification scheme for canine lymphomas. 19 An appropriate classification scheme should adequately group tumors into clinicopathologic entities and serve as a basis for prediction of biological behavior and choice of treatment. With advances in research and diagnostic methods, classification schemes are subject to constant refinement and evolution.
The current most commonly accepted classification scheme for human lymphomas is the World Health Organization (WHO) system. 18 The majority of WHO entities are defined by clinical, morphological, immunophenotypic, and genetic criteria. One such example is hepatosplenic T-cell lymphoma (HS-TCL). HS-TCL is defined as a T-cell lymphoma that is centered on the liver and spleen without significant involvement of peripheral lymph nodes. 18 HS-TCL is thought to arise from splenic cytotoxic T cells and is predominantly of γδ T-cell origin.1,4,16,21 Patients clinically present with splenomegaly and/or hepatomegaly, thrombocytopenia, and anemia. Histologically, neoplastic cells are predominantly found within splenic and hepatic sinusoids with concurrent bone marrow involvement in most cases.
HS-TCL has recently been adopted as a new entity in the canine WHO classification. However, so far only 2 cases have been reported in dogs.3,6 Although these cases resembled the human disease, their singularity precluded identification of general characteristics of HS-TCL in dogs. Additional data are needed to more precisely characterize this tumor type and to validate its status as a distinct WHO entity in dogs.
In contrast to HS-TCL, other WHO entities are more heterogeneous and include a range of different tumor types that have not been further characterized. One such example, in humans as well as in dogs, is peripheral T-cell lymphoma–not otherwise specified (PTCL-NOS).18,19 In humans, this entity is being refined as more neoplasms are classified with the help of immunophenotypic or genetic markers. Analogously, a more comprehensive analysis of poorly characterized canine T-cell tumors is needed. This will result in the identification of new clinicopathologic entities and ultimately improve diagnosis and treatment through refinement of the current classification scheme.
The objective of this study was to examine 9 canine lymphomas that involved the liver in the absence of peripheral lymphadenopathy. Clinical, clinicopathologic, and pathological data were evaluated. Seven dogs were diagnosed with HS-TCL, which supports its classification as a distinct WHO entity in this species. In 2 dogs, the pattern of liver infiltration, immunophenotype, and clinicopathologic features differed markedly. On the basis of the distinct tropism of neoplastic cells for hepatic cords, the name hepatocytotropic T-cell lymphoma (HC-TCL) is proposed. The findings of this study support the notion that HC-TCL represents a distinct biological entity that warrants classification separate from HS-TCL and PTCL-NOS.
Materials and Methods
Case selection
The electronic medical records of the Veterinary Medical Teaching Hospital (VMTH) of the University of California, Davis were searched for dogs that had histologically confirmed lymphoma in liver without peripheral lymphadenopathy.
Nine cases were retrieved and consisted of 8 necropsy specimens and 1 biopsy specimen. Clinical, clinicopathologic, and pathological data were reported previously for 1 dog (dog No. 1). 6 Complete blood counts (CBCs), done on an ADVIA 120 (Siemens Healthcare Diagnostics, Deerfield, Illinois); serum biochemical results (Hitatchi 917; Roche, Basel, Switzerland); urinalysis; and coagulation profiles were downloaded into an Excel spreadsheet for evaluation (Excel; Microsoft Corp, Redmond, Washington). When available, Wright-Giemsa–stained aspirate smears and immunocytochemically stained smears were reviewed. Lymphomas were classified based on the histologic pattern of liver involvement. In HS-TCL, neoplastic lymphocytes were confined to the sinusoids, whereas neoplastic lymphocytes in HC-TCL also invaded hepatic cords.
Statistical analysis
Differences in clinicopathologic analytes between HS-TCL and HC-TCL were analyzed using a 1-tailed Mann-Whitney test (Analyse-it Software, Ltd, Leeds, UK). For all analyses, significance was set at P < .05. To further assess the clinicopathologic data, a complete-linkage hierarchical cluster analysis using an L2 dissimilarity measure was done (Stata/IC 12.1; StataCorp LP, College Station, Texas), using the following: hematocrit; concentrations of platelets, white blood cells, neutrophils, bands, and unclassified cells; total protein; albumin; globulin; alkaline phosphatase (ALP); γ-glutamyltransferase (GGT); alanine aminotransferase (ALT); total bilirubin; and cholesterol.
Antibodies
Mouse monoclonal antibodies (mAbs) specific for canine leukocyte antigens were developed in one author’s laboratory (PFM). They included mAbs specific for canine CD3 (CA17.2A12 and CD3-12), CD4 (CA13.1E4), CD8α (CA9.JD3), CD8β (CA15.4D2), CD11d (CA18.3C6), TCRβ subunit (CA15.8G7), and TCRγδ (CA20.8H1 and CA20.6A3). These antibodies have been extensively characterized by immunohistology, multiparameter flow cytometry, antigen immunoprecipitation, and in some instances by functional studies and reactivity with cloned canine recombinant proteins. A rabbit antihuman polyclonal antibody was used for the detection of granzyme B (E2580; Spring Biosciences, Fremont, California).
Tissue handling and immunohistochemistry
Tissues from all dogs were fixed in 10% neutral buffered formalin and embedded in paraffin, and 5-μm-thick sections were stained with hematoxylin and eosin (HE). In addition, tissues from 6 dogs were snap frozen in isopentane, which was cooled to freezing point in liquid nitrogen. Immunohistochemistry was done using a streptavidin–horseradish peroxidase method as previously described. Immunohistochemistry for granzyme B was performed according to the manufacturer’s recommendations. Appropriate positive controls were run. Negative controls were done by omission of the primary antibody or by substitution of an irrelevant primary antibody (Fe1.7B12 specific for feline CD4).
Electron microscopy
Formalin-fixed liver tissue of 1 HC-TCL (dog No. 8) was postfixed in osmium tetroxide and embedded in epoxy resin, and ultrathin sections were stained with uranyl acetate and lead citrate.
Clonality assay
T cell receptor γ (TRG) gene rearrangements were assessed with a novel multiplex polymerase chain reaction (PCR) as described elsewhere. 11 The assay was based on the complete description of the canine TRG locus and covered all rearranged variable and joining genes.12,13 In short, DNA was extracted from paraffin blocks of liver and/or spleen according to the manufacturer’s recommendations (DNeasy tissue kit; Qiagen, Valencia, California). PCR reactions were run in triplicate. Products were size separated using capillary electrophoresis (eGene HDA-GT12; Qiagen). A sample was regarded clonal if at least 1 band/peak of identical size was seen in each of the simultaneously run triplicates.
Results
Clinical features
Dogs with HS-TCL were 5 to 18 years (median age, 11.5 years), and dogs with HC-TCL were 6 and 12 years (Table 1). The clinical history for both entities was similar and included progressive lethargy, anorexia, weight loss, diarrhea, and vomiting ranging from 1 week to 3 months prior to presentation to the UC Davis VMTH. Physical examination revealed cranial abdominal organomegaly in all dogs as well as icteric mucus membranes in both dogs with HC-TCL and 1 dog with HS-TCL. Diffuse hepatomegaly and splenomegaly with or without altered echotexture were noted ultrasonographically in 4 and 6 dogs with HS-TCL, respectively. One dog with HC-TCL (No. 9) had both hepatomegaly and splenomegaly. Other findings in dogs with HS-TCL included abdominal effusion (1) and pleural effusion (1). One of the dogs with HC-TCL (dog No. 8) had a severely thickened gallbladder wall and was taken to surgery for cholecystectomy and liver biopsy. Histopathology of the gallbladder revealed a mild cholecystitis with bile inspissation. Dog No. 5 was treated with dexamethasone and l-asparaginase. Dog No. 7 was initially diagnosed with aleukemic chronic lymphocytic leukemia of granular lymphocyte type and sequentially received prednisone, chlorambucil, cyclophosphamide, and CCNU, alone or in combination. All other dogs did not receive chemotherapy. Seven dogs were euthanized and 1 died (dog No. 3) from 1 to 23 days after initial diagnosis. One dog with HS-TCL was euthanized 196 days postdiagnosis (dog No. 7). Euthanasia or spontaneous death was a consequence of lymphoma in all cases.
Signalment and Affected Organs From Canine Patients With Hepatosplenic T-Cell Lymphoma (HS-TCL) and Hepatocytotropic T-Cell Lymphoma (HS-TCL).
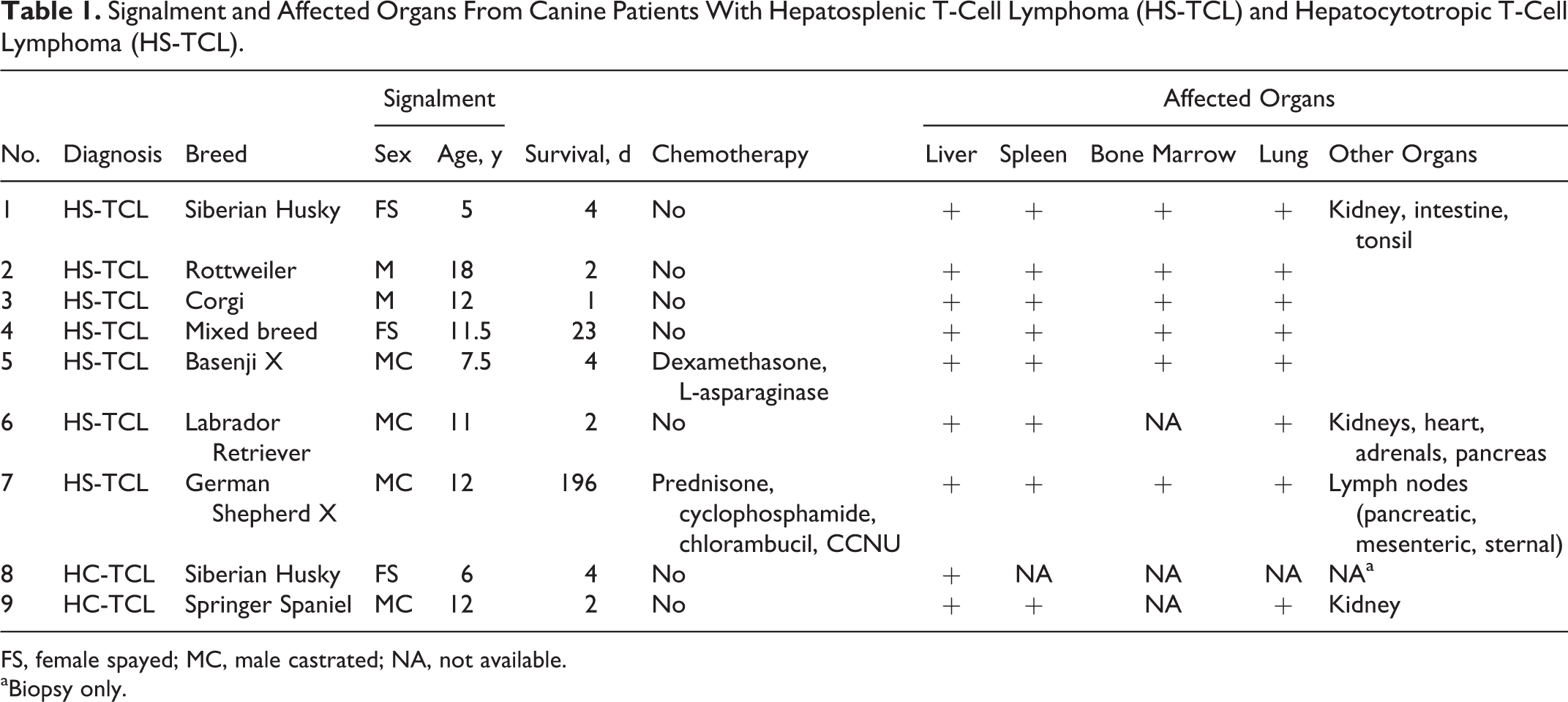
FS, female spayed; MC, male castrated; NA, not available.
aBiopsy only.
Clinicopathologic features
All 7 dogs with HS-TCL were anemic on presentation, with a median hematocrit of 29.9% (reference interval, 40%–55%) (Table 2). Five of 6 dogs with HS-TCL for which a reticulocyte count was done had a concurrent regenerative response (median reticulocyte concentration 118 300/μl; reference interval, 7000–65 000/μl). Thrombocytopenia was confirmed in 6 dogs with HS-TCL (median platelet concentration 76 000/μl; reference interval, 150 000–400 000/μl) and was suspected in another dog upon review of the blood smear (clumping invalidated the Advia count).
Clinicopathological Data From Canine Patients With Hepatosplenic T-Cell Lymphoma (HS-TCL) and Hepatocytotropic T-Cell Lymphoma (HC-TCL).
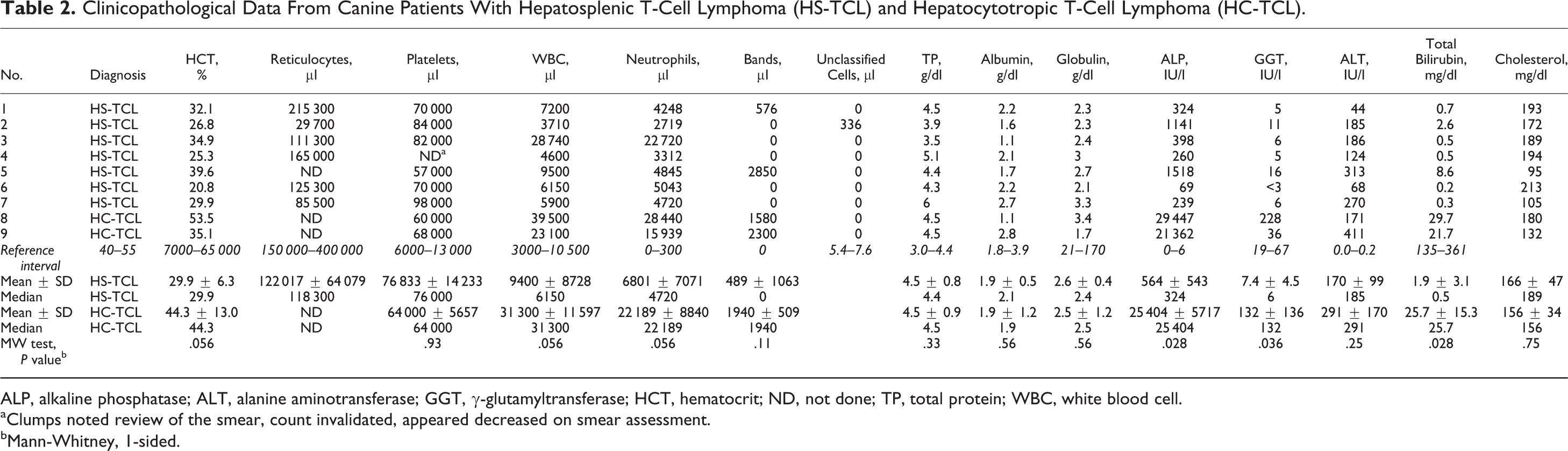
ALP, alkaline phosphatase; ALT, alanine aminotransferase; GGT, γ-glutamyltransferase; HCT, hematocrit; ND, not done; TP, total protein; WBC, white blood cell.
aClumps noted review of the smear, count invalidated, appeared decreased on smear assessment.
bMann-Whitney, 1-sided.
The median hematocrit in dogs with HC-TCL (44.3%; reference interval, 40%–55%) was higher than in dogs with HS-TCL (P = .056). Both dogs with HC-TCL were thrombocytopenic (median platelet concentration 64 000/μl; reference interval, 150 000–400 000/μl). Dogs with HC-TCL had higher leukocyte counts than dogs with HS-TCL (P = .056) (Table 2), and this was due to a higher mature neutrophilia (P = .056) that was also accompanied by mild left shifts in both instances.
Hypoproteinemia was present in 6 of 7 dogs with HS-TCL and both dogs with HC-TCL, predominantly due to hypoalbuminemia (median total protein of HS-TCL = 4.4 g/dl and HC-TCL = 4.5 g/dl; reference interval, 5.4–7.6 g/dl; median albumin = 2.1 g/dl and 1.9 g/dl, respectively; reference interval, 3.0–4.4 g/dl). Most dogs (8/9) had mild to moderate increases in hepatocellular leakage enzymes. Dogs with HS-TCL usually had mild increases in ALP, GGT, and total bilirubin. However, these 3 parameters were significantly higher in both dogs with HC-TCL (P = .028, P = .036, and P = .028, respectively). Both dogs with HC-TCL had bilirubin concentrations exceeding 20 mg/dl (reference interval, 0.0–0.2 mg/dl) and ALP activity exceeding 20 000 IU/L (reference interval, 21–170 IU/L). Both dogs with HC-TCL had coagulation profiles performed and had prolonged prothrombin time (PT) and partial thromboplastin time (PTT), increased D-dimer concentrations, and evidence of red blood cell (RBC) fragmentation on the CBC submitted at the same time. As these 2 dogs were also thrombocytopenic, these data indicate the likelihood of concurrent disseminated intravascular coagulation (DIC). Complete-linkage hierarchical cluster analysis was used to further analyze the clinical pathology of the 9 dogs (Fig. 1). Dog Nos. 1, 5, and 6 (all HS-TCLs) were closely clustered, as were dog Nos. 2, 3, 4, and 7 (all HS-TCLs). Both of these clusters were more closely related to each other than to a separate cluster containing dog Nos. 8 and 9 (both HC-TCLs). Dog Nos. 8 and 9 (both HC-TCL), although closely linked, were only distantly related to the individuals in the other 2 clusters (due to dissimilarities in the clinical diagnostic metrics).
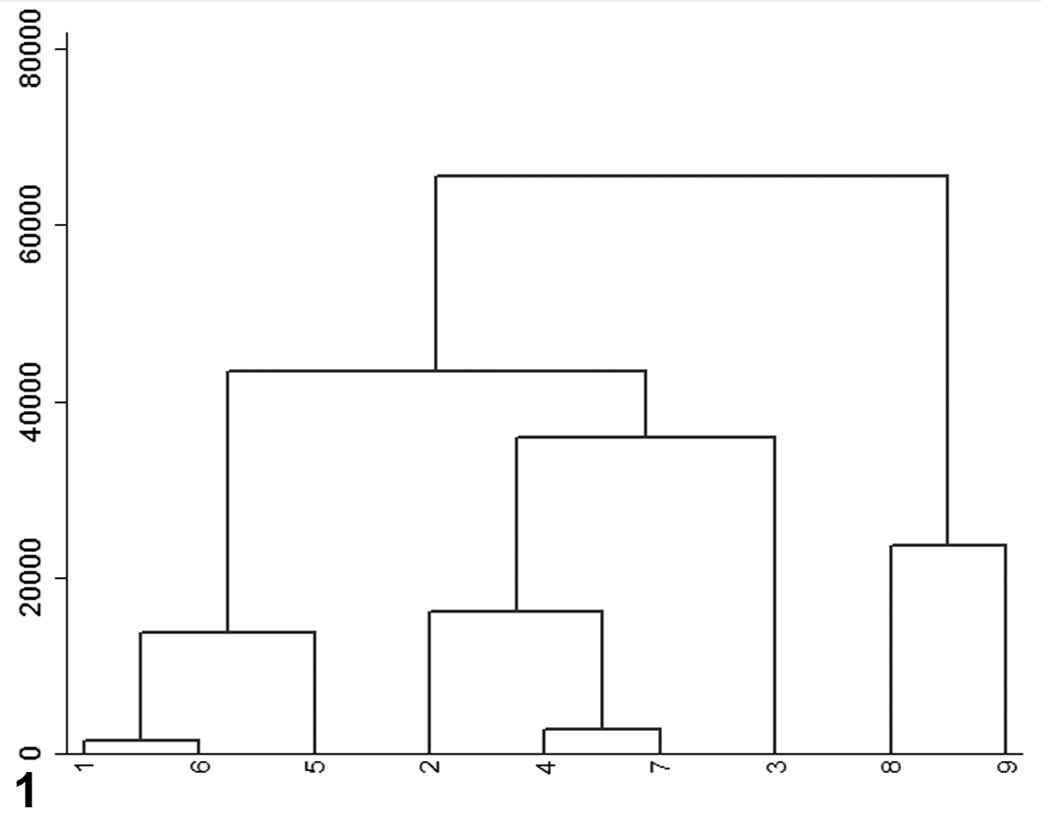
Dendrogram based on complete hierarchical linkage cluster analysis of the study population. Linked dogs with smaller dissimilarity scores are more closely related than dogs linked with higher dissimilarity scores. Dog Nos. 8 and 9 (both hepatocytotropic T-cell lymphomas), although closely linked, are only distantly related to all other cases. X-axis: dog Nos. 1 to 9. Y-axis: branch points 0 (same) to 80 000 (very different).
Cytologic findings
Four of the 7 dogs with HS-TCL had fine-needle aspirates of the liver performed by ultrasound guidance, which were interpreted as lymphoma in all but one (dog No. 2). All 7 dogs with HS-TCL had splenic aspirates, and all but one (dog No. 2) were interpreted as lymphoma. Dog No. 2 had marked macrophage hyperplasia and extramedullary hematopoiesis in liver and spleen, and the correct diagnosis was made only after interpretation of CD3 immunostains. On review of available Wright-Giemsa–stained smears, neoplastic lymphocytes had consistent cytomorphology. Lymphocytes were intermediate to large in size with nuclei from 1.5 to 3 red cells in diameter. Lymphocytes had moderate amounts of pale to medium blue cytoplasm that contained variable numbers of fine pink to magenta cytoplasmic granules that sometimes packeted in a perinuclear location (Fig. 2). Nuclei were round to oval or highly irregular in shape and had finely stippled chromatin and variably prominent nucleoli. Erythrophagia was noted in both neoplastic lymphocytes and the attendant hyperplastic macrophage population (Fig. 2). Fine-needle aspiration cytology was not done in either of the 2 dogs with HC-TCL.
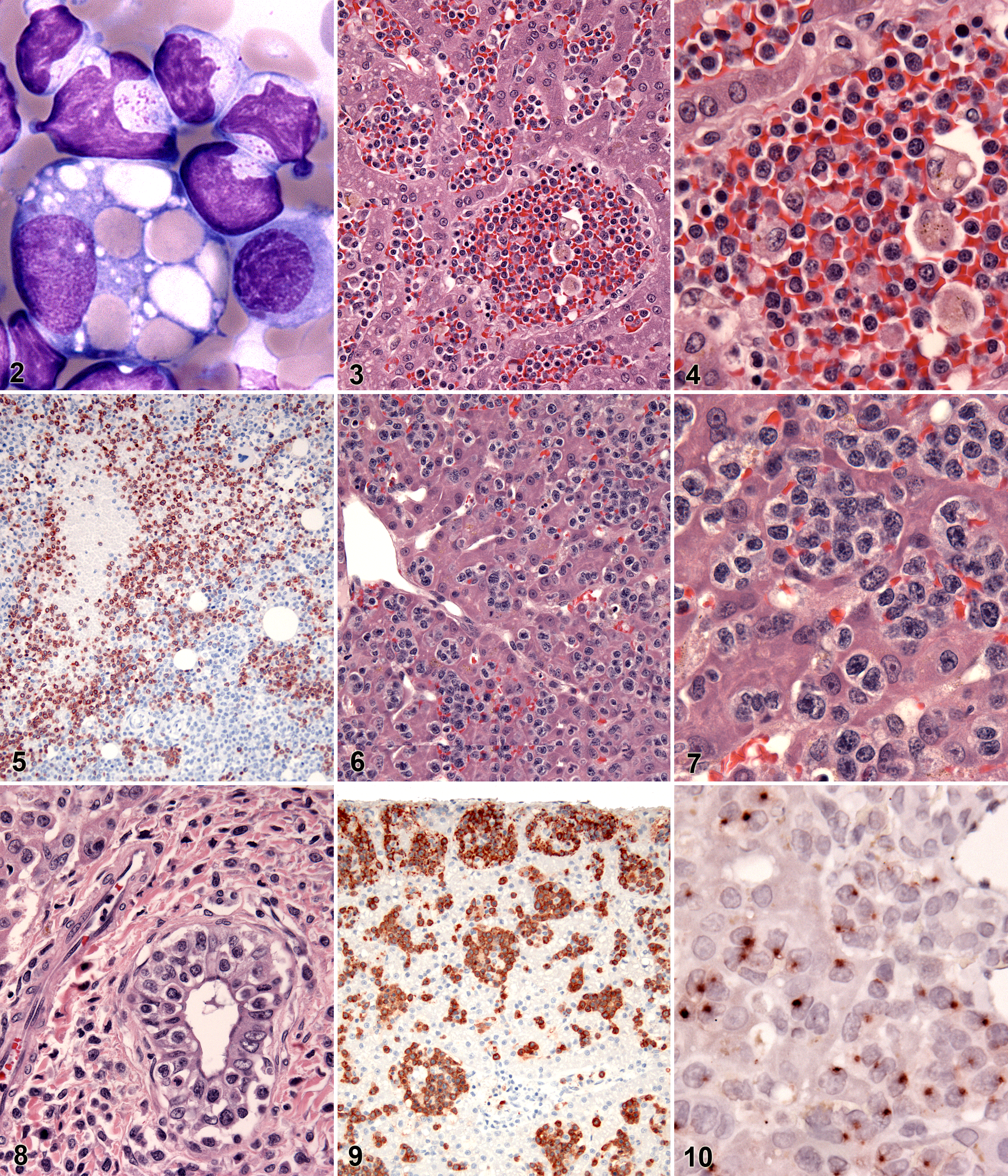
Spleen. Fine-needle aspirate. Canine hepatosplenic T-cell lymphoma, dog No. 7. Neoplastic lymphocytes contain fine, pink cytoplasmic granules and have irregular nuclear membranes. A macrophage contains multiple phagocytized erythrocytes. Wright-Giemsa stain.
Gross findings
The most consistent necropsy finding in HS-TCL was diffuse enlargement of the liver (mean, 5% of body weight; range, 4.0%–5.9%). The assessment of splenic weight and size was hampered by increased blood filling due to euthanasia in most cases. Necropsy data were only available for 1 dog with HC-TCL (dog No. 9), and no enlargement of either liver or spleen was noted subjectively. Four dogs had ascites (dog Nos. 1, 5, 7, 9), 1 had hemoabdomen secondary to splenic rupture (dog No. 3), and 1 dog had bile inspissation in the gallbladder (dog No. 8). All other findings were considered incidental or unrelated to the main lesion.
Histopathology
Hepatosplenic T-Cell Lymphoma
Liver, spleen, lung, and bone marrow were the most commonly involved organs. Other organs were affected inconsistently (Table 1).
In the liver, neoplastic lymphocytes were predominantly found within sinusoids (Fig. 3) with variable involvement of portal tracts and/or central venous areas. The overall tumor cell burden ranged from few, inconspicuous cells to large numbers that markedly expanded hepatic sinusoids and compressed adjacent cords. Neoplastic lymphocytes were commonly accompanied by increased numbers of erythrophagocytic macrophages (Fig. 4). Extramedullary hematopoiesis (EMH) was seen in 3 dogs. Fibrin thrombi variably accompanied by ischemic necrosis were present in all dogs.
In the spleen, neoplastic lymphocytes were centered on the sinusoids and cords of the red pulp. The red pulp involvement was extensive and led to white pulp atrophy. Abundant erythrophagocytic macrophages were seen in most dogs, and EMH was present in all dogs.
In the bone marrow, neoplastic lymphocytes appeared as variably sized clusters of monomorphic lymphocytes within a heterogeneous background of normal hematopoietic cells. Identification of neoplastic cells necessitated immunophenotyping (CD3) in some instances (Fig. 5).
In the lungs of all dogs, tumor cells were found within capillaries of alveolar septae. The severity of the infiltrate ranged from few, inconspicuous cells to complete filling of capillaries. A subset of dogs also had cells surrounding small- to medium-sized vessels or, to a lesser degree, forming small clusters within alveolar spaces.
Neoplastic lymphocytes were predominantly medium to large with round to oval nuclei, mostly indistinct nucleoli, a mild to moderate amount of eosinophilic to clear cytoplasm, and variably distinct cell borders (Fig. 4). Mitotic figures averaged between zero and 2 per 10 high-power fields (HPFs), and anisocytosis and anisokaryosis were generally mild. Occasionally, neoplastic lymphocytes were erythrophagocytic.
Hepatocytotropic T-Cell Lymphoma
The histopathological hallmark of HC-TCL was its distinct pattern of liver involvement. In addition to marked infiltration of hepatic sinusoids, neoplastic lymphocytes invaded hepatic cords individually or in clusters (Figs. 6 and 7). Despite the intimate association of lymphocytes with hepatocytes, no degenerative changes of hepatocytes were apparent. Macrophages were considerably less frequent in HC-TCL than in HS-TCL, and erythrophagocytosis was therefore not a significant feature. Extramedullary hematopoiesis was absent in the liver of both dogs. Despite the clinicopathologic evidence of DIC, neither infarcts nor fibrin thrombi were observed. Lymphocytic infiltration of bile duct epithelium was observed in 1 dog (dog No. 9) (Fig. 8).
The involvement of spleen and lung was minimal. The histopathologic findings in these organs paralleled HS-TCL with the exception that splenic macrophages were less numerous and splenic EMH was not apparent. No signs of gastrointestinal involvement were noted. Cytological features of neoplastic lymphocytes in HC-TCLs were similar to those observed in HS-TCL.
Immunohistochemistry
Neoplastic lymphocytes in HS-TCL expressed CD3 in 5 of 7 dogs (Fig. 5 and Table 3). Three of 5 dogs, for which frozen specimens were available, had neoplastic lymphocytes that expressed a γδ TCR. Neoplastic lymphocytes in 2 dogs (dog Nos. 5 and 7) lacked TCR and CD3 expression. Neoplastic lymphocytes did not express the coreceptor molecules CD4 and CD8β. In 3 of 5 dogs, neoplastic lymphocytes expressed CD8α likely as a homodimer. CD11d was expressed by neoplastic lymphocytes in 6 of 7 dogs (Fig. 9). In both dogs with HC-TCL, neoplastic lymphocytes had a CD3+, CD11d– immunophenotype. In the dog for which frozen tissue was available (dog No. 9), neoplastic lymphocytes expressed a γδ TCR but lacked expression of CD4 and CD8β with variable expression of CD8α.
Immunohistochemical Findings in Canine Hepatosplenic T-Cell Lymphoma (HS-TCL) and Hepatocytotropic T-Cell Lymphoma (HC-TCL).
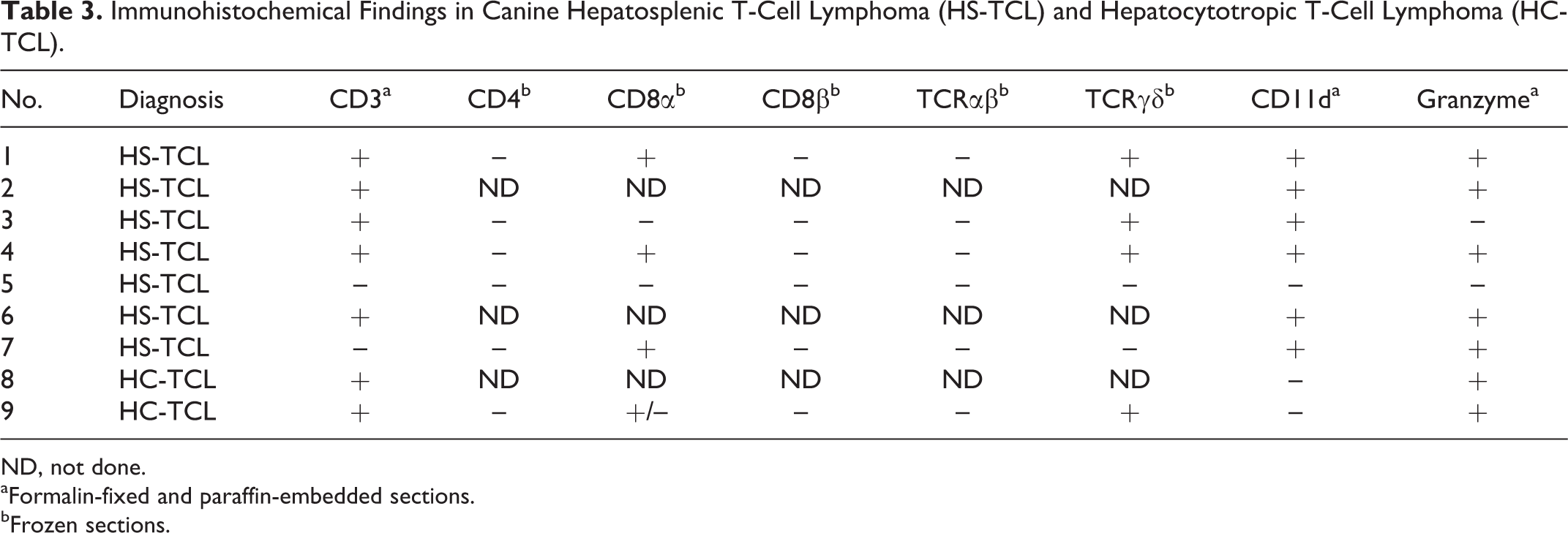
ND, not done.
aFormalin-fixed and paraffin-embedded sections.
bFrozen sections.
Granzyme B was expressed by neoplastic lymphocytes in 5 of 7 dogs with HS-TCL and both dogs with HC-TCL. Although the staining pattern for other markers was diffusely membranous and cytoplasmic, granzyme B+ cells had one to multiple, variably sized, punctate, cytoplasmic granules, often clustered in one area of the cell (Fig. 10).
Transmission electron microscopy
Transmission electron microscopy (TEM) was performed on 1 dog with HC-TCL (dog No. 8) to investigate the relationship between hepatocytes and invading lymphocytes. Neoplastic lymphocytes were not located within the cytoplasm proper of hepatocytes. Instead, lymphocytes were separated from the cytoplasm of hepatocytes by a clear space and an additional membrane (Fig. 11).
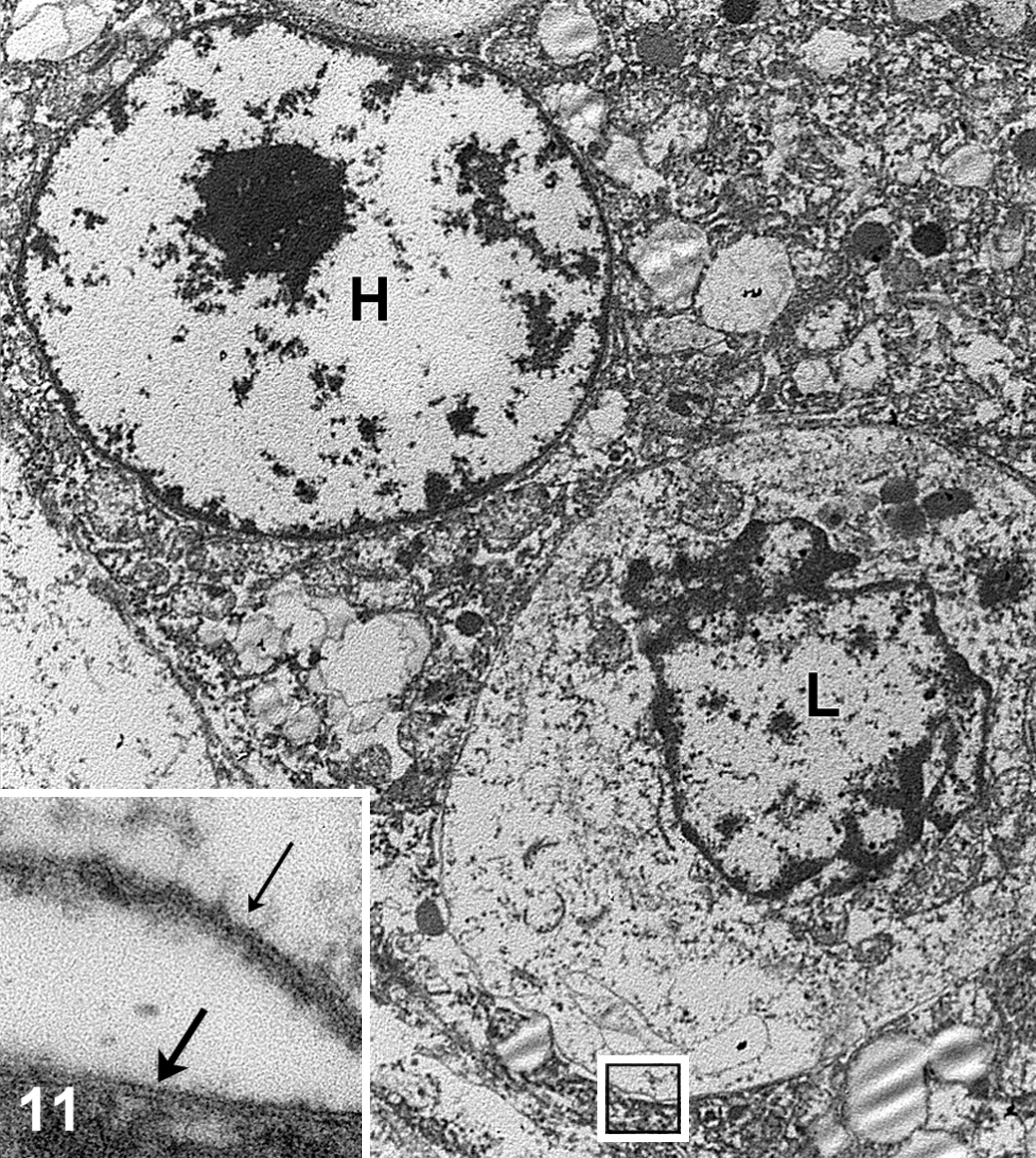
Liver. Canine hepatocytotropic T-cell lymphoma, dog No. 8. A neoplastic lymphocyte is located within the cytoplasm of a hepatocyte (H, hepatocyte; L, lymphocyte); the square indicates the position of the inset. Inset: the lymphocyte cytoplasmic membrane (thin arrow) is surrounded by a clear space and the cytoplasmic membrane of the hepatocyte (thick arrow). Transmission electron microscopy.
Clonality analysis
Neoplastic lymphocytes in all cases had between 3 and 6 clonal rearrangements of the TRG gene. A detailed description of gene usage and rearrangement patterns is given elsewhere. 12
Discussion
This study evaluated the clinicopathologic, histologic, and immunophenotypic findings in 9 canine T-cell lymphomas involving the liver in the absence of a peripheral lymphadenopathy. Seven dogs had HS-TCL, supporting its classification as a distinct WHO entity analogous to the human disease. However, 2 dogs differed in their clinicopathologic presentation (Table 2, Fig. 1), histologic pattern of liver involvement, and immunophenotype of neoplastic cells (Table 4). In contrast to the 7 dogs with HS-TCL, these 2 dogs had higher hematocrits, higher neutrophil counts, and more severe cholestasis. Using complete-linkage hierarchical cluster analysis, the clinical pathology data segregated into 2 distinct clusters representing HS-TCL and these 2 dogs. The clinicopathologic differences along with a distinctly different pattern of liver involvement and different immunophenotype indicate a separate biological entity rather than a histologic variant of HS-TCL. On the basis of the distinct tropism of neoplastic lymphocytes for hepatocytes, the term hepatocytotropic T-cell lymphoma (HC-TCL) is proposed.
Summary of Findings in Hepatosplenic T-Cell Lymphoma (HS-TCL) vs Hepatocytotropic T-Cell Lymphoma (HC-TCL).
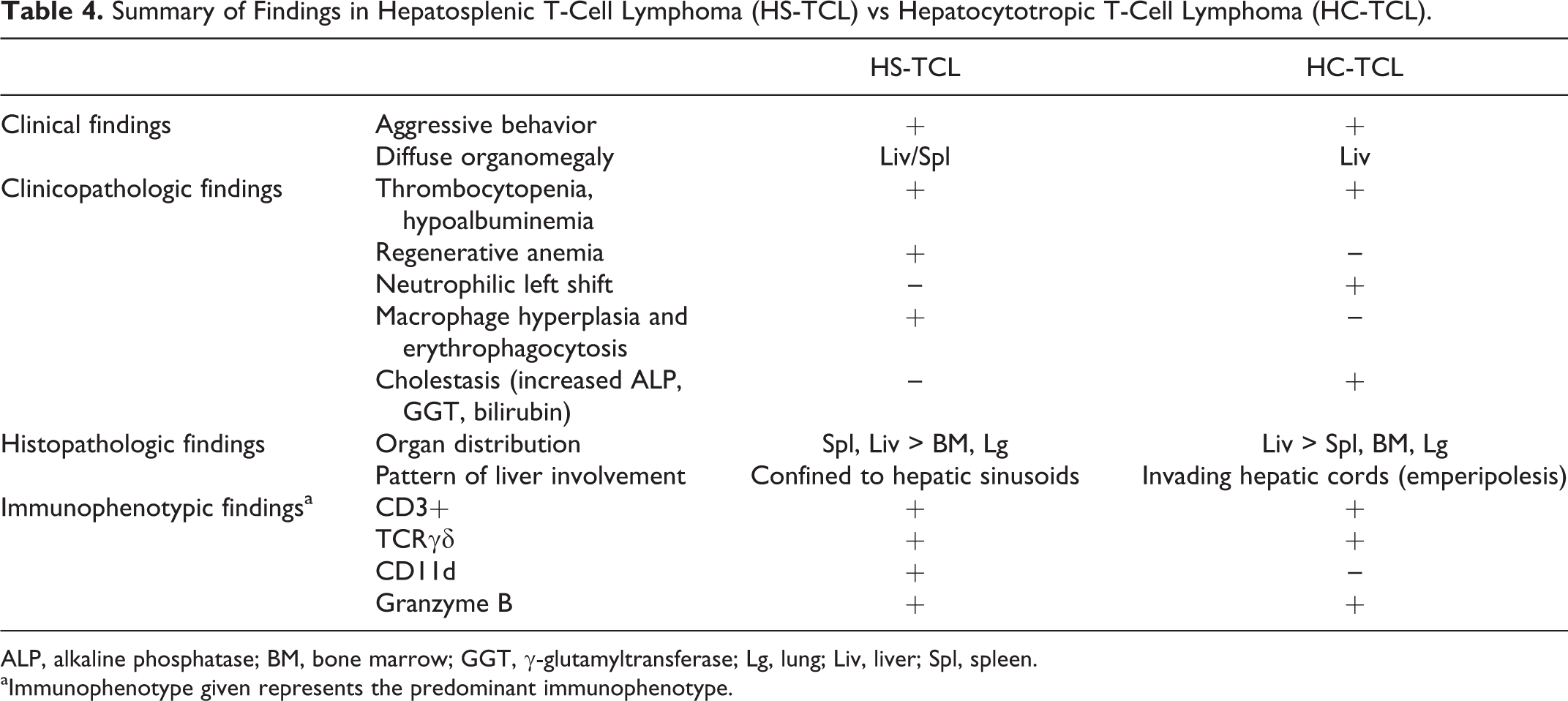
ALP, alkaline phosphatase; BM, bone marrow; GGT, γ-glutamyltransferase; Lg, lung; Liv, liver; Spl, spleen.
aImmunophenotype given represents the predominant immunophenotype.
Human HS-TCL is believed to arise from splenic cytotoxic T cells, most commonly of γδ origin, and exhibits distinct clinicopathologic features. The findings in canine HS-TCL closely recapitulated the human disease. Neoplastic lymphocytes in most dogs, for which the TCR could be assessed, expressed a γδ TCR. Gamma delta T cells are a special group of T cells that bridge innate and adaptive immunity and are enriched in various epithelia as well as the red pulp of the spleen. Neoplastic lymphocytes in 2 dogs lacked expression of a T-cell antigen receptor (αβ or γδ chains) and CD3. Given that both had clonally rearranged TRG genes, lack of reactivity with CD3 and TCR antibodies is assumed to be due to complete loss of T-cell antigen receptor complex expression. A natural killer (NK) cell origin of neoplastic lymphocytes is theoretically possible but is considered less likely. Rearrangement of the TRG locus has been shown only in approximately 1% of murine splenic NK cells. 20 Assuming a similar prevalence in the dog, the occurrence of 2 NK cell neoplasms with rearranged TRG chains in this study is considered unlikely. The precise lineage of the neoplastic cells in these 2 dogs remains unknown. Neoplastic lymphocytes in all dogs lacked expression of CD4 and CD8β and inconsistently expressed CD8α. This is in line with reports of HS-TCL in humans and is a common immunophenotype of γδ T cells. 9
Hepatosplenic T-cell lymphoma in dogs most likely originates from CD11d+ splenic red pulp γδ T cells. Neoplastic lymphocytes expressed CD11d in all but 1 dog and markedly expanded the splenic red pulp. In contrast to the liver, the splenic red pulp has been shown to harbor high numbers of CD11d+ lymphocytes normally. 14 Gamma delta T cells that express CD11d are 4-fold enriched in splenic red pulp compared with peripheral blood (S. McDonough and P. Moore, unpublished observations). Further evidence in support of a splenic origin was the pronounced involvement of the spleen with minimal involvement of the liver in 1 dog (dog No. 3).
Granzyme B expression in neoplastic lymphocytes of most dogs with HS-TCL was consistent with a cytotoxic T-cell origin. Lack of reactivity despite the presence of cytoplasmic granules in the remaining 2 dogs does not exclude a cytotoxic T-cell origin since expression of granzyme B has been shown to depend on the activation state of the cell.2,8
The clinicopathologic findings in canine HS-TCL closely mimicked the human counterpart. All dogs lacked peripheral blood lymphocytosis. Dogs were variably thrombocytopenic and anemic, which was typically regenerative. Erythrophagocytosis by neoplastic lymphocytes and a concurrent hyperplastic population of (erythophagocytic) macrophages were a consistent feature in HS-TCL, suggesting that anemia is, at least in part, attributable to a secondary hemophagocytic syndrome. The common presence of a hemophagocytic syndrome secondary to HS-TCL in this series of dogs with HS-TCL is in agreement with previous reports in both people and dogs.5,6 In dog No. 2, the markedly expanded population of hemophagocytic macrophages in association with relatively low numbers of neoplastic T cells in some sections resembled hemophagocytic histiocytic sarcoma (HHS). Differentiation of the 2 entities in this instance was further confounded by their similar biochemical profiles. Patients with either HHS or HS-TCL typically present with regenerative anemia, thrombocytopenia, and hypoalbuminemia. Hemophagocytic histiocytic sarcoma is therefore a potential differential diagnosis in dogs with HS-TCL, necessitating thorough and concurrent evaluation of the clinicopathologic, histopathologic, immunophenotypic, and molecular clonality data to make the distinction. Seven of 9 dogs did not receive chemotherapy and died or were euthanized within 23 days of diagnosis. One of the 2 dogs that did receive treatment survived for 196 days. However, the low number of treated dogs precludes conclusions regarding the efficacy of chemotherapy. In most cases, the owners elected euthanasia because of advanced disease progression at the time of diagnosis.
Hepatocytotropic T-cell lymphoma shared several features with HS-TCL but also showed distinct differences suggestive of a separate clinicopathologic entity. Like HS-TCL, HC-TCL seems to arise from a cytotoxic γδ T cell. Neoplastic lymphocytes in the dog available for TCR immunophenotyping expressed a γδ TCR, and neoplastic lymphocytes in both dogs were positive for CD3 and granzyme B. HC-TCL had an aggressive clinical course, and patients presented with thrombocytopenia and hypoalbuminemia. HC-TCL differed from HS-TCL in the pattern of hepatic involvement, lack of expression of CD11d, and clinicopathologic features. The most striking histopathologic feature of HC-TCL was the invasion of hepatic cords by neoplastic lymphocytes, which resembled emperipolesis. The term emperipolesis (from Greek, “wandering round about within”) was coined by Humble et al 10 in 1956 to describe the phenomena of cells wandering freely within the cytoplasm of larger host cells. However, transmission electron microscopy revealed that lymphocytes in HC-TCL resided between hepatocytes or within invaginations of hepatocyte cell membranes rather than within the cytoplasm proper of hepatocytes. These findings parallel the location of “intraepithelial” lymphocytes in the intestine and indicate a similar epitheliotropism. Invasion of hepatic cords by neoplastic lymphocytes has been described in cats.15,17 The pattern of liver involvement in cats was identical to that in dogs in the present study. However, most feline cases described to date lack comprehensive clinical, clinicopathologic, and pathological data.
Neoplastic lymphocytes in both dogs with HC-TCL lacked expression of CD11d. This could indicate that HC-TCL does not arise from lymphocytes of the splenic red pulp, as these cells commonly express CD11d. Instead, a primary hepatic origin is most likely. Also, the most severely affected organ in the only dog with HC-TCL available for necropsy was the liver with only minimal involvement of the spleen. Similarly, involvement of the spleen was not emphasized in previous reports of feline lymphoma similar to HC-TCL, although spleen was available only in 2 of 14 total cats.15,17 A primary hepatic origin would also be consistent with the liver’s role as an organ with predominantly innate immunity and relatively high numbers of γδ T cells. 7 However, antigen loss by neoplastic cells cannot be ruled out, and careful assessment of organ involvement in future cases is needed to fully elucidate this question.
The most remarkable clinicopathologic difference between HC-TCL and HS-TCL was the presence of severe jaundice and cholestasis in both dogs with HC-TCL. Neither prehepatic causes of hyperbilirubinemia nor posthepatic biliary obstruction was noted in either dog. Given the intimate association of hepatocytes with neoplastic lymphocytes, it is logical to speculate that intracellular and bile canalicular transport and secretion of bilirubin were impeded by the latter. In addition, dogs with HC-TCL had higher hematocrits than dogs with HS-TCL. The lack of secondary hemophagocytic syndrome, which was common in HS-TCL, likely explains this hematological difference.
In conclusion, this study supports the classification of HS-TCL as a distinct entity in dogs, which is analogous to the human counterpart in the WHO classification scheme for hematopoietic neoplasia. In addition, a new form of hepatic lymphoma with distinctive architectural, immunophenotypic, and clinicopathologic features was recognized. It is characterized by marked tropism for hepatocytes, and the term hepatocytotropic T-cell lymphoma is proposed. Additional cases with detailed clinicopathologic, histopathologic, and immunophenotypic data are needed to further define this entity in dogs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.